
Abstract
Background
The Clínica Universidad de Navarra-Body Adiposity Estimator (CUN-BAE) index has been recommended as an ideal indicator of body fat and exhibited significant correlation with cardiometabolic risk factors. However, whether the CUN-BAE index correlates with incident diabetes in Asian populations is unknown. Therefore, this longitudinal study was designed to evaluate the association between baseline CUN-BAE index and type 2 diabetes mellitus (T2DM).
Methods
This retrospective longitudinal study involved 15,464 participants of 18–79 years of age in the NAGALA (NAfld in the Gifu Area Longitudinal Analysis) study over the period of 2004–2015. Cox proportional hazards regression was performed to test the relationship between the baseline CUN-BAE index and diabetes incidence. Further stratification analysis was conducted to ensure that the results were robust. The diagnostic utility of the CUN-BAE index was tested by the receiver operating characteristic (ROC) curve.
Results
Over the course of an average follow-up of 5.4 years, 373 (2.41%) participants developed diabetes. A higher diabetes incidence was associated with higher CUN-BAE quartiles (P for trend< 0.001). Each 1 unit increase in CUN-BAE index was associated with a 1.08-fold and 1.14-fold increased risk of diabetes after adjustment for confounders in males and females, respectively (both P < 0.001). Stratification analysis demonstrated a consistent positive correlation between baseline CUN-BAE and diabetes incidence. Moreover, based on ROC analysis, CUN-BAE exhibited a better capacity for diabetes prediction than both body mass index (BMI) and waist circumference (WC) in both sexes.
Conclusions
The baseline CUN-BAE level was independently related to the incidence of diabetes. Increased adiposity determined by CUN-BAE could be used as a strong nonlaboratory predictor of incident diabetes in clinical practice.
Similar content being viewed by others


Background
Diabetes is a significant contributor to health-system costs and a significant cause of death and morbidity worldwide [1]. The 10th edition of the IDF Diabetes Atlas reported that by 2045, the prevalence of diabetes is estimated to rise from 10.5% (536.6 million people) in 2021 to 12.2% (783.2 million people) globally [2]. Additionally, its prevalence in Asian regions is notably increasing, and more than 60% of all cases of diabetes occur in these regions [3, 4]. The risk of diabetic neuropathy, cerebrovascular disease, and even carcinoma is significantly increased in patients with diabetes [3, 5,6,7,8]. Therefore, there is an urgent need for efficient and simple methods to improve early detection, especially in Asian populations.
Obesity, which refers to an overabundance of body fat, is a recognized risk factor for diabetes [9, 10]. Although BMI is a traditional diagnostic method that is most frequently employed in the present classification system, its ability to discriminate between lean and fat mass is limited and varies by sex and age [11, 12]. In addition, the waist-to-hip ratio or waist circumference is used to reflect the degree of abdominal fat accumulation, but they are insufficient for a comprehensive assessment of body fat mass [13, 14]. Body fat percentage (BF%) has been proven to be an effective and robust method for identifying obesity and the risk of obesity-related diabetes [15, 16]. It has been recognized that extra body fat could result in insulin resistance and thus promote the occurrence and development of diabetes [17,18,19,20]. Furthermore, BF% has been confirmed as a risk factor that affects cardiometabolic function independently of BMI and abdominal obesity in previous studies [13, 21, 22]. Thus, BF% may be a notable index for predicting individuals at high risk of obesity-related type 2 diabetes.
Currently, various methods, including magnetic resonance imaging (MRI) and dual-energy X-ray absorptiometry (DXA), can be used for the measurement of BF% [11]. However, their wide application is largely limited by high costs and radiation exposure [23, 24]. Recently, a newly developed alternative anthropometric method, the CUN-BAE index, has attracted much attention. This BF% estimator is based on the age, sex and BMI of Caucasian subjects [25]. A strong association between CUN-BAE and BF% was identified in a previous study, and this association was stronger than that of other anthropometric measurements [25, 26]. In addition, the CUN-BAE index was better than BMI or WC at predicting cardiometabolic risk factors [25, 27,28,29]. In this regard, it is already known that CUN-BAE is an optimal and accessible method for estimating BF% and identifying people at high risk for metabolic disorders. However, the CUN-BAE index has not been extensively studied for the prediction or identification of diabetes to the best of our knowledge [28]. Thus, CUN-BAE was evaluated for its importance and contribution to the prediction of diabetes in adulthood in Asian individuals in the current study.
