
Abstract
Background
During the transitional phase from childhood to adulthood, adolescents encounter many changes and challenges. Stress is associated with reduced health-related quality of life (HRQOL) in adolescents and, thus, impacts all aspects of their life. Adolescents’ thoughts and beliefs in their capacity may be essential with regard to their subjective perception of stress and coping with it. Insights into the complexity of stress and exploration of the possible underlying mechanisms in adolescence are needed. We sought to describe stress, HRQOL, and self-efficacy and explore the association between stress and HRQOL by testing for self-efficacy as a possible mediator in adolescents.
Methods
In total, 696 school-based adolescents aged 14–15 years participated in this study. Participants were recruited from 22 schools in the Eastern and Southern parts of Norway. All participants completed an electronic survey in their respective classrooms. The survey included demographic data, the Perceived Stress Questionnaire, the KIDSCREEN-27 questionnaire measuring HRQOL, and the General Perceived Self-Efficacy Scale. Statistical analyses were conducted using the PROCESS macro for SPSS Statistics software by Andrew Hayes model 4.
Results
Descriptive analyses revealed overall low levels of stress with a score of 0.29 (SD, 0.15). Nevertheless, stress was negatively associated with all HRQOL subscales: physical well-being (B = − 25.60), psychological well-being (B = − 38.43), autonomy and parents (B = − 28.84), social support and peers (B = − 21.05), and school environment (B = − 30.28). Furthermore, these respective associations were all mediated by self-efficacy, which explained approximately one-fifth of the reduction in HRQOL. The highest degree of mediation and, thus, the largest indirect effect was estimated for the HRQOL subscale physical well-being (31.7%).
Conclusions
Our findings extend prior research on the mechanisms underlying the relationship between perceived stress and HRQOL in adolescents. They demonstrated that perceived stress explained most of the reduction in the HRQOL after adjusting for the effect of self-efficacy. Hence, stress itself appears to be an important target for future interventions to enhance HRQOL, rather than purely focusing on increasing self-efficacy to enhance the HRQOL in adolescents. Our findings highlight the importance of a better understanding of the underlying mechanisms to develop strategic and accurate interventions for adolescents.
Similar content being viewed by others

Background
During the transitional phase from childhood to adulthood, adolescents may encounter many stressful changes and challenges concomitantly. The drive for independence and greater autonomy, brain development, pressure to conform to peers, exploration of sexual identity, physical development, and increased access to and use of technology have been suggested as important factors in this time period [1, 2]. Moreover, perceived stress in adolescence may be related to different expectations and general high demands of being successful in many aspects of life, such as school, social media, and peer relations [3]. Hence, adolescence is often defined as a period of heightened stress [4]. According to Lazarus and Folkman, stress is defined as a relationship between the person and their environment that is appraised by the person as taxing or exceeding their resources and as endangering their well-being [5]. Previous stress experiences may predict the stress response and coping in adolescents. The rate of perceived stress experiences among adolescents in modern society is reported to be high (up to 50%) [6], and the stress levels among adolescents are even higher than those in adults [7]. Furthermore, perceived stress and maladaptive coping are reported to be positively associated with adjustment problems in adolescence [8].
According to the World Health Organization’s Mental Health Action Plan, coping with the normal stressors of life enables adolescents to reach their potential [9]. However, the Action Plan highlights that some adolescents have a greater risk of stressful health conditions because of their living conditions, discrimination, stigma, or a lack of access to quality support and services [9]. Norwegian adolescents are likely to possess advantageous prerequisites in terms of living conditions and access to quality support and services compared with adolescents living in other countries. However, the Ungdata, which is a Norwegian national data collection scheme targeted at the youth, showed that approximately half of the Norwegian adolescents in high schools reported having concerns such as “everything feels like a struggle” or feeling like they were “worrying too much” [6]. The survey was conducted almost every year among Norwegian adolescents aged 14–19 years and has since 2010 shown an increase in perceived stress, especially among girls [6]. For instance, two-thirds of the Norwegian girls and one-third of the Norwegian boys reported being often or very often stressed by schoolwork [10].
