
Abstract
Background
Lipid profiles are believed to play an important role in the tumorigenesis and progression of prostate cancer (PCa), but research combining those data is lacking. Therefore, this meta-analysis aims to assess the prognostic role of lipid profiles after RP.
Method
We systematically searched PubMed, Embase, and Cochrane Library Central Register of Controlled Trials for articles evaluating association between lipid profiles and prognosis after RP. Odds ratio (OR) and hazard ratio (HR) of lipid profiles for advanced pathological tumor features and biochemical recurrence (BCR) were extracted and pooled OR and HR were calculated. Newcastle-Ottawa scale was used for study quality assessment and funnel plot was used for evaluating publication bias.
Results
Twelve articles involving 11,108 patients were eventually selected. We found low HDL was associated with more frequent occurrence of pathological T stage (pT) ≥ T3 (pooled OR = 1.29, 95% CI 1.07–1.56) and Gleason score (GS) ≥8 (pooled OR = 1.32, 95% CI 1.02–1.72) after RP. Hypertriglyceridemia was also linked with higher risk of pT ≥ T3 (pooled OR = 1.20, 95% CI 1.01–1.42) and positive surgical margin (PSM) (pooled OR = 1.36, 95% CI 1.11–1.65). However, no significant association was observed between BCR and abnormal lipid profile levels.
Conclusion
Low HDL level was associated with more common occurrence of pT ≥ T3 and GS ≥8, and elevated triglycerides level was linked higher risk of pT ≥ T3 and PSM, but none of the lipid subfractions was correlated with biochemical recurrence after RP.
Similar content being viewed by others


Introduction
Prostate cancer is (PCa) one of the most commonly diagnosed cancer in men worldwide [1]. For localized PCa, radical prostatectomy (RP) has been strongly recommended as a standard treatment option [2, 3]. However, biochemical recurrence (BCR) and aggressive clinicopathological features are not rare after RP [4].
Cholesterol has been confirmed as promising biomarkers of cardiovascular disease [5]. Multiple studies have also investigated the role of serum lipid profiles, including total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL) and triglycerides (TG), in the incidence of PCa and generated conflicting results [6,7,8,9]. A meta-analysis integrated those outcomes and suggested that serum lipid profiles are not associated with PCa risk [10]. Similarly, the prognostic value of lipid profiles regarding BCR and postoperative aggressive clinicopathological features after RP remains controversial [11,12,13,14], but yet no research has combined those data and clearly clarified the prognostic role of lipid profiles after RP.
Therefore, based on those disputed studies, the purpose of the current meta-analysis is to comprehensively evaluate the association between serum lipid profiles with BCR and aggressive clinicopathological features after RP.
Method
Search strategy and study selection
PRISMA guidelines were followed to perform this systematic review and meta-analysis [15, 16]. We systematically searched PubMed, Embase, and Cochrane Library Central Register of Controlled Trials to date using terms including “radical prostatectomy”, “lipid”, “cholesterol”, “high density lipoprotein”, “low density lipoprotein”. “metabolic syndrome”, which may comprise LDL and TG, was also one of our searching terms. The references cited by the finally selected articles were also reviewed.
Studies assessing the association between outcomes post RP and lipid profiles were potentially eligible for inclusion. The detailed inclusion criteria were as following: 1. Patients must be treated with only RP, no radiation therapy or chemotherapy was administrated alongside; 2. Study must evaluate the association between lipid profiles and outcomes after RP; 3. Outcomes must include at least one of positive surgical margin (PSM), lymph node involvement (LNI), Gleason score (GS) on surgical specimen ≥8, pT on surgical specimen ≥T3 and BCR; 4. Lipid profiles must include at least one of TC, LDL, HDL and TG; 5. Data must be presented in the fashion of odds ratio (OR) or hazard ratio (HR); 6. Literature must be published in English. The excluding criteria were: 1. Patients were treated RP and radiation therapy or chemotherapy at the same, or patients were treated with either RP or other treatments, but the data was not distinguishable; 2. Publication not evaluating the association between lipid profiles and outcomes post RP; 3. Other lipid profiles rather than TC, LDL, HDL or TG were used for analysis; 4. Other postoperative outcomes rather than PSM, LNI, GS on surgical specimen ≥8, pT on surgical specimen ≥T3 or BCR were assessed; 5. Data was not presented in the fashion of OR and HR; 5. Literature published in non-English language.
