
Abstract
Objective
This study aimed to conduct a systematic review and meta-analysis to compare differences in health utilities (HUs) assessed by self and proxy respondents in children, as well as to evaluate the effects of health conditions, valuation methods, and proxy types on the differences.
Methods
Eligible studies published in PubMed, Embase, Web of Science, and Cochrane Library up to December 2019 were identified according to PRISMA guidelines. Meta-analyses were performed to calculate the weighted mean differences (WMDs) in HUs between proxy- versus self-reports. Mixed-effects meta-regressions were applied to explore differences in WMDs among each health condition, valuation method and proxy type.
Results
A total of 30 studies were finally included, comprising 211 pairs of HUs assessed by 15,294 children and 16,103 proxies. This study identified 34 health conditions, 10 valuation methods, and 3 proxy types. In general, proxy-reported HUs were significantly different from those assessed by children themselves, while the direction and magnitude of these differences were inconsistent regarding health conditions, valuation methods, and proxy types. Meta-regression demonstrated that WMDs were significantly different in patients with ear diseases relative to the general population; in those measured by EQ-5D, Health utility index 2 (HUI2), and Pediatric asthma health outcome measure relative to Visual analogue scale method; while were not significantly different in individuals adopting clinician-proxy and caregiver-proxy relative to parent-proxy.
Conclusion
Divergence existed in HUs between self and proxy-reports. Our findings highlight the importance of selecting appropriate self and/or proxy-reported HUs in health-related quality of life measurement and economic evaluations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Economic evaluation is used to compare the costs and consequences of alternative healthcare interventions. The measurements of various costs are similar; but the forms of health outcomes vary by different evaluation techniques, including cost-effectiveness analysis (CEA), cost–benefit analysis (CBA), and cost-utility analysis (CUA) [1]. The CUA has been recommended by many government agencies to support the decision-making process and increasingly used in economic evaluations [2,3,4]. In CUA, quality-adjusted life years (QALYs), which combine health utilities (HUs) and length of life into a single metric, are used as health outcomes. The HU which can reflect the societal preference for different health states is usually a value between 0 and 1, where 0 represents death and 1 represents perfect heath. There are also HUs for coditions worse than death, which theoretically has no minimum limit [5]. However, in order to avoid the large impact that a negative value has on the average HU calculation, it is usually converted to a value between − 1 and 0, which is symmetrical to the value range for health conditions better than death [1].
When estimating HUs associated with different health states, both direct and indirect valuation methods can be used [5]. Direct methods indicate that the assessment and measurement process can be completed in one step. Common direct methods include the visual analogue scale (VAS), standard gamble (SG), and time trade-off (TTO) techniques [1]. Indirect methods rely on the multi-attribute utility instruments (MAUIs) which comprise two main elements: a descriptive system for measuring health states and a scoring algorithm for valuing the health states defined by the descriptive system [6]. Commonly used indirect methods for children include the Health Utilities Index (HUI) [7], the EuroQol 5-dimension (EQ-5D) Youth version (EQ-5D-Y) [8], and the Child Health Utility 9-Dimension (CHU9D) [9].
It is documented in the literature that there are more challenges when measuring HUs for children than for adults [10]. The cognitive capability and the reading level of children are lower than that of adults, which will make it very challenging applying valuation methods to obtain their HUs [11]. Therefore, proxy-assessment is needed on this occasion. Proxy-assessment is a way to measure children’s HUs by children’s proxies such as their parents, clinician or other people knowing children’s health states instead of themselves. However, the consistency between proxy-reported and self-reported HU values is controversial. Mark et al. [12] found that the interrater agreement was the highest between cancer survivors and parents and the lowest between controls and physicians or teachers. Miguel et al. [13] found that the level of agreement was poor in the HRQoL assessment between children with cerebral palsy and parents in all the questionnaire domains of EQ-5D-Y and fair or poor in the visual analogue scale. Bull et al. [14] found that parents of children with mild to moderate health conditions rated utilities similar to their children.
Reviews involving self-reported and proxy-reported HUs have been conducted in children. Khadka et al. [15] used narrative synthesis and found that utilities derived from children or proxies are not interchangeable. Kwon et al. [11, 16] identified proportions of respondent types and analyzed the influence of proxy type on HUs obtained by HUI3 and VAS. However, there is no systematic review using quantitative analysis to compare the differences between self-reported and proxy-reported HU values, and exploring the potential influence factors. Since Proxy-assessment are commomly used for obtaining children’s HUs due to children’s limited cognitive capability regardless of the severity of children’s health condition, it is of necessity and importance to understand the differences of magnitude and direction between self and proxy-reported HUs, as well as which factors have potential impact on the differences [11]. Based on this, the researchers may select proper methods or proxies to measure the primary HUs, or to select the proper HUs for performing economic evaluations. Therefore, we conducted this study to compare the differences between self and proxy-reported HUs and to explore the effects of different health conditions, valuation methods, and proxy types on these differences.