Given that stress has an impact on healthy behaviors and may influence all aspects of life, the concept of health-related quality of life (HRQOL) is of relevance because it is defined as a multidimensional concept, which is used to assess the adolescents’ subjective well-being in terms of physical, psychological, social, and spiritual aspects of life [11]. The multidimensionality of HRQOL can provide important information about the impact of stress on different aspects of life, and it may serve as a framework for identifying and developing strategies to improve HRQOL [12]. Several studies have reported that stress symptoms are associated with a low HRQOL [13,14,15]. Nevertheless, a complex situation involving several factors and strong correlations between the HRQOL dimensions and interacting psychological health variables exists [16], which indicates the need to further explore these associations in school-based populations of adolescents.
The determinants of stress include not only social, cultural, and economic factors but also individual attributes, such as the ability to manage own thoughts and emotions [17]. Thus, adolescents’ thoughts and cognition may be essential in terms of the subjective perception of stress. According to Albert Bandura, self-efficacy might act as a mediator between stress experiences and outcomes, such as well-being [18]. A mediator seeks to identify causal-based mechanisms underlying the observed associations of an exploratory nature [19]. A well-known potential mediator is self-efficacy. Because self-efficacy refers to a person’s thoughts and cognition, it may act as a third interacting variable between the observed associations [18]. Bandura defined self-efficacy as “one’s beliefs (cognition) in one’s capability to organize and execute the courses of action required to achieve given results” [20, 21]. General self-efficacy (GSE) has been shown to positively impact HRQOL by reducing stress, and therefore, it increases the HRQOL in adult patients [22, 23]. Moreover, higher degrees of self-efficacy are shown to be related to higher HRQOL scores in adolescents [24]. Self-efficacy was recently revealed as a mediator in the relationship between pain and HRQOL in a school-based sample of Norwegian adolescents [25]. Although several factors may influence the HRQOL in adolescence, highlighting stress as a potential exponential cause and testing for self-efficacy as a mediator appears to be highly relevant for understanding the underlying mechanisms in adolescence.
Thus, the purpose of this study was to describe stress, HRQOL, and GSE in a school-based population of Norwegian adolescents and explore the possible associations between stress and HRQOL by testing GSE as a possible mediator. We hypothesized that stress is negatively associated with HRQOL and that self-efficacy would play a role as a mediator for the associations between stress and HRQOL.
Methods
Design
This cross-sectional study was a part of the “Start Young—quality of life and pain in generations” study, which is a longitudinal study aimed at acquiring new knowledge about HRQOL and pain in adolescents and their parents [26]. The present study used data collected at baseline from November 2018 to April 2019.
Study setting
A total of 59 elementary schools from the south-eastern part of Norway were invited to participate. Twenty-two schools agreed to participate. The schools varied in size and localization (from city to suburb), admitting adolescents with different sociocultural and economic backgrounds. The potential study participants consisted of 1663 adolescents in the 9th grade from the participating schools, of whom 696 finally participated in the study (response rate, 41.8%). The response rate varied across schools from 92.1 to 8.6%.
Study procedures
Project members visited each school approximately 1 week before the data collection to provide the adolescents with verbal and written information about the study. Written information was also distributed to the parents. Informed consent was obtained from both adolescents and their parents. A web-based questionnaire was administered and completed in the classrooms during school hours. The schools provided the adolescents with computers to complete the questionnaire. One or two project members and a teacher were present to provide assistance when needed. The collected data was stored in a safe data server.
The “Start Young” study was reviewed by the Norwegian Centre for Research Data (Reference Number: 60981), and the necessary approvals were obtained.
Measures
Demographic variables
The baseline questionnaire included questions regarding demographic data, including gender, age, parental status, living conditions, and ethnicity. Parental status and living conditions were used as indicators of the family resources and environment. Furthermore, the baseline questionnaire included the following study variables: stress (independent variable), HRQOL (dependent variable), and GSE (mediator variable).
