
Abstract
Background
To investigate the association between weight status and health-related quality of life (HRQOL) among pupils in Guangzhou, China.
Methods
The study comprised 5781 children aged 8–12 years from 29 schools. Height and weight were objectively measured using standardized methods, and BMI z-score derived using the age and sex specific WHO reference 2007 for 5–19 years. Weight status was classified as underweight (<−2SD), healthy weight (between -2SD and 1SD), overweight/obesity (>1SD). HRQOL was measured by the self-report version of the Pediatric Quality of Life Inventory 4.0.
Results
After controlling for gender, age, school type, parental education, and family income, HRQOL scores were significantly lower in overweight/obese compared with healthy weight children only in the social functioning domain (β = −1.93, p = 0.001). Compared with healthy weight children, underweight children had significantly lower total (β = −1.47, p = 0.05) and physical summary scores (β = −2.18, p = 0.02). Subgroup analysis for gender indicated that compared to healthy weight, total (β = −1.96, p = 0.02), psychosocial (β = −2.40, p = 0.01), social functioning (β = −3.36, p = 0.001), and school functioning (β = −2.19, p = 0.03) scores were lower in overweight/obese girls, but not boys. On the other hand, being underweight was associated with lower physical functioning (β = −2.27, p = 0.047) in girls, and lower social functioning (β = −3.63, p = 0.01) in boys. The associations were mainly observed in children aged 10 and over, but were not significant in younger children. Children from private schools had generally lower HRQOL compared to those in public schools, but the associations with weight status were similar in both groups.
Conclusions
The relationship between overweight/obesity and HRQOL in children in China is not as prominent as that seen in children in western or high-income countries. However, there appears to be gender and age differences, with more of an impact of overweight on HRQOL in girls and older children compared with boys and younger children. Underweight is also associated with lower HRQOL. Future intervention to prevent both obesity and undernutrition may have a positive impact on the HRQOL in children in China.
Similar content being viewed by others


Background
During recent years, the prevalence of overweight and obesity in children and adolescents has increased dramatically worldwide, especially in low and low middle-income countries [1, 2]. In China, a country which has been undergoing a substantial economic transition in the past few decades, the prevalence of childhood overweight and obesity has increased from 1.1 to 9.6% between 1985 and 2010 [3]. Although the prevalence of obese children in China is still lower than that in western countries, research on Chinese and other Asian immigrants in the US has shown that the longer the time spent in the US, the greater the risk of obesity [4], suggesting a significant environmental impact on the development of obesity. Thus, with the rapid economic development in China, and without intervention to prevent it, obesity in children and adults may become a major public health problem in this country.
Obesity has well documented adverse physical health consequences both in childhood and adulthood, including increased risk of cardiometabolic disease and some cancers [5–8]. In addition there is growing evidence that obesity in childhood and adolescence has a detrimental effect on health-related quality of life (HRQOL) [9–14], with severely obese children having HRQOL that is comparable to that of children with cancer [15]. HRQOL is a comprehensive and multi-dimensional construct that includes self-assessment of physical, emotional and social well-being [16]. Dimensions of HRQOL that appear to be most strongly associated with obesity are physical, social and school functioning [9, 17–19]. However, there is evidence to suggest that the impact of childhood obesity on HRQOL is influenced by culture [20], and may differ between boys and girls and with age, from childhood to adolescence [14, 21]. In some communities obesity is not recognized as a problem and is associated with good health, so one would expect HRQOL to be less influenced by obesity in these communities [22–24]. In addition to the relationship between obesity and HRQOL, the potential effect of underweight on HRQOL should also be considered, although some population studies have reported that the HRQOL of underweight youth was generally no different from those with normal weight [25]. To date, most studies that examine the relationship between weight status and HRQOL have been conducted in western or other high income countries and much of the evidence for an adverse relationship is based on studies in clinical populations [9, 17], the effect of weight status on HRQOL among children living in the community in lower income countries, such as China, has been rarely studied.