Methods
Data source
The Dryad Digital Repository (www.datadryad.org) provided the original data, which were openly published and freely available to researchers. The Dryad database was created in September 2008 and funded by the US National Science Foundation. This database was used to deposit high-quality data resources, making the data underlying scientific publications freely reusable, discoverable and citable. In the current study, these population-based longitudinal data were available from this online database, which was originally analysed and released by Professor Okamura [30]. The original data contained the following variables: age, sex, waist circumference, fatty liver, fasting plasma glucose (FPG), body mass index (BMI), exercise habit, smoking status, glycosylated haemoglobin (HbA1c), and diastolic and systolic blood pressure (DBP and SBP). In addition, gamma-glutamyl transferase (GGT), lipid profile (total cholesterol, triglycerides, and HDL-C) alanine aminotransferase (ALT), aspartate aminotransferase (AST) and diabetes incidence was also included in this database. Furthermore, each of the participants was required to complete a survey that included lifestyle variables, such as alcohol consumption, physical activities and smoking status. Three groups of individuals were categorized based on their smoking habits: nonsmokers, former smokers, and current smokers. Drinking habits were divided into high consumption (> 280 g/week), moderate consumption (140–280 g/week), light consumption (40–140 g/week), and minimal consumption (< 40 g/week). For physical exercise, patients who worked out more than once a week were characterized as standard exercisers.
Study population
Study participants included all patients who participated in Murakami Memorial Hospital’s physical examination program between 2004 and 2015. In addition, an incident diabetes follow-up study was conducted. These participants were enrolled over different time points, and most of them received exams annually. In this study, the median follow-up time was 5.4 years (1967 days), ranging from 0.5 years (164 days) to 13.0 years (4732 days). Individuals who met one of the following criteria were excluded: (1) alcoholic fatty liver disease; (2) diabetes at baseline; (3) utilization of any medication; (4) hepatitis B antigen and hepatitis C antibody found at baseline in patients with viral hepatitis; and (5) lost information on covariates. The study ultimately included 15,464 subjects, 7034 of whom were females and 8430 of whom were males (Fig. 1).

Flowchart of patient enrollment. Abbreviations: T2DM, type 2 diabetes mellitus
Measurement of the CUN-BAE index
CUN-BAE = − 44.988 + (3.172 × BMI) + (10.689 × sex) + (0.503 × age) – (0.026 × BMI2) + (0.181 × BMI × sex) – (0.02 × BMI × age) + (0.00021 × BMI2 × age) – (0.005 × BMI2 × sex).
Male = 0; Female = 1.
Ascertainment of diabetes
The criteria for diagnosing diabetes were HbA1c no less than 6.5%, fasting plasma glucose no less than 7 mmol/L, or reporting diabetes diagnoses on the follow-up questionnaire.
Statistical analysis
We stratified baseline characteristics based on sex because males and females have significantly different body compositions. Then, four groups were formed according to CUN-BAE quartiles (Q1-Q4). Continuous variables are presented as means and standard deviation. Categorical data are presented as frequencies and percentages. For variables with a normal distribution, one-way ANOVA was performed, and variables with nonnormal distributions were tested using the Kruskal–Wallis test. Categorical variables among groups were compared using the chi-square test. Univariate and multivariate Cox regression analyses were applied to calculate the hazards ratio (HR) and 95% confidence intervals (CIs) between the baseline CUN-BAE index and diabetes after adjusting for age, BMI (category), smoking status, alcohol consumption, fatty liver disease, GGT, HDL, TGs, TC, SBP and exercise habits. These may be important factors in T2DM development as a previous study has shown [31]. BMI (category) was calculated according to WHO criteria for Asian individuals (< 24 kg/m2; ≥24 kg/m2 and < 28 kg/m2; ≥28 kg/m2) [32]. Then, the differences among different CUN-BAE quartile groups were determined by log-rank tests.
Furthermore, ROC curves were also drawn to measure the diagnostic efficacy of different anthropometric parameters. The results were further validated through stratification analysis and likelihood ratio tests according to the following factors: sex, BMI, age, SBP, fatty liver disease, HDL-C, GGT, TC, TGs, smoking status, exercise habits and alcohol consumption. Statistical analysis and data processing were carried out in R (http://project.r-project.org) and Empower Stats (http://www.empowerststs.com, X&Y Solutions, Inc., Boston, MA). A probability of P < 0.05 was used as a measure of statistical significance (two-sided).