Methods
Systematic review
The systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17]. The full PRISMA checklist was included in Additional file 1: Appendix 1. The following databases were searched for studies between inception and December 31, 2019: Pubmed, Embase, Web of Science, and Cochrane Library. The search terms and the detailed search strategy was outlined in Additional file 1: Appendix 2.
Studies were included if they (1) reported HUs assessed by pairwise (children and proxies) populations, (2) contained participants were aged under 18 years, and (3) were published in English. Studies were excluded if they (1) did not focus on pediatric populations, (2) did not include HU values, (3) proxy respondents reported their own HUs, (4) were published in the form of systematic review, meta-analysis, abstract, or dissertation. The literature search and screening were conducted independently by two investigators. Any disagreements were adjudicated by senior investigators.
Data extraction
The following information was extracted: general characteristics of studies and participants, study designs, health conditions, valuation methods, and types of proxy. Data extracted or calculated from studies included sample size and mean, as well as standard deviation (SD) of HUs. The VAS scores were divided by 100 if the primary data were assessed using a 0–100 scale. In addition, health conditions were classified according to the International Classification of Diseases 10 revision (ICD-10) chapters [16]. Two investigators independently extracted the data from the full text. If any inconsistency was found, senior investigators reviewed the original literature and made a final decision.
Quality assessment
The risk of bias was evaluated using the Newcastle–Ottawa Scale for longitudinal studies [18] and an adapted form for cross-sectional and patient case series studies [19]. Specific assessment results were listed in Additional file 1: Appendix 3. Two investigators independently conduct the quality assessment and inconsistent results were resolved by senior investigators.
Statistical analysis
Weighted mean difference (WMD) is a summary statistic commonly used for meta analysis of continuous data, it can be used to measure the absolute difference between the mean value in two groups [20]. Therefore, we conducted meta-analysis to estimate WMD which was defined as proxy-reported HUs minus self-reported HUs, and associated 95% confidence intervals (CI), by specific health conditions, valuation methods, and proxy types. The mean and SD of HU values as well as sample sizes were included to pool the WMDs. The heterogeneity was quantified using the I2 statistic, fixed effects models were applied if the value of I2 was smaller than 50%; otherwise, random effects models were used [21, 22].
Meta-regression can be used to investigate differences for categorical independent variables [23].In Meta-regressions, the dependent variable is the effect estimate, the independent variables are characteristics of studies that might influence the size of effect. The regression coefficients will estimate how the effect in each subgroup differs from a reference subgroup [20]. Therefore, we performed meta-regression using linear mixed-effects models with restricted maximum likelihood method to evaluate the effects of different factors on the difference in HUs between self-reports and proxy-reports, after controlling for methodological factors and study specific random effects not accounted for by the independent variables [20]. The dependent variable were WMDs estimated from the meta-analysis, and the independent variables included health conditions, valuation methods, and proxy types. Independent variables regarding health condition were introduced on condition level instead of diagnosis level since too many diagnosis types existed. The coefficients and 95% CIs were reported and P values < 0.05 were deemed to be statistically significant. P values were also adjusted by using a Monte Carlo permutation test with 1000 iterations to obtain more realistic values. Statistical analyses were performed using Stata software, version 15.0.
Results
Systematic review
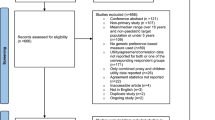
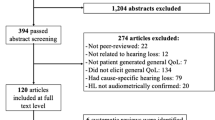
Figure 1 presented the flow chart of the literature search and screening. The literature search identified 71,439 articles and 35,104 articles were excluded due to duplicates. A total of 35,739 articles were excluded by titles and abstracts screening, the main reason for exclusion was no HU values reported. Hence, 596 articles entered full-text articles screening and 566 articles were excluded mainly for not reporting pairwise HU values. Finally, 30 articles comprising 211 pairs of self-reported and proxy-reported HUs were included in meta-analyses [9, 24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52].

Flow diagram of literature search and study identification
Study characteristics
Table 1 summarized the characteristics of the included studies. These studies were published between 1994 and 2019, and most of them were conducted in USA (23%), UK (17%), and Canada (10%). In terms of study design, 15 studies were cross-sectional (50%), 7 were longitudinal (23%) and 8 were patient case series (27%). There were 211 pairs of HUs assessed by 15,294 children and 16,103 proxies, covering the general population and individuals with different health conditions.
Nine valuation instruments were identified. Direct instruments contained VAS (74 pairs; 35%), SG (15 pairs; 7%), and TTO (7 pairs, 3%); while indirect instruments contained EQ-5D (10 pairs, 5%), EQ-5D-Y (9 pairs, 4%), HUI2 (22 pairs, 10%), HUI3(37 pairs, 15%), CHU-9D (6 pairs, 3%), QWB (1 pair, 0.5%), and Pediatric asthma health outcome measure (PAHOM) (30 pairs, 14%). The most commonly used proxy respondent type was parents (169 pairs, 80%), followed by caregivers (35 pairs, 17%) and clinicians (7 pairs, 3%).