Questionnaires
HRQOL
To assess HRQOL, the Norwegian version of the KIDSCREEN-27 questionnaire was used [27]. This questionnaire is considered a valid and reliable multidimensional measure of HRQOL in adolescents and is organized into the following five subscales: (1) physical well-being, (2) psychological well-being, (3) autonomy and parents, (4) social support and peers, and (5) school environment [28,29,30,31]. The KIDSCREEN instrument comprises a 5-point Likert scale (e.g., from “never” to “always”). Each subscale was transformed into Rasch-scores and had t-values with a mean of 50 and a standard deviation (SD) of 10 [32]. Higher values in the respective subscales indicate better HRQOL and well-being.
Self-efficacy
To assess self-efficacy, the Norwegian 10-item version of the General Perceived Self-Efficacy Scale revised and translated by Røysamb and colleagues was used [33]. This scale is considered a valid and reliable psychometric scale developed to identify a person’s optimistic self-belief and global confidence in one’s abilities across a wide range of challenging situations [34, 35]. It comprises 10 statements that the respondent rates on a scale from 1 (completely wrong) to 4 (completely right). The individual scores are then summed into a total score, wherein higher scores indicate higher levels of GSE.
Stress
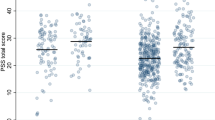
To assess stress, the Norwegian version of the Perceived Stress Questionnaire (PSQ) was used [36,37,38]. The PSQ comprises 30 items referring to the last 4 weeks and can be answered with a 4-point rating scale ranging from 1 (“almost never”) to 4 (“almost always”). The Norwegian version of the instrument has been shown to have good reliability and validity [38, 39]. Higher values indicate higher levels of perceived stress. The resulting PSQ total score is linearly transformed between 0 and 1; PSQ = (raw value − 30)/90 [36]. Commonly used cutoff levels of stress with respect to the PSQ are low, < 0.33; medium, 0.33–0.45; moderate, 0.45–0.60; and severe, > 0.60 [36, 37].
Statistical analyses
The statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Demographic data were described using descriptive measures. Continuous variables were described using mean and standard deviation, and categorical variables with frequencies and percentages. Linear regression analyses were conducted between the independent variable stress and dependent variables HRQOL and GSE. Mediation analysis was conducted using the PROCESS macro model 4 for SPSS by Andrew Hayes [19] and the model was controlled for gender, ethnicity, parental status, and living conditions. To increase precision, all the estimates were calculated using bootstrapping. The mediation effect was regarded as statistically significant if the 95% confidence interval (CI) for this effect did not include 0. Finally, both the indirect and direct effects were each divided by the total effect, multiplied by 100 and, thus, presented as percentages. p-values < 0.05 were considered statistically significant and all tests were two-sided. We used a simple mediation model presented in Fig. 1.

Illustration of the simple mediation model
Results
Participants
In total, 696 school-based adolescents (more girls [57.5%] than boys [42.5%]) participated in this study. The participants’ ages were 13 years (1.6%), 14 years (88.2%), and 15 years (10.2%). Most adolescents (79.1%) had parents who were born in Norway, 12.5% of the adolescents had one parent born in Norway, and 8.3% had both parents born in other countries.
Descriptive data of study variables: stress, HRQOL, and GSE
The mean level of stress for the total study sample was categorized as low with a score of 0.29 (SD, 0.15). Girls reported a higher mean stress level (0.33 [SD, 0.16]), which lies on the cutoff level between low and medium levels, than boys (0.24 [SD, 0.14]). The study sample had a mean GSE of 31.08 (SD, 4.31). Girls had a lower mean GSE (30.25 [SD, 4.27]) than boys (32.21 [SD, 1.9]). Boys had higher scores in the HRQOL subscales than girls (Table 1). The largest gender difference in mean was observed for the HRQOL subscale psychological well-being, wherein girls and boys had a mean score of 44.46 (SD, 8.02) and 49.52 (SD, 8.08), respectively.
Associations between stress, HRQOL subscales, and GSE
Stress was negatively and statistically significantly associated with all HRQOL subscales and GSE (Table 2, all p < 0.01): physical well-being (B = − 25.60), psychological well-being (B = − 38.43), autonomy and parents (B = − 28.84), social support and peers (B = − 21.05), school environment (B = − 30.28), and GSE (B = − 12.97).