Results
Study population characteristics
Approximately 15,464 participants without diabetes participated in the present study (average age of 43.7 ± 8.9 years). Overall, 8430 males (54.5%) and 7034 females (45.5%) were included in this study. Males and females demonstrated significant differences in anthropometric indicators, blood pleasure values, lifestyles and laboratory indicators. The average CUN-BAE index in females was remarkably higher than that in males (29.8 ± 4.9 vs. 20.9 ± 4.7). As demonstrated in Table 1, participants in the top quartile of the CUN-BAE (Q4) presented with older age, higher waist circumference, higher BMI, higher levels of AST, ALT, GGT, FBG, DBP, SBP, TC, TGs, and HbA1c, a higher incidence of fatty liver and a higher percentage of smokers and drinkers compared with the other groups (Q1-Q3) (all P values < 0.001). In addition, it was remarkable that in both males and females, diabetes incidence increased with increasing quartiles of the baseline CUN-BAE index (P for trend< 0.001) (Fig. 2).

Prevalence of diabetes according to the baseline CUN-BAE index quartiles. Notes: All of the study participants were divided into four groups according to quartiles of CUN-BAE index (In male: quartile 1 [Q1]: < 17.826; quartile 2 [Q2]: 17.826 to ≤20.862; quartile 3 [Q3]: 20.868 to ≤23.945; quartile 4 [Q4]: > 23.945. In female: quartile 1 [Q1]: < 26.374; quartile 2 [Q2]: 26.374 to ≤29.434; quartile 3 [Q3]: 29.434 to ≤32.833; quartile 4 [Q4]: > 32.833). The prevalence of diabetes increased with ascending quartiles of CUN-BAE index (P for trend < 0.05). A Males; B Females
Clinical outcome and Kaplan–Meier analysis stratified by CUN-BAE index
Over 5.4 years of follow-up (min-max: 0.5 years–13.0 years) from 2004 to 2015, 373 (2.4%) participants suffered from T2DM in this cohort. As shown in Fig. 3, among different CUN-BAE index quartile groups, the cumulative incidence of diabetes differed considerably (log-rank P < 0.001).

Cumulative incidence of T2DM during follow-up. Notes: The incidence of diabetes increased with ascending CUN-BAE quartiles in both males and females. Both Log-rank P < 0.001. A Males; B Females
Association between the CUN-BAE and T2DM
As illustrated in Table 2, the unadjusted model of CUN-BAE revealed a significant association with diabetes risk in both sexes (both P < 0.001). Significant correction remained after controlling for BMI, age, smoking status, alcohol consumption, exercise habits and fatty liver disease (both P < 0.001). The increased baseline CUN-BAE index was still independently linked to an elevated diabetes risk when HDL, TC, TGs, GGT and SBP were also included in Model 3 (both P < 0.01). Further, a 2-unit increase in CUN-BAE index was associated with a significantly higher diabetes risk (HR = 1.16 and 1.30 in males and females, respectively, both P < 0.01). The top CUN-BAE quartile group remained significantly correlated with incident diabetes after controlling for all variables in Model 2 (P < 0.05), while the relationship was moderately attenuated after further adjustment for HDL, TC, TGs, SBP, and GGT in Model 3.
Stratification analysis and interaction test
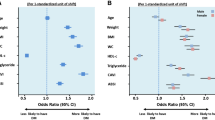
As shown in Fig. 4, subgroup analysis was conducted to identify potential confounding factors affecting the correlation between the baseline CUN-BAE index and type 2 diabetes. All of the covariates used in Model 3 were factored into the model used for the stratified analyses except the variables used for stratification, including sex, age, BMI, smoking status, fatty liver disease, exercise habits, alcohol consumption, HDL, TC, TGs, SBP and GGT. Multiple subgroups analyses of the study found a consistent link between an elevated CUN-BAE index and diabetes incidence (all interaction P > 0.05).