The aim of this study was to evaluate the association between HRQOL and weight status in a community sample of school children aged 8–12 years in Guangzhou, China.
Methods
Sampling and participants
The analysis presented comes from a sub-group of participants drawn from a larger study; a cross-sectional study undertaken in Guangzhou, which aimed to determine the prevalence and risk factors for overweight and obesity in children age 5–12 years. To achieve a representative sample, a multi-stage stratified cluster random sampling method was used. First, five of the ten urban districts in Guangzhou were selected using a random number generator. Second, within each selected district, schools were stratified by public or private status. Children who are permanently resident in Guangzhou are eligible to attend public schools, whereas children of economic migrant families are obliged to attend private schools. Six primary schools were randomly chosen from each district with a 2:1 (public: private school) ratio, therefore 4 public and 2 private schools were selected. Third, within each school two classes per grade (from grade 1 to 5) were randomly selected. Finally, all pupils from selected classes (age 5–12 years) were invited to take part. Children were excluded if they had a significant physical and psychological condition that was felt by teaching staff to compromise their participation in the study (e.g. children with a major disability, or serious cognitive or psychological dysfunction). Of the 30 selected schools, permission for the study was not obtained for one school (a private school), leaving 29 participating schools.
Written informed consent was sought from the parents of 11445 eligible children aged 5–12 years (on behalf of their children), 9917 (86.6%) of which agreed to participate. Data collection took place from April to June 2014. All participating children had anthropometric measurements taken in school by trained research staff using standardized procedures and equipment. The parents of all participating children were asked to complete a questionnaire which included questions about sociodemographic and lifestyle characteristics. Given the inherent difficulties of collecting survey data from young children [26], we administered a self-completion student questionnaire, which included a measure of HRQOL to children in grade 3 and above only (8+ years; n = 5962). After exclusion of 181 student questionnaires which were incomplete, the number of children aged 8–12 years included in this analysis was 5781.
The study was approved by the Ethical Committee of Guangzhou Center for Disease Control and Prevention and the University of Birmingham Ethics Committee. Permission to conduct the study in the identified schools was granted by the relevant Departments of Education and Health.
Measurement of weight status
Children wore light clothing with no shoes for height and weight measurements. Height was measured to the nearest 0.1 cm using a TGZ type height tester (Dalian). Weight was measured to the nearest 0.1 kg using an electronic scale (JH-1993 T, weighing Apparatus Co. Ltd. Dalian). Body Mass Index was calculated (weight (kg)/Height (m)2) and standard deviation score (BMI z-score) derived using the age and sex specific WHO reference 2007 for children aged 5–19 years. Children were also categorized as underweight (<−2SD), healthy weight (between -2SD and 1SD), overweight (>1SD) and obese (>2SD) [27]. Measuring devices were systematically calibrated.
Measurement of HRQOL
The PedsQL 4.0 was used to assess HRQOL in this study. This is a validated 23-item questionnaire for children aged 2–18 years [28], administered as either a child self-report or a parent proxy-report. Detailed information about the questionnaire has been reported elsewhere [28]. In brief, the PedsQL comprises four subscales: physical (8 items), social (5 items), emotional (5 items), and school functioning (5 items). Mean scores are calculated based on a 5-point response scale for each item and transformed to a 0–100 scale with a higher score representing better quality of life. The PedsQL subscales can be used to derive three summary scores: a total score (mean of all items), a physical health score (mean of physical functioning items) and a psychosocial health score (mean of emotional, social and school functioning items).
Collection of parental data
Parents were asked to complete a questionnaire which included questions on level of maternal and paternal education, maternal and paternal height and weight (to calculate BMI), and family income.
Statistical analyses
All statistical analyses were performed using SPSS for windows (version 21.0, SPSS, Inc., Chicago, IL). Descriptive statistics were used to summarise demographic anthropometric and HRQOL data. To explore differences in HRQOL between different subgroups independent-sample t tests (two groups) or general linear models (three groups) were used.