In Table 3, findings from the linear regressions of GSE on the HRQOL subscales are listed. GSE was positively associated with all respective HRQOL subscales. The HRQOL subscale social support and peers revealed the largest regression coefficient (B = 2.31).
Mediation effect of self-efficacy on the relationship between stress and HRQOL subscales
The mediation effect was assessed using the PROCESS macro [41]. After controlling for gender, ethnicity, parental marital status, and living conditions, a significant indirect effect was found for all selected HRQOL subscales (Fig. 2): physical well-being (95% CI [− 9.77 to − 4.81]), psychological well-being (95% CI [− 6.95 to − 3.75]), autonomy and parents (95% CI [− 6.45 to − 2.28]), social support and peers (95% CI [− 6.56 to − 2.44]), and school environment (95% CI [− 9.11 to − 5.08]).

Mediation effect of self-efficacy on the association between stress and HRQOL subscales (physical well-being, psychological well-being, autonomy and parents, social support and peers, and school environment). *p < 0.05, **p < 0.01, ***p < 0.001
Approximately one-fifth of the relationship between stress and HRQOL was explained by the mediating variable GSE. Our data revealed the lowest indirect effect (14.4%) for the HRQOL subscale psychological well-being, where the direct path of stress (C′ = − 30.9) explained the majority of the total path (C = − 36.1). The highest indirect effect (31.7%) was found for the HRQOL subscale physical well-being (Table 4). The estimates of regression coefficients are illustrated in Fig. 2.
Discussion
This study evaluated the stress, HRQOL, and GSE in a sample from a school-based population of Norwegian adolescents and explored the associations between stress and HRQOL by modeling GSE as a possible mediator. As hypothesized, stress was negatively associated with all HRQOL subscales and self-efficacy. Furthermore, our findings revealed an indirect effect of self-efficacy on the relationship between stress and all selected HRQOL subscales after controlling for possible confounders. The highest indirect effect of self-efficacy, which explained approximately one-third of the reduction in the association between stress and HRQOL, was observed for the subscale physical well-being.
Our descriptive findings revealed overall low levels of perceived stress in a school-based sample of Norwegian adolescents, which is an important finding because stress, especially high levels of stress, is known to negatively impact the adolescents’ everyday life [13, 14, 16]. Therefore, we believe that it is important to differentiate between common everyday struggles and various perceived stress levels causing maladaptive behaviors. Inconsistencies in findings of stress levels in adolescents might partly be explained by methodological assessments, such as differences in scoring, measurements, and cutoff levels, used to categorize the instruments. Because adolescence is a transition period, which naturally evokes worries and struggles [1], the high levels of everyday struggles reported in Norwegian school-based samples of adolescents appear to be rational [6, 10].
Our findings showed that girls experienced higher stress levels and reported both lower mean GSE and HRQOL scores than boys, which is in accordance with the literature [16, 40,41,42]. Gender differences in HRQOL are common for adolescents and are more pronounced in older than younger children [43]. Several studies reported a lower HRQOL and mean GSE for girls than boys in adolescence [25, 44, 45]. Interestingly, a Norwegian study revealed no significant difference between the decline in HRQOL for boys and girls during 3 years in high school [45]. Because the decline in HRQOL is comparable between the genders in late adolescence, this might imply that the gender difference increases most rapidly from early adolescence. Thus, further understanding of the underlying mechanisms and associations of HRQOL in this population is important.
Although our findings revealed low levels of perceived stress, a negative association was observed between stress and all HRQOL subscales and self-efficacy, wherein the strongest associations were found for the subscale psychological well-being. Nevertheless, the directions of predicative assumptions should be addressed because stress and psychological well-being might interact in the adolescent’s everyday life, as some individuals might experience a reduction in psychological well-being due to the experience of stress and demands that exceed their resources. Other individuals might experience higher levels of stress due to concerns regarding their psychological well-being. This implies that stress may probably act as a cause (predictor) and/or a symptom (outcome) in relation to several aspects of the adolescents’ lives, which illustrates the complexity of stress. Another interesting finding was the statistically significant association between self-efficacy and the respective HRQOL subscales, revealing GSE as a predictor for HRQOL. Although HRQOL is defined as a multidimensional concept, the generic measure of self-efficacy (GSE) appears from an isolated perspective to have great potential for targeted intervention strategies for all dimensions of the HRQOL.