Additional file 1: Appendix 3 presented the quality of included studies. In general, all the studies showed low risks of bias, which indicated high quality.
WMDs in HUs by health conditions
We pooled the WMDs of HUs between self-reports and proxy-reports by health conditions (Table 2). On this basis, the WMDs assessed by different valuation methods (Additional file 1: Appendix 4) and proxy types (Additional file 1: Appendix 5) were estimated, respectively. In Table 2, the proxy-reported HUs were significantly higher than self-reported ones in general (WMD: 0.034; 95% CI: 0.021, 0.047), overweight or obese (WMD: 0.059; 95% CI: 0.045, 0.073), cystic fibrosis (WMD: 0.030; 95% CI: 0.005, 0.055), and ELBW/EP (WMD: 0.065; 95% CI: 0.023, 0.106) populations. While the proxy-reported HUs were significantly lower in meningitis (WMD: − 0.117; 95% CI − 0.167, − 0.067), pediatric mobility impairment (WMD: − 0.059; 95% CI − 0.059, − 0.027), prolonged acute convulsive seizures (WMD: − 0.265; 95% CI − 0.344, − 0.186), asthma (WMD: − 0.034; 95% CI: − 0.039, − 0.029), lung disease (WMD: − 0.030; 95% CI − 0.057, − 0.003), spina bifida (WMD: − 0.044; 95% CI − 0.078, − 0.010), injury (WMD: − 0.083; 95% CI − 0.155, − 0.012), and chronic illness populations (WMD: − 0.047; 95% CI − 0.080, − 0.013).
WMDs in HUs by valuation methods
In Additional file 1: Appendix 4, VAS scores assessed by proxies were higher than those assessed by children themselves in general (WMD: 0.041; 95% CI 0.019, 0.064), overweight or obese (WMD: 0.058; 95% CI 0.037, 0.079) and pelvic inflammatory disease (WMD: 0.146; 95% CI 0.119, 0.714) populations, while lower in patients with spina bifida (WMD: − 0.061; 95% CI − 0.072, − 0.050). Proxy-reported HUs assessed by TTO were higher in pelvic inflammatory disease patients (WMD: 0.085; 95% CI 0.051, 0.120) and lower in chronic illness patients (WMD: − 0.150; 95% CI − 0.287, − 0.013). Proxy-reported HUs assessed by SG were higher in ELBW/EP (WMD: 0.065; 95% CI: 0.023, 0.106) populations.
For HUI2, proxy-reported HU values were higher for hearing loss patients (WMD: 0.080; 95% CI 0.033, 0.127) and otitis media patients (WMD: 0.120; 95% CI 0.052, 0.188), and lower for patients with meningitis (WMD: − 0.140; 95% CI − 0.216, − 0.064), paediatric mobility impairment (WMD: − 0.043; 95% CI − 0.087, 0.000) and chronic illness (WMD: − 0.130; 95% CI − 0.234, − 0.026). For HUI3, proxies generated higher HUs in general (WMD: 0.029; 95% CI 0.016, 0.042), mixed cancer diagnosis (WMD: 0.186; 95% CI 0.137, 0.235), diabetes (WMD: 0.020; 95% CI 0.003, 0.037), overweight or obese (WMD: 0.093; 95% CI 0.084, 0.103), hearing loss (WMD: 0.170; 95% CI: 0.096, 0.244) and otitis media (WMD: 0.200; 95% CI 0.097, 0.303) populations; and generated lower HUs in meningitis (WMD: − 0.160; 95% CI − 0.304, − 0.016), paediatric mobility impairment (WMD: − 0.060; 95% CI − 0.112, − 0.008) and spina bifida (WMD: − 0.026; 95% CI − 0.040, − 0.012) patients.
Regarding HUs obtained by EQ-5D, proxies reported lower values for meningitis patients (WMD: − 0.230; 95% CI − 0.383, − 0.077) and patients with prolonged acute convulsive seizures (WMD: − 0.265; 95% CI − 0.344, − 0.186), and higher values in hearing loss population (WMD: 0.070; 95% CI 0.032, 0.108). In addition, children-specific instrument, EQ-5D-Y, was used in overweight or obese and paediatric mobility impairment populations, CHU-9D was used in anxiety disorders population, and disease-specific instrument, PAHOM, was used for asthma patients. All the P-values were less than 0.05 except for HUs assessed by CHU-9D.
WMDs in HUs by proxy types
In Additional file 1: Appendix 5, parent-reported HUs were statistically significantly higher than self-reported HUs in general (WMD: 0.034; 95% CI 0.021, 0.047), MSKD (WMD: 0.019; 95% CI 0.005, 0.033), pelvic inflammatory disease (WMD: 0.121; 95% CI 0.096, 0.146), and ELBW/EP (WMD: 0.075; 95% CI 0.048, 0.103) populations. On the contrary, parents reported lower HUs in patients diagnosed with paediatric mobility impairment (WMD: − 0.058; 95% CI − 0.087, − 0.028), prolonged acute convulsive seizures (WMD: − 0.270; 95% CI − 0.382, − 0.158), asthma (WMD: − 0.034; 95% CI − 0.039, − 0.029), injury (WMD: − 0.083; 95% CI − 0.155, − 0.012) and chronic illness (WMD: − 0.047; 95% CI − 0.080, − 0.013).
