
Abstract
Objective
Although synchronous multiple primary lung cancers (sMPLCs) are common in clinical practice, the choice of surgical modalities for the main lesion is still at the stage of exploration. This study is designed to analyze the prognosis of sMPLCs and single primary lung cancers with similar tumor stages and to explore whether sublobar resection has a similar prognosis as lobectomy for sMPLCs.
Methods
One-hundred forty-one cases of sMPLCs were selected, including the following: 65 cases underwent lobectomy for main lesions, and 76 cases underwent sublobar resection for main lesions. One thousand one hundred forty-four cases of single primary lung cancer were matched at 1:1 by propensity score matching. Then, the patients with sMPLCs were divided into a lobectomy group and a sublobar group according to the first tumor stage. Ninety-eight cases of patients with sMPLCs were matched. The short-term perioperative effect, 5-year disease-free survival (DFS) rate, and 5-year overall survival (OS) rate between the two groups were compared.
Results
There was no significant difference in OS between sMPLCs and single primary lung cancer after lobectomy (77.1% vs. 77.2%, P = 0.157) and sublobar resection (98.7% vs. 90.7%, P = 0.309). There was no significant difference in OS (86.7% vs. 83.9%, P = 0.482) or DFS (67.6 vs. 87.7%, P = 0.324) between the lobectomy group and sublobar group with sMPLCs. The sublobar resection group obtained a lower incidence of postoperative complications (40.8% vs. 16.3%, P = 0.007) and shorter postoperative hospital stay (11.22 vs. 9.27, P = 0.049).
Conclusion
The prognosis of patients with sMPLCs generally depends on the main tumor state, which has no statistical difference regardless of sublobar resection or lobectomy, and the perioperative period of sublobar resection is safer than that of lobectomy.
Similar content being viewed by others


Key question
Is there a difference in the survival of sMPLCs and single primary lung cancers with similar tumor stages? Does sublobar resection have the similar prognosis as lobectomy for sMPLCs?
Key findings
There was no difference in survival between sMPLCs and single primary lung cancer after lobectomy and sublobar resection. There was no significant difference in survival between the lobectomy group and sublobar group with sMPLCs.
Take-home message
The prognosis of sMPLCs generally depends on its main tumor state. Whether sublobar resection or lobectomy, the prognosis of sMPLCs has no statistical difference.
Introduction
In 1924, Beyreuthe [1] first reported two cases of independent lung cancer at the same time and introduced the concept of multiple primary lung cancer (MPLC) for the first time, that is, two or more primary lung malignant tumors occur simultaneously or successively in the same patient. According to the diagnosis interval of 2 years, it can be divided into synchronous MPLC (sMPLCs) and metachronous MPLC (mMPLC). MPLC was considered as a rare disease in the past. However, in recent years, due to the increasingly obvious trend of population aging, its detection rate is gradually increasing, and its incidence is on the rise, accounting for 3–13% of the total number of lung cancer cases [2,3,4,5].
Due to the differences in the characteristics of lung cancer, and more complex characteristics after the combination of multiple tumors, the difficulty of prognosis research of MPLC is greatly increased. Recently, most sMPLCs are diagnosed as early lung cancer, which can be cured in principle and have a good prognosis, but the results of prognostic studies are quite different [6,7,8,9]. The 2017 NCCN guidelines [10] recommend that standard lobectomy should be performed in patients with MPLC with sufficient pulmonary function reserve, while sublobar resection including segmentectomy resection and wedge resection can be used as an alternative. At present, among single-center studies, due to few cases, short follow-up time, less grouping, and other reasons, there is no reliable study on the relationship between surgical methods and the prognosis of sMPLCs, and whether the prognosis of sMPLCs depends entirely on the single staging of the first tumor is still lack of credible reports.
Therefore, this study conducted a single-center retrospective analysis to compare the efficacy of sublobar resection and lobectomy in the treatment of sMPLCs and to investigate whether the prognosis of sMPLCs is the same as that of matched single primary lung cancer, hoping to provide some references for the treatment of sMPLCs.