To explore the association between weight status and HRQOL, taking into account the effect of school as cluster, multilevel random effects models were developed with HRQOL scores (total, physical summary, psychosocial summary, emotional functioning, social functioning and school functioning scores) as dependent, and weight status (grouped into underweight, healthy weight (reference group), or overweight/obese) as the independent variables. Other covariates (gender, age group, school type, maternal education, paternal education and family income) were included in the multilevel models if statistically significant differences in HRQOL were found between the subgroups in the univariate analyses. School was added as a random effect and was significant in all models (p < 0.01). In addition, we conducted subgroup analyses to explore differences in the association between weight status and HRQOL in boys and girls, in younger (8–9 years old) and older (10–12 years old) age groups, and by type of school (public or private) attended. Level of significance in the analyses was set at 0.05.
Results
Participant characteristics
The characteristics of participating children are shown in Table 1. The average age was 9.7 years (SD = 1.01), and 54.5% were boys. Approximately 70% were public school students. The mean BMI z-score was −0.1 (SD = 1.33, range −4.07 to 5.47), although more than 20% of the children were overweight (13.0%) or obese (7.4%). The prevalence of overweight/obesity was higher in the public compared with the private schools (22.4% and 15.9% respectively, χ 2 = 31.79, p < 0.01).
As shown in Table 1, participants reported an overall mean total HRQOL score of 78.88 (SD = 13.57). The unadjusted mean total HRQOL score in girls was slightly higher than in boys (t = 2.83, p = 0.005), and older children (10–12 years old) had higher HRQOL score than younger children (8–9 years old) (79.63 and 77.93 respectively, t = 4.70, p < 0.001). The HRQOL score of public school students was much higher than private school students (80.40 and 75.36 respectively, t = 13.14, p < 0.001). There was also a statistically significant trend for higher HRQOL scores with increasing years of parental education and family income. However, there was no significant difference in total HRQOL score across the three weight categories (F = 1.25, p = 0.288).
Weight status and HRQOL
Table 2 shows the results of the adjusted models (after adjustment for gender, age, school type, length of maternal education, length of paternal education, family income). HRQOL scores across all domains were generally lower in both overweight/obese and underweight children compared with those who were healthy weight, although the differences were only statistically significantly lower for social functioning in the overweight/obese group (β = −1.93, p = 0.001) and total (β = −1.47, p = 0.05) and physical summary scores (β = −2.18, p = 0.02) among underweight children, compared with those who were healthy weight.
Weight status and HRQOL in subgroups
Subgroup analysis by gender, school type and age group are shown in Tables 3, 4 and 5 respectively. For boys, there was no significant association between overweight/obesity and HRQOL in any dimension of PedsQL. However, underweight boys had lower social functioning scores (β = −3.63, p = 0.01). In girls, the overweight/obese group had significantly lower total (β = −1.96, p = 0.02), psychosocial (β = −2.40, p = 0.01), social functioning (β = −3.36, p = 0.001), and school functioning (β = −2.19, p = 0.03) scores than the healthy weight group. Physical summary scores were significantly lower in underweight compared with healthy weight girls (β = −2.27, p = 0.047). In addition, we found underweight boys had significantly lower social functioning scores than underweight girls (t = 5.5, p < 0.01).
Regarding school type, children from public schools had higher scores in all dimensions of PedsQL than children from private schools across all weight categories, but the relationship between HRQOL and overweight/obesity did not differ by school type. Inverse association was just founded between overweight/obesity and social functioning in both public and private schools (β = −1.65, p = 0.013; and β = −2.77, p = 0.029 respectively). Significantly lower physical summary scores in the underweight compared to the healthy weight group was only seen in public schools (β = −2.38, p = 0.02).
