
Abstract
Background
Effects of simvastatin on serum level of adiponectin, a protein conferring benefits in both cardiovascular and metabolic system, are not fully determined.
Methods
A meta-analysis of randomized controlled trials (RCTs) was performed. Studies were identified by searching of Pubmed, Embase, and the Cochrane Library databases. Heterogeneity among the RCTs was determined by Cochrane’s Q test and I2 statistics. Meta-analysis was performed with random-effect model or fixed-effect model according to the heterogeneity. Meta-regression and subgroup analyses were performed to analyze the source of heterogeneity.
Results
Twelve RCTs with 16 comparisons and 1042 patients were included. Overall, serum adiponectin was not significantly affected by simvastatin (WMD: 0.42 μg/mL; 95% CI, -0.66–1.50 μg/mL). However, significant heterogeneity was detected (Cochrane’s Q test: p < 0.01; I2 = 83%). Subsequent meta-regression analyses indicated that treatment duration was a significant determinant of the effects of simvastatin treatment on serum adiponectin (Coefficient 0.04, p = 0.03). Subgroup analyses demonstrated that simvastatin treatment was associated with increased adiponectin in studies with treatment duration of 12 weeks (WMD: 3.65 μg/mL; p < 0.01), but not in studies with treatment duration of ≤ 8 weeks (WMD: -0.20 μg/mL; p = 0.38). The different between the two stratums was significant (p < 0.01).
Conclusions
Treatment with simvastatin of 12 weeks may increase the serum level adiponectin in patients at risk for cardiovascular diseases, but not for the short term treatment of ≤ 8 weeks.
Similar content being viewed by others


Background
Accumulating evidence from previous clinical trials has confirmed the role of statins, a class of medications used to lower low-density-lipoprotein cholesterol (LDL-C) levels, as the cornerstone for the primary and secondary prevention of cardiovascular diseases [1, 2]. The subsequent studies regarding the mechanisms of statins indicate that many other potential mechanisms contribute to the benefits of statins in patients at risk for cardiovascular diseases (CVDs), such as anti-inflammation, anti-oxidation, and stabilization of the atherosclerotic plaques [3]. Simvastatin, as a representative medication of the first generation statins, has become one of the most commonly used statins for the treatment of hypercholesterolemia and dyslipidemia [4, 5]. The efficacy and safety of this medication have been well established in previous clinical trials [6]. Therefore, further elucidation of its potential therapeutic mechanisms in patients with cardiovascular diseases other than lipids-lowering is of significance. Recent studies have suggested that simvastatin may have influence on glucose metabolic pathways, such as glucose transport, insulin secretion, and insulin resistance [7]. However the potential mechanisms underlying these effects remain to be determined.
Adiponectin is a protein that is synthesized in adipose tissue and exerts both the cardiovascular and metabolic benefits [8, 9]. Previous experimental studies suggest that the beneficial effects of adiponectin include multiple mechanisms, such as anti-inflammatory, anti-oxidant, anti-atherogenic, and anti-thrombotic, as well as improving insulin resistance and anti-diabetes [10]. Consistently, higher plasma level of adiponectin has been related to the decreased risks of CVDs and diabetes mellitus (DM) [11, 12], suggesting the potential role of adiponectin as an important target for the prevention and treatment of CVDs and DM. Previous studies have suggested that simvastatin treatment may affect serum level of adiponectin [13–24]. However, these studies are generally of limited scale and results of these studies are not always consistent. Therefore, in this study, we performed a meta-analysis to evaluate the effect of simvastatin on serum level adiponectin. The results of our study may be of significance to further elucidate the potential mechanisms of potential influence of simvastatin on cardiovascular and metabolic systems.
Methods
Database searching
This systematic review and meta-analysis was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [25] and the Cochrane’s Handbook of Systematic Review and Meta-analyses [26]. We searched the Pubmed, Embase, and Cochrane Library databases with the words “simvastatin” paired with “adiponectin”, which were limited to studies in humans. The final search was completed on Nov 20th, 2016. The references of the original studies were manually screened for possible relevant studies.
Inclusion and exclusion criteria
In accordance with the aim of the meta-analysis, studies were included if they met all of the following criteria: (a) designed as RCTs and published as full-length article in English; (b) included participants randomized to simvastatin (with no limitations to the dose and treatment duration) or control group; (c) circulating adiponectin levels were reported; and (d) data (means and standard deviations [SDs]) regarding changes of adiponectin from baseline were reported or could be calculated. Reviews, nonhuman studies, observational studies without longitudinal follow-up, cross-sectional studies, duplicate publications, and studies in which changes of adiponectin were not reported or unavailable were excluded.