Materials and methods
Patients
This study retrospectively analyzed the clinical data of 2635 patients with non-small cell lung cancer (NSCLC) who underwent surgery in Jiaxing First Hospital from January 2012 to June 2019 and was approved by the Ethics Committee of Jiaxing First Hospital. Patients with sMPLCs with at least 2 lesions were screened out.
Entry conditions
In accordance with the diagnostic criteria of Martini and Melamed [11], sMPLC is as follows:
-
(1) different pathological types; (2) multiple lesions found at the same time but located in different lobes and without lymph node or systemic metastasis; and (3) the same histological type but located in different segments, lobes, or bilateral lungs and originated from different carcinoma in situ; there was no cancer in the common lymph node drainage site and no extrapulmonary metastasis at the time of diagnosis.
The inclusion criteria of single primary lung cancer are as follows: (1) NSCLC with stages 1A–3A, (2) only one lesion, and (3) there was no cancer in the common lymph node drainage site and no extrapulmonary metastasis at the time of diagnosis.
-
A.
According to the eighth edition of the international lung cancer staging standard, the main focus stage is the 1A–3A stage of NSCLC.
-
B.
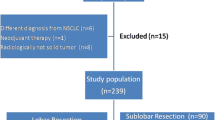
According to the eighth edition of the international lung cancer staging standard, NSCLC in which the secondary lesions were staged as stages 1A–3A, the loss of clinical data or survival follow-up time of less than 1 year was excluded. The detailed screening process is shown in Fig. 1.

Screening and matching flowchart
Finally, 141 cases of sMPLCs with complete clinical data and postoperative survival follow-up data were selected, accounting for 5.3% of lung cancer patients in our hospital in the same period. The incidence rate is similar to the existing report [2,3,4,5]. In addition, a total of 1144 patients with single primary lung cancer were enrolled.
In order to balance the basic data of sMPLCs group and single primary lung cancer group, we performed the 1:1 tendency matching method according to the different surgical methods of the main tumor.
Follow-up and related definition
All patients with sMPLCs had complete medical history and follow-up data. The main preoperative examinations were chest CT, abdominal color ultrasound, craniocerebral MRI or CT, and bone scan. The observation indicators included age, sex, preoperative complications, smoking history, and family history of lung cancer. The perioperative observation indexes included operation mode, operation time, postoperative drainage, postoperative hospital stay, postoperative complications, and hospitalization expenses. The postoperative pathological indexes included the size and stage of the main tumor, the size of the secondary tumor, the pathological type and the degree of pathological differentiation, and the time and location of recurrence or metastasis after operation. The follow-up time was from the operation day to the tumor recurrence, metastasis, death, or research cutoff date. Local recurrence was defined as lung recurrence and hilar lymph node and mediastinal lymph node recurrence on the operative side, and distant metastasis was defined as distant organ metastasis. The 5-year disease-free survival (DFS) was defined as the proportion of patients who had no tumor recurrence, metastasis, or cancer-related death from the end of the operation to the end of follow-up. The 5-year overall survival (OS) was defined as the proportion of patients who did not have cancer-related deaths from the end of the operation to the end of follow-up.
Statistical methods
The data were processed by the SPSS 25.0 statistical software package, the measurement data were expressed by mean ± standard deviation (x ± s), and the propensity score matching was used to balance the basic data of the two groups of patients. T-test was used for data analysis among groups, percentage (%) was used for counting data, four-grid chi-square test was used for comparison between the groups, Kaplan–Meier survival curve was used for DFS analysis and OS analysis, and log rank was used for statistical analysis.
Results
Basic data statistics of patients with sMPLCs and single primary lung cancers
A total of 141 patients with sMPLCs who met the inclusion and exclusion criteria were divided into a lobectomy group (n = 65) and a sublobar resection group (n = 76). A total of 1144 patients with single primary lung cancer were enrolled in the group and divided into a lobectomy group (n = 729) and a sublobar resection group (n = 415). In order to balance the basic data of the two groups, we performed the 1:1 tendency matching method according to the different surgical methods of the main tumor, and the matching value was set at 0.01, which was 5% of the standard deviation of the tendency index. As a result, 65 pairs were matched in the lung lobectomy group, and 75 pairs were matched in the sublobar group. There were no significant differences in age, sex, and tumor stage between the two groups. The clinical features are shown in Tables 1 and 2.