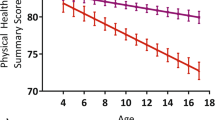
There were no significant associations between weight status and HRQOL in children under 10 years, but in those aged 10 and over, physical summary scores were lower in both the overweight/obese group and the underweight group compared with the healthy weight group (β = −1.87, p = 0.009; and β = −2.90, p = 0.009 respectively). Social functioning scores were lower in overweight/obese children compared with healthy weight children only in this older age group (β = −1.91, p = 0.01).
Discussion
Overall, the study findings did not provide evidence for a strong association between overweight/obesity and health related quality of life among children aged 8 to 12 years in Guangzhou, China. Although our study indicated that overweight/obese children reported significantly lower scores in social functioning than healthy weight children, the absolute difference in scores was small, particularly in relation to the larger effect of social factors (such as parental education, income and migrant status) on HRQOL. Our findings in relation to weight status are in keeping with other studies conducted in low income countries. Studies in Fiji (with 8947 children aged 12–18 years) [29], and Kuwait (with 500 children aged 10–14 years) [30], both reported that HRQOL was similar in obese and healthy weight children. Another smaller study with 778 children, aged 6–13 years in Guangzhou in China also showed that, except for school functioning, obesity had no significant association with HRQOL [31]. A further study with 98 pairs of obese adolescents and healthy weight peers in Kuwait found that only the physical dimension of HRQOL was lower in the obese participants [30]. However, the findings of this study contrast with several other studies which suggest that overweight and obesity could significantly impair children’s HRQOL [9–12, 17, 21, 32]. There may be two potential reasons for this. Firstly, much of the evidence for an adverse relationship was based on studies in clinical populations [9, 10, 12, 17, 32], which may have resulted in an overestimation of the strength of the association [14]. Cultural differences may be another factor. Similar to Fiji [29], most Chinese people, especially the elderly, expect children to be heavy, as this is taken as a sign of health and prosperity [26, 33]. Additionally, in this study we found that the total and physical summary scores were lower in the underweight group, particularly among older children. This contrasts with several studies which report no significant difference in HRQOL between underweight and healthy weight children [25, 34, 35]. Again, this could be linked to cultural influences; if heaviness is taken to be a sign of health, growth and prosperity, then underweight may indicate poor health and poverty, and thus lead to a lower quality of life.
Subgroup analyses revealed a different pattern of associations between weight and dimensions of HRQOL in certain groups. There were gender differences, with more prominent associations between psychosocial summary scores and overweight/obesity in girls, but not in boys. These findings are somewhat consistent with a Lebanese study conducted with adolescents, which found that obesity was related to all dimensions in girls except emotional and school functioning, but in boys, only the inverse association between obesity and physical functioning was significant [36]. Other studies have also reported associations between obesity and lower HRQOL scores in girls, but not in boys [14, 37]. A potential explanation for this may be the difference between boys and girls in the perception of ideal body image. Influenced by television, magazines, advertisements and Chinese culture, thinness represents the ideal body image for girls, but not for boys. A previous study (with 12750 participants aged 10–26 years) conducted in Guangzhou showed that 47.18% girls with healthy weight perceived themselves as being overweight, but this percentage was just 18.08% in boys. Furthermore, 28.55% healthy weight boys expected to be bigger [38]. This different perception between genders of the ideal body shape is coherent with the finding of lower psychosocial quality of life in girls who are overweight and lower social functioning scores in boys who are underweight. A French study, reported similar findings, with higher BMI in girls and lower BMI in boys associated with lower mental HRQOL scores [39]. We also found that the association between overweight/obesity and HRQOL was more apparent in the older age group (10–12 years) affecting both physical and social functioning. A potential explanation for the impact of weight status on physical functioning as children get older, is that the physical manifestations of both overweight and underweight become more prominent with increasing age. This is in line with a study by Fontaine, in which the authors reported that the impact of obesity on physical functioning was significantly more than its impact on psychological functioning in adults [40].
