
Abstract
Background
We retrospectively examined the relationship among skeletal muscle mass index (SMI), prognosis, and chemotherapy side effects in patients with recurrent gastric cancer (RGC).
Methods
Sixty-seven patients who developed recurrence after undergoing curative gastrectomy for gastric cancer at Tottori University Hospital and received palliative chemotherapy were included in this study. Pretreatment computed tomography was performed to measure the skeletal muscle mass (SMM) and cross-sectional SMM at the third lumbar vertebra. We focused on haematologic toxicity (neutropenia, thrombocytopenia, and anaemia), febrile neutropenia, and gastrointestinal toxicity (diarrhoea, vomiting, and stomatitis) as the side effects of chemotherapy.
Results
Median SMIs for males and females (43.9 and 34.7 cm2/m2, respectively) were used as cutoff values. The patients were classified into high (SMIHigh; n = 34) and low SMI groups (SMILow; n = 33). The SMILow group included more patients treated with monotherapy (P = 0.016) compared with the SMIHigh group, had a significantly lower number of chemotherapy lines (P = 0.049), and had a significantly higher incidence of grade 3 or 4 side effects (P = 0.010). The median survival rate was significantly higher in the SMIHigh group (17.8 vs 15.8 months; P = 0.034). In the univariate analysis, body mass index, SMI, histological type, and prognostic nutritional index were identified as prognostic indicators. The multivariate analysis identified SMI (P = 0.037) and histological type (P = 0.028) as independent prognostic factors.
Conclusion
The incidence of grade 3 or 4 side effects was significantly higher in patients with SMILow RGC. SMI was a useful prognostic marker of RGC.
Similar content being viewed by others

Introduction
Gastric cancer remains the fourth most common cancer and the second leading cause of cancer-related death worldwide [1, 2]. Gastrectomy is the main treatment strategy for gastric cancer. However, patients with advanced gastric cancer often experience recurrence [3, 4]. Chemotherapy is the main treatment for recurrent gastric cancer (RGC). Despite the improvements in prognosis as well as survival outcomes in patients with RGC, the overall outcome remains poor [5, 6].
Sarcopenia is characterised by a loss of skeletal muscle mass (SMM) and has been widely reported to impair physical performance and survival in the elderly [7, 8]. The relationship between sarcopenia and prognosis has been reported in various cancers, including gastric cancer [9,10,11,12,13,14,15,16,17]. In patients with cancer, sarcopenia is more likely to develop due to increased protein catabolism, inflammatory reactions, metabolic abnormalities, and poor oral intake. Sarcopenia may be associated with cancer cachexia [18]. Cancer cachexia disturbs the regenerative ability of skeletal muscle [19]. Patients with advanced gastric cancer often receive perioperative chemotherapy and the side effects of chemotherapy can cause loss of SMM. In addition, patients experience weight loss after gastrectomy because of poor dietary intake, which leads to various postoperative disorders and SMM loss [20, 21].
At the time of recurrence after gastrectomy, treatment options are limited to chemotherapy or best supportive care, and chemotherapy is administered despite the decrease in SMM. Sarcopenia is reported to possibly influence the pharmacokinetics of chemotherapy, which could be associated with the adverse effects of chemotherapy in several cancers [22]. However, there are few reports on SMM and chemotherapy side effects in patients with RGC. Moreover, there are few reports on SMM and RGC prognosis at the time of recurrence.
In this study, we retrospectively examined the relationship among skeletal muscle index (SMI), prognosis, and side effects of chemotherapy in patients with RGC after undergoing gastrectomy.
Patients and methods
Patients
Between January 2008 and December 2019, 605 patients were pathologically diagnosed with gastric cancer and had undergone curative gastrectomy at Tottori University Hospital. Gastrectomy was performed with D2 lymph node dissection for advanced cancer and D1+ lymph node dissection for early gastric cancer. Patients with stage II or III gastric cancer underwent adjuvant chemotherapy according to the Japanese gastric cancer treatment guidelines [23]. Sixty-seven patients developed recurrence, received palliative chemotherapy, and were included in this study. All the patients received first-line chemotherapy 4 weeks after a computed tomography (CT) scan. Clinicopathological findings were determined according to the Japanese gastric cancer treatment guidelines [23]. Clinical data, including age, sex, histology, history of gastrectomy, and metastatic site at the time of recurrence, were collected from electronic medical records. The patients were followed up every 3 months to check for recurrence by performing blood tests, including those for tumour markers, and by physical examination after the operation. Moreover, CT was performed at least every 6 months after the operation. Recurrence patterns and causes of death were examined from clinical records, CT, and positron emission tomography–CT. A family inquiry was conducted for patients who were difficult to follow up.