HUs reported by clinicians were higher in brain tumour patients (WMD: 0.104; 95% CI 0.054, 0.155) and mixed cancer diagnosis patients (WMD: 0.186; 95% CI 0.137, 0.235), while lower in patients with prolonged acute convulsive seizures (WMD: − 0.260; 95% CI − 0.373, − 0.147). In addition, caregiver-reported HUs were statistically significantly lower than self-reported ones in meningitis (WMD: − 0.117; 95% CI − 0.167, − 0.067), lung disease(WMD: − 0.030; 95% CI − 0.057, − 0.003), and spina bifida (WMD: − 0.044; 95% CI − 0.078, − 0.010) populations.
Differences in WMDs
The results of the meta-regression were shown in Table 3. The general population, VAS instrument, and proxy assessment by parents were set as the reference. The constant indicated that parent-reported HUs were higher than self-reported HUs in the general population (β: 0.047; 95% CI 0.004, 0.090) when the VAS instrument was applied. We determined statistical significance based on the adjusted P values which estimated by Monte Carlo permutation test. Compared with the general population applying the VAS instrument and parental proxy, the HU values of WMDs between children and their proxies were significantly higher in patients diagnosed with diseases of the ear (β: 0.127; 95% CI 0.046, 0.209); and were significantly lower in patients applying EQ-5D (β: − 0.110; 95% CI − 0.163, − 0.058), HUI2 (β: − 0.067; 95% CI − 0.111, − 0.024), and PAHOM (β: − 0.104; 95% CI − 0.175, − 0.034).
Main findings
According to the results from WMDs of different health conditions, we found that for mild health conditions such as the general population, overweight or obese, and ELBW/EP, proxies tended to report higher HUs than children themselves; however, proxies tended to report lower HUs for severe diseases such as meningitis, pediatric mobility impairment, asthma, lung disease, spina bifida, injury, and chronic illness. In addition, results of meta-regression indicated that in comparison with the general population, WMDs of HUs in patients diagnosed with ear disease had significant differences.
On the basis of WMDs obtained by different valuation methods, we found that most pairs applied direct methods including VAS, SG, and TTO generated no significant difference between self- and proxy-reported HUs. And meta-regression showed that WMDs obtained by SG and TTO have no significant difference compared with those obtained by VAS, indicating the WMDs in HUs obtained using direct methods were similar. For indirect methods, both general instruments including HUI2, HUI3, and EQ-5D and children specific instruments including EQ-5D-Y and CHU-9D generated inconsistent WMDs in the direction and magnitude. Meta-regression indicated that the WMDs of HUs assessed by EQ-5D, HUI2, and PAHOM differed significantly from those assessed using the VAS instrument.
Regarding WMDs assessed by different proxy types, we found that parental proxy was dominantly used in the selected studies, and no obvious trend was found regarding the WMDs in HUs reported by this proxy. However, caregivers might underestimate the child’s HUs since all the related statistically significant WMD values were negative. On the contrary, clinicians might overestimate children’s HUs in cancer patients. Moreover, meta-regression demonstrated that WMDs obtained by the clinician and caregiver proxies were not significantly different from those obtained by parents.
Discussion
This study was the first systematic and meta-analysis to compare self- and proxy-reported HUs quantitatively. The WMDs in HUs between self- and proxy-reports stratified by health conditions, valuation methods, and proxy types were estimated using meta-analysis, and the difference in WMDs between each health conditions, valuation methods, and proxy types were evaluated using meat-regressions. In general, disagreement exists between self- and proxy-reported HUs.
Comparisons and implications
As regards proxy- versus self -reports specified by health conditions, consistent results were reported in some previous studies focused on specific health conditions. Jardine et al. [53] analyzed 21 studies including HRQoL data from both children with congenital health conditions and their parents, and concluded that a child’s perception of QoL differed from their parents, with parents frequently underestimating QoL. Pickard et al. [54] compared the HRQoL outcomes measured from children with acute lymphoblastic leukemia (ALL) and their parents, and they also found the responses of children and proxy were not interchangeable. Litsenburg et al. [55] included 15 studies to compare utility scores between self- and proxy-respondents for children with ALL, and the conclusion was that proxy-respondents were less reliable for observable conditions. Although these studies did not report specific differences, the fact that differences exist in self- and proxy-reported HUs between different health conditions were emphasized. Therefore, when researchers determine whether to include the self- or proxy-reported HUs, health conditions of the target populations should be one of important factors to consider.