Data analysis
Two investigators independently extracted data from the included articles and all the members of our team resolved the discrepancies by consensus. All the analyses were performed using Review Manager (version 5.3) or STATA (version 12.0).
The primary outcome was the association between each lipid subfraction and each postoperative aggressive pathological outcome. Pooled OR value for abnormal versus normal lipid levels was estimated. Cut-off values for abnormal serum levels were commonly defined as ≥200 mg/dl for TC, ≥130 mg/dl for LDL, ≤40 mg/dl for HDL and ≥ 150 mg/dl for TG according to guidelines [17]. The second outcome was the association between each lipid subfraction and BCR, which was defined as a single prostate-specific antigen (PSA) > 0.2 ng/ml, two consecutive concentrations at 0.2 ng/ml, or secondary treatment for detectable postoperative PSA [11]. Pooled HR value of lipid profiles for BCR was calculated. When a trial presented both univariate and multivariate OR/HR, the latter was extracted for analysis.
Outcomes were taken as significant when the P value for Z test was < 0.05 or no intersection between the middle line of the forest plot and the diamond indicating the pooled effect estimate (OR/HR) happened. Heterogeneity among trials was tested using both I2 test or Q test. An I2 > 50% or Q test reporting P values < 0.1 were considered to denote heterogeneity. Sensitivity analyses were performed through the exclusion of one or more studies suspected of causing heterogeneity. Quality assessment of included studies was performed by two independent reviewers using Newcastle–Ottawa Scale (NOS) [18] and publication bias were assessed using funnel plot. When the two reviewers encountered discrepancies in the outcomes, they resolved those through discussion.
Result
Description of included studies
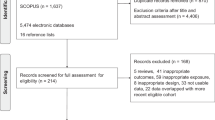
As showed in PRISMA flowchart (Additional file 1: Figure S1, 236 publications were identified and 55 of them were full-text reviewed for eligibility. Eventually, 12 articles involving 11,108 patients met the inclusion criteria and were included in the present study [11,12,13,14, 19,20,21,22,23,24,25,26] (Table 1). Seven of those studies purely emphasized lipid profiles while five other studies focused on MetS and prognosis after RP. All of those studies were published between 2014 and 2018. The cohort size varied from 199 to 3662 with a median follow-up ranged from 14.8 months to 134.4 months. All participants in those studies underwent RP (open, laparoscopic or robot-assisted). Statin use percentage varied from none to 50.7% in eight studies. Cofactors were inconsistently adjusted in multivariate analysis in those original trials. But Age, body mass index (BMI), preoperative PSA, Gleason score and statin were generally adjusted in most selected trials.
Postoperative pathological outcomes
Comparisons of the occurrence of postoperative pathological outcomes between patients with and without abnormal baseline lipid levels were performed in the fashion of pooled OR value. All comparisons were grouped by TC, LDL, HDL and TG. In Fig. 1, patients with abnormal HDL (OR = 1.29, 95% CI 1.07–1.56, P = 0.008) or TG (OR = 1.20, 95% CI 1.01–1.42, P = 0.04) had a significant higher rate of pT ≥3. However, there was no significant difference of pT ≥3 associated with abnormal TC (P = 0.74) or LDL (P = 0.91). Postoperative pathological GS ≥8 was observed to be associated with abnormal HDL (OR = 1.32, 95% CI 1.02–1.72, P = 0.04) and TG (OR = 1.20, 95% CI 1.01–1.42, P = 0.04) (Fig. 2). Figure 3 and Fig. 4 showed that patients with abnormal lipid profile levels had generally similar risk of LNI and PSM. The only exception was that abnormal TG level was linked [12] with higher risk of PSM (OR = 1.36, 95% CI 1.11–1.65, P = 0.003).