Definition of SMI
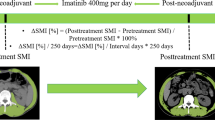
Pretreatment CT was performed to measure SMM and the SYNAPSE VINCENT system was used to measure the cross-sectional SMM at the level of the third lumbar vertebra (L3) [24]. The areas covered by SMM were calculated from pixels in the density range of − 29 to + 150 Hounsfield Units [25], which includes muscle and intra-abdominal organs but excludes bone and fat. The L3 region comprises the psoas, paraspinal, and abdominal wall muscles (Fig. 1). The skeletal muscle area in a single abdominal image is proportional to the whole-body muscle mass [26], and SMI is defined as the muscle area normalised by the square of the height (m2) [27].

Measurement of SMM in RGC patients. Axial computed tomography slice of the third lumbar vertebra (L3). Green areas indicate skeletal muscle mass. Abbreviations: RGC, recurrent gastric cancer; SMM, skeletal muscle mass
Details of first-line chemotherapy
The standard first-line palliative systemic chemotherapy was a fluoropyrimidine-, taxane-, or irinotecan-based regimen that was administered in accordance with the gastric cancer treatment guidelines for each decade [23, 28]. At the physician’s discretion, a single agent was used in patients with PS 2, those older than 80 years, or those who refused combined chemotherapy. In this study, monotherapy was administered in 23 patients and combination chemotherapy was administered in 44 patients. The monotherapy regimens included the following: (i) CPT-11 (n = 11), (ii) S-1 (n = 8), and (iii) paclitaxel (n = 4). The combination chemotherapy regimens were as follows: (iv) combined paclitaxel + ramucirumab (n = 11), (v) combined S-1 + cisplatin (n = 8), (vi) combined S-1 + docetaxel (n = 7), (vii) combined capecitabine + oxaliplatin (n = 5), (viii) combined S-1 + oxaliplatin (n = 4), (ix) combined capecitabine + cisplatin (n = 3), (x) combined S-1 + paclitaxel + intraperitoneally infused paclitaxel (n = 3), (xi) combined CPT-11 + cisplatin (n = 2), and (xii) combined capecitabine + trastuzumab (n = 1). Of the 67 patients who underwent chemotherapy for RGC, 55 patients (82.1%) received second-line chemotherapy.
Definition of side effect
The side effects of chemotherapy were graded according to the National Cancer Institute Common Toxicity Criteria, version 4.0 [29]. In this study, we examined the side effects observed during cycles 1–2 of first-line chemotherapy. If multiple side effects were observed, the higher grade was used in the present study. We specifically focused on haematologic toxicity (neutropenia, thrombocytopenia, and anaemia), febrile neutropenia (FN), and gastrointestinal toxicity (diarrhoea, vomiting, and stomatitis).
Statistical analysis
Continuous variables were expressed as means ± standard deviation and compared using the Mann–Whitney U test. The χ2 test or Fisher’s exact test was used to compare categorical variables. Survival curves were calculated using the Kaplan–Meier method, and differences between survival curves were examined using the log-rank test. The univariate and multivariate analyses of the prognostic factors of overall survival (OS) were performed using Cox’s proportional hazards model. P < 0.05 was considered significant, and all statistical analyses were performed using SPSS software (SPSS for Windows version 24; IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
The average SMI was 42.3 cm2/m2, and the median SMI for each sex (male, 43.9 cm2/m2; female, 34.7 cm2/m2) was used as cutoff values to classify patients into a high SMI group (SMIHigh group; n = 34) and a low SMI group (SMILow group; n = 33). The patients’ clinicopathological characteristics are shown in Table 1. Overall, there were 55 male and 12 female patients, and their average age was 67.6 years. The Eastern Cooperative Oncology Group performance status (ECOG PS) of 59 and 8 patients was 0–1 and 2, respectively. Details of the initial surgery showed that 8 patients had stage I disease, 20 had stage II disease, and 39 had stage III disease. The most common metastatic site was the peritoneum, followed by the haematogenous site and lymph nodes. Regarding histology, 36 patients had a differentiated-type carcinoma and 31 had an undifferentiated-type carcinoma. The relationships between SMI and clinicopathological variables of the patients are shown in Table 1, and the relationships between SMI and characteristics of initial surgery of the patients are shown in Table 2. Body mass index (BMI) was significantly higher in patients in the SMIHigh group than in the SMILow group (P < 0.001). The number of chemotherapy lines was significantly lower in the SMILow group than in the SMIHigh group (P = 0.049). No significant differences were observed with respect to age, sex, ECOG PS, adjuvant chemotherapy, prognostic nutritional index (PNI), metastatic site, tumour size, tumour invasion depth, lymph node metastasis, histological type, lymphatic invasion, venous invasion, pathological stage, tumour size, and gastrectomy type.