Stratification analysis on the relationship of CUN-BAE index with diabetes occurrence. Notes: HR was calculated using 1 − unit increase of CUN-BAE index. All variables except the stratification variables were included in the stratified analyses of Model 3. HDL < 1.04 mmol/L in men and < 1.29 mmol/L in women was defined as low HDL-C; GGT < 50 U/L in men and < 32 U/L in women was defined as low GGT. Abbreviations: BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; GGT, gamma-glutamyl transferase; TC, total cholesterol; TGs, triglycerides; SBP, systolic blood pressure
Predictive value of the CUN-BAE index in incident diabetes
The baseline CUN-BAE index was assessed for its predictive power through the use of an ROC curve (Fig. 5). Among males and females, the areas under the curves (AUCs) of CUN-BAE were 0.711 (95% CI: 0.701–0.721) and 0.779 (95% CI: 0.769–0.788), respectively. In comparison to BMI and WC, the CUN-BAE index demonstrated the largest AUC. In exception to its comparison with WC in male participants, all pairwise AUC comparisons showed significant differences (Table 3).

ROC curves of CUN-BAE, BMI and WC for predicting incident T2DM. Notes: A Males; B Females. Abbreviations: BMI, body mass index; WC, waist circumference; ROC, receiver-operating characteristics
Discussion
This population-based study showed an overall increase in the risk of developing type 2 diabetes with increasing CUN-BAE index after potential confounders were taken into account in a Japanese cohort. Compared to BMI and WC, the CUN-BAE index exhibited a better predictive value for diabetes. To our knowledge, this is the first longitudinal study to investigate the relationship between the CUN-BAE index and T2DM, focusing on the Japanese population.
Obesity is a substantial risk factor for T2DM [33]. Prior studies found that the prevalence of obesity assessed by BF% was two to six times higher than that calculated using BMI [29, 34,35,36]. A possible explanation was that BMI, as a traditional anthropometric measure for general obesity, was unable to differentiate between weight increase caused by muscle and fat, and may thus overlook the slim people with excessive body fat [37, 38]. BF% was proven to be a more precise indicator for obesity identification and obesity-related metabolic diseases, such as T2DM and metabolic syndrome, even in people with normal BMI categories [13, 21]. In recent years, the CUN-BAE index was considered to be an excellent estimation for BF% [28, 39, 40]. In addition, the CUN-BAE index has also been found to be more closely linked to insulin resistance than BMI in males in previous studies [25]. Thus, the CUN-BAE index could be a more meaningful and effective predictor of diabetes.
In the present study, it is remarkable that the CUN-BAE index, as a proxy index for BF%, showed a strong correlation with diabetes incidence. Additionally, our study also revealed that the CUN-BAE was shown to be a more reliable and useful predictor of T2DM incidence than BMI and WC. In a similar manner, diabetes can also be predicted with the CUN-BAE index based on previous studies. A cohort study with 6796 participants from Norway found that CUN-BAE had a closer link with diabetes in both sexes than BMI [28]. In line with our results, CUN-BAE identified more people with metabolic syndrome, diabetes, and hypertension than BMI and other indicators in a European cohort of 12,328 participants [27, 39]. There were several potential reasons for this beneficial relationship. First, the accumulation of fat enhances the release of free fatty acids and results in increased lipid accumulation [19]. This induces insulin resistance by activating the diacylglycerol-protein kinase C pathway [20]. Second, excess body fat results in the dysregulation of a wide range of adipokines including classic hormones such as leptin, which may contribute to diabetes via the alteration of glucose metabolism, lipid metabolism and inflammation [17, 18, 41]. Third, individuals who are genetically susceptible to diabetes show a greater risk of obesity because there is a tendency toward insulin resistance in their skeletal muscle and pancreatic islet β-cells [42, 43]. However, another cross-sectional study including 69,388 Chinese participants aged ≥60 years showed that BMI and CUN-BAE were less reliable predictors of male health than WC [43]. This discrepancy may be caused by the diverse ages of the study population, but it could also be a result of the different study methodologies and designs.