Data extraction and quality evaluation
The database searching, data extraction and study quality evaluation were independently performed by two authors (WC and ZH), and the discrepancies were resolved by consensus. For studies with more than one intervention group (e.g. different statin dosages), multiple comparisons were considered and the controls were split into multiple groups to overcome a unit of analysis error [26]. Data regarding study design, patient characteristics (health status, number of participants, mean age, gender, mean body mass index [BMI]), intervention strategies (dosages, and treatment durations), adiponectin measurement methods and the type of adiponectin measured were extracted. The seven domains of the Cochrane Risk of Bias Tool was applied to evaluate the quality of the included RCTs, which addressing aspects of sequence generation, allocation concealment, participant and personnel blinding, outcome assessor blinding, incomplete outcome data, selective outcome reporting, and other potential threats to validity.
Statistics
The main outcome for the current meta-analysis was the change of serum adiponectin level between baseline and endpoint in response to statin therapy as compared with controlled. The pooled effect was expressed as weighted mean difference (WMD) with 95% confidence intervals (CI). Heterogeneity among the included studies was formally tested using Cochrane’s Q test, and significant heterogeneity was considered if p values < 0.10 [26]. The I2 statistic, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance, was also examined, and values of I2 > 50% indicated significant heterogeneity [27]. A random-effect was applied to estimate the overall outcome if I2 > 50%, otherwise, a fixed-effect model was used. To identify whether differences in study characteristics were potential contributors to heterogeneity, we performed univariate meta-regression and subgroup analyses subsequently, and predefined study characteristics included age, gender, mean BMI, and dosage and treatment duration of simvastatin. Potential publication bias was assessed with a funnel plot and Egger’s regression asymmetry test [28]. P values were two-tailed and statistical significance was set at 0.05. The meta-analysis and statistical analysis were performed with RevMan software (Version 5.3; Cochrane Collaboration, Oxford, UK) and Stata software (version 12.0; Stata Corporation, College Station, TX, USA).
Results
Database searching
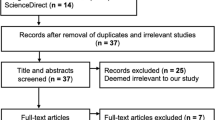
The process of database searching and study identification was shown in Fig. 1. Briefly, 174 records were retrieved after initial database searching and 12 RCTs [13–24] were finally included. Two of the included studies [18, 21] had more than one interventional arm with different doses of simvastatin, and multiple comparisons were included.

Process of literature searching
Study characteristics and quality evaluation
The characteristics of the included studies were summarized in Table 1. Briefly, these RCTs generally included patients at risk for CVDs, such as those with hypertension, hypercholesterolemia, diabetes, or carotid atherosclerosis. The mean ages of the patients varied from 45 to 60 years, and the BMI ranged from 24 to 39 Kg/m2. Simvastatin was administered in the treatment group with the doses of 10, 20, 40 and 80 mg/d, and durations of 2 to 12 weeks. The serum adiponectin was measured via enzyme-linked immunosorbent assay in most of the included studies, and the total circulating adiponectin levels were measured in all of the included studies. The quality of the study as evaluated by the Cochrane risk of biases tool was presented in Table 2, and the overall quality of the included studies were moderate.
Effects of simvastatin treatment on serum adiponectin
Overall, 16 comparisons with 594 patients in the simvastatin group and 448 in the control group were included in the meta-analysis. Significant heterogeneity was detected (Cochrane’s Q test: p < 0.01; I2 = 83%); therefore, the random-effect model was applied. The pooled results indicated that serum adiponectin was not significantly affected by simvastatin (WMD: 0.42 μg/mL; 95% CI, -0.66–1.50 μg/mL; p = 0.45; Fig. 2). Pooled results with only double-blinded, placebo-controlled trials [13–16, 18, 23] retrieved similar results (WMD: -0.15 μg/mL; 95% CI, -0.64–0.34 μg/mL; p = 0.54).