Pooled odd ratios of abnormal lipid profiles levels for pT ≥ T3 after radical prostatectomy

Pooled odd ratios of abnormal lipid profiles levels for GS ≥8 after radical prostatectomy

Pooled odd ratios of abnormal lipid profiles levels for LNI after radical prostatectomy

Pooled odd ratios of abnormal lipid profiles levels for PSM after radical prostatectomy
Biochemical recurrence
Figure 5 displayed the adjusted pooled HR values of abnormal versus normal lipid profile levels for BCR. Several studies indicated lipid subfractions could lower the risk of BCR (adjusted HR = 0.22, 95% CI 0.05–0.94 of TC (Kang [12]), adjusted HR = 0.41, 95% CI 0.21–0.79 of HDL (Wettstein [13]), and adjusted HR = 0.62, 95% CI 0.45–0.86 of TG (Bhindi [22])). However, the pooled HR showed that, compared to normal levels, abnormal lipid profile levels led to a generally similar risk of BCR (TC: P = 0.66; LDL: P = 0.62; HDL: P = 0.50; TG: P = 0.69).

Pooled hazard ratios of abnormal lipid profiles levels for BCR after radical prostatectomy
Quality assessment and publication bias
The NOS for non-randomized studies was employed to evaluate the quality of the data and the risk of bias. The selection, compatibility, and outcome of those studies were assessed. Each study meeting one of the numbered items was awarded one star, with a possible maximum of nine stars awarded to a single study. Studies awarded at least seven stars were defined as high quality. Additional file 1: Table S1 summarized the outcomes of quality assessment. Accordingly, all of the included studies were of a relatively high quality. Funnel plots were also presented in supplementary materials and no evident publication bias were observed (Figure S2-S6).
Discussion
The current meta-analysis demonstrated low HDL was associated with more frequent occurrence of pathological T stage (pT) ≥ T3 (OR = 1.29, 95% CI 1.07–1.56, P = 0.008) and Gleason score (GS) ≥8 (OR = 1.32, 95% CI 1.02–1.72, P = 0.04) after RP. Hypertriglyceridemia was also linked with higher risk of pT ≥ T3 (OR = 1.20, 95% CI 1.01–1.42, P = 0.04) and positive surgical margin (PSM) (OR = 1.36, 95% CI 1.11–1.65, P = 0.04). However, no significant association was observed between BCR and abnormal lipid profile levels. Despite that researchers have conducted multiples studies, the role of lipid profiles in PCa still remains unclear. A recent meta-analysis suggested that serum TC, HDL, LDL and TG may not be associated with risk of overall PCa or high-grade PCa [10]. But opposite argument that metabolic syndrome (MetS), of which hypertriglyceridemia and low HDL levels may also be components [27], was associated with risk of overall PCa, in particularly high-grade PCa was proposed by Gacci [28]. Moreover, they also claimed MetS was linked with advanced tumor features and BCR. While several original researches presented controversial outcomes, data regarding prognostic value of lipid profiles after RP remains limited. To our knowledge, the current comprehensive systematic review and meta-analysis is the first to evaluate data about the prognostic value of lipid profiles after RP.