Comparisons with other studies and what does the current work add to the existing knowledge
CUN-BAE is a body fat prediction equation that has been proven to be linked to hypertension, cardiovascular events and cardiometabolic risk factors in prior studies [25, 27,28,29]; however, these relationships have only been explored in Caucasian populations. In addition, the predictive potential of CUN-BAE for incident diabetes has not yet been compared with BMI and WC. We first revealed the level of CUN-BAE in a Japanese population. Compared with other studies, we observed that the level of the CUN-BAE index varies across different ethnic groups. The present study showed that the CUN-BAE was 24.96 ± 6.52 in this Japanese population (20.9 ± 4.7 in males and 29.8 ± 4.9 in females), which is similar to findings in a Chinese population [44, 45]. The mean level of CUN-BAE was 29.8 ± 7.8 in a Spanish population (25.4 ± 6.6 in males and 33.5 + 6.7 in females) [40]. These findings are similar to the results of a study by Davila-Batista et al. [46] but higher than the results of a study in South Africa (27.28 ± 8.28) [47]. It is possible that this discrepancy is due to differences in body composition, body size, and body fat distribution among various ethnic groups. Asian individuals tend to be small and have a low BMI, while Caucasian individuals are more likely to be large and muscular with a high BMI. Furthermore, we demonstrate an independent association of CUN-BAE with diabetes and its clinical usefulness for diabetes prediction in an Asian population, providing new evidence for the application and promotion of CUN-BAE in Asian ethnic groups. Moreover, this is the first experiment to find that CUN-BAE exceeds BMI and WC in diabetes prediction, which is beneficial for the accurate and early identification of patients at risk of diabetes and might have potential reference value for the adjustment of treatment strategies.
Study strengths and limitations
There are several advantages in the present study. First, this study is the first longitudinal study that investigated the link between CUN-BAE and diabetes in a Japanese population. Second, we made comparisons with traditional anthropometric indicators, including BMI and WC, to further evaluate the clinical value of the CUN-BAE index. Third, subgroup analysis was conducted to ensure that CUN-BAE and T2DM were associated in a stable manner among different participants.
Nevertheless, several limitations are inherent in the study. First, the findings might be difficult to generalize to other ethnicities, as the present study only considers the Japanese population. Second, HbA1c, FPG, or patient self-reported data were primarily used for diabetes diagnosis, rather than oral glucose tolerance tests (OGTTs), in this study, which may result in an underestimation of the prevalence of diabetes. Third, the CUN-BAE index was evaluated at baseline. Thus, it did not consider the dynamic changes over time, which may profoundly affect the incidence of diabetes. Finally, we could not fully adjust the confounding factors in the original study that could affect the results.
Conclusions
In conclusion, diabetes incidence is significantly correlated with increased adiposity assessed by the CUN-BAE index. The CUN-BAE index is more effective in predicting T2DM than both BMI and WC. It could be employed as a prominent indicator for the early detection and prediction of a high risk of T2DM in clinical practice.
Availability of data and materials
Data for the study can be obtained from the “Dryad” database, which is publicly accessible. (https://datadryad.org/stash/data/set/doi:10.5061/dryad.8q0p192).
Abbreviations
- CUN-BAE:
-
The Clínica Universidad de Navarra-Body Adiposity Estimator index
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-density lipoprotein-cholesterol
- FBG:
-
Fasting blood glucose
- HbA1c:
-
Glycosylated haemoglobin A1c
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- GGT:
-
Gamma-glutamyl transferase
- ROC:
-
Receiver-operating characteristics
- AUC:
-
Area under the curve
- SD:
-
Standard deviation
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- T2DM:
-
Type 2 diabetes mellitus
- NAGALA:
-
NAfld in Gifu Area, Longitudinal Analysis
References
Zhou B, Lu Y, Hajifathalian K, Bentham J, Di Cesare M, Danaei G, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4·4 million participants. Lancet. 2016;387(10027):1513–30.
Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pr. 2022;183:109119.
Chan JCN, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon K, et al. Diabetes in Asia. JAMA. 2009;301(20):2129.
Ramachandran A. Trends in prevalence of diabetes in Asian countries. World J Diabetes. 2012;3(6):110.
Strain WD, Paldánius PM. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc Diabetol. 2018;17(1):57.
Suh S, Kim K. Diabetes and cancer: cancer should be screened in routine diabetes assessment. Diabetes Metab J. 2019;43(6):733.
Lin X, Xu Y, Pan X, Xu J, Ding Y, Sun X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep-Uk. 2020;10(1):14790.
Phillips J, Chen JHC, Ooi E, Prunster J, Lim WH. Global Epidemiology, Health Outcomes, and Treatment Options for Patients With Type 2 Diabetes and Kidney Failure. Front Clin Diabetes Healthc. 2021;2:731574.
Park SK, Ryoo J, Oh C, Choi J, Jung JY. Longitudinally evaluated the relationship between body fat percentage and the risk for type 2 diabetes mellitus: Korean Genome and Epidemiology Study (KoGES). Eur J Endocrinol. 2018;178(5):513–21.