For proxy- versus self-reports obtained by different valuation methods, Kwon et al. [16] performed a meta-regression and found that proxy-reported HUs were significantly higher when using HUI3 and VAS than self-reported HUs. In adult populations, significant differences in HUs were also found between direct and indirect valuation methods [56,57,58]. These evidences were consistent with our findings that valuation methods including direct and indirect instruments might cause a divergence between self- and proxy-reported HUs, direct valuation methods are straightforward and convenient for reseachers but not very comprehensible for respondents, indirect valuation methods are more complicated for reaseachers to calculate but easier for respondents to understand and answer. Researchers should take into full consideration about characteristics of different valuation methods for both direct and indirect ones. Hence, our study highlighted the importance of applying appropriate valuation methods, especially when it is necessary to measure the primary HUs, or to select the HUs obtained by different direct or indirect valuation methods for economic evaluations.
In terms of proxy- versus self-reports assessed by different proxy types, an earlier review conducted by Fluchel et al. [59] proved different proxy types can lead to differences in the inter-rater effects in HU estimates. Other studies showed that proxy-assessment by clinicians might lead to a discrepancy in HUs compared to proxy-assessment by parents [25, 32, 59]. It should be noted that meta-regression results showed no difference existing in WMDs assessed by caregivers or physicains versus parents, which does not mean that no difference presented in HUs assessed by proxy versus children themselves. Therefore, we suggest that the HUs to be assessed by children and proxies simultaneously, and researchers need to consider the HUs on the perspective from both self and proxy rather than just considering single perspective in order to obtain more comprehensive results. In addition, in order to avoid proxy-reports are from proxy’s personal judgment, clear instructions about incorporating the child’s perspective into assessment could be developed for all proxy types, which would improve the quality and accuracy of proxy-assessed HUs..
Strengths and limitations
This study has two primary strengths. First, different from earlier reviews mainly used qualitative methods, our study included all the literatures which reported the HU values in pairwise self-proxy population to perform quantitative analyses, which can provide more direct evidence. WMD is used to estimate the difference in mean values between two groups, which is the suitable effect size for continuous data exactly as the HUs for this meta-analysis [20]. While meta-regression is commonly used to investigate heterogeneity for a meta-analysis, but it can also be used to investigate differences for categorical independent variables, so we applied meta-regression to assess the differences in WMDs among each potential factors [20]. Second, the differences in HUs were compared within and between each factor comprehensively. Since we not only compared the difference in HUs between self- and proxy-reports stratified by factors including health conditions, valuation methods, and proxy types, as well as to explore the divergence in WMDs between each factor by conducting meta-regression.
This study also has several limitations. First, when conducting meta-analysis, the heterogeneity was high (I2 > 50%) in certain results, which may be mainly caused by the target population coming from different studies. Although we tried our best to conduct sub-group analysis by taking health conditions, valuation methods, and proxy types into consideration, more specific sub-group analysis considering participant characteristics such as gender and age cannot be performed due to the lack of information. Second, when performing meta-regression, we adopted health conditions but not diagnoses as the independent variable, which made it unable to understand the differences in WMDs between each diagnoses, for the reason that limited sample size (211 pairs) cannot tolerate that many grouping variables. Third, the number of groups and associated sample sizes were relatively small for certain groups especially when specific to valuation methods under certain diagnoses, which may compromise the validity of our findings. Similarly, although meta-regression showed that differences in WMDs existed or not existed in certain group relative to reference group, the results may be biased given the small numbers of groups of interest. Fourth, funnel plots used to identify publication bias were not given in our study, for the reason that the funnel plots generated in our study cannot indicate publication bias, since certain pairs of self- and proxy-reports included in one single meta-analysis to estimate WMD were from same article. Fifth, the reasons why the differences existed among the valuation measures or the proxy types cannot be addressed by conducting this meta-analyses. Therefore, we cannot suggest which valuation method or proxy type is most reliable based on our current results. Lastly, our systematic review only included studies published in the English language.
Conclusions
Assessment of children’s HUs which can be measured by both self and proxy is important not only for HRQoL researches but also for economic evaluations such as cost-utility/effectiveness analysis regarding children population. However, the way to measure and cite children’s HUs in relative studies has been a challenge for current researchers due to the lack of quantitative analysis comparing differences between proxy- and self-reported HUs. The results of our study show that differences indeed exist in HUs between self- and proxy-reports, and potential factors including health conditions, valuation methods, and proxy types impact the direction and magnitude of the differences in different ways. These findings may provide certain guidance for measuring primay children’s HUs, or be an available source for conducting economic evaluations regarding children population. In addition, due to the paucity and heterogeneity of existing studies, there are inevitable bias in our study, so future studies are needed to synthesize more evidence and to explore the trend of differences.
Availability of data and materials
Not applicable.