Comparison of prognosis between sMPLC and single lung cancer
A total of 140 cases of single primary lung cancer were matched, including 65 pairs of lobectomy (including 65 cases in sMPLC group, 65 cases in single primary lung cancer group, and 664 cases in single primary lung cancer group were removed) and 75 pairs of sublobar resection (including 75 cases in sMPLC group, 75 cases in single primary lung cancer group; 1 case in sMPLC groups and 340 cases in single primary lung cancer group were removed). The patients in the two groups were followed up for 14–81 months. Up to the end of follow-up, 7 cases died after lobectomy for single primary lung cancer and 12 cases with recurrence and metastasis. Eleven cases died after lobectomy for sMPLCs and 14 cases with recurrence and metastasis. The 5-year DFS was 67.6 vs. 65.3%, P = 0.319. The 5-year OS was 77.1% vs. 77.2%, P = 0.157. A total of 1 case died of sublobar resection of single primary lung cancer; 3 cases of recurrence and metastasis; 3 cases of death of sublobar resection of multiple lung cancer; 5 cases of recurrence and metastasis; 5-year OS was 98.7% vs. 90.7%, P = 0.309; and 5-year DFS was 90.6% vs. 90.8%, P = 0.587. In the matched MPLC and single primary lung cancer, whether the main tumor underwent lobectomy or sublobar resection, the DFS and OS of the two groups were not significantly abnormal (Fig. 2).

a Comparison of single primary lung cancer and sMPLC DFS after lobectomy. b Comparison of single primary lung cancer and sMPLC OS after lobectomy. c Comparison of single primary lung cancer and sMPLC DFS after sublobar resection. d Comparison of single primary lung cancer and sMPLC OS after sublobar resection
Basic data statistics of patients with MPLCs
General information of sMPLCs pre-matching and after matching
A total of 141 patients with sMPLCs were enrolled, including 50 males and 91 females. Their age ranged from 35 to 81, with an average of 55.8 years. The clinical characteristics of sMPLCs pre-matching and after matching with lobectomy and sublobar resection are shown in Table 3. In order to balance the basic data of the two groups of patients, we performed a 1:1 propensity matching method according to the different surgical methods of the main lesion (lobectomy and sublobar resection) in the sMPLCs group. The included parameters were age, sex, the primary lesion tumor size, primary lesion stage, number of lesions, secondary lesion size, smoking history, and family history of lung cancer. The matching value was set at 0.2, which was 20% of the standard deviation of the propensity index. The results matched 49 pairs of sMPLC lobectomy and sublobar resection, with a total of 98 cases (43 cases were excluded). Although there were still differences in the size of primary and secondary lesions after matching, the difference was decreasing, and there was no statistically significant difference in the stages of primary lesions and tumor differentiation between the two groups after matching. Due to the limitation of the number of cases, perfect propensity matching could not be achieved, but overall, there was no significant difference in age, sex, main lesion size and stage, degree of differentiation, number of lesions, and pathological type between the two groups of patients (P > 0.05).
The perioperative situation of two groups of sMPLCs
There were no deaths during the perioperative period of the enrolled sMPLCs. The operation time of lobectomy for sMPLCs, postoperative drainage, hospitalization expenses, and sublobar resection were not significantly different, but the hospital stay after lobectomy was longer than sublobar resection (Table 4).
Prognosis of sMPLCs undergoing lobectomy and sublobar resection
A total of 49 pairs of patients were matched, with a total of 98 cases. Patients in the two groups were followed up for 12–81 months. By the end of the follow-up, 3 cases of the sublobar group patients died and 4 cases of recurrence and metastasis, 6 cases of patients died in lobectomy group and 8 cases of recurrence and metastasis, and all deaths and recurrence or metastasis were cancer related. DFS rate is as follows: the 1-year, 3-year, and 5-year DFS of the two groups were 93.9% vs. 98.0%, 84.4% vs. 91.1%, and 67.6 vs. 87.7%, log rank = 0.974, P = 0.324; the survival rates are as follows: 1-year, 3-year, and 5-year OS were 95.9% vs. 100%, 86.7% vs. 93.2%, and 86.7% vs. 83.9%, log rank = 0.495, P = 0.482. The DFS and OS of matched sMPLCs were not statistically significant regardless of sublobar resection or lobectomy (survival curve comparison is shown in Fig. 3.)