Al-Sulaiti H, Diboun I, Banu S, Al-Emadi M, Amani P, Harvey TM, et al. Triglyceride profiling in adipose tissues from obese insulin sensitive, insulin resistant and type 2 diabetes mellitus individuals. J Transl Med. 2018;16(1):175.
Borga M, West J, Bell JD, Harvey NC, Romu T, Heymsfield SB, et al. Advanced body composition assessment: from body mass index to body composition profiling. J Invest Med. 2018;66(5):1–10.
Miyahira SA, de Azevedo JL, Araújo E. Fuzzy obesity index (MAFOI) for obesity evaluation and bariatric surgery indication. J Transl Med. 2011;9:134.
Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab Syndr Obes. 2022;15:1677–86.
Lear SA, Humphries KH, Kohli S, Chockalingam A, Frohlich JJ, Birmingham CL. Visceral adipose tissue accumulation differs according to ethnic background: results of the Multicultural Community Health Assessment Trial (M-CHAT). Am J Clin Nutr. 2007;86(2):353–9.
Xu S, Ming J, Jia A, Yu X, Cai J, Jing C, et al. Normal weight obesity and the risk of diabetes in Chinese people: a 9-year population-based cohort study. Sci Rep-Uk. 2021;11(1):6090.
De Lorenzo A, Gratteri S, Gualtieri P, Cammarano A, Bertucci P, Di Renzo L. Why primary obesity is a disease? J Transl Med. 2019;17(1):169.
Hauner H. Secretory factors from human adipose tissue and their functional role. Proc Nutr Soc. 2005;64(2):163–9.
Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860–7.
Jung UJ, Choi MS. Obesity and its metabolic complications: the role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int J Mol Sci. 2014;15(4):6184–223.
Yung J, Giacca A. Role of c-Jun N-terminal Kinase (JNK) in Obesity and Type 2 Diabetes. Cells-Basel. 2020;9(3):706.
Gómez-Ambrosi J, Silva C, Galofré JC, Escalada J, Santos S, Gil MJ, et al. Body adiposity and type 2 diabetes: increased risk with a high body fat percentage even having a normal BMI. Obesity. 2011;19(7):1439–44.
Romero-Corral A, Somers VK, Sierra-Johnson J, Korenfeld Y, Boarin S, Korinek J, et al. Normal weight obesity: a risk factor for cardiometabolic dysregulation and cardiovascular mortality. Eur Heart J. 2010;31(6):737–46.
Belarmino G, Horie LM, Sala PC, Torrinhas RS, Heymsfield SB, Waitzberg DL. Body adiposity index performance in estimating body fat in a sample of severely obese Brazilian patients. Nutr J. 2015;14(1):130.
Chambers AJ, Parise E, Mccrory JL, Cham R. A comparison of prediction equations for the estimation of body fat percentage in non-obese and obese older Caucasian adults in the United States. J Nutr Health Aging. 2014;18(6):586–90.
Gómez-Ambrosi J, Silva C, Catalán V, Rodríguez A, Galofré JC, Escalada J, et al. Clinical usefulness of a new equation for estimating body fat. Diabetes Care. 2012;35(2):383–8.
Molina-Luque R, Yañez AM, Bennasar-Veny M, Romero-Saldaña M, Molina-Recio G, López-González Á. A comparison of equation Córdoba for estimation of body fat (ECORE-BF) with other prediction equations. Int J Env Res Pub He. 2020;17(21):7940.
Głuszek S, Ciesla E, Głuszek-Osuch M, Kozieł D, Kiebzak W, Wypchło Ł, et al. Anthropometric indices and cut-off points in the diagnosis of metabolic disorders. PLoS One. 2020;15(6):e235121.
Vinknes KJ, Nurk E, Tell G, Sulo G, Refsum H, Elshorbagy A. The relation of CUN-BAE index and BMI with body fat, cardiovascular events and diabetes during a 6-year follow-up: the Hordaland Health Study. Clin Epidemiol. 2017;9:555–66.
Martín V, Dávila-Batista V, Castilla J, Godoy P, Delgado-Rodríguez M, Soldevila N, et al. Comparison of body mass index (BMI) with the CUN-BAE body adiposity estimator in the prediction of hypertension and type 2 diabetes. BMC Public Health. 2015;16(1):82.
Okamura T, Hashimoto Y, Hamaguchi M, Obora A, Kojima T, Fukui M. Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Int J Obes (Lond). 2019;43(1):139–48.
Carbone S, Del BM, Ozemek C, Lavie CJ. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog Cardiovasc Dis. 2019;62(4):327–33.
Consultation W H O E. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63.
Rodriguez A, Catalan V, Gomez-Ambrosi J, Fruhbeck G. Visceral and subcutaneous adiposity: are both potential therapeutic targets for tackling the metabolic syndrome? Curr Pharm Des. 2007;13(21):2169–75.
Okorodudu DO, Jumean MF, Montori VM, Romero-Corral A, Somers VK, Erwin PJ, et al. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: a systematic review and meta-analysis. Int J Obes (Lond). 2010;34(5):791–9.
Pongchaiyakul C, Nguyen TV, Kosulwat V, Rojroongwasinkul N, Charoenkiatkul S, Pongchaiyakul C, et al. Defining obesity by body mass index in the Thai population: an epidemiologic study. Asia Pac J Clin Nutr. 2006;15(3):293–9.
Rodríguez-Rodríguez E, López-Plaza B, López-Sobaler AM, Ortega RM. Overweight and obesity among Spanish adults. Nutr Hosp. 2011;26(2):355–63.
Wu L, Pu H, Zhang M, Hu H, Wan Q. Non-linear relationship between the body roundness index and incident type 2 diabetes in Japan: a secondary retrospective analysis. J Transl Med. 2022;20(1):110.
Gómez-Ambrosi J, Silva C, Galofré JC, Escalada J, Santos S, Millán D, et al. Body mass index classification misses subjects with increased cardiometabolic risk factors related to elevated adiposity. Int J Obes (Lond). 2012;36(2):286–94.
Suliga E, Ciesla E, Głuszek-Osuch M, Rogula T, Głuszek S, Kozieł D. The usefulness of anthropometric indices to identify the risk of metabolic syndrome. Nutrients. 2019;11(11):2598.
Fuster-Parra P, Bennasar-Veny M, Tauler P, Yañez A, López-González AA, Aguiló A. A comparison between multiple regression models and CUN-BAE equation to predict body fat in adults. PLoS One. 2015;10(3):e122291.
Wu SF, Noren HN, Freeman DW, Mode NA, Zonderman AB, Evans MK. Extracellular vesicles in diabetes mellitus induce alterations in endothelial cell morphology and migration. J Transl Med. 2020;18(1):230.
Malone JI, Hansen BC. Does obesity cause type 2 diabetes mellitus (T2DM)? Or is it the opposite? Pediatr Diabetes. 2019;20(1):5–9.
Bai K, Chen X, Song R, Shi W, Shi S. Association of body mass index and waist circumference with type 2 diabetes mellitus in older adults: a cross-sectional study. BMC Geriatr. 2022;22(1):489.
Chen X, Fan R, Peng F, Liu J, Huang J, Chen Z, et al. Blood pressure and body fat percent in women with NMOSD. Brain Behav. 2019;9(9):e1350.
Guo X, Ding Q, Liang M. Evaluation of eight anthropometric indices for identification of metabolic syndrome in adults with diabetes. Diabetes Metab Syndr Obes. 2021;14:1431–43.
Davila-Batista V, Molina AJ, Vilorio-Marqués L, Lujan-Barroso L, de Souza-Teixeira F, Olmedo-Requena R, et al. Net contribution and predictive ability of the CUN-BAE body fatness index in relation to cardiometabolic conditions. Eur J Nutr. 2019;58(5):1853–61.
Sekgala MD, Opperman M, Mpahleni B, Mchiza ZJ. Anthropometric indices and cut-off points for screening of metabolic syndrome among south African taxi drivers. Front Nutr. 2022;9:974749.
Acknowledgements
Thanks to Okamura for conducting the NAGALA study and sharing the data.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
QP and ZH-F designed the study and wrote the draft. WK-C organized this study and made contributions to the study design and data interpretation. ZJ-C and DX-L were mainly responsible for the analysis of patient data and the revision of the manuscript. JN-Z, HJ-Z and XW-Z participated in the effort to look up pertinent data. The final manuscript was written and approved by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Research Ethics Committee approval was obtained for the NAGALA study from Murakami Memorial Hospital. Data from each participant were used anonymously for the study after informed consent was obtained from each participant.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peng, Q., Feng, Z., Cai, Z. et al. The relationship between the CUN-BAE body fatness index and incident diabetes: a longitudinal retrospective study. Lipids Health Dis 22, 21 (2023). https://doi.org/10.1186/s12944-023-01784-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-023-01784-5