Although the association between weight status and HRQOL was similar across the different school types, children in public schools had higher scores in almost all domains of HRQOL compared with those in private schools. A possible explanation for this is that most of the children attending private schools are migrants. Migrant families tend to be less affluent and less well educated relative to the resident families whose children attend the public schools [41].
In contrast to previous studies, we found that HRQOL scores overall were higher in older children. Most previous research reports lower HRQOL in adolescents compared with children [42–44], although the majority of these studies were undertaken in western countries, and may reflect cultural differences, such as differences in parental and peer relationships and in adolescent expectations.
A strength of this study is that it is one of the first and larger studies to explore the relationship between childhood weight status and HRQOL in a country undergoing rapid economic transition. Also, the findings will be generalizable to other Chinese urban populations as they are drawn from a large representative sample of both resident and migrant communities. The study also has some limitations. We only measured HRQOL from the child’s perspective. Parent proxy-reported HRQOL would have enabled triangulation of findings and potentially more robust conclusions could have been drawn. A further limitation is the cross-sectional nature of the study, which means a temporal relationship between weight status and quality of life cannot be explored.
Conclusions
This study has demonstrated that the relationship between overweight/obesity and HRQOL in children in China is not as prominent as that seen in children in western or high-income countries. However, the gender differences in the association between adiposity and HRQOL that exist in other populations have been observed to a certain extent in this study. In Chinese populations, underweight may be an important contributor to lower HRQOL. Future intervention to prevent both over and undernutrition may improve quality of life in both the underweight and the overweight and obese groups.
Abbreviations
- BMI:
-
Body mass index
- HRQOL:
-
Health-related quality of life
- SD:
-
Standard deviation
- WHO:
-
World Health Organization
References
World Health Organization. Noncommunicable diseases: country profiles 2011. Scand J Soc Med. 2011;14(1):7–14.
Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25.
Jun M, Ci-he C, Hai-jun W, Bin D, Yi S, Pei-jin H, Bing Z. The trend analysis of overweight and obesity in Chinese students during 1985–2010. Chin J Pre Med. 2012;46(9):776–80.
Lauderdale DS, Rathouz PJ. Body mass index in a US national sample of Asian Americans: effects of nativity, years since immigration and socioeconomic status. Int J Obes Relat Metab Disord. 2000;24(9):1188–94.
Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The relation of overweight to cardiovascular risk factors among children and adolescents: the Bogalusa Heart Study. Pediatrics. 1999;103(6 Pt 1):1175–82.
Valerio G, Licenziati MR, Iannuzzi A, Franzese A, Siani P, Riccardi G, Rubba P. Insulin resistance and impaired glucose tolerance in obese children and adolescents from Southern Italy. Nutr Metab Cardiovasc Dis. 2006;16(4):279–84.
Kipping RR, Jago R, Lawlor DA. Obesity in children. Part 1: epidemiology, measurement, risk factors, and screening. BMJ. 2008;337:a1824.
Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. The epidemiology of obesity. Gastroenterology. 2007;132(6):2087–102.
Buttitta M, Iliescu C, Rousseau A, Guerrien A. Quality of life in overweight and obese children and adolescents: a literature review. Qual Life Res. 2014;23(4):1117–39.
Riazi A, Shakoor S, Dundas I, Eiser C, McKenzie SA. Health-related quality of life in a clinical sample of obese children and adolescents. Health Qual Life Outcomes. 2010;8(1):134.
Zeller MH, Inge TH, Modi AC, Jenkins TM, Michalsky MP, Helmrath M, Courcoulas A, Harmon CM, Rofey D, Baughcum A, et al. Severe obesity and comorbid condition impact on the weight-related quality of life of the adolescent patient. J Pediatr. 2015;166(3):651–9. e654.
Pratt KJ, Lamson AL, Swanson MS, Lazorick S, Collier DN. The importance of assessing for depression with HRQOL in treatment seeking obese youth and their caregivers. Qual Life Res. 2012;21(8):1367–77.