Our overall findings indicated that approximately one-fifth of the association between stress and the HRQOL subscales was explained by the indirect effect of self-efficacy when controlled for possible confounders. Hence, strategic interventions aimed at increasing the HRQOL often focus on strengthening self-efficacy because it is shown to be an important determinant of HRQOL. However, because stress is assumed to be a predictive factor for HRQOL, the lowest indirect effect of GSE was found for the subscale psychological well-being. These findings indicated that the degree of self-efficacy may not have the potential to influence psychological well-being in adolescents as expected, because stress itself appears to be the primary predictor. The highest indirect effect, which explained approximately one-third of the reduction in the association between stress and HRQOL, was found for the subscale physical well-being, which is especially interesting. It is important to highlight that the HRQOL subscale physical well-being does not represent physical activity levels but is theorized as the subjective perception of the physical well-being of the person’s own beliefs and expectations [21]. Despite this, previous findings suggested that self-perception of physical activity and fitness is associated with lower psychosomatic health symptoms in adolescents [46]. Because self-efficacy is defined as the confidence in the ability to perform a particular task, it appears logical that the adolescents probably perceived a decline in their physical well-being when their stress levels increased. Moreover, previous findings in a school-based population of Norwegian adolescents with persistent pain, revealed that self-efficacy mediated the relationship between pain intensity and HRQOL, herein the largest indirect effect of 67.2% was estimated for the HRQOL subscale physical well-being [25]. Hence, it appears that several reasons and different stressors, such as pain intensity and stress make maintaining high beliefs of their own capacity a challenge for Norwegian adolescents in a school-based population, which seems to be increasing the barriers for their physical well-being.
Strengths and limitations
The mediation model in this study was built on assumptions of the current understanding of the research area. The assumptions and understandings were based on the empiric and research evidence provided by researchers within the field and aimed to provide new insights into the potential mechanisms underlying the relationship between perceived stress and HRQOL. Hence, we may only assume the direction of direct and indirect effects. Furthermore, because we only used cross-sectional data, we can only present associations revealed using our analyses and present evidence that confirmed our anticipated mediation model. However, no causal relationships could be identified. The mediation analysis was conducted using available and relevant possible confounders, such as gender and ethnicity. We did not have information regarding the parents’ education and/or salary indicating their socioeconomic status, which would be a more suitable covariate than parental status and living conditions. Thus, this should be considered a limitation of the present study. Another limitation is linked to the low overall response rate (41.8%) and the high variability of response rates across schools (from 92.1 to 8.6%). The response rate was lowest in two large schools in the east of Norway and highest in two small schools in the south of Norway, but due to General Data Protection Regulation laws, we could not collect information to assess whether the participants and nonparticipants nor the schools differed in any respect. However, in our sample, most adolescents had a parent with high education level and relatively high household income, which indicate that our findings may not be representative of Norwegian adolescents with a lower socioeconomic status. Our findings may only be generalized to a Norwegian school-based population of adolescents with a higher socioeconomic status. A clear strength of this study is that it had a comparatively large sample size in a research field where large studies are scarce. Because large study samples statistically affect the p-value, the present study provided clear estimates for clinical interpretation. Finally, the KIDSCREEN-27 questionnaire employed in this study used a 1-week recall period, which is considered an advantage for preventing recall bias [28, 47].