Abbreviations
- Hus:
-
Health utilities
- WMDs:
-
Weighted mean differences
- CEA:
-
Cost-effectiveness analysis
- CBA:
-
Cost–benefit analysis
- CUA:
-
Cost-utility analysis
- QALYs:
-
Quality-adjusted life years
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- ICD-10:
-
International classification of diseases 10 revision
- MAUIs:
-
Multi-attribute utility instruments
- VAS:
-
Visual analogue scale
- SG:
-
Standard gamble
- TTO:
-
Time trade-off
- CHU9D:
-
Child health utility 9-dimension
- HUI:
-
Health utility index
- PAHOM:
-
Pediatric asthma health outcome measure
- ALL:
-
Acute lymphoblastic leukemia
- VLBW/VP:
-
Very low birth weight/very preterm
- ELBW/EP:
-
Extremely low birth weight/extremely preterm
- ODD:
-
Oppositional defiant disorder
- CD:
-
Conduct disorder
- DBD:
-
Disruptive behaviour disorder
- ADHD:
-
Attention deficit hyperactivity disorder
- SA:
-
Substance abuse
- SD:
-
Standard deviation
- CI:
-
Confidence intervals
References
Drummond MF SM, Claxton K, et al. Methods forthe Economic Evaluation of Health Care Programmes, 4th ed2015.
Excellence NIfHaC. Guide to the methods of technology appraisal 2013. 2013.
PBAC. Guidelines for preparing submissions to the Pharmaceutical Benefits Advisory Committee (Version 4.5) (2015).
CADTH. Guidelines for the economic evaluation of health technologies: Canada 4th Edition (2017).
Streiner DL, Norman GR, Cairney J. Health measurement scales: a practical guide to their development and use (5th edition). Aust N Z J Public Health. 2016;40(3):294–5. https://doi.org/10.1111/1753-6405.12484.
Chen G, Ratcliffe J. A review of the development and application of generic multi-attribute utility instruments for paediatric populations. Pharmacoeconomics. 2015;33(10):1013–28.
Barr RD, Chalmers D, De Pauw S, et al. Health-related quality of life in survivors of Wilms’ tumor and advanced neuroblastoma: a cross-sectional study. J Clin Oncol. 2000;18(18):3280–7.
Barr R, Gonzalez A, Longchong M, et al. Health status and health-related quality of life in survivors of cancer in childhood in Latin America: a MISPHO feasibility study. Int J Oncol. 2001. https://doi.org/10.3892/ijo.19.2.413.
Baumann N, Bartmann P, Wolke D. Health-related quality of life into adulthood after very preterm birth. Pediatrics. 2016;137(4):e20153148. https://doi.org/10.1542/peds.2015-3148.
Ungar DWJ. Challenges in health state valuation in paediatric economic evaluation. Pharmacoeconomics. 2011;29(8):641–52.
Kwon J, Kim SW, Ungar WJ, et al. Patterns, trends and methodological associations in the measurement and valuation of childhood health utilities. Qual Life Res. 2019;28(7):1705–24.
Fluchel M, Horsman JR, Furlong W, Castillo L, Alfonz Y, Barr RD. Self and proxy-reported health status and health-related quality of life in survivors of childhood cancer in Uruguay. Pediatr Blood Cancer. 2008;50(4):838–43. https://doi.org/10.1002/pbc.21299.
Perez-Sousa MA, Olivares PR, Gusi N. Parent-child discrepancy in the assessment of health- related quality of life using the EQ-5D-Y questionnaire. Archivos Argentinos de Pediatria. 2017;115(5 1):541–6.
Bull KS, Kennedy CR, Bailey S, Ellison DW, Clifford SC. Improved health-related quality of life outcomes associated with SHH subgroup medulloblastoma in SIOP-UKCCSG PNET3 trial survivors. Acta Neuropathol. 2014;128(1):151–3. https://doi.org/10.1007/s00401-014-1300-4.
Khadka J, Kwon J, Petrou S, Lancsar E, Ratcliffe J. Mind the (inter-rater) gap. An investigation of self-reported versus proxy-reported assessments in the derivation of childhood utility values for economic evaluation: A systematic review. Soc Sci Med. 2019;240:112543. https://doi.org/10.1016/j.socscimed.2019.112543.
Kwon J, Kim SW, Ungar WJ, Tsiplova K, Madan J, Petrou S. A systematic review and meta-analysis of childhood health utilities. Med Decis Making. 2018;38(3):277–305. https://doi.org/10.1177/0272989X17732990.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Wells G, Shea B, O'Connell D et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 18 Dec 2018.
Herzog R, Alvarez-Pasquin MJ, Diaz C, et al. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health. 2013;13:154.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane handbook for systematic reviews of interventions. 2nd ed. Chichester: Wiley; 2019.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Higgins JPT, Green S (editors). Cochrane handbook for systematic reviews of interventions version 5.1.0 [The Cochrane Collaboration, 2011. www.cochrane-handbook.org. Accessed 1 January].
Chandler J, Hopewell S. Cochrane methods—twenty years experience in developing systematic review methods. Syst Rev. 2013;2:76. https://doi.org/10.1186/2046-4053-2-76.
Czyzewski DI, Mariotto MJ, Bartholomew LK, LeCompte SH, Sockrider MM. Measurement of quality of well being in a child and adolescent cystic fibrosis population. Med Care. 1994;32(9):965–72. https://doi.org/10.1097/00005650-199409000-00007.