a Comparison of DFS in sMPLC groups: sublobar resection vs lobectomy. b Comparison of OS in sMPLC groups: sublobar resection vs lobectomy
Discussion
sMPLC was considered a rare disease in the past. In recent years, due to the continuous improvement of the diagnosis level, its incidence has increased. Existing research suggests that the incidence of MPLCs is on the rise. Guo [12] summarized 326 cases of MPLC with the incidence rate of 5.6%, and our result showed that the rate was 5.7%, which is similar to global research [5, 13,14,15] after the twentieth century. There are currently no clear diagnostic criteria for sMPLC, and the MM diagnostic criteria in 1975 [11] are the most classic. Of course, ACCP [16] guidelines have partially revised the MM criteria in 2003, 2007, and 2013, and the main point of the improvement is to increase the identification of differences in molecular genetics on the original basis. Dr. Liu Yi [17] found that the diagnostic criteria for MM and the second-generation gene sequencing technology based on gene rearrangement have a diagnostic consistency rate of 91.9% in the multicenter sMPLCs diagnostic verification test. Because gene sequencing technology has not been widely used clinically, the current MM standard is still the main reference standard for the diagnosis of MPLCs. Our research on the diagnosis of MPLCs also followed the MM standard in 1975. In this study, the pathological results of sMPLCs were mainly adenocarcinoma-adenocarcinoma, followed by squamous cell carcinoma-squamous cell carcinoma. However, different pathological types of sMPLCs were relatively rare, which is also in line with existing reports [12, 18, 19].
Many investigations have been carried out to help predict and improve the prognosis of lung cancer in recent years [20, 21]. For example, Le V. H. et al. [22] developed a model for predicting OS in patients with NSCLC based on risk scores of CT-based radiomics signatures. However, due to the complicated design of research involving sMPLC, there are still no multicenter prospective controlled studies to support and guide the treatment of this disease. At present, the treatment of sMPLCs only relies on the experience of clinicians and the consensus of a few experts. There are few studies on the prognosis regarding surgical treatment of MPLCs and single primary lung cancers. Early studies [23,24,25,26,27,28,29] have shown that lobectomy has a better prognosis than limited resection. In recent years, due to the overall diagnostic level of lung cancer improvement, the staging of operable lung cancer is relatively early, especially for the single ground-glass nodules with tumors ≤ 2 cm; sublobar resection can obtain a similar prognosis to lobectomy [30, 31]. Yu’s study [10] showed that there was no significant difference in the 5-year survival rate of MPLCs matching the single primary lung cancer stage (61.3% vs. 68.8%, P = 0.474). The sample size in our research was expanded. A total of 141 patients with sMPLC were enrolled in the group, and the grouping was more refined. We compared the prognosis of patients with sMPLCs and single primary lung cancers who underwent lobectomy or sublobectomy for main tumor, respectively. We used statistical methods to match single primary lung cancers with sMPLCs in terms of age, sex, and size of main tumor, especially similar in stage of main tumor, whether lobectomy was selected (77.1% vs. 77.2%, P = 0.157) or sublobar resection (98.7% vs. 90.7%, P = 0.309) can achieve similar oncological prognosis. This result also indicates that the prognosis of sMPLCs depends on its main tumor stage.