A range of studies investigated the potential mechanisms behind lipid profiles and PCa. As an immunocompetent organ, the prostate gland contains lymphocytes, macrophage and granulocytes and is able to secret various cytokine, chemokine and growth factors. Hypotheses including inflammation, membrane organization and effects on cell proliferation have been introduced [29,30,31,32,33]. Zhuang [29] and Solomon [30] used a xenograft model and observed hypercholesterolemia could accelerate the prostatic tumor growth. Furthermore, Llaverias also argued that hypercholesterolemia could lead to increased prostatic tumor volume and progression and metastases [31]. Some experiments also proved the involvement of cholesterol in element controlling signaling events of PCa cells [29, 32, 33]. In summary, it is feasible to assume that faster growing PCa cells have higher consumption of cholesterol. Thus, our outcomes that abnormally high levels of cholesterol or TG promote more advanced pathologic tumors features after RP looks reasonable. A cohort study supporting this hypothesis by Schnoeller [34] defined patients with pT3–4 and/or pN+ and/or GS ≥8 after RP as high-risk and showed hypercholesterolemia was a risk factor of high-risk PCa (OR = 2.01, P < 0.001). Using similar settings, Zhao [35] reported low level of HDL was attributable to high-risk PCa. Not only that, abnormal LDL levels could also lead to higher risk of BCR, claimed by Macleod [36]. Even though, there is still a lack of definitive conclusion between lipid profiles and PCa pathogenesis. Therefore, high-quality translational research and randomized control trials are further needed.
Known as an important cholesterol-controlling medicine, statin was believed to have contrast effect to cholesterol on PCa and commonly used. A flaw of our study was that data of statin use at baseline was not complete and we could not factor statin use into meta-analysis. However, evidence indicated that statin use had no significant association with BCR after RP [21, 26]. Recent studies by Murtola, Wettstein and Zhang also confirmed statin use was not an independent risk factor of advanced pathologic features or BCR after RP [6, 13, 14]. Moreover, three meta-analyses supported these conclusion by demonstrating that statin use was not associated with either PCa risk [37] or BCR [38, 39]. What is more, a Lancet study even revealed there was no association between reduction of LDL by statin therapy with overall cancer incidence [40]. Therefore, it’s feasible to assume that the deficit of the data of statin use would not substantially affect our analysis.
For the first time, our study included 12 articles related to the prognostic value of lipid profiles after RP and perform quantitative analysis. Notably, to make our outcomes more reliable, we did not only include studies purely assessing lipid profiles, but also selected available MetS researches. However, our study should not interpret without limitation. First, baseline cofactors (age, BMI, race, PSA level, biopsy Gleason score and etc.) were major concerns that might influence our outcomes. Although instead of performing a crude analysis using the number of events of advanced pathological outcomes and BCR, we primarily extracted the adjusted OR and HR, but the cofactors adjusted in those studies were ununiformed, leading to a negative effect on the accuracy. Furthermore, this could also be the major reason causing the substantial heterogeneity in part of our analyses. Second, given that no related randomized controlled trials have been conducted, we systematically searched the mainstream database but could only include prospective and retrospective studies. It’s noted although these selected studies were not highest-level evidence, but all variables and outcomes were recorded pre- or after surgery rather than recalled by patients. Thus, recall bias could be avoided. Third, data of some important outcomes including overall mortality and cancer-specific mortality were not reported in those studies and we were also unable to perform further analysis.
On the basis of existed original studies, the aim of our study is to maximally discriminate the prognostic value of lipid profiles after RP. Our data should be carefully assessed in decision-making of treatment and follow-up. However, it is obvious that more high-quality researches, in particular randomized controlled trials and basic research, are warranted to verify our findings. Future studies should evaluate the prognostic value of lipid profile of not only pathologic outcomes but also oncologic outcomes. Also, considering that GS 3 + 4 and GS4 4 + 3 have been categorized differently, it would be meaningful for future studies to put more effort into this issue.
Conclusion
In this meta-analysis, we found that low HDL level (≤40 mg/dl) was associated with pT ≥ T3 and GS ≥8 after RP, and we also found that elevated serum TG level (≥150 mg/dl) was linked with pT ≥ T3 and PSM. There was no significant correlation between other abnormal lipid subfractions levels with advanced pathologic features or BCR after RP.
Take home message
-
1.
Our meta-analysis is the first to evaluate the association between lipid profiles and prognosis after radical prostatectomy
-
2.
Elevated TC level was associated with LNI and pT ≥ T3.
-
3.
Elevated triglycerides level was linked with pT ≥ T3.
-
4.