Glaser AW, Furlong W, Walker DA, et al. Applicability of the health utilities index to a population of childhood survivors of central nervous system tumours in the U.K. Eur J Cancer. 1999;35(2):1–261.
Saigal S, Stoskopf BL, Feeny D, et al. Differences in preferences for neonatal outcomes among health care professionals, parents, and adolescents. JAMA. 1999;281(21):1991–7. https://doi.org/10.1001/jama.281.21.1991.
Verrips GH, Stuifbergen MC, den Ouden AL, et al. Measuring health status using the Health Utilities Index: agreement between raters and between modalities of administration. J Clin Epidemiol. 2001;54(5):475–81. https://doi.org/10.1016/s0895-4356(00)00317-6.
Brunner HI, Maker D, Grundland B, et al. Preference-based measurement of health-related quality of life (HRQL) in children with chronic musculoskeletal disorders (MSKDs). Med Decis Mak. 2003;23(4):314–22.
Brunner HI, Klein-Gitelman MS, Miller MJ, et al. Health of children with chronic arthritis: relationship of different measures and the quality of parent proxy reporting. Arthritis Rheum. 2004;51(5):763–73. https://doi.org/10.1002/art.20689.
Sung L, Young NL, Greenberg ML, et al. Health-related quality of life (HRQL) scores reported from parents and their children with chronic illness differed depending on utility elicitation method. J Clin Epidemiol. 2004;57(11):1–1166.
Cardarelli C, Cereda C, Masiero L, et al. Evaluation of health status and health-related quality of life in a cohort of Italian children following treatment for a primary brain tumor. Pediatr Blood Cancer. 2006;46(5):637–44. https://doi.org/10.1002/pbc.20480.
Fu L, Talsma D, Baez F, et al. Measurement of health-related quality of life in survivors of cancer in childhood in Central America: feasibility, reliability, and validity. J Pediatr Hematol Oncol. 2006;28(6):331–41.
Hanberger L, Ludvigsson J, Nordfeldt S. Health-related quality of life in intensively treated young patients with type 1 diabetes. Pediatr Diabetes. 2009;10(6):374–81. https://doi.org/10.1111/j.1399-5448.2008.00496.x.
Jelsma J, Ramma L. How do children at special schools and their parents perceive their HRQoL compared to children at open schools? Health Qual Life Outcomes. 2010;8:72. https://doi.org/10.1186/1477-7525-8-72.
Penn A, Lowis SP, Stevens MC, et al. A detailed prospective longitudinal assessment of health status in children with brain tumors in the first year after diagnosis. J Pediatr Hematol Oncol. 2011;33(8):592–9. https://doi.org/10.1097/MPH.0b013e31821388c0.
Lee JM, Rhee K, O’grady MJ, et al. Health utilities for children and adults with type 1 diabetes. Med Care. 2011;49(10):924–31. https://doi.org/10.1097/MLR.0b013e318216592c.
Belfort MB, Zupancic JA, Riera KM, Turner JH, Prosser LA. Health state preferences associated with weight status in children and adolescents. BMC Pediatr. 2011;11:12. https://doi.org/10.1186/1471-2431-11-12.
Trent M, Lehmann HP, Qian Q, Thompson CB, Ellen JM, Frick KD. Adolescent and parental utilities for the health states associated with pelvic inflammatory disease. Sex Transm Infect. 2011;87(7):583–7. https://doi.org/10.1136/sextrans-2011-050187.
Gerald JK, McClure LA, Harrington KF, Moore T, Hernández-Martínez AC, Gerald LB. Measurement characteristics of the pediatric asthma health outcome measure. J Asthma. 2012;49(3):260–6. https://doi.org/10.3109/02770903.2012.656863.
Rhodes ET, Goran MI, Lieu TA, et al. Health-related quality of life in adolescents with or at risk for type 2 diabetes mellitus. J Pediatr. 2012;160(6):911–7. https://doi.org/10.1016/j.jpeds.2011.11.026.
Wolke D, Chernova J, Eryigit-Madzwamuse S, Samara M, Zwierzynska K, Petrou S. Self and parent perspectives on health-related quality of life of adolescents born very preterm. J Pediatr. 2013;163(4):1020-6.e2. https://doi.org/10.1016/j.jpeds.2013.04.030.
Kulpeng W, Sornsrivichai V, Chongsuvivatwong V, et al. Variation of health-related quality of life assessed by caregivers and patients affected by severe childhood infections. BMC Pediatr. 2013;13:122. https://doi.org/10.1186/1471-2431-13-122.
Robertson W, Fleming J, Kamal A, et al. Randomised controlled trial and economic evaluation of the “Families for Health” programme to reduce obesity in children. Arch Dis Child. 2017;102(5):416–26. https://doi.org/10.1136/archdischild-2016-311514.