Clinical implications
Because self-efficacy is regarded as a self-regulatory mechanism that is possible to change, a natural intervention strategy from a clinical perspective should be the enhancement of self-efficacy when aiming to improve HRQOL in a school-based population of adolescents. However, our findings indicated that stress itself explained the majority of the reduction in its association with all HRQOL subscales, especially in the subscale of psychological well-being, and thus, the corresponding lowest indirect effect of GSE. Based on these findings, it is reasonable to assume that intervention strategies that solely focus on self-efficacy among school-based adolescents experiencing stress might have a reduced potential for improvement in HRQOL. For instance, for adolescents with persistent pain, wherein the alleviation of pain itself might be a challenge and thus, in that case, self-efficacy is a more appropriate intervention target to increase HRQOL than pain. Therefore, this leads to the question of how to optimize intervention strategies targeting stress itself. Moreover, health care personnel, staff, and teachers in schools should be aware of the negative impact stress appears to have on the HRQOL in a school-based population of adolescents.
Conclusions
Our findings extend prior research on the mechanisms underlying the relationship between perceived stress and HRQOL. Overall, the present study showed how important perceived stress is for adolescents with regard to all aspects of their HRQOL. As hypothesized, stress was negatively associated with all HRQOL subscales, and self-efficacy mediated these associations. Moreover, our findings revealed that perceived stress explained the majority of the reduction in HRQOL after testing for the mediating variable self-efficacy. Hence, for this study sample, stress itself appears to be an important target for future intervention to enhance HRQOL. Thus, such interventions should not purely focus on increasing self-efficacy to enhance HRQOL in adolescents. Our findings highlight the importance of a better understanding of the underlying mechanisms in adolescence to develop more strategic and accurate interventions.
Availability of data and materials
The datasets used and/or analyzed during the present study are not publicly available due to the General Data Protection Regulation laws but are available from the corresponding author on reasonable request and with permission from the Norwegian Centre for Research Data.
Abbreviations
- CI:
-
Confidence interval
- GSE:
-
General self-efficacy
- HRQOL:
-
Health-related quality of life
- PSQ:
-
Perceived Stress Questionnaire
- SD:
-
Standard deviation
References
Blakemore SJ. The social brain in adolescence. Nat Rev Neurosci. 2008;9(4):267–77.
Casey BJ, Giedd JN, Thomas KM. Structural and functional brain development and its relation to cognitive development. Biol Psychol. 2000;54(1):241–57.
Samdal O, Wold B, Harris A, Torsheim T. Stress and coping. Rapport by the Norwegian Directorate of Health, 2017. HEMIL-Center, University in Bergen(IS-2655).
Spear LP. The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev. 2000;24(4):417–63.
Lazarus RS, Folkman S. Cognitive theories of stress and the issue of circularity. In: Appley MH, Trumbull R, editors. Dynamics of stress. Boston: Springer; 1986. p. 63–80.
Bakken A. Ungdata. Nasjonale resultater 2018. NOVA Rapport 10/18, 2018. https://oda.oslomet.no/oda-xmlui/bitstream/handle/20.500.12199/5128/Ungdata-2018.%20Nasjonale%20resultater.pdf?sequence=1&isAllowed=y
Bethune S. Teen stress rivals that of adults. Monit Psychol. 2014;45(4):20.
Hampel P, Petermann F. Perceived stress, coping, and adjustment in adolescents. J Adolesc Health. 2006;38(4):409–15.
World Health Organization. Mental health action plan 2013–2020. Geneva: World Health Organization; 2013.
Sletten MA, Bakken A. Psykiske helseplager bland ungdom - Tidstrender og samfunnsmessige forklaringer. En kunnskapsoversikt og empirisk analyse NOVA, 2016. Notat 4/2016. https://oda.oslomet.no/oda-xmlui/bitstream/handle/20.500.12199/5203/Web-Utgave-Notat-4-16.pdf?sequence=1&isAllowed=y
Eiser C, Morse R. The measurement of quality of life in children: past and future perspectives. J Dev Behav Pediatr. 2001;22(4):248–56.
Otto C, Haller AC, Klasen F, Hölling H, Bullinger M, Ravens-Sieberer U, et al. Risk and protective factors of health-related quality of life in children and adolescents: results of the longitudinal BELLA study. PLoS ONE. 2017;12(12):e0190363.
Raknes S, Pallesen S, Himle JA, Bjaastad JF, Wergeland GJ, Hoffart A, et al. Quality of life in anxious adolescents. Child Adolesc Psychiatry Ment Health. 2017;11(1):33.