Lipid profiles were not correlated with biochemical recurrence.
Abbreviations
- BCR:
-
Biochemical recurrence
- BMI:
-
Body mass index
- GS:
-
Gleason score
- HDL:
-
High-density lipoprotein
- HR:
-
Hazard ratio
- LDL:
-
Low-density lipoprotein
- LNI:
-
Lymph node involvement
- MetS:
-
Metabolic syndrome
- NOS:
-
Newcastle-Ottawa scale
- OR:
-
Odds ratio
- PCa:
-
Prostate cancer
- PSA:
-
Prostate-specific antigen
- PSM:
-
Positive surgical margin
- RP:
-
Radical prostatectomy
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67:7–30.
Bill-Axelson A, Holmberg L, Garmo H, Rider JR, Taari K, Busch C, Nordling S, Haggman M, Andersson SO, Spangberg A, et al. Radical prostatectomy or watchful waiting in early prostate cancer. N Engl J Med. 2014;370:932–42.
EAU Guidelines. Edn. Presented at the EAU annual congress Barcelona 2019. ISBN 978-94-92671-04-2.
Isbarn H, Wanner M, Salomon G, Steuber T, Schlomm T, Kollermann J, Sauter G, Haese A, Heinzer H, Huland H, Graefen M. Long-term data on the survival of patients with prostate cancer treated with radical prostatectomy in the prostate-specific antigen era. BJU Int. 2010;106:37–43.
Chandra A, Rohatgi A. The role of advanced lipid testing in the prediction of cardiovascular disease. Curr Atheroscler Rep. 2014;16:394.
Murtola TJ, Kasurinen TVJ, Talala K, Taari K, Tammela TLJ, Auvinen A. Serum cholesterol and prostate cancer risk in the Finnish randomized study of screening for prostate cancer. Prostate Cancer Prostatic Dis. 2018.
Mondul AM, Weinstein SJ, Virtamo J, Albanes D. Serum total and HDL cholesterol and risk of prostate cancer. Cancer Causes Control. 2011;22:1545–52.
Mondul AM, Clipp SL, Helzlsouer KJ, Platz EA. Association between plasma total cholesterol concentration and incident prostate cancer in the CLUE II cohort. Cancer Causes Control. 2010;21:61–8.
Masko EM, Allott EH, Freedland SJ. The relationship between nutrition and prostate cancer: is more always better? Eur Urol. 2013;63:810–20.
YuPeng L, YuXue Z, PengFei L, Cheng C, YaShuang Z, DaPeng L, Chen D. Cholesterol levels in blood and the risk of prostate Cancer: a meta-analysis of 14 prospective studies. Cancer Epidemiol Biomark Prev. 2015;24:1086–93.
Allott EH, Howard LE, Cooperberg MR, Kane CJ, Aronson WJ, Terris MK, Amling CL, Freedland SJ. Serum lipid profile and risk of prostate cancer recurrence: results from the SEARCH database. Cancer Epidemiol Biomark Prev. 2014;23:2349–56.
Kang M, Jeong CW, Ku JH, Kwak C, Kim HH. Hypertriglyceridemia is a potential preoperative predictor for biochemical recurrence after radical prostatectomy. PLoS One. 2015;10:e0122438.
Wettstein MS, Saba K, Umbehr MH, Murtola TJ, Fankhauser CD, Adank JP, Hofmann M, Sulser T, Hermanns T, Moch H, et al. Prognostic role of preoperative serum lipid levels in patients undergoing radical prostatectomy for clinically localized prostate Cancer. Prostate. 2017;77:549–56.
Zhang GM, Qin XJ, Zhang HL, Xiao WJ, Zhu Y, Gu CY, Dai B, Shi GH, Ye DW. Serum lipid profiles: novel biomarkers predicting advanced prostate cancer in patients receiving radical prostatectomy. Asian J Androl. 2015;17:239–44.