If the prognosis of multiple primary tumors depends on the staging of its main tumor, whether the surgical options for the main lesions of sMPLCs are the same as that of single primary lung cancer remains to be further studied. For single primary lung cancer, the North American Lung Cancer Research Group’s research [32] established the gold standard positioning of lobectomy + mediastinal lymph node dissection for the treatment of operable lung cancer more than 20 years ago. In recent years, due to changes in the types of lung cancer, more and more indolent lung cancers, sMPLCs, and elderly lung cancer patients who cannot tolerate lobectomy have gradually increased. Sublobar resection with less damage, including anatomical segmentectomy and wedge resection, is gradually increasing [33]. The current research [30, 34] supports anatomical segmentectomy for the treatment of stage 1 NSCLC, especially for stage 1 lung cancer with a diameter of ≤ 2 cm. These studies only focus on single primary lung cancer, and there is no prospective study on sublobar resection for sMPLCs. Previous retrospective studies [13,14,15,16] included few cases and did not specifically compare the prognosis of sMPLCs with different surgical methods. Trousse [13] believes that pneumonectomy alone is an independent risk factor for MPLC surgery. Yu [10] pointed out that for patients with stage 1 bilateral MPLC, sublobar resection can achieve a 5-year survival rate of 75%, not inferior to lobectomy. Xue [35] also believes that sMPLCs with two or more tumors should be evaluated separately and treated as independent tumors, and the prognosis of MPLCs is significantly better than that of metastatic lung tumors.
Because of the limitations of surgical access in the sublobar group, the diameter of the main lesion of sublobar group was smaller than that of lobectomy group, and the main lesion in the lobectomy group was staged relatively late. The sMPLCs are generally dominated by 2 lesions, and the pathological type is mainly adenocarcinoma-adenocarcinoma, which is also consistent with existing reports [12, 25, 30, 31, 10, 32, 33, 30, 34, 35]. Because carcinoma in situ often does not spread to local lymph nodes or distant metastases, the 5-year survival rate of patients with carcinoma in situ is close to 100%; while patients with invasive adenocarcinoma are more aggressive and prone to recurrence and metastasis after surgery, the prognosis is poor [36, 37]. In this study, we excluded patients whose main lesion was carcinoma in situ, and the 5-year OS rate of 141 patients with sMPLC was 84.6%, which was higher than some current retrospective studies [9, 10, 17, 30, 34], similar to Guo Haifa’s research results [12]. It is worth noting that this study suggests that different surgical methods for the main lesion do not affect the prognosis of sMPLCs. In order to further balance the bias between the MPLC group and the sublobar group, we performed a tendency-matching analysis of sublobar resection and lobectomy in the main tumor of sMPLCs. A total of 49 pairs of sMPLCs were matched. Although the size of the primary and secondary lesions after matching is still different, the difference is decreasing, and there was no statistically significant difference in the stage of the main lesions and the degree of tumor differentiation. Due to the limitation of the number of cases, perfect propensity matching could not be achieved. However, there were still no statistically significant differences in age, sex, main lesion size and stage, degree of differentiation, number of lesions, and pathological types between the two groups. On this basis, we compared the prognosis of patients with sMPLCs who underwent lobectomy and sublobar resection. The 1-year, 3-year, and 5-year DFS rates of the two groups were 93.9% vs. 98.0%, 84.4,% vs. 91.1%, and 67.6 vs. 87.7%, P = 0.324, and the 1-year, 3-year, and 5-year OS rates were 95.9% vs. 100%, 86.7% vs. 93.2%, and 86.7% vs. 83.9%, P = 0.482, indicating no statistically significant difference in the DFS rate and OS rate of the matched MPLC lesions regardless of sublobar resection or lobectomy. The possible reason is that the main lesion staging is caused by a larger proportion of stage 1 MPLC. As the number of cases increases, this result may change but for the main lesion stage 1 MPLC, and the choice of method is not a decisive factor affecting the prognosis.
At present, with the popularization of thoracic surgery techniques, the surgical method of sublobar resection, especially anatomical segment resection, is gradually becoming more mature [38]. At present, from a technical point of view, sublobar resection is safe and feasible to treat early invasive NSCLC [39]. In the current literature, 10% of these major complications reported in some prospective trials and large database analyses occur late. In a recently published randomized study [40] (CALGB/Alliance 140,503), the inpatient mortality after lobectomy for patients with suitable cardiopulmonary function was 1.1%, and the inpatient mortality after segmentectomy was 0.6%. This study found that the incidence rate of serious complications of sMPLCs such as pulmonary embolism (3/141, 2.1%), respiratory failure (1/141, 0.7%), but the more frequent occurrence is lung infection (24/141, 17.0%). Postoperative complications in the sublobar resection group (7 cases of respiratory infection, 0 case of respiratory failure, 1 case of pulmonary embolism) were significantly less than that of the lobectomy group (17 cases of respiratory infection, 1 case of respiratory failure, 2 cases of pulmonary embolism). There was no death during the perioperative period. In general, sublobar resection for sMPLCs has shorter hospital stays than lobectomy (9.72 ± 4.33 vs. 11.22 ± 5.35, P = 0.049) and a lower incidence of postoperative complications (16.3% vs. 40.8%, P = 0.007). We believe that the advantages of sublobar resection in the perioperative period are mainly because the wound area is smaller than that of lobectomy, and the exudation is less; at the same time, its perioperative complication rates were lower than that of lobectomy. Therefore, in patients with MPLCs, sublobar resection can be considered as an effective alternative to lobectomy in perioperative.
There is no statistically significant difference in the prognosis of sMPLCs, whether lobectomy or sublobar resection is selected for the main lesion, compared with the corresponding single primary lung cancer. The prognosis of sMPLCs generally depends only on the main lesion. This special form of lung cancer can be considered in the traditional TNM staging system according to the staging of the main lesion to predict the patient’s prognosis more accurately. The main focus of MPLC surgery can be selected according to the patient’s lung function. Sublobar resection or lobectomy, and sublobal treatment of sMPLC, is safer than lobectomy in the perioperative period and shorter postoperative hospital stay.
This study is a retrospective study of a single institution with a small sample size and a certain degree of bias. Due to the limitation of the sublobar resection entry criteria, the tumor diameter of the sublobar resection group is smaller than that of the lobectomy, older age, and more comorbidities, which are often incalculable confounding factors. Based on these factors, we tried our best to balance the confounding factors of tumor staging and tumor size by propensity matching analysis. We did not observe a difference in survival between the two groups. In addition, compared with lobectomy, sublobar resection has perioperative advantages such as shorter hospital stay and lower postoperative complications. Finally, it should be pointed out that the choice of surgical methods for MPLCs is still in the exploratory stage, and prospective studies are needed to further verify these observations.
Availability of data and materials
The data used to support the findings of this study are included within the article.
References
Beyreuther H. Multiplicität von Carcinomen bei einem Fall von sog. “Schneeberger” Lungenkrebs mit Tuberkulose. Virchows Archiv für pathologische Anatomie und Physiologie und für klinische Medizin. 1924;250(1):230–43.
Warth A, Macher-Goeppinger S, Muley T, Thomas M, Hoffmann H, Schnabel PA, et al. Clonality of multifocal nonsmall cell lung cancer: implications for staging and therapy. Eur Respir J. 2012;39(6):1437–42.
Henschke CI, Yankelevitz DF, Libby DM, Pasmantier MW, Smith JP, Miettinen OS. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med. 2006;355(17):1763–71.
Ryerson AB, Eheman CR, Altekruse SF, Ward JW, Jemal A, Sherman RL, et al. Annual Report to the Nation on the Status of Cancer, 1975–2012, featuring the increasing incidence of liver cancer. Cancer. 2016;122(9):1312–37.
Nakata M, Sawada S, Yamashita M, Saeki H, Kurita A, Takashima S, et al. Surgical treatments for multiple primary adenocarcinoma of the lung. Ann Thorac Surg. 2004;78(4):1194–9.
Goldstraw PJHoTSiLC. IASLC staging manual in thoracic oncology. 2009.
Fonseca A, Detterbeck FC. How many names for a rose: inconsistent classification of multiple foci of lung cancer due to ambiguous rules. Lung Cancer. 2014;85(1):7–11.
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th Edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–4.
Wittekind CJWJS. TNM supplement. 2012.
Yu YC, Hsu PK, Yeh YC, Huang CS, Hsieh CC, Chou TY, et al. Surgical results of synchronous multiple primary lung cancers: similar to the stage-matched solitary primary lung cancers? Ann Thorac Surg. 2013;96(6):1966–74.
Martini N, Melamed MR. Multiple primary lung cancers. J Thoracic Cardiovasc Surg. 1975;70(4):606–12.
Guo H, Mao F, Zhang H, Qiu Y, Shen-Tu Y. Analysis on the prognostic and survival factors of synchronous multiple primary lung cancer. Zhongguo Fei Ai Za Zhi. 2017;20(1):21–7.
Trousse D, Barlesi F, Loundou A, Tasei AM, Doddoli C, Giudicelli R, et al. Synchronous multiple primary lung cancer: an increasing clinical occurrence requiring multidisciplinary management. J Thorac Cardiovasc Surg. 2007;133(5):1193–200.
Chang YL, Wu CT, Lee YC. Surgical treatment of synchronous multiple primary lung cancers: experience of 92 patients. J Thorac Cardiovasc Surg. 2007;134(3):630–7.
Rostad H, Strand TE, Naalsund A, Norstein J. Resected synchronous primary malignant lung tumors: a population-based study. Ann Thorac Surg. 2008;85(1):204–9.
Kozower BD, Larner JM, Detterbeck FC, Jones DR. Special treatment issues in non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e369S – e399.
Liu Y, Tang Y, Xue Z, Yang P, Ma K, Ma G, et al. Ratio of lymph node to primary tumor SUVmax multiplied by maximal tumor diameter on positron emission tomography/integrated computed tomography may be a predictor of mediastinal lymph node malignancy in lung cancer. Medicine. 2016;95(46):e5457.
Ishikawa Y, Nakayama H, Ito H, Yokose T, Tsuboi M, Nishii T, et al. Surgical treatment for synchronous primary lung adenocarcinomas. Ann Thorac Surg. 2014;98(6):1983–8.
Ishigaki T, Yoshimasu T, Oura S, Ota F, Nakamura R, Hirai Y, et al. Surgical treatment for metachronous second primary lung cancer after radical resection of primary lung cancer. Ann Thorac Cardiovasc Surg. 2013;19(5):341–4.
Dang HH, Ta HDK, Nguyen TTT, Anuraga G, Wang CY, Lee KH, et al. Prospective role and immunotherapeutic targets of sideroflexin protein family in lung adenocarcinoma: evidence from bioinformatics validation. Funct Integr Genomics. 2022;22(5):1057–72.
Liu B, Song Z, Fan Y, Zhang G, Cao P, Li D, et al. Downregulation of FPN1 acts as a prognostic biomarker associated with immune infiltration in lung cancer. Aging (Albany NY). 2021;13(6):8737–61.
Le VH, Kha QH, Hung TNK, Le NQK. Risk score generated from CT-based radiomics signatures for overall survival prediction in non-small cell lung cancer. Cancers (Basel). 2021;13(14):3616.
Rosengart TK, Martini N, Ghosn P, Burt M. Multiple primary lung carcinomas: prognosis and treatment. Ann Thorac Surg. 1991;52(4):773–8 discussion 8-9.
Adebonojo SA, Moritz DM, Danby CA. The results of modern surgical therapy for multiple primary lung cancers. Chest. 1997;112(3):693–701.
Voltolini L, Paladini P, Luzzi L, Ghiribelli C, Di Bisceglie M, Gotti G. Iterative surgical resections for local recurrent and second primary bronchogenic carcinoma. Eur J Cardiothorac Surg. 2000;18(5):529–34.
Asaph JW, Keppel JF, Handy JR Jr, Douville EC, Tsen AC, Ott GY. Surgery for second lung cancers. Chest. 2000;118(6):1621–5.
van Rens MT, Zanen P, de la Rivière AB, Elbers HR, van Swieten HA, van den Bosch JM. Survival after resection of metachronous non-small cell lung cancer in 127 patients. Ann Thorac Surg. 2001;71(1):309–13.
Rea F, Zuin A, Callegaro D, Bortolotti L, Guanella G, Sartori F. Surgical results for multiple primary lung cancers. Eur J Cardiothorac Surg. 2001;20(3):489–95.
Aziz TM, Saad RA, Glasser J, Jilaihawi AN, Prakash D. The management of second primary lung cancers. A single centre experience in 15 years. Eur J Cardiothorac Surg. 2002;21(3):527–33.
Landreneau RJ, Normolle DP, Christie NA, Awais O, Wizorek JJ, Abbas G, et al. Recurrence and survival outcomes after anatomic segmentectomy versus lobectomy for clinical stage I non-small-cell lung cancer: a propensity-matched analysis. J Clin Oncol. 2014;32(23):2449–55.
Tsutani Y, Tsubokawa N, Ito M, Misumi K, Hanaki H, Miyata Y, et al. Postoperative complications and prognosis after lobar resection versus sublobar resection in elderly patients with clinical stage I non-small-cell lung cancer. 2017;53(2):366–71.
Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60(3):615–22.
Qu X, Wang K, Zhang T, Shen H, Dong W, Liu Q, et al. Long-term outcomes of stage I NSCLC (≤3 cm) patients following segmentectomy are equivalent to lobectomy under analogous extent of lymph node removal: a PSM based analysis. J Thorac Dis. 2017;9(11):4561–73.
Bott MJ, Patel AP, Crabtree TD, Colditz GA, Kreisel D, Krupnick AS, et al. Pathologic upstaging in patients undergoing resection for stage I non-small cell lung cancer: are there modifiable predictors? Ann Thorac Surg. 2015;100(6):2048–53.
Xue X, Xue Q, Wang N, Zhang L, Guo L, Li X, et al. Early clinical diagnosis of synchronous multiple primary lung cancer. Oncol Lett. 2012;3(1):234–7.
Yoshizawa A, Motoi N, Riely GJ, Sima CS, Gerald WL, Kris MG, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Modern Pathol. 2011;24(5):653–64.
Woo T, Okudela K, Mitsui H, Tajiri M, Yamamoto T, Rino Y, et al. Prognostic value of the IASLC/ATS/ERS classification of lung adenocarcinoma in stage I disease of Japanese cases. Pathol Int. 2012;62(12):785–91.
Lex JR, Naidu B. In patients with resectable non-small-cell lung cancer, is video-assisted thoracoscopic segmentectomy an appropriate alternative to video-assisted thoracoscopic lobectomy? Interact Cardiovasc Thorac Surg. 2016;23(5):826–31.
Novellis P, Bottoni E, Voulaz E, Cariboni U, Testori A, Bertolaccini L, et al. Robotic surgery, video-assisted thoracic surgery, and open surgery for early stage lung cancer: comparison of costs and outcomes at a single institute. J Thorac Dis. 2018;10(2):790–8.
Altorki NK, Wang X, Wigle D, Gu L, Darling G, Ashrafi AS, et al. Perioperative mortality and morbidity after sublobar versus lobar resection for early-stage non-small-cell lung cancer: post-hoc analysis of an international, randomised, phase 3 trial (CALGB/Alliance 140503). Lancet Respir Med. 2018;6(12):915–24.
Acknowledgements
Not applicable
Funding
This study was supported by the program of Jiaxing Science and Technology Bureau (2017AY33007), Zhejiang Province Medical and Health Technology (2021KY1016), and Jiaxing Key Discipline of Medicine—Thoracic Surgery (Supporting Subject: 2019-ZC-10).
Author information
Authors and Affiliations
Contributions
Conception and design: Niu Niu and Weibo Qi. Collection and assembly of data: Liang Zhou and Junjie Zhao. Data analysis and interpretation: Xingjie Ma and Fan Yang. Manuscript drafting: Niu Niu. Reviewing and editing: Weibo Qi. Final approval of manuscript: All authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study protocol was reviewed and approved by the Ethics Committee of Jiaxing First Hospital, approval number 2016–072.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Niu, N., Zhou, L., Zhao, J. et al. Sublobar resection versus lobectomy in the treatment of synchronous multiple primary lung cancer. World J Surg Onc 21, 135 (2023). https://doi.org/10.1186/s12957-023-02996-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-023-02996-w