World Health Organization. Risks to mental health: an overview of vulnerabilities and risk factors. Geneva: World Health Organization; 2012.
Linde M, Gustavsson A, Stovner LJ, Steiner TJ, Barré J, Katsarava Z, et al. The cost of headache disorders in Europe: the Eurolight project. Eur J Neurol. 2012;19(5):703–11.
Gaspar T, Matos MG, Pais R, Jose L, Leal I, Ferreira A. Health-related quality of life in children and adolescents and associated factors. J Cognit Behav Psychother. 2009;9(1):33–48.
Kessler RC, Angermeyer M, Anthony JC, De Graaf RO, Demyttenaere K, Gasquet I, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry. 2007;6(3):168–76.
Bandura A. Self-efficacy: the exercise of control. 1997.
Hayes AF. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach. New York, NY: The Guilford Press. J Educ Meas. 2014;51(3):335–337.
Tsang SKM, Hui EKP, Law BCM. Self-efficacy as a positive youth development construct: a conceptual review. Sci World J. 2012;2012:452327.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Kreitler S, Peleg D, Ehrenfeld M. Stress, self-efficacy and quality of life in cancer patients. Psychooncology. 2007;16(4):329–41.
Börsbo B, Gerdle B, Peolsson M. Impact of the interaction between self-efficacy, symptoms and catastrophising on disability, quality of life and health in with chronic pain patients. Disabil Rehabil. 2010;32(17):1387–96.
Kvarme LG, Haraldstad K, Helseth S, Sørum R, Natvig GK. Associations between general self-efficacy and health-related quality of life among 12–13-year-old school children: a cross-sectional survey. Health Qual Life Outcomes. 2009;7(1):85.
Grasaas E, Helseth S, Fegran L, Stinson J, Småstuen M, Haraldstad K. Health-related quality of life in adolescents with persistent pain and the mediating role of self-efficacy: a cross-sectional study. Health Qual Life Outcomes. 2020;18(1):19.
Mikkelsen HT, Haraldstad K, Helseth S, Skarstein S, Småstuen MC, Rohde G. Health-related quality of life is strongly associated with self-efficacy, self-esteem, loneliness, and stress in 14–15-year-old adolescents: a cross-sectional study. Health Qual Life Outcomes. 2020;18(1):352.
Andersen JR, Natvig GK, Haraldstad K, Skrede T, Aadland E, Resaland GK. Psychometric properties of the Norwegian version of the Kidscreen-27 questionnaire. Health Qual Life Outcomes. 2016;14(1):58.
Ravens-Sieberer U, Erhart M, Wille N, Wetzel R, Nickel J, Bullinger M. Generic health-related quality-of-life assessment in children and adolescents. Pharmacoeconomics. 2006;24(12):1199–220.
Ravens-Sieberer U. The Kidscreen questionnaires: quality of life questionnaires for children and adolescents; handbook. Lengerich: Pabst Science Publishers; 2006.
Ravens-Sieberer U, Auquier P, Erhart M, Gosch A, Rajmil L, Bruil J, et al. The European KIDSCREEN approach to measure quality of life and well-being in children: development, current application, and future advances. Qual Life Res. 2014;23(3):791–803.
Robitail S, Ravens-Sieberer U, Simeoni MC, Rajmil L, Bruil J, Power M, et al. Testing the structural and cross-cultural validity of the KIDSCREEN-27 quality of life questionnaire. Qual Life Res. 2007;16(8):1335–45.
Ravens-Sieberer U, Auquier P, Erhart M, Gosch A, Rajmil L, Bruil J, et al. The KIDSCREEN-27 quality of life measure for children and adolescents: psychometric results from a cross-cultural survey in 13 European countries. Qual Life Res. 2007;16(8):1347–56.
Røysamb E, Schwarzer R, Jerusalem M. Norwegian version of the general perceived self-efficacy scale.Oslo: University of Oslo; 1998.
Schwarzer R, Baßler J, Kwiatek P, Schröder K, Zhang JX. The assessment of optimistic self-beliefs: comparison of the German, Spanish, and Chinese versions of the general self-efficacy scale. Appl Psychol. 1997;46:69–88.