McInnes MDF, Moher D, Thombs BD, McGrath TA, Bossuyt PM, Clifford T, Cohen JF, Deeks JJ, Gatsonis C, Hooft L, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. Jama. 2018;319:388–96.
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1–12.
Third Report of the National Cholesterol Education Program (NCEP). Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation. 2002;106:3143–421.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–5.
Salgado-Montilla J, Soto Salgado M, Surillo Trautmann B, Sanchez-Ortiz R, Irizarry-Ramirez M. Association of serum lipid levels and prostate cancer severity among Hispanic Puerto Rican men. Lipids Health Dis. 2015;14:111.
Rantaniemi L, Tammela TLJ, Kujala P, Murtola TJ. Blood cholesterol, tumor clinical characteristics and risk of prostate cancer progression after radical prostatectomy. Scand J Urol. 2018;52:269–76.
Ohno Y, Ohori M, Nakashima J, Okubo H, Satake N, Hashimoto T, Tachibana M. Association between preoperative serum total cholesterol level and biochemical recurrence in prostate cancer patients who underwent radical prostatectomy. Mol Clin Oncol. 2016;4:1073–7.
Bhindi B, Xie WY, Kulkarni GS, Hamilton RJ, Nesbitt M, Finelli A, Zlotta AR, Evans A, van der Kwast TH, Alibhai SM, et al. Influence of metabolic syndrome on prostate Cancer stage, grade, and overall recurrence risk in men undergoing radical prostatectomy. Urology. 2016;93:77–85.
Colicchia M, Morlacco A, Rangel LJ, Carlson RE, Dal Moro F, Karnes RJ. Role of metabolic syndrome on perioperative and oncological outcomes at radical prostatectomy in a low-risk prostate Cancer cohort potentially eligible for active surveillance. Eur Urol Focus. 2018.
Lebdai S, Mathieu R, Leger J, Haillot O, Vincendeau S, Rioux-Leclercq N, Fournier G, Perrouin-Verbe MA, Doucet L, Azzouzi AR, et al. Metabolic syndrome and low high-density lipoprotein cholesterol are associated with adverse pathological features in patients with prostate cancer treated by radical prostatectomy. Urol Oncol. 2018;36:80.e17–24.
Post JM, Beebe-Dimmer JL, Morgenstern H, Neslund-Dudas C, Bock CH, Nock N, Rundle A, Jankowski M, Rybicki BA. The metabolic syndrome and biochemical recurrence following radical prostatectomy. Prostate Cancer. 2011;2011:245642.
Shiota M, Yokomizo A, Takeuchi A, Imada K, Kiyoshima K, Inokuchi J, Tatsugami K, Naito S. The feature of metabolic syndrome is a risk factor for biochemical recurrence after radical prostatectomy. J Surg Oncol. 2014;110:476–81.
Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, Smith SC Jr. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; National Heart, Lung, and Blood Institute; American Heart Association; world heart federation; international atherosclerosis society; and International Association for the Study of obesity. Circulation. 2009;120:1640–5.
Gacci M, Russo GI, De Nunzio C, Sebastianelli A, Salvi M, Vignozzi L, Tubaro A, Morgia G, Serni S. Meta-analysis of metabolic syndrome and prostate cancer. Prostate Cancer Prostatic Dis. 2017;20:146–55.
Zhuang L, Kim J, Adam RM, Solomon KR, Freeman MR. Cholesterol targeting alters lipid raft composition and cell survival in prostate cancer cells and xenografts. J Clin Invest. 2005;115:959–68.
Solomon KR, Pelton K, Boucher K, Joo J, Tully C, Zurakowski D, Schaffner CP, Kim J, Freeman MR. Ezetimibe is an inhibitor of tumor angiogenesis. Am J Pathol. 2009;174:1017–26.
Llaverias G, Danilo C, Wang Y, Witkiewicz AK, Daumer K, Lisanti MP, Frank PG. A Western-type diet accelerates tumor progression in an autochthonous mouse model of prostate cancer. Am J Pathol. 2010;177:3180–91.