Forest plot for the estimation of the effect of simvastatin treatment of serum adiponectin stratified by the treatment duration
Treatment duration and the effects of simvastatin treatment on serum adiponectin
In view of significant heterogeneity among the included, we subsequently performed univariate meta-regression analyses to explore the potential source of heterogeneity. We found that simvastatin treatment duration was a significant determinant of the effects of simvastatin treatment on serum adiponectin (Coefficient 0.04, p = 0.03; Table 3), but were not for other potential variables such as age, gender, BMI, or dosages of simvastatin. Specifically, longer treatment duration was associated with more remarkable increment of adiponectin following simvastatin, which may partly explain the heterogeneity. This was confirmed by results of subgroup analyses which demonstrated that simvastatin treatment was associated with increased adiponectin in studies with treatment duration of 12 weeks (WMD: 3.65 μg/mL; 95% CI, 2.14–5.16 μg/mL; p < 0.01; I2 = 48%; Fig. 2), but not in studies with treatment duration of ≤ 8 weeks (WMD: -0.20 μg/mL; 95% CI, -0.65–0.25 μg/mL; p = 0.38; I2 = 0%; Fig. 2). The different between the two stratums was significant (p < 0.01).
Publication bias
No significant publication biases were indicated by the funnel plots (Fig. 3) or the results of Egger’s significance tests for the effects of individual simvastatin treatment on circulating adiponectin (p = 0.47).

Begg’s funnel plot for the evaluation of publication bias. WMD, weighed mean difference
Discussion
In this study, by pooling the results of previous published studies, the overall results of the meta-analysis showed that simvastatin treatment was not associated with significant change of adiponectin in patients at risk for CVDs. However, considerable heterogeneity exists among these studies, and results of subsequent analyses suggested that treatment duration may influence the effect of simvastatin treatment on serum adiponectin. Indeed, subgroup analyses indicated that simvastatin treatment was associated with significantly enhanced adiponectin level in studies with treatment duration of 12 weeks, but not in those of ≤ 8 weeks. These results suggested that simvastatin may enhance the serum level of adiponectin at least after 12 weeks of treatment duration, and chronic benefits of simvastatin in cardiovascular and metabolic systems may involve the regulation of serum adiponectin.
Our study has clinical relevance in the following aspects. Firstly, a previous meta-analysis indicated that patients with higher serum level of adiponectin were with a 17% lower risk of coronary artery disease (CAD) [12]. Therefore, the preventative effects of simvastatin on CAD may be related to their stimulatory effect on adiponectin. Interestingly, recent studies have indicated an inverse association between serum adiponectin levels and carotid intima-media thickness, an early manifestation of atherosclerosis [29]. Secondly, long-term administration of simvastatin has been reported to be associated with increased new-onset diabetes (NOD), although the mechanisms were not clear [30]. In view of the important role of adiponectin in pathogenesis of insulin resistance and DM, suppression of serum adiponectin has been proposed to be potential mechanisms underlying the effects of statins on NOD [31]. Our studies did not support that simvastatin was associated with decreased serum adiponectin, which indicated that simvastatin may increase the risk NOD via mechanisms other than suppression of adiponectin. Finally, the enhanced serum level of adiponectin was observed in studies with simvastatin treatment of 12 weeks, suggesting that future studies regarding the potential benefits of simvastatin in CVDs should at least be performed with 12-week of medication administration.
The potential mechanisms underlying regulatory effect of chronic simvastatin treatment on adiponectin were not fully understood at this stage, although the findings of some experimental studies may provide some evidence. An early in vitro study found that simvastatin could significantly increase the lipopolysaccharide-induced adiponectin secretion and mRNA expression in a dose-dependent manner, indicating that simvastatin could exert beneficial effects on prevention of obesity-induced metabolic changes in adipocytes [32]. Another in vitro study indicated that simvastatin counteracted the stimulatory effect of tumor necrotic factor α on secretion and expression of adiponectin, implying a potential anti-atherogenic effect during the inflammatory process [33]. Of note, these in vitro studies were performed to investigation the acute effect of simvastatin on adipocytes. Future in vivo studies with chronic administration of simvastatin are warranted to clarify the mechanisms underlying the regulatory effect of simvastatin on adiponectin.
Our study has limitations which should be noted when interpreting the results. Firstly, the quality of the included RCTs was modest and the scales of the studies were small. Further RCTs with high quality and adequate sample size are needed to confirm our results. Secondly, the follow-up durations of the RCTs were up to 12 weeks. Effects of simvastatin on serum adiponectin beyond 12 weeks deserve further investigation. Thirdly, many other factors, such as concurrent medications, diet factors, exercise habits, and sex hormone levels may modify the effects of simvastatin on serum adiponectin levels, but this was difficult to control and may have contributed to confounding of the results. Finally, effects of other statins on circulating adiponectin deserve further evaluation.