Romppel M, Herrmann-Lingen C, Wachter R, Edelmann F, Düngen HD, Pieske B, et al. A short form of the General Self-Efficacy Scale (GSE-6): development, psychometric properties and validity in an intercultural non-clinical sample and a sample of patients at risk for heart failure. Psychosoc Med. 2013;10:Doc01.
Levenstein S, Prantera C, Varvo V, Scribano ML, Berto E, Luzi C, et al. Development of the Perceived Stress Questionnaire: a new tool for psychosomatic research. J Psychosom Res. 1993;37(1):19–32.
Kocalevent RD, Levenstein S, Fliege H, Schmid G, Hinz A, Brähler E, et al. Contribution to the construct validity of the Perceived Stress Questionnaire from a population-based survey. J Psychosom Res. 2007;63(1):71–81.
Østerås B, Sigmundsson H, Haga M. Psychometric properties of the perceived stress questionnaire (PSQ) in 15–16 years old Norwegian adolescents. Front Psychol. 2018;9:1850.
Østerås B, Sigmundsson H, Haga M. Physical fitness levels do not affect stress levels in a sample of Norwegian adolescents. Front Psychol. 2017;8:2176.
Bisegger C, Cloetta B, Von Bisegger U, Abel T, Ravens-Sieberer U. Health-related quality of life: gender differences in childhood and adolescence. Soz Praventivmed. 2005;50(5):281–91.
Meade T, Dowswell E. Health-related quality of life in a sample of Australian adolescents: gender and age comparison. Qual Life Res. 2015;24(12):2933–8.
Østerås B, Sigmundsson H, Haga M. Pain is prevalent among adolescents and equally related to stress across genders. Scand J Pain. 2016;12(1):100–7.
Michel G, Bisegger C, Fuhr DC, Abel T. Age and gender differences in health-related quality of life of children and adolescents in Europe: a multilevel analysis. Qual Life Res. 2009;18(9):1147–57.
Haraldstad K, Christophersen KA, Helseth S. Health-related quality of life and pain in children and adolescents: a school survey. BMC Pediatr. 2017;17(1):174.
Langeland IO, Sollesnes R, Nilsen RM, Almenning G, Langeland E. Examining boys’ and girls’ health-related quality of life from the first to the third year of upper secondary school: a prospective longitudinal study. Nurs Open. 2019;6(4):1606–14.
Baceviciene M, Jankauskiene R, Emeljanovas A. Self-perception of physical activity and fitness is related to lower psychosomatic health symptoms in adolescents with unhealthy lifestyles. BMC Public Health. 2019;19(1):980.
Haraldstad K, Christophersen KA, Eide H, Nativg GK, Helseth S. Health related quality of life in children and adolescents: reliability and validity of the Norwegian version of KIDSCREEN-52 questionnaire, a cross sectional study. Int J Nurs Stud. 2011;48(5):573–81.
Acknowledgements
We wish to thank all cooperating schools and participants for allowing us to use their data and contributing to this important research area.
Funding
All data from this study is part of a project financially supported by the Norwegian Ministry of Education and Research.
Author information
Authors and Affiliations
Contributions
KH, SH, SS, MCS, and GR developed the project protocol. HTM mainly conducted the participant recruitment process. EG made a substantial contribution to writing the manuscript and conducting the statistical analyses. All authors contributed to manuscript preparation and approved its final version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Start Young study was approved by the Norwegian Centre for Research Data (Reference number: 60981) and an ethics committee at the University of Agder, Norway. All participants and their parents/guardians provided consent to participate. All data were anonymized. All study procedures were performed in accordance with the 1964 Helsinki declaration for ethical standards in research.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Grasaas, E., Skarstein, S., Mikkelsen, H.T. et al. The relationship between stress and health-related quality of life and the mediating role of self-efficacy in Norwegian adolescents: a cross-sectional study. Health Qual Life Outcomes 20, 162 (2022). https://doi.org/10.1186/s12955-022-02075-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-022-02075-w