Details of first-line chemotherapy and side effects
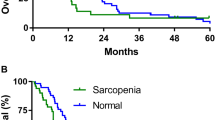
The details of SMI and first-line chemotherapy are presented in Table 3. The SMILow group included more patients treated with monotherapy compared with the SMIHigh group (P = 0.016). The details of SMI and side effects are presented in Table 4. The incidence of all side effects of grade 3 or 4 was significantly higher in the SMILow group than in the SMIHigh group (P = 0.010). The incidence of grade 3 or 4 gastrointestinal toxicity was significantly higher in the SMILow group than in the SMIHigh group (P = 0.018). No significant differences were observed in terms of neutropenia, anaemia, thrombocytopenia, and FN. In patients receiving monotherapy, the incidence of grade 3 or 4 gastrointestinal toxicity tended to be higher in the SMILow group than in the SMIHigh group (P = 0.106, Table 5). In patients receiving combined chemotherapy, the incidence of grade 3 or 4 gastrointestinal toxicity was significantly higher in the SMILow group than in the SMIHigh group (P = 0.011, Table 5). The median survival rate was significantly higher in the SMIHigh group than in the SMILow group (17.8 vs 15.8 months; P = 0.034, Fig. 2).

Overall survival curves according to SMI in patients with RGC. Abbreviations: RGC, recurrent gastric cancer; SMIHigh, high skeletal muscle mass; SMILow, low skeletal muscle mass
Univariate and multivariate analyses of patients with RGC
We performed a univariate analysis of the clinicopathological factors considered prognostic for OS in patients with RGC. In the univariate analysis, BMI, SMI, histological type, and PNI were identified as prognostic indicators (Table 6). In the multivariate analysis, we included significant parameters that were identified in the univariate analysis. The multivariate analysis revealed that SMI and histological type were independent prognostic factors (Table 6).
Discussion
In this study, the SMILow group had significantly more grade 3 or 4 side effects than the SMIHigh group, even though the SMILow group underwent less monotherapy than the SMIHigh group. The SMILow group had a significantly worse prognosis and significantly less conversion to second-line chemotherapy than the SMIHigh group.
Moreover, SMILow in patients with RGC was associated with grade 3 or 4 gastrointestinal side effects; this result was similar to that of a previous report by Carla et al. [30], where the side effects in 55 patients with metastatic breast cancer receiving capecitabine treatment were retrospectively reviewed. The cross-sectional skeletal muscle area at the third lumbar vertebra was measured using CT, and sarcopenia was defined using a previously published cutoff point. Consequently, sarcopenia was found to be associated with grade 3–4 diarrhoea and stomatitis. Shachar et al. also reported that they retrospectively reviewed side effects in 40 patients with metastatic breast cancer and showed that SMILow was associated with grade 3–4 toxicity [31]. Likewise, Tan et al. reported that sarcopenia was associated with dose-limiting toxicity in 89 patients with oesophagogastric cancer undergoing neoadjuvant chemotherapy [32]. Their multivariate analysis revealed that only sarcopenia was an independent risk factor of dose-limiting toxicity. These results show that SMILow is related to the high-grade toxicity of chemotherapy. However, the mechanism associating SMILow and toxicity is unclear. One possible explanation is that changes in body composition are related to alterations in the distribution and clearance of the anticancer agent [32]. 5-FU, a key drug in gastric cancer, is hydrophilic but widely distributed through active transport [33]. This drug undergoes extensive metabolism, primarily through dihydropyrimidine dehydrogenase. Variants of dihydropyrimidine dehydrogenase have been associated with an increased risk of 5-FU toxicity [34]. The clearance of 5-FU is increased in individuals with higher SMM [35]. These findings suggest that decreased clearance of 5-FU due to SMILow may be related to the increased side effects. To the best of our knowledge, this is the first report in which SMILow was associated with grade 3 or 4 side effects in patients with RGC.
Sarcopenia has been shown to negatively impact long-term outcomes of patients with several cancer types [11, 36, 37]. However, only a few studies have investigated the effect of sarcopenia on the prognosis of patients with RGC. Willemieke et al. retrospectively reviewed the prognosis of 88 patients with advanced oesophagogastric cancer treated with standard first-line palliative chemotherapy. They showed that the survival rate was not different between patients with and without sarcopenia in univariate and multivariate analyses. The cutoff in this study was set based on the presence or absence of sarcopenia, which is different from our cutoff, and may have caused the discrepancy. By contrast, Kouzu et al. concluded that sarcopenia was a poor prognostic factor after gastric cancer recurrence. They retrospectively reviewed 67 patients who experienced gastric cancer recurrence and found that sarcopenia was an independent negative prognostic factor in a multivariate analysis, which is similar to our result. They calculated the psoas muscle index (PMI) and used a receiver operating characteristic curve to determine the cutoff PMI. These results suggest that SMILow may be associated with prognosis, although there are problems with SMI evaluation and setting of the cutoff values.
The reason for the poor prognosis of patients with SMILow RGC has not been sufficiently elucidated. One potential explanation is that these patients were less likely to receive second-line chemotherapy. The first choice of treatment for patients with metastatic gastric cancer is chemotherapy, and patients need to undergo second- and third-line chemotherapy for further improvement of treatment outcomes [38,39,40]. In this study, the rate of second-line chemotherapy was significantly lower in the SMILow group than in the SMIHigh group, which might have led to the poor prognosis in the SMILow group.
The standard first-line palliative systemic chemotherapy is a combined regimen in accordance with the Japanese gastric cancer treatment guidelines [41]. However, SMILow in patients with RGC was associated with grade 3 or 4 side effects and the rate of second-line chemotherapy was significantly lower in the SMILow group than in the SMIHigh group. Gastrectomy causes not only weight loss but also SMM loss [21]. Preoperative nutritional and exercise interventions for gastric cancer may be useful in improving postoperative outcomes [42]. However, few reports have focused on the effects of postoperative nutritional or rehabilitative interventions on the postoperative development of sarcopenia and outcomes [43]. Postoperative nutritional management and regular exercise may be important for the maintenance of SMM and nutritional status at the time of gastric cancer recurrence in patients at a high risk of recurrence after gastrectomy. In addition, nutritional and rehabilitative interventions during chemotherapy to maintain SMM and nutritional status may be associated with decreased side effects and an increased rate of second-line chemotherapy administration.
This study has several limitations. First, we conducted this study in a single institution, and the number of patients who experienced postoperative recurrence was relatively small. Second, the optimal cutoff SMI value has not been determined in patients with RGC. Because postoperative patients with gastric cancer often have lower dietary intake, body weight, and SMM, and reports of SMM in patients with RGC are few, hence, the SMI median value of all patients was used as the cutoff value in this study. Third, the first-line chemotherapy was not unified. Although this was a long-term study and the guidelines changed over time, chemotherapy was administered in accordance with the guidelines at that time. Therefore, well-designed, randomised, prospective studies with larger populations are needed to confirm these findings.
In conclusion, patients with SMILow RGC had significantly more grade 3 or 4 side effects than those with SMIHigh, and SMI was a useful prognostic marker of RGC. In patients with advanced gastric cancer after gastrectomy with a high risk of recurrence, interventions to prevent the loss of SMM, such as nutritional therapy and regular exercise, might be needed to improve the prognosis in patients with RGC.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- ECOG PS:
-
Eastern Cooperative Oncology Group performance status
- FN:
-
Febrile neutropenia
- OS:
-
Overall survival
- PNI:
-
The prognostic nutritional index
- pN:
-
Pathological lymph node metastasis
- pStage:
-
Pathological stage
- pT:
-
Pathological depth of tumour invasion
- RGC:
-
Recurrent gastric cancer
- SMI:
-
Skeletal muscle mass index
- SMIHigh :
-
High skeletal muscle mass
- SMILow :
-
Low skeletal muscle mass
- SMM:
-
Skeletal muscle mass
References
Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancer transitions according to the Human Development Index (2008-2030): a population-based study. Lancet Oncol. 2012;13(8):790–801. https://doi.org/10.1016/S1470-2045(12)70211-5.
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86. https://doi.org/10.1002/ijc.29210.
Moon YW, Jeung HC, Rha SY, Yoo NC, Roh JK, Noh SH, et al. Changing patterns of prognosticators during 15-year follow-up of advanced gastric cancer after radical gastrectomy and adjuvant chemotherapy: a 15-year follow-up study at a single Korean institute. Ann Surg Oncol. 2007;14(10):2730–7. https://doi.org/10.1245/s10434-007-9479-4.
Zou ZH, Zhao LY, Mou TY, Hu YF, Yu J, Liu H, et al. Laparoscopic vs open D2 gastrectomy for locally advanced gastric cancer: a meta-analysis. World J Gastroenterol. 2014;20(44):16750–64. https://doi.org/10.3748/wjg.v20.i44.16750.
Koizumi W, Narahara H, Hara T, Takagane A, Akiya T, Takagi M, et al. S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): a phase III trial. Lancet Oncol. 2008;9(3):215–21. https://doi.org/10.1016/S1470-2045(08)70035-4.
Fuchs CS, Tomasek J, Yong CJ, Dumitru F, Passalacqua R, Goswami C, et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2014;383(9911):31–9. https://doi.org/10.1016/S0140-6736(13)61719-5.
Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. 2002;50(5):889–96. https://doi.org/10.1046/j.1532-5415.2002.50216.x.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412–23. https://doi.org/10.1093/ageing/afq034.
Kamarajah SK, Bundred J, Tan BHL. Body composition assessment and sarcopenia in patients with gastric cancer: a systematic review and meta-analysis. Gastric Cancer. 2019;22(1):10–22. https://doi.org/10.1007/s10120-018-0882-2.
Ubachs J, Ziemons J, Minis-Rutten IJG, Kruitwagen R, Kleijnen J, Lambrechts S, et al. Sarcopenia and ovarian cancer survival: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2019;10(6):1165–74. https://doi.org/10.1002/jcsm.12468.
Yang M, Shen Y, Tan L, Li W. Prognostic value of sarcopenia in lung cancer: a systematic review and meta-analysis. Chest. 2019;156(1):101–11. https://doi.org/10.1016/j.chest.2019.04.115.
Deng HY, Zha P, Peng L, Hou L, Huang KL, Li XY. Preoperative sarcopenia is a predictor of poor prognosis of esophageal cancer after esophagectomy: a comprehensive systematic review and meta-analysis. Dis Esophagus. 2019;32(3). https://doi.org/10.1093/dote/doy115.
Qian Y, Liu H, Pan J, Yu W, Lv J, Yan J, et al. Preoperative Controlling Nutritional Status (CONUT) score predicts short-term outcomes of patients with gastric cancer after laparoscopy-assisted radical gastrectomy. World J Surg Oncol. 2021;19(1):25. https://doi.org/10.1186/s12957-021-02132-6.
Lee CS, Won DD, Oh SN, Lee YS, Lee IK, Kim IH, et al. Prognostic role of pre-sarcopenia and body composition with long-term outcomes in obstructive colorectal cancer: a retrospective cohort study. World J Surg Oncol. 2020;18(1):230. https://doi.org/10.1186/s12957-020-02006-3.
Sakamoto T, Yagyu T, Uchinaka E, Miyatani K, Hanaki T, Kihara K, et al. Sarcopenia as a prognostic factor in patients with recurrent pancreatic cancer: a retrospective study. World J Surg Oncol. 2020;18(1):221. https://doi.org/10.1186/s12957-020-01981-x.
Maeda N, Shirakawa Y, Tanabe S, Sakurama K, Noma K, Fujiwara T. Skeletal muscle loss in the postoperative acute phase after esophageal cancer surgery as a new prognostic factor. World J Surg Oncol. 2020;18(1):143. https://doi.org/10.1186/s12957-020-01908-6.
Nakano Y, Hirata Y, Shimogawara T, Yamada T, Mihara K, Nishiyama R, et al. Frailty is a useful predictive marker of postoperative complications after pancreaticoduodenectomy. World J Surg Oncol. 2020;18(1):194. https://doi.org/10.1186/s12957-020-01969-7.
Peixoto da Silva S, Santos JMO, Costa ESMP, Gil da Costa RM, Medeiros R. Cancer cachexia and its pathophysiology: links with sarcopenia, anorexia and asthenia. J Cachexia Sarcopenia Muscle. 2020;11:619–35.
Inaba S, Hinohara A, Tachibana M, Tsujikawa K, Fukada SI. Muscle regeneration is disrupted by cancer cachexia without loss of muscle stem cell potential. PLoS One. 2018;13(10):e0205467. https://doi.org/10.1371/journal.pone.0205467.
Kanazawa Y, Yamada T, Kakinuma D, Matsuno K, Ando F, Fujita I, et al. Skeletal muscle mass depletion after gastrectomy negatively affects the prognosis of patients with gastric cancer. Anticancer Res. 2020;40(8):4271–9. https://doi.org/10.21873/anticanres.14429.
Yamazaki Y, Kanaji S, Takiguchi G, Urakawa N, Hasegawa H, Yamamoto M, et al. Skeletal muscle loss after laparoscopic gastrectomy assessed by measuring the total psoas area. Surg Today. 2020;50(7):693–702. https://doi.org/10.1007/s00595-019-01936-0.
Antoun S, Borget I, Lanoy E. Impact of sarcopenia on the prognosis and treatment toxicities in patients diagnosed with cancer. Curr Opin Support Palliat Care. 2013;7(4):383–9. https://doi.org/10.1097/SPC.0000000000000011.
Japanese Gastric Cancer Association: The Japanese Gastric Cancer Treatment Guidelines 2014 (version 4). Gastric Cancer. 2017;20(1):1–19. https://doi.org/10.1007/s10120-016-0622-4.
Harada K, Ida S, Baba Y, Ishimoto T, Kosumi K, Tokunaga R, et al. Prognostic and clinical impact of sarcopenia in esophageal squamous cell carcinoma. Dis Esophagus. 2016;29(6):627–33. https://doi.org/10.1111/dote.12381.
Mitsiopoulos N, Baumgartner RN, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol (1985). 1998;85:115–22.
Shen W, Punyanitya M, Wang Z, Gallagher D, St-Onge MP, Albu J, et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985). 2004;97:2333–8.
Martin L, Birdsell L, Macdonald N, Reiman T, Clandinin MT, McCargar LJ, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. 2013;31(12):1539–47. https://doi.org/10.1200/JCO.2012.45.2722.
Japanese Gastric Cancer Association: The Japanese Gastric Cancer Treatment Guidelines 2010 (version 3). Gastric Cancer. 2011;14(2):113–23. https://doi.org/10.1007/s10120-011-0042-4.
Basch E, Reeve BB, Mitchell SA, Clauser SB, Minasian LM, Dueck AC, et al. Development of the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106(9):dju244. https://doi.org/10.1093/jnci/dju244.
Prado CM, Baracos VE, McCargar LJ, Reiman T, Mourtzakis M, Tonkin K, et al. Sarcopenia as a determinant of chemotherapy toxicity and time to tumor progression in metastatic breast cancer patients receiving capecitabine treatment. Clin Cancer Res. 2009;15(8):2920–6. https://doi.org/10.1158/1078-0432.CCR-08-2242.
Shachar SS, Deal AM, Weinberg M, Nyrop KA, Williams GR, Nishijima TF, et al. Skeletal muscle measures as predictors of toxicity, hospitalization, and survival in patients with metastatic breast cancer receiving taxane-based chemotherapy. Clin Cancer Res. 2017;23(3):658–65. https://doi.org/10.1158/1078-0432.CCR-16-0940.
Tan BH, Brammer K, Randhawa N, Welch NT, Parsons SL, James EJ, et al. Sarcopenia is associated with toxicity in patients undergoing neo-adjuvant chemotherapy for oesophago-gastric cancer. Eur J Surg Oncol. 2015;41(3):333–8. https://doi.org/10.1016/j.ejso.2014.11.040.
Nies AT, Magdy T, Schwab M, Zanger UM. Role of ABC transporters in fluoropyrimidine-based chemotherapy response. Adv Cancer Res. 2015;125:217–43. https://doi.org/10.1016/bs.acr.2014.10.007.
Caudle KE, Thorn CF, Klein TE, Swen JJ, McLeod HL, Diasio RB, et al. Clinical pharmacogenetics implementation consortium guidelines for dihydropyrimidine dehydrogenase genotype and fluoropyrimidine dosing. Clin Pharmacol Ther. 2013;94(6):640–5. https://doi.org/10.1038/clpt.2013.172.
Gusella M, Toso S, Ferrazzi E, Ferrari M, Padrini R. Relationships between body composition parameters and fluorouracil pharmacokinetics. Br J Clin Pharmacol. 2002;54(2):131–9. https://doi.org/10.1046/j.1365-2125.2002.01598.x.
Voron T, Tselikas L, Pietrasz D, Pigneur F, Laurent A, Compagnon P, et al. Sarcopenia impacts on short- and long-term results of hepatectomy for hepatocellular carcinoma. Ann Surg. 2015;261(6):1173–83. https://doi.org/10.1097/SLA.0000000000000743.
Lee JS, Kim YS, Kim EY, Jin W. Prognostic significance of CT-determined sarcopenia in patients with advanced gastric cancer. PLoS One. 2018;13(8):e0202700. https://doi.org/10.1371/journal.pone.0202700.
Takahari D. Second-line chemotherapy for patients with advanced gastric cancer. Gastric Cancer. 2017;20(3):395–406. https://doi.org/10.1007/s10120-017-0707-8.
Hironaka S, Ueda S, Yasui H, Nishina T, Tsuda M, Tsumura T, et al. Randomized, open-label, phase III study comparing irinotecan with paclitaxel in patients with advanced gastric cancer without severe peritoneal metastasis after failure of prior combination chemotherapy using fluoropyrimidine plus platinum: WJOG 4007 trial. J Clin Oncol. 2013;31(35):4438–44. https://doi.org/10.1200/JCO.2012.48.5805.
Ford HE, Marshall A, Bridgewater JA, Janowitz T, Coxon FY, Wadsley J, et al. Docetaxel versus active symptom control for refractory oesophagogastric adenocarcinoma (COUGAR-02): an open-label, phase 3 randomised controlled trial. Lancet Oncol. 2014;15(1):78–86. https://doi.org/10.1016/S1470-2045(13)70549-7.
Japanese Gastric Cancer Association: The Japanese Gastric Cancer Treatment Guidelines 2018 (version 5). Gastric Cancer. 2017;24:1–21. https://doi.org/10.1007/s10120-020-01042-y.
Yamamoto K, Nagatsuma Y, Fukuda Y, Hirao M, Nishikawa K, Miyamoto A, et al. Effectiveness of a preoperative exercise and nutritional support program for elderly sarcopenic patients with gastric cancer. Gastric Cancer. 2017;20(5):913–8. https://doi.org/10.1007/s10120-016-0683-4.
Kimura Y, Nishikawa K, Kishi K, Inoue K, Matsuyama J, Akamaru Y, et al. Long-term effects of an oral elemental nutritional supplement on post-gastrectomy body weight loss in gastric cancer patients (KSES002). Ann Gastroenterol Surg. 2019;3(6):648–56. https://doi.org/10.1002/ags3.12290.
Acknowledgements
We thank Enago Group for editing a draft of this manuscript.
Funding
The authors have no financial support to declare.
Author information
Authors and Affiliations
Contributions
Study conception: TM; study design: TM; data acquisition: WM, YS, KM, YM, TH, and KK; quality control of data and algorithms: MY and NT; data analysis and interpretation: ST, TS, and TH; statistical analysis: TM; manuscript preparation: TM; manuscript editing: HS; manuscript review: YF; final approval of the article: all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional review board of ethics committee and national research committee with the 1964 Helsinki Declaration and its later amendments. The institutional review board of our institution approved the study (Tottori University, number 18A154). The informed consent requirement was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Matsunaga, T., Satio, H., Miyauchi, W. et al. Impact of skeletal muscle mass in patients with recurrent gastric cancer. World J Surg Onc 19, 170 (2021). https://doi.org/10.1186/s12957-021-02283-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-021-02283-6