Conclusions
In conclusion, treatment with simvastatin of 12 weeks may increase the serum level adiponectin in patients at risk for cardiovascular diseases, but not for the short term treatment of ≤ 8 weeks. These results suggest that chronic benefits of simvastatin in cardiovascular and metabolic systems may involve the regulation of serum adiponectin.
References
Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–81.
Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, Voysey M, Gray A, Collins R, Baigent C. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–90.
Satoh M, Takahashi Y, Tabuchi T, Minami Y, Tamada M, Takahashi K, Itoh T, Morino Y, Nakamura M. Cellular and molecular mechanisms of statins: an update on pleiotropic effects. Clin Sci (Lond). 2015;129:93–105.
Effect of simvastatin on coronary atheroma: the Multicentre Anti-Atheroma Study (MAAS). Lancet. 1994;344:633–638.
Kolovou GD, Katerina A, Ioannis V, Cokkinos DV. Simvastatin: two decades in a circle. Cardiovasc Ther. 2008;26:166–78.
Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994. 344;1383–1389.
Koh KK, Sakuma I, Quon MJ. Differential metabolic effects of distinct statins. Atherosclerosis. 2011;215:1–8.
Han SH, Quon MJ, Kim JA, Koh KK. Adiponectin and cardiovascular disease: response to therapeutic interventions. J Am Coll Cardiol. 2007;49:531–8.
Turer AT, Scherer PE. Adiponectin: mechanistic insights and clinical implications. Diabetologia. 2012;55:2319–26.
Phillips SA, Kung JT. Mechanisms of adiponectin regulation and use as a pharmacological target. Curr Opin Pharmacol. 2010;10:676–83.
Li S, Shin HJ, Ding EL, van Dam RM. Adiponectin levels and risk of type 2 diabetes: a systematic review and meta-analysis. JAMA. 2009;302:179–88.
Zhang H, Mo X, Hao Y, Huang J, Lu X, Cao J, Gu D. Adiponectin levels and risk of coronary heart disease: a meta-analysis of prospective studies. Am J Med Sci. 2013;345:455–61.
Koh KK, Quon MJ, Han SH, Chung WJ, Ahn JY, Seo YH, Kang MH, Ahn TH, Choi IS, Shin EK. Additive beneficial effects of losartan combined with simvastatin in the treatment of hypercholesterolemic, hypertensive patients. Circulation. 2004;110:3687–92.
Koh KK, Quon MJ, Han SH, Ahn JY, Jin DK, Kim HS, Kim DS, Shin EK. Vascular and metabolic effects of combined therapy with ramipril and simvastatin in patients with type 2 diabetes. Hypertension. 2005;45:1088–93.
Devaraj S, Siegel D, Jialal I. Simvastatin (40 mg/day), adiponectin levels, and insulin sensitivity in subjects with the metabolic syndrome. Am J Cardiol. 2007;100:1397–9.
Pfutzner A, Hanefeld M, Lubben G, Weber MM, Karagiannis E, Kohler C, Hohberg C, Forst T. Visfatin: a putative biomarker for metabolic syndrome is not influenced by pioglitazone or simvastatin treatment in nondiabetic patients at cardiovascular risk—results from the PIOSTAT study. Horm Metab Res. 2007;39:764–8.
Gouni-Berthold I, Berthold HK, Chamberland JP, Krone W, Mantzoros CS. Short-term treatment with ezetimibe, simvastatin or their combination does not alter circulating adiponectin, resistin or leptin levels in healthy men. Clin Endocrinol (Oxf). 2008;68:536–41.
Koh KK, Quon MJ, Han SH, Lee Y, Ahn JY, Kim SJ, Koh Y, Shin EK. Simvastatin improves flow-mediated dilation but reduces adiponectin levels and insulin sensitivity in hypercholesterolemic patients. Diabetes Care. 2008;31:776–82.
Hu Y, Tong G, Xu W, Pan J, Ryan K, Yang R, Shuldiner AR, Gong DW, Zhu D. Anti-inflammatory effects of simvastatin on adipokines in type 2 diabetic patients with carotid atherosclerosis. Diab Vasc Dis Res. 2009;6:262–8.
Koh KK, Quon MJ, Han SH, Lee Y, Kim SJ, Park JB, Shin EK. Differential metabolic effects of pravastatin and simvastatin in hypercholesterolemic patients. Atