
Abstract
Background
Chronic nonspecific low back pain (cNLBP) is a common health problem worldwide, affecting 65–80% of the population and greatly affecting people’s quality of life and productivity. It also causes huge economic losses. Manual therapy (MT) and therapeutic exercise (TE) are effective treatment options for cNLBP physiotherapy-based treatment. However, the underlying mechanisms that promote cNLBP amelioration by MT or TE are incompletely understood.
Methods
Seventeen recruited subjects were randomly divided into an MT group and a TE group. Subjects in the MT group performed muscular relaxation, myofascial release, and mobilization for 20 min during each treatment session. The treatment lasted for a total of six sessions, once every two days. Subjects in the TE group completed motor control and core stability exercises for 30 min during each treatment session. The motor control exercise included stretching of the trunk and extremity muscles through trunk and hip rotation and flexion training. Stabilization exercises consisted of the (1) bridge exercise, (2) single-leg-lift bridge exercise, (3) side bridge exercise, (4) two-point bird-dog position with an elevated contralateral leg and arm, (5) bear crawl exercise, and (6) dead bug exercise. The treatment lasted for a total of six sessions, with one session every two days. Serum samples were collected from subjects before and after physiotherapy-based treatment for lipidomic and metabolomic measurements.
Results
Through lipidomic analysis, we found that the phosphatidylcholine/phosphatidylethanolamine (PC/PE) ratio decreased and the sphingomyelin/ceramide (SM/Cer) ratio increased in cNLBP patients after MT or TE treatment. In addition, eight metabolites enriched in pyrimidine and purine differed significantly in cNLBP patients who received MT treatment. A total of nine metabolites enriched in pyrimidine, tyrosine, and galactose pathways differed significantly in cNLBP patients after TE treatment during metabolomics analysis.
Conclusion
Our study was the first to elucidate the alterations in the lipidomics and metabolomics of cNLBP physiotherapy-based treatment and can expand our knowledge of cNLBP physiotherapy-based treatment.
Similar content being viewed by others

Introduction
Chronic nonspecific low back pain (cNLBP) is not caused by recognizable pathology; it lasts for more than three months and occurs between the lower rib and the inferior gluteal fold [1]. It is estimated that approximately four out of five people have lower back pain at some time during their lives, and it greatly affects their quality of life, productivity, and ability to work [2].
cNLBP can be caused by many factors, such as lumbar strain, nerve irritation, and bony encroachment. However, the etiology of cNLBP is typically unknown and poorly understood [3]. Medical treatments and physiotherapy are recommended to treat and resolve issues associated with cNLBP [3]. Therapeutic exercise and manual therapy have a lower risk of increasing future back injuries or work absence and are more effective treatment options for chronic pain than medication or surgery, and they can be performed at rehabilitation clinics [4,5,6]. Exercise therapy is a widely used strategy to cope with low back pain that includes a heterogeneous group of interventions ranging from aerobic exercise or general physical fitness to muscle strengthening and various types of flexibility and stretching exercises [7]. Manual therapy is another effective method to deal with low back pain, in which hands are used to apply a force with a therapeutic intent, including massage, joint mobilization/manipulation, myofascial release, nerve manipulation, strain/counter strain, and acupressure [8]. However, the reasons therapeutic exercise and manual therapy ameliorate cNLBP are still unknown.
With the development of lipidomics and metabolomics, many studies have indicated that lipid or metabolite alterations are associated with chronic pain [9, 10]. Lipids, as primary metabolites, are not only structural components of membranes but can also be used as signaling molecules to regulate many physiological activities. For example, fatty acid (FA) chains can be saturated (SFA), monounsaturated (MUFA), or polyunsaturated (PUFA), and the ratio of saturated to unsaturated FAs participates in the regulation of longevity [11]. Phosphatidylcholine (PC) phosphatidylethanolamine (PE) is abundant in membranes. In mammals, cellular PC/PE molar ratios that are out of balance and increase or decrease abnormally can cause diseases [12]. For example, a reduced PC/PE ratio can protect mice against atherosclerosis [13]. Decreasing the PC/PE molar ratio can change the intracellular energy supply by activating the electron transport chain and mitochondrial respiration [14]. Lysophosphatidylcholine (LPC) 16:0 correlated with pain outcomes in a cohort of patients with osteoarthritis [15]. Apart from phospholipids, studies have shown that sphingolipid metabolism also contributes to chronic pain. Increased ceramide and sphingosine-1-phosphate (S1P) are involved in the progression of chronic pain in the nervous system [16]. Previous studies reported that metabolites were also associated with pain. Patients with neuropathic pain showed elevated choline-containing compounds in response to myoinositol [tCho/mI] under magnetic resonance spectroscopy [17]. Flavonoids are the most common secondary plant metabolites used as tranquilizers in folkloric medicine and have been claimed to reduce neuropathic pain [18]. Patients with chest pain and high plasma levels of deoxyuridine, homoserine, and methionine had an increased risk of myocardial infarction [19]. Despite the evidence presented above that pain is associated with specific lipids and metabolites, no studies have shown that MT and TE can relieve cNLBP by altering lipids and metabolites.
In this article, we compared the lipidomics and metabolomics of patients with cNLBP before and after treatment to explore differences in lipids and metabolites correlated with cNLBP physiotherapy-based treatment. The newly found data will expand our knowledge of cNLBP physiotherapy-based treatment.
Material and methods
Participants
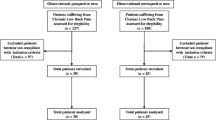
Patients with cNLBP were recruited through advertising. The inclusion criteria were as follows: (1) patients aged between 18 years and 65 years [20]; (2) patients with pain in the area between the lower rib and the inferior gluteal fold; (3) patients with persistent pain > 3 months or intermittent pain > 6 months and having been clinically diagnosed as having cNLBP by two licensed medical doctors in accordance with the diagnostic guidelines published by the American College of Physicians and the American Pain Society [21, 22]; (4) patients with a minimum score of 2 on the Visual Analog Scale (VAS) in the previous week [23]; (5) patients who were right-hand dominant, with no neurological diseases (e.g., traumatic brain injury, or epilepsy), or intracranial lesions; and (6) patients who did not receive pain treatment within the past 3 months.
The exclusion criteria were as follows: (1) patients with radiating pain, menstrual pain, recent/current pregnancy, or postpartum low back pain; (2) patients who suffered known inflammatory disease of the spine, vertebral fracture, severe osteoporosis, autoinflammatory arthritis, and cancer or had significant unexplained weight loss; (3) patients who had cardio-cerebrovascular disease or endocrine disorders; (4) patients with mental illness requiring immediate pharmacotherapy; (5) patients who showed an unwillingness to sign research consent and unwillingness or inability to follow the research protocol; and (6) patients with current alcohol or drug dependence.
All participants were assessed for pain intensity using the visual analog scale (VAS), and serum samples for LC‒MS measurements were collected before and after treatment. The First Affiliated Hospital of Sun Yat-sen University approved the ethical approval document of the study (no. [2019] 408). The recruited subjects signed informed consent forms prior to the experiment.
Therapy of subjects
Seventeen recruited subjects were randomly divided into the MT group and the TE group. Patients in the MT group received manual therapy, and patients in the TE group received therapeutic exercise. Subjects in the manual therapy group were involved in muscular relaxation, myofascial release, and mobilization for 20 min during each session. The treatment lasted for a total of six sessions, once every two days. Subjects in the therapeutic exercise group completed motor control exercise and core stability exercise for 30 min during each session. The motor control exercises included stretching of the trunk and extremity muscles, trunk and hip rotation, and flexion training. Stabilization exercises consisted of the (1) bridge exercise, (2) single-leg-lift bridge exercise, (3) side bridge exercise, (4) two-point bird-dog position elevated contralateral leg and arm, (6) bear crawl exercise, and (7) dead bug exercise. The treatment lasted for a total of six sessions, once every two days.
Lipidomic analysis
Lipid samples were prepared as described by Xuan et al. with some modifications [24]. Briefly, venous blood was collected in heparinization tubes and then centrifuged for 15 min at 2000 g at 4 °C to collect serum. A total of 200 µL serum samples with lipid standards were mixed with 400 µL tert-butyl methyl ether (MTBE) and 80 µL methanol and then vortexed for 30 s. Next, the samples were centrifuged, after which the upper phases were collected, transferred into new tubes, and dried by vacuum evaporation. Samples were reconstituted with 100 µL of methylene chloride:methanol (1:1, v/v).
Lipid analysis was carried out with a Shimadzu LC-30 A (Shimadzu, Kyoto, Japan) coupled with a mass spectrometer (QTRAP 6500, AB SCIEX, Framingham, MA, USA). The chromatographic parameters were as follows: chromatographic column: ACQUITY UPLC® BEH C18 column (2.1 × 100 mm, 1.7 μm, Waters, Milford, MA, USA), volume of injection: 5 µl, flow rate: 0.26 mL/min, oven temperature: 55 °C. The mobile phase included reagent A (acetonitrile:ultrapure water = 60:40, v/v, with 10 mM ammonium acetate) and reagent B (isopropanol:acetonitrile = 90:10, v/v, with 10 mM ammonium acetate). A binary gradient was set as follows: 0–1.5 min, mobile phase including 68% reagent A and 32% reagent B; 1.5–15.5 min, mobile phase including 15% reagent A and 85% reagent B; 15.5–15.6 min, mobile phase including 3% reagent A and 97% reagent B; 15.6–18 min, mobile phase including 3% reagent A and 97% reagent B; 18–18.1 min, mobile phase including 68% reagent A and 32% reagent B; 18.1–20 min, mobile phase including 68% reagent A and 32% reagent B. Electrospray ionization (QTRAP 6500, AB SCIEX, Framingham, MA, USA) was used with the following parameters: ion source voltage was − 4500 or 5500 V, ion source temperature was 600 °C, curtain gas was 20 psi, atomizing gas was 60 psi, and auxiliary gas was 60 psi. Scanning was performed through multiple reaction monitoring (MRM). Samples under test conditions were mixed and used as QC samples for LC‒MS analysis every third sample to correct deviations caused by instrumental drift and evaluate the quality of data.
Metabolomic measurement
Metabolomic samples were prepared as described by Wang et al. [25]. Briefly, venous blood was collected in heparinization tubes and then centrifuged at 8000 g at 4 °C to collect serum. A total of 100 µL of serum sample was mixed with 400 µL of solution (methanol:acetonitrile:ultrapure water = 2:2:1, v/v/v) and then sonicated for 10 min in a 4 °C water bath. Next, the samples were incubated for one hour at − 20 °C and then centrifuged. The supernatant was collected and evaporated by vacuum evaporation. Each sample was resuspended in solution (acetonitrile:ultrapure water, 1:1, v/v).
Metabolomic analysis was carried out with a Shimadzu LC-30 A (Shimadzu, Kyoto, Japan) coupled with a mass spectrometer (QTRAP 4500, AB SCIEX, Framingham, MA, USA). The chromatographic parameters were set as follows: chromatographic column: UPLC BEH Amide column (2.1 × 100 mm, 1.7 μm, Waters, Milford, MA, USA), volume of injection: 5 µl, flow rate: 0.3 mL/min, oven temperature: 55 °C. The mobile phase included reagent A (100% ultrapure water with 0.025 M ammonium hydroxide and 0.025 M ammonium acetate) and reagent B (100% acetonitrile). A binary gradient was set as follows: 0–1 min, mobile phase including of 15% reagent A and 85% reagent B; 1–12 min, mobile phase including of 35% reagent A and 65% reagent B; 12–12.1 min, mobile phase including of 60% reagent A and 40% reagent B; 12.1–15 min, mobile phase including of 60% reagent A and 40% reagent B; 15–15.1 min, mobile phase including of 15% reagent A and 85% reagent B; 15.1–20 min, mobile phase including of 15% reagent A and 85% reagent B. An electrospray ionization (QTRAP 4500, AB SCIEX, Framingham, MA, USA) was used with parameters as follows: ion source voltage was − 4500 or 5500 V, ion source temperature was 600 °C, the ion source voltage was − 4500 or 5500 V, curtain gas was 20 psi, atomizing gas was 60 psi, and auxiliary gas was 60 psi. Scanning was performed via multiple reaction monitoring (MRM). Samples under test conditions were mixed and used as QC samples for LC‒MS analysis every third sample to correct deviations caused by instrumental drift and evaluate the quality of data. After the test, raw data were converted to mzXML format with the web-based tool ProteoWizard and then analyzed for peak alignment, retention time correction, and peak area extraction based on XCMS. Metabolite annotation was carried out based on the online human metabolome database (HMDB, http://www.hmdb.ca) using mass-to-charge ratio information and metabolite structures. Metabolite structures were accurately matched using primary and secondary spectrograms (< 25 ppm).
Statistical analyses
Lipid and metabolite abundance were determined by peak area. Then, data were processed and normalized based on a reference sample (PQN) following the process outlined on the website https://www.metaboanalyst.ca/, which was mainly designed for raw spectra processing and general statistical and functional analysis of targeted metabolomics data [26,27,28]. The maximum covariance between nontreated samples and MT- or ET-treated samples in lipidomic analysis was determined with partial least squares-discriminant analysis (PLS-DA). The maximum covariance between nontreated samples and MT- or ET-treated samples in metabolomic analysis was determined using orthogonal partial least-squares discriminant analysis (OPLS-DA). The correlation between lipid molecules was analyzed with correlation heatmaps. The content difference of lipids in each sample was indicated with hierarchical clustering analysis. Pathway analysis was carried out with the web-based tool METPA.
The raw data were logarithmically transformed and tested for normality before the means were compared between different groups. If normality was assumed, Student’s t test was applied. To visualize the differentiation between different groups, PLS-DA and OPLS-DA were performed using MetaboAnalyst 5.0 (http://www.metaboanalyst.ca/). Data are presented as the mean ± SEM. GraphPad Prism (version 8, GraphPad Software, San Diego, CA, USA) was used to perform statistical analyses between the nontreatment and physiotherapy-based treatment groups using Student’s t test (P < 0.05).
Results
Lipid composition analysis of cNLBP patients before and after manual therapy
We recruited 17 patients with cNLBP whose demographic information is shown in Table 1. The recruited subjects were randomly divided into MT or TE groups, with no significant differences in age, weight, height, BMI, or VAS score between them. We found that MT treatment was effective in alleviating cNLBP (Fig. 1). After treatment, the VAS score decreased in almost the entire MT group (Fig. 1). Serum lipidomics were determined after six MT treatment sessions. Since one participant’s blood sample could not be collected after treatment, there were eight effective participants in the MT group.

Manual therapy and therapeutic exercise were effective in cNLBP amelioration Seventeen patients were randomly divided into two groups: one group received manual therapy, and the other group received therapeutic exercise. VAS was recorded before and after treatment. Asterisks show a significant difference from patients before treatment using Student’s t tests (**P < 0.01)
We completed lipid extraction and performed qualitative analysis. Through lipidomic analysis, we identified 290 lipids, which can be divided into the ten subclasses of phosphatidylcholine (PC), phosphatidylethanolamine (PE), lysophosphatidylcholines (LPC), lysophosphatidylethanolamine (LPE), triacylglycerol (TG), phosphatidylinositol (PI), sphingomyelin (SM), ceramide (Cer), hexosylceramide (HexCer), and fatty acid (FA). As a multivariate statistical analysis, PLS-DA could maximize the distinction and discover different metabolites between groups. We performed PLS-DA analysis with the MetaboAnalyst R software package and found a clear difference in the nontreated group (pink) and MT-treated group (green), suggesting differential lipidomic profiles in cNLBP patients before and after manual therapy (Fig. 2 A). Next, we used Pearson correlation analysis to measure the closeness of different lipids (Fig. 2B). Using volume measurements of lipids, we analyzed the lipidomic composition of cNLBP patients before and after manual therapy and found a decrease in phosphatidylcholine (PC)/phosphatidylethanolamine (PE) molar ratios but an increase in sphingomyelin (SM)/ceramide (Cer) molar ratios in the patients after manual therapy. Meanwhile, there were also decreases in the volumes of fatty acids (FAs) and increases in lysophosphatidylcholine (LPC) and lysophosphatidylethanolamine (LPE) when cNLBP patients were treated with MT (Fig. 3 A). We also generated a heatmap to present the volume of the lipids in each sample (Fig. 3B).

Lipidomic profiles in cNLBP patients before and after treatment with MT. A The PLS-DA analysis of cNLBP patients treated with MT versus the control group. “1” represents the nontreated group, and “2” represents the MT-treated group. B Correlation analysis of the significantly different lipids. Different colors represent the level of Pearson’s correlation coefficient

Lipid identification in cNLBP patients before and after treatment with MT. A The composition of nontreated samples and MT-treated samples based on the volume of lipids in each lipid category. B Hierarchical clustering analysis of the 10 lipids in each sample. For class name, red represents the control group, and green represents the MT-treated group
Lipid composition analysis of cNLBP patients before and after therapeutic exercise (TE)
Therapeutic exercise (TE) is another effective method for improving cNLBP [29]. We found that TE treatment was also effective in alleviating cNLBP (Fig. 1). After treatment, patients’ VAS scores decreased significantly in the TE-treated group (Fig. 1).
We performed lipid extraction from cNLBP patients before and after therapeutic exercise and performed qualitative analysis. PLS-DA results indicated a distinct separation between the nontreated group (pink) and the TE-treated group (green) (Fig. 4A). Pearson correlation analysis showed the closeness of different lipids (Fig. 4B). Based on the volume of lipids, PC/PE molar ratios decreased, while SM/Cer molar ratios increased in the patients after therapeutic exercise. The volume of FA also decreased, while the volume of LPC and LPE increased in cNLBP patients after therapeutic exercise, similar to the results of the MT-treated group. Interestingly, the volume of TG (triacylglycerol) increased in the TE-treated group, while it decreased in the MT-treated group (Fig. 5A). A heatmap was produced to indicate the volume of lipids in the nontreated group (red) and the TE-treated group (green) (Fig. 5B).

Lipidomic profiles in cNLBP patients before and after treatment with TE. A PLS-DA analysis of cNLBP patients treated with TE versus the control group. “1” represents the nontreated group, and “2” represents the TE-treated group. B Correlation analysis of the significantly different lipids. Different colors represent the level of Pearson’s correlation coefficient

Lipid identification in cNLBP patients before and after treatment with TE. A The composition of nontreated samples and TE-treated samples based on the volume of lipids in each lipid category. B Hierarchical clustering analysis of the 10 lipids in each sample. For class name, red represents the control group, and green represents the TE-treated group
Metabolite alterations in cNLBP patients
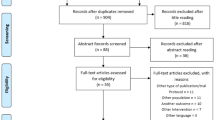
To further identify therapeutic targets for cNLBP physiotherapy-based treatment, we analyzed the metabolome of cNLBP patients before and after treatment. In our sample of patients, the metabolomic analysis annotated and quantified 171 metabolites. Through KEGG-based enrichment analysis, these metabolites were enriched in the metabolism of tryptophan or aspartate, ammonia recycling, the metabolism of methionine or glycine, and serine, among others (Fig. 6A). Combining enrichment and topology analysis, pathway analysis was carried out for all patients. We found a total of 14 pathways that were significantly changed in patients (P value < 0.05). These metabolites mainly belonged to aminoacyl-tRNA biosynthesis; arginine biosynthesis; valine, leucine and isoleucine biosynthesis; amino acid metabolism; pyrimidine and purine metabolism; ascorbate and aldarate metabolism; taurine and hypotaurine metabolism; beta-alanine metabolism; and nicotinate and nicotinamide metabolism (Fig. 6B).

Metabolite alteration in cNLBP patients. A Pathway enrichment analysis revealed different metabolic pathways enriched in cNLBP patients (P value cutoff ≤ 0.05). B The results from the pathway analysis carried out with the web-based tool METPA using the concentrations of metabolites identified in cNLBP patients. Total cmpd, the total number of compounds in the pathway. Hits are the matched number from the uploaded data. Raw P is the original P value. Impact is the pathway impact value calculated from pathway topology analysis
Metabolite profiles of cNLBP patients treated with manual therapy
Serum metabolome analysis was performed on samples collected after MT treatment. Since two participants’ blood samples could not be collected after treatment, there were seven included participants in the MT group for metabolomes. Orthogonal PLS-DA was performed to demonstrate the suitability of the system (Fig. 7A). The orthogonal PLS-DA score plot revealed good discrimination of the MT treatment group against untreated samples (Fig. 7A). MT-treated and nontreated samples were separated with no outliers (Fig. 7A), demonstrating that our metabolomic analysis could sufficiently reflect the metabolic profile alteration of MT treatment. The VIP scores derived from orthogonal PLS-DA, based on the first 20 metabolites with a VIP score > 1.5, revealed uridine, guanosine, kynurenic acid, 2’-deoxyadenosine, allantoin, stachydrine, inosine, uridine 5’-monophosphate, nicotinuric acid, 3,4-dihydroxybenzeneacetic acid, 2’-deoxyuridine, 2’-deoxyguanosine, 4-aminohippuric acid, cytidine, pyridoxylamine, glutathione oxidized, desaminotyrosine, L − valine, N-acetyl-5-hydroxytryptamine, and 4-acetamidobutanoic acid with the highest VIP scores for MT treatment (Fig. 7B). Finally, we screened out metabolites (fold changes > 2) in the MT treatment group compared with the nontreated group, which were cytidine, uridine 5’-monophosphate, kynurenic acid, guanosine, inosine, 2’-deoxyadenosine, and stachydrine (Fig. 8A). The KEGG-based enrichment analysis revealed that these metabolites were significantly enriched in pyrimidine metabolism and purine metabolism pathways, demonstrating that MT treatment relieves pain by altering the metabolism of these two pathways (Fig. 8B).

Discrimination through orthogonal PLS-DA of patients before and after manual therapy analyzed based on metabolomics analysis. A Orthogonal PLS-DA showing score plots comparing nontreated patients (indicated in the legend as 1) and patients after manual therapy (indicated as 2). B Variable importance of projection (VIP) features for the groups from orthogonal PLS-DA analysis

Manual therapy could alter target metabolites in patients with cNLBP. A Comparison of the volumes of cytidine, uridine 5’-monophosphate, kynurenic acid, guanosine, inosine, 2’-deoxyadenosine, stachydrine, and N-acetyl-5-hydroxytryptamine in patients treated with and without manual therapy for 2 weeks. Different letters show a significant difference from nontreated patients using Student’s t test (P < 0.05). B Pathway enrichment analysis revealed that pyrimidine metabolism and purine metabolism pathways were enriched in patients treated with manual therapy (P value cutoff ≤ 0.05)
Metabolite profiles of cNLBP patients treated with therapeutic exercise
We also performed metabolite identification in the serum metabolomes pooled from cNLBP patients treated with TE. Since one participant’s blood sample could not be collected after treatment, there were seven included participants in the TE group for metabolomes. Orthogonal PLS-DA was performed on untreated samples and TE treatment samples. The orthogonal PLS-DA score plot revealed good discrimination between the TE treatment group and the nontreated samples (Fig. 9A). The VIP score > 1.5 derived from orthogonal PLS-DA, based on the first 20 metabolites, revealed liothyronine, 2’-deoxyadenosine, uridine, L − homocystine, N-acetyl-5-hydroxytryptamine, stachydrine, γ-aminobutyric acid, nicotinuric acid, glutaric acid, 2’-deoxyuridine, adenine, N-acetyl-L-aspartic acid, cinnamic acid, cytidine, uridine 5’-monophosphate, D-(-)-mandelic acid, L-cysteine, 4-aminobenzoic acid, 5’-deoxyadenosine, and D-sorbitol with the highest VIP scores for TE treatment (Fig. 9B).

Discrimination through orthogonal PLS-DA of patients before and after therapeutic exercise examined by metabolomic analysis. A Orthogonal PLS-DA showing score plots comparing nontreated patients (indicated in the legend with 1) and patients after therapeutic exercise (indicated with 2). B Variable importance of projection (VIP) features for the groups from orthogonal PLS-DA analysis
Finally, nine metabolites with fold changes > 2 in the TE treatment group were found, including uridine 5’-monophosphate, thymidine, 2’-deoxyadenosine, 5’-deoxyadenosine, N-acetyl-5-hydroxytryptamine, stachydrine, inosine, gallic acid, and γ-aminobutyric acid (Fig. 10A). The KEGG-based enrichment analysis revealed that these nine metabolites were significantly enriched in pyrimidine metabolism, tyrosine metabolism, and galactose metabolism pathways, demonstrating that TE treatment relieves pain by altering the metabolism of these three pathways (Fig. 10B).

Therapeutic exercise could alter target metabolites in patients with cNLBP. A Comparison of the volumes of uridine 5’-monophosphate, thymidine, 2’-deoxyadenosine, 5’-deoxyadenosine, N-acetyl-5-hydroxytryptamine, stachydrine, inosine, gallic acid, and γ-aminobutyric acid in patients treated with therapeutic exercise for two weeks or without therapeutic treatment. Different letters show a significant difference from nontreated patients using Student’s t test (P < 0.05). B Pathway enrichment analysis revealed that pyrimidine metabolism, tyrosine metabolism, and galactose metabolism were enriched in patients treated with therapeutic exercise (P value cutoff ≤ 0.05)
Discussion
Lipids can act as bioactive compounds that play critical roles in signal transduction. The balance of cellular PC/PE molar ratios is crucial to maintain cell survival and participates in the regulation of many diseases. However, PC/PE molar ratios associated with physiotherapy with cNLBP have not been studied. In this study, we found that PC/PE molar ratios decreased in cNLBP patients either treated with MT or treated with TE when compared with control groups, suggesting that PC/PE molar ratios are involved in cNLBP physiotherapy-based treatment. We still do not know the exact reason why decreased PC/PE molar ratios induced by MT or TE can cause cNLBP relief. However, we believe that the most likely explanation is that decreased PC/PE can alter the properties of membranes and inhibit TNFa-induced inflammatory responses significantly, which is an important inducer of sensory nerve growth [30, 31]. Studies have also shown that the growth of sensory nerves into the inner layer of IVDs (intervertebral discs, IVDs) is a potential factor in low back pain [32, 33].
Sphingolipids are another kind of bioactive lipid that can be used as powerful signaling molecules, and dysregulation of sphingolipid metabolism changes is known to have a significant impact on signal transduction [34]. Sphingomyelin (SM) and ceramide (Cer) are the most enriched classes of sphingolipids, and the balance between SM and Cer is associated with human disease. For example, SM/Cer imbalance can promote lipid dysregulation and apoptosis [35]. Studies have shown that altered sphingolipid metabolism causes neuropathic pain in humans [36]. N,N-dimethylsphingosine induces mechanical hypersensitivity, and the SM/Cer ratio is altered in rats with neuropathic pain [37]. There has, however, been no investigation examining whether the changes in the SM/Cer ratio were related to the physiotherapy of cNLBP. In our study, we found that the SM/Cer ratio increased in cNLBP patients treated with MT or TE compared with control groups, suggesting that SM/Cer ratio alteration is involved in cNLBP physiotherapy-based treatment. However, thus far, there has been no study on the mechanism of the SM/Cer ratio in cNLBP. SM can be hydrolyzed to produce biologically active molecules, such as ceramide and sphingosine, which can be used as potent inhibitors of protein kinase C (PKC) [38]. Therefore, SM/Cer ratio alterations can control many signaling pathways related to inflammation through PKC to relieve low back pain, since inflammation is the primary source of low back pain [28, 39]. In addition, SM/Cer ratio alterations can decrease chronic inflammatory responses through ER stress [40].
We further performed metabolome analysis to identify the underlying mechanisms in cNLBP physiotherapy-based treatment through MT or TE. We found that pyrimidine metabolism and purine metabolism pathways related to MT caused cNLBP amelioration, while pyrimidine metabolism, tyrosine metabolism, and galactose metabolism pathways were responsible for TE-generated cNLBP amelioration. There is literature demonstrating that pyrimidines and purine have widespread functions in responding to pain therapeutics [41, 42]. For example, the nucleotides cytidine and uridine are helpful for dealing with low back pain [43]. The amount of tyramine sulphate was significantly lower in pain patients than in control patients [41]. Purine antagonists can reduce chronic pain and inflammatory pain. Adenosine and its analogs have the ability to suppress nociception by activating adenosine receptors [44]. In addition to the pyrimidine pathway, tyrosine metabolism is also associated with pain [45]. In headache patients, tyrosine metabolism levels are abnormal [46]. Tyrosine can be hydrolyzed to DOPA, dopamine (DA), and noradrenaline (NE), which govern pain and vegetative functions [47]. Galactose was not only used as a primary source of energy but also considered a candidate for pharmacological applications [48].
In comparing the lipidomic and metabolomic profiles of patients with cNLBP before and after treatment, we found that alterations in the PC/PE ratio, SM/Cer ratio, and target metabolites may be the cause of cNLBP amelioration by MT or TE. However, the relationship between lipids and target metabolites is still unclear. We still do not know whether lipid alteration affects metabolite volume or whether metabolite volume affects lipid alteration. Many studies have demonstrated that lipids can affect gene expression, which can then alter the level of metabolites [49, 50]. For example, S1P can inhibit the activity of histone deacetylases by binding with HDAC1 and HDAC2 specifically to the epigenetic regulation of gene expression [49]. Lipids can also directly affect the activity of protein kinase C, which is an important downstream target of Cer. They can also modulate pyrimidine biosynthesis [50]. In turn, metabolite alteration can also affect lipid metabolism. For example, prenyloxycoumarin is a secondary metabolite and can be used as a modulator of lipid metabolism [51]. Very-low-density lipoproteins (VLDL) are a risk factor for modic changes. These changes result in low back pain (LBP), and receptors can enhance lipid metabolism and promote the expression of interleukin-33 (IL-33) [9, 52]. More studies are needed, however, to investigate the relationship between lipid metabolism and metabolite metabolism in the process of MT or TE in reducing cNLBP. Our study identified the target lipids and metabolites involved in the improvement of cNLBP treated with MT or TE, which has expanded our knowledge of cNLBP physiotherapy-based treatment.
Study strengths and limitations
The greatest strength of this study is to reveal the possible mechanism of promoting cNLBP amelioration through MT or TE treatment from the perspective of lipidomics and metabolomics in cNLBP patients. However, the experiment only involved with alterations in lipids and metabolites, and the deeper mechanisms of these lipids and metabolites affecting cNLBP physiotherapy-based treatment are uncertain. Therefore, more evidences are needed to explore.
Conclusions and clinical perspective
MT or TE treatment were effective strategies in alleviating cNLBP. The possible mechanism is that MT or TE treatment was able to cause alterations in the lipidomics and metabolomics in cNLBP patients. This study was the first to elucidate cNLBP physiotherapy-based treatment was associated with specific lipids and metabolites. These results indicate that physiotherapy or agents targeting these lipids and metabolites alteration might be useful for treatment of cNLBP.
Availability of data and materials
All data in this study can be obtained from the corresponding author upon request.
References
Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379:482–91.
Kameda T, Fukui S, Tominaga R, Sekiguchi M, Iwashita N, Ito K, Tanaka-Mizuno S, Konno SI. Brain metabolite changes in the anterior cingulate cortex of chronic low back pain patients and correlations between metabolites and psychological state. Clin J Pain. 2018;34:657–63.
Urits I, Viswanath O, Galasso AC, Sottosani ER, Mahan KM, Aiudi CM, Kaye AD, Orhurhu VJ. Platelet-Rich plasma for the treatment of low back Pain: a Comprehensive Review. Curr Pain Headache Rep. 2019;23:52.
Slater SL, Ford JJ, Richards MC, Taylor NF, Surkitt LD, Hahne AJ. The effectiveness of sub-group specific manual therapy for low back pain: a systematic review. Man Ther. 2012;17:201–12.
Hidalgo B, Detrembleur C, Hall T, Mahaudens P, Nielens H. The efficacy of manual therapy and exercise for different stages of non-specific low back pain: an update of systematic reviews. J Man Manip Ther. 2014;22:59–74.
Jones KC, Tocco EC, Marshall AN, Valovich McLeod TC, Welch Bacon CE. Pain education with therapeutic exercise in chronic nonspecific low back pain rehabilitation: a critically appraised topic. J Sport Rehabil. 2020;29:1204–9.
Hayden JA, van Tulder MW, Malmivaara AV, Koes BW. Meta-analysis: exercise therapy for nonspecific low back pain. Ann Intern Med. 2005;142:765–75.
Smith AR. Manual therapy: the historical, current, and future role in the treatment of pain. TheScientificWorldJOURNAL. 2007;7:458986.
Li S, Hua D, Wang Q, Yang L, Wang X, Luo A, Yang C. The role of bacteria and its derived metabolites in chronic pain and depression: recent findings and research progress. Int J Neuropsychopharmacol. 2020;23:26–41.
Reveille JD. Biomarkers in axial spondyloarthritis and low back pain: a comprehensive review. Clin Rheumatol. 2022;41:617–34.
Mutlu AS, Duffy J, Wang MC. Lipid metabolism and lipid signals in aging and longevity. Dev Cell. 2021;56:1394–407.
van der Veen JN, Kennelly JP, Wan S, Vance JE, Vance DE, Jacobs RL. The critical role of phosphatidylcholine and phosphatidylethanolamine metabolism in health and disease. Biochim et Biophys Acta (BBA) - Biomembr. 2017;1859:1558–72.
Zhao Y, Su B, Jacobs RL, Kennedy B, Francis GA, Waddington E, Brosnan JT, Vance JE, Vance DE. Lack of phosphatidylethanolamine N-methyltransferase alters plasma VLDL phospholipids and attenuates atherosclerosis in mice. Arterioscler Thromb Vasc Biol. 2009;29:1349–55.
Birner R, Bürgermeister M, Schneiter R, Daum G. Roles of phosphatidylethanolamine and of its several biosynthetic pathways in Saccharomyces cerevisiae. Mol Biol Cell. 2001;12:997–1007.
Jacquot F, Khoury S, Labrum B, Delanoe K, Pidoux L, Barbier J, et al. Lysophosphatidylcholine 16: 0 mediates chronic joint pain associated to rheumatic diseases through acid-sensing ion channel 3. PAIN. 2022;163:1999–2013.
Langeslag M, Kress M. The ceramide-S1P pathway as a druggable target to alleviate peripheral neuropathic pain. Expert Opin Ther Targets. 2020;24:869–84.
Pfyffer D, Wyss PO, Huber E, Curt A, Henning A, Freund P. Metabolites of neuroinflammation relate to neuropathic pain after spinal cord injury. Neurology. 2020;95:e805–14.
Uddin MS, Mamun AA, Rahman MA, Kabir MT, Alkahtani S, Alanazi IS, Perveen A, Ashraf GM, Bin-Jumah MN, Abdel-Daim MM. Exploring the promise of flavonoids to combat neuropathic pain: from molecular mechanisms to therapeutic implications. Front Neurosci. 2020;14:478.
Aa N, Lu Y, Yu M, Tang H, Lu Z, Sun R, Wang L, Li C, Yang Z, Aa J, et al. Plasma metabolites alert patients with chest pain to occurrence of myocardial infarction. Front Cardiovasc Med. 2021;8:652746.
Meints SM, Mawla I, Napadow V, Kong J, Gerber J, Chan ST, Wasan AD, Kaptchuk TJ, McDonnell C, Carriere J, et al. The relationship between catastrophizing and altered pain sensitivity in patients with chronic low-back pain. Pain. 2019;160:833–43.
Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30:77–94.
van Dieën JH, Reeves NP, Kawchuk G, van Dillen LR, Hodges PW. Motor Control Changes in Low Back Pain: divergence in presentations and mechanisms. J Orthop Sports Phys Ther. 2019;49:370–9.
Price DD. Psychological and neural mechanisms of the affective dimension of pain. Science. 2000;288:1769–72.
Xuan Q, Zheng F, Yu D, Ouyang Y, Zhao X, Hu C, Xu G. Rapid lipidomic profiling based on ultra-high performance liquid chromatography-mass spectrometry and its application in diabetic retinopathy. Anal Bioanal Chem. 2020;412:3585–94.
Wang J, Zhang T, Shen X, Liu J, Zhao D, Sun Y, et al. Serum metabolomics for early diagnosis of esophageal squamous cell carcinoma by UHPLC-QTOF/MS. Metabolomics. 2016;12:116.
Xia J, Psychogios N, Young N, Wishart DS. MetaboAnalyst: a web server for metabolomic data analysis and interpretation. Nucleic Acids Res. 2009;37:W652–60.
Xia J, Wishart DS. Web-based inference of biological patterns, functions and pathways from metabolomic data using MetaboAnalyst. Nat Protoc. 2011;6:743–60.
Pang Z, Zhou G, Ewald J, Chang L, Hacariz O, Basu N, Xia J. Using MetaboAnalyst 5.0 for LC-HRMS spectra processing, multi-omics integration and covariate adjustment of global metabolomics data. Nat Protoc. 2022;17:1735–61.
Dvorak H, Kujat C, Brumitt J. Effect of therapeutic exercise versus manual therapy on athletes with chronic low back pain. J Sport Rehabil. 2011;20:494–504.
Treede I, Braun A, Sparla R, Kuhnel M, Giese T, Turner JR, Anes E, Kulaksiz H, Fullekrug J, Stremmel W, et al. Anti-inflammatory effects of phosphatidylcholine. J Biol Chem. 2007;282:27155–64.
Hayashi S, Taira A, Inoue G, Koshi T, Ito T, Yamashita M, et al. TNF-alpha in nucleus pulposus induces sensory nerve growth: a study of the mechanism of discogenic low back pain using TNF-alpha–deficient mice. Spine. 2008;33:1542–6.
Ohtori S, Inoue G, Miyagi M, Takahashi K. Pathomechanisms of discogenic low back pain in humans and animal models. Spine J. 2015;15:1347–55.
Lim TKY, Anderson KM, Hari P, Di Falco M, Reihsen TE, Wilcox GL, Belani KG, LaBoissiere S, Pinto MR, Beebe DS, et al. Evidence for a role of nerve injury in painful intervertebral disc degeneration: a cross-sectional proteomic analysis of human cerebrospinal fluid. J Pain. 2017;18:1253–69.
Hannun YA, Obeid LM. Sphingolipids and their metabolism in physiology and disease. Nat Rev Mol Cell Biol. 2018;19:175–91.
Mühle C, Reichel M, Gulbins E, Kornhuber J. Sphingolipids in psychiatric disorders and pain syndromes. Handb Exp Pharmacol. 2013;216:431–56.
Dawkins JL, Hulme DJ, Brahmbhatt SB, Auer-Grumbach M, Nicholson GA. Mutations in SPTLC1, encoding serine palmitoyltransferase, long chain base subunit-1, cause hereditary sensory neuropathy type I. Nat Genet. 2001;27:309–12.
Patti GJ, Yanes O, Shriver LP, Courade JP, Tautenhahn R, Manchester M, Siuzdak G. Metabolomics implicates altered sphingolipids in chronic pain of neuropathic origin. Nat Chem Biol. 2012;8:232–4.
Kontny E, Ziółkowska M, Ryzewska A, Maśliński W. Protein kinase c-dependent pathway is critical for the production of pro-inflammatory cytokines (TNF-alpha, IL-1beta, IL-6). Cytokine. 1999;11:839–48.
Klyne DM, Barbe MF, Hodges PW. Systemic inflammatory profiles and their relationships with demographic, behavioural and clinical features in acute low back pain. Brain Behav Immun. 2017;60:84–92.
Choi S, Snider JM, Olakkengil N, Lambert JM, Anderson AK, Ross-Evans JS, Cowart LA, Snider AJ. Myristate-induced endoplasmic reticulum stress requires ceramide synthases 5/6 and generation of C14-ceramide in intestinal epithelial cells. FASEB J. 2018;32:5724–36.
Aghabeigi B, Feinmann C, Glover V, Goodwin B, Hannah P, Harris M, Sandler M, Wasil M. Tyramine conjugation deficit in patients with chronic idiopathic temporomandibular joint and orofacial pain. Pain. 1993;54:159–63.
Jacobson KA, Giancotti LA, Lauro F, Mufti F, Salvemini D. Treatment of chronic neuropathic pain: purine receptor modulation. Pain. 2020;161:1425–41.
Mibielli MAN, Nunes CP, Goldberg H, Buchman L, Oliveira L, Mezitis SGE, Wajnzstajn F, Kaufman R, Nigri R, Cytrynbaum N, et al. Nucleotides cytidine and uridine associated with vitamin B12 vs B-complex vitamins in the treatment of low back pain: the NUBES Study. J Pain Res. 2020;13:2531–41.
Burnstock G. Purinergic receptors and pain. Curr Pharm Des. 2009;15:1717–35.
Brumovsky P, Shi TS, Landry M, Villar MJ, Hokfelt T. Neuropeptide tyrosine and pain. Trends Pharmacol Sci. 2007;28:93–102.
D’Andrea G, Cevoli S, Colavito D, Leon A. Biochemistry of primary headaches: role of tyrosine and tryptophan metabolism. Neurol Sci. 2015;36(Suppl 1):17–22.
D’Andrea G, D’Amico D, Bussone G, Bolner A, Aguggia M, Saracco MG, Galloni E, De Riva V, Colavito D, Leon A, et al. The role of tyrosine metabolism in the pathogenesis of chronic migraine. Cephalalgia. 2013;33:932–7.
Coelho AI, Berry GT, Rubio-Gozalbo ME. Galactose metabolism and health. Curr Opin Clin Nutr Metab Care. 2015;18:422–7.
Fu P, Ebenezer DL, Ha AW, Suryadevara V, Harijith A, Natarajan V. Nuclear lipid mediators: role of nuclear sphingolipids and sphingosine-1-phosphate signaling in epigenetic regulation of inflammation and gene expression. J Cell Biochem. 2018;119:6337–53.
Sigoillot FD, Kotsis DH, Masko EM, Bame M, Evans DR, Evans HI. Protein kinase C modulates the up-regulation of the pyrimidine biosynthetic complex, CAD, by MAP kinase. Front Biosci. 2007;12:3892–8.
Fiorito S, Epifano F, Marchetti L, Palumbo L, Orhan IE, Sharifi-Rad M, Genovese S. Oxyprenylated secondary metabolites as modulators of lipid and sugar metabolism. Curr Top Med Chem. 2022;22:189–98.
Yang X, Chen J, Wang J, Ma S, Feng W, Wu Z, Guo Y, Zhou H, Mi W, Chen W, et al. Very-low-density lipoprotein receptor-enhanced lipid metabolism in pancreatic stellate cells promotes pancreatic fibrosis. Immunity. 2022;55:1185–99.e1188.
Acknowledgements
We would like to thank Guangzhou VeryGenome Technology Co., Ltd. for providing technical support.
Funding
This work was supported by the National Natural Science Foundation of China (82002375).
Author information
Authors and Affiliations
Contributions
QHY and ZZ conceived and designed the experiments. ZZ, CJZ, YLL performed the experiments. ZZ, CHW and QHY analyzed the data. ZZ and QHY wrote the article. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This work was approved by the ethics committee of the First Affiliated Hospital of Sun Yat-sen University (ethics: no. [2019] 408). Written informed consent was obtained from all the participants prior to the experiment.
Consent for publication
Not applicable.
Competing interests
All authors approved the manuscript and declared no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Z., Zhang, C., Li, Y. et al. Lipid and metabolic alteration involvement in physiotherapy for chronic nonspecific low back pain. Lipids Health Dis 21, 125 (2022). https://doi.org/10.1186/s12944-022-01737-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-022-01737-4