Graff JR, Konicek BW, McNulty AM, Wang Z, Houck K, Allen S, Paul JD, Hbaiu A, Goode RG, Sandusky GE, et al. Increased AKT activity contributes to prostate cancer progression by dramatically accelerating prostate tumor growth and diminishing p27Kip1 expression. J Biol Chem. 2000;275:24500–5.
El Sheikh SS, Domin J, Abel P, Stamp G, Lalani el N. Phosphorylation of both EGFR and ErbB2 is a reliable predictor of prostate cancer cell proliferation in response to EGF. Neoplasia. 2004;6:846–53.
Schnoeller TJ, Jentzmik F, Schrader AJ, Steinestel J. Influence of serum cholesterol level and statin treatment on prostate cancer aggressiveness. Oncotarget. 2017;8:47110–20.
Zhao R, Cheng G, Wang B, Qin C, Liu Y, Pan Y, Wang J, Hua L, Zhu W, Wang Z. BMI and serum lipid parameters predict increasing risk and aggressive prostate cancer in Chinese people. Oncotarget. 2017;8:66051–60.
Macleod LC, Chery LJ, Hu EY, Zeliadt SB, Holt SK, Lin DW, Porter MP, Gore JL, Wright JL. Metabolic syndrome, dyslipidemia and prostate cancer recurrence after primary surgery or radiation in a veterans cohort. Prostate Cancer Prostatic Dis. 2015;18:190–5.
Bansal D, Undela K, D'Cruz S, Schifano F. Statin use and risk of prostate cancer: a meta-analysis of observational studies. PLoS One. 2012;7:e46691.
Mass AY, Agalliu I, Laze J, Lepor H. Preoperative statin therapy is not associated with biochemical recurrence after radical prostatectomy: our experience and meta-analysis. J Urol. 2012;188:786–91.
Scosyrev E, Tobis S, Donsky H, Wu G, Joseph J, Rashid H, Messing E. Statin use and the risk of biochemical recurrence of prostate cancer after definitive local therapy: a meta-analysis of eight cohort studies. BJU Int. 2013;111:E71–7.
Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, Voysey M, Gray A, Collins R, Baigent C. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–90.
Acknowledgements
The authors acknowledge Ian Charles Tobias for reviewing the manuscript. We also thank the dedicated researchers who contributed the explore data for us.
Funding
This research is supported by the National key research and development program of China (Grant No. SQ2017YFSF090096), the Prostate Cancer Foundation Young Investigator Award 2013, the National Natural Science Foundation of China (Grant No. 81300627, 81370855, 81702536, 81770756), Programs from Science and Technology Department of Sichuan Province (Grant No. 2014JY0219 and 2017HH0063) and Young Investigator Award of Sichuan University 2017 (2017SCU04A17).
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Author information
Authors and Affiliations
Contributions
QW, JZA, LY: Project designation, public funding. XNZ, XH, HX: Acquisition of data, Analysis and interpretation of data; XNZ, XH: Drafting of manuscript. XNZ, QW, LY: Critical revision of the manuscript for important intellectual content. XZ had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Quality assessment of the included studies by Newcastle-Ottawa Scale. Figure S1. PRISMA flowchart of literature selection. Figure S2. Publication bias of data for lipid profiles and pathological T stage ≥T3 after radical prostatectomy. Figure S3. Publication bias of data for lipid profiles and Gleason score ≥ 8 after radical prostatectomy. Figure S4. Publication bias of data for lipid profiles and lymph node involvement after radical prostatectomy. Figure S5. Publication bias of data for lipid profiles and positive surgical margin after radical prostatectomy. Figure S6. Publication bias of data for lipid profiles and biochemical recurrence after radical prostatectomy. (DOCX 227 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Zheng, X., Han, X., Xu, H. et al. Prognostic value of lipid profiles after radical prostatectomy: a systematic review and meta-analysis. Lipids Health Dis 18, 124 (2019). https://doi.org/10.1186/s12944-019-1068-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-019-1068-6