Vermeulen KM, Jansen DEMC, Buskens E, Knorth EJ, Reijneveld SA. Serious child and adolescent behaviour disorders; a valuation study by professionals, youth and parents. BMC Psychiatry. 2017;17(1):208. https://doi.org/10.1186/s12888-017-1363-6.
Sims-Williams HJ, Sims-Williams HP, Mbabazi Kabachelor E, Warf BC. Quality of life among children with spina bifida in Uganda. Arch Dis Child. 2017;102(11):1057–61. https://doi.org/10.1136/archdischild-2016-312307.
Bray N, Noyes J, Harris N, Edwards RT. Measuring the health-related quality of life of children with impaired mobility: examining correlation and agreement between children and parent proxies. BMC Res Notes. 2017;10(1):377. https://doi.org/10.1186/s13104-017-2683-9.
Creswell C, Violato M, Fairbanks H, et al. Clinical outcomes and cost-effectiveness of brief guided parent-delivered cognitive behavioural therapy and solution-focused brief therapy for treatment of childhood anxiety disorders: a randomised controlled trial. Lancet Psychiatry. 2017;4(7):529–39. https://doi.org/10.1016/S2215-0366(17)30149-9.
Shiroiwa T, Fukuda T, Shimozuma K. Psychometric properties of the Japanese version of the EQ-5D-Y by self-report and proxy-report: reliability and construct validity. Qual Life Res. 2019;28(11):3093–105. https://doi.org/10.1007/s11136-019-02238-1.
Perez-Sousa MA, Olivares PR, Garcia-Hermoso A, Gusi N. Does anthropometric and fitness parameters mediate the effect of exercise on the HRQoL of overweight and obese children/adolescents? Qual Life Res. 2018;27(9):2305–12. https://doi.org/10.1007/s11136-018-1893-5.
de Medeiros CB, Moxon-Emre I, Scantlebury N, et al. Medulloblastoma has a global impact on health related quality of life: findings from an international cohort. Cancer Med. 2020;9(2):447–59. https://doi.org/10.1002/cam4.2701.
Kirkham FJ, Vigevano F, Raspall-Chaure M, et al. Health-related quality of life and the burden of prolonged seizures in noninstitutionalized children with epilepsy. Epilepsy Behav. 2020;102:106340. https://doi.org/10.1016/j.yebeh.2019.04.058.
López-Bastida J, López-Siguero JP, Oliva-Moreno J, et al. Health-related quality of life in type 1 diabetes mellitus pediatric patients and their caregivers in Spain: an observational cross-sectional study. Curr Med Res Opin. 2019;35(9):1589–95. https://doi.org/10.1080/03007995.2019.1605158.
Jardine J, Glinianaia SV, Mcconachie H, et al. Self-reported quality of life of young children with conditions from early infancy: a systematic review. Pediatrics. 2014;134(4):e1129–48.
Pickard AS. A structured review of studies on health-related quality of life and economic evaluation in pediatric acute lymphoblastic leukemia. J Natl Cancer Inst Monogr. 2004;2004(33):102–25.
Van Litsenburg RRL, Kunst A, Huisman J, et al. Health status utilities in pediatrics: a systematic review of acute lymphoblastic leukemia. Med Decis Mak. 2014;34(1):21–32.
McLernon DJ, Dillon JF, Donnan PT. Health-state utilities in liver disease: a systematic review and meta-analysis. Value Health. 2006;9(6):A245–6.
Peasgood T, Ward SE, Brazier J. Health-state utility values in breast cancer. Expert Rev Pharmacoecon Outcomes Res. 2010;10(5):553–66. https://doi.org/10.1586/erp.10.65.
Wyld M, Morton RL, Hayen A, Howard K, Webster AC. A systematic review and meta-analysis of utility-based quality of life in chronic kidney disease treatments. PLoS Med. 2012;9(9):e1001307. https://doi.org/10.1371/journal.pmed.1001307.
Mark F, Horsman JR, et al. Self and proxy-reported health status and health-related quality of life in survivors of childhood cancer in Uruguay. Pediatr Blood Cancer. 2008;50(4):838–43.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
PYC and AXM were responsible for the study design. MYJ and YM completed the database search, screening, data extraction and quality assessment, under the guidance of AXM and PYC. MYJ and PYC performed the statistical analysis and interpreted the data. MYJ, YM and MHL contributed to the writing and translating of the manuscript. MHL and RM checked and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors have declared that no competing interests exist.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Appendix 1: PRISMA checklist. Appendix 2: Search terms and strategy. Appendix 3: Risk of bias assessment by Newcastle Ottawa Scale. Appendix 4: Weighted mean differences in health utilities between self- and proxy-reports by health conditions and valuation methods. Appendix 5: Weighted mean differences in health utilities between self- and proxy-reports by health conditions and proxy types.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jiang, M., Ma, Y., Li, M. et al. A comparison of self-reported and proxy-reported health utilities in children: a systematic review and meta-analysis. Health Qual Life Outcomes 19, 45 (2021). https://doi.org/10.1186/s12955-021-01677-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-021-01677-0