Morrison KM, Shin S, Tarnopolsky M, Taylor VH. Association of depression & health related quality of life with body composition in children and youth with obesity. J Affect Disord. 2015;172:18–23.
Bolton K, Kremer P, Rossthorn N, Moodie M, Gibbs L, Waters E, Swinburn B, de Silva A. The effect of gender and age on the association between weight status and health-related quality of life in Australian adolescents. BMC Public Health. 2014;14:898.
Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life of severely obese children and adolescents. JAMA. 2003;289(14):1813–9.
Williams J, Wake M, Hesketh K, Maher E, Waters E. Health-related quality of life of overweight and obese children. JAMA. 2005;293(1):70–6.
Tsiros MD, Olds T, Buckley JD, Grimshaw P, Brennan L, Walkley J, Hills AP, Howe PR, Coates AM. Health-related quality of life in obese children and adolescents. Int J Obes (Lond). 2009;33(4):387–400.
Ottova V, Erhart M, Rajmil L, Dettenborn-Betz L, Ravens-Sieberer U. Overweight and its impact on the health-related quality of life in children and adolescents: results from the European KIDSCREEN survey. Qual Life Res. 2012;21(1):59–69.
Chan CM, Wang WC. Quality of life in overweight and obese young Chinese children: a mixed-method study. Health Qual Life Outcomes. 2013;11(33):33.
Hamzaid H, Talib RA, Azizi NH, Maamor N, Reilly JJ, Wafa SW. Quality of life of obese children in Malaysia. Int J Pediatr Obes. 2011;6(5–6):450–4.
Helseth S, Haraldstad K, Christophersen KA. A cross-sectional study of Health Related Quality of Life and body mass index in a Norwegian school sample (8–18 years): a comparison of child and parent perspectives. Health Qual Life Outcomes. 2015;13:47.
Fredriks AM, Van Buuren S, Sing RA, Wit JM, Verloove-Vanhorick SP. Alarming prevalences of overweight and obesity for children of Turkish, Moroccan and Dutch origin in The Netherlands according to international standards. Acta Paediatr. 2005;94(4):496–8.
Greenhalgh T, Helman C, Chowdhury AM. Health beliefs and folk models of diabetes in British Bangladeshis: a qualitative study. BMJ. 1998;316(7136):978–83.
Pallan M, Parry J, Adab P. Contextual influences on the development of obesity in children: a case study of UK south Asian communities. Prev Med. 2012;54(3–4):205–11.
Wallander JL, Kerbawy S, Toomey S, Lowry R, Elliott MN, Escobar-Chaves SL, Franzini L, Schuster MA. Is obesity associated with reduced health-related quality of life in Latino, black and white children in the community? Int J Obes. 2013;37(7):920–5.
Bell A. Designing and testing questionnaires for children. J Res Nurs. 2007;12(5):461–9.
de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85(9):660–7.
Varni JW, Seid M, Rode CA. The PedsQL: measurement model for the pediatric quality of life inventory. Med Care. 1999;37(2):126–39.
Petersen S, Moodie M, Mavoa H, Waqa G, Goundar R, Swinburn B. Relationship between overweight and health-related quality of life in secondary school children in Fiji: results from a cross-sectional population-based study. Int J Obes. 2014;38(4):539–46.
Boodai SA, Reilly JJ. Health related quality of life of obese adolescents in Kuwait. BMC Pediatr. 2013;13(1):105.
Cui-ling W, Yu-ming C, Zhong-lin Z, Wei-qing C, Jian-ping W, Wen-heng Z, Jiang-nan W, Yu-ming C, Zhong-lin Z, Wei-qing C, et al. Impact of obesity on health-related quality of life in elementary school children. Maternal and Child Health Care China. 2007;36:5148–50.
Hughes AR, Farewell K, Harris D, Reilly JJ. Quality of life in a clinical sample of obese children. Int J Obes (Lond). 2007;31(1):39–44.
Jiang J, Rosenqvist U, Wang H, Greiner T, Lian G, Sarkadi A. Influence of grandparents on eating behaviors of young children in Chinese three-generation families. Appetite. 2007;48(3):377–83.
Jalali-Farahani S, Chin YS, Amiri P, Taib M. Body mass index (BMI)-for-age and health-related quality of life (HRQOL) among high school students in Tehran. Child Care Health Dev. 2014;40(5):731–9.
Arif AA, Rohrer JE. The relationship between obesity, hyperglycemia symptoms, and health-related quality of life among Hispanic and non-Hispanic white children and adolescents. BMC Fam Pract. 2006;7:3.
Fazah A, Jacob C, Moussa E, El-Hage R, Youssef H, Delamarche P. Activity, inactivity and quality of life among Lebanese adolescents. Pediatr Int. 2010;52(4):573–8.
Kunkel N, Oliveira WF, Peres MA. Overweight and health-related quality of life in adolescents of Florianopolis, Southern Brazil. Rev Saude Publica. 2009;43(2):226–35.
Wei L, Wei-jia L, Zhong-shan G, Rong L, Li-hua X, Lin L, Si-yu C, Wei-jia L, Zhong-shan G, Rong L, et al. Self-evaluation of weight and unhealthy weight control behaviors among adolescents in Guangzhou. Chin J Sch Health. 2014;12:1829–32.
Bonsergent E, Benie-Bi J, Baumann C, Agrinier N, Tessier S, Thilly N, Briancon S. Effect of gender on the association between weight status and health-related quality of life in adolescents. BMC Public Health. 2012;12:997.
Fontaine KR, Cheskin LJ, Barofsky I. Health-related quality of life in obese persons seeking treatment. J Fam Pract. 1996;43(3):265–70.
Liu W, Liu W, Lin R, Li B, Pallan M, Cheng KK, Adab P. Socioeconomic determinants of childhood obesity among primary school children in Guangzhou China. BMC Public Health. 2016;16:482.
Michel G, Bisegger C, Fuhr DC, Abel T. group K. Age and gender differences in health-related quality of life of children and adolescents in Europe: a multilevel analysis. Qual Life Res. 2009;18(9):1147–57.
Simeoni MC, Auquier P, Antoniotti S, Sapin C, San Marco JL. Validation of a French health-related quality of life instrument for adolescents: the VSP-A. Qual Life Res. 2000;9(4):393–403.
Christophe S, Marie-Claude S, Mohammed EK, Stéphanie A, Pascal A. Reliability and validity of the VSP-A, a health-related quality of life instrument for ill and healthy adolescents. J Adolesc Health. 2005;36(4):327–36.
Acknowledgements
The authors gratefully acknowledge the contribution of Yuexiu, Haizhu, Liwan, Luogang and Nansha Education Bureau and 29 elementary schools.
Funding
The data used for this analysis came from a study funded by the Guangzhou Medical Foundation (20131A031001).
Availability of data and materials
Participant level data are available from the corresponding author.
Authors’ contributions
WL wrote the first draft of the paper, with contribution from MP and PA. All authors contributed to study design and conduct of the study, and contributed to the final manuscript. All authors have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Permissions to conduct the study were granted by the Guangzhou Departments of Education and Health. The study was approved by the Ethical Committee of Guangzhou Center for Disease Control and Prevention and the University of Birmingham Ethics Committee (reference ERN_13-1519). Informed consent for measurements was sought from the parents of all eligible children, and verbal assent was obtained from the children at the time of measurement.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Liu, W., Lin, R., Liu, W. et al. Relationship between weight status and health-related quality of life in Chinese primary school children in Guangzhou: a cross-sectional study. Health Qual Life Outcomes 14, 166 (2016). https://doi.org/10.1186/s12955-016-0567-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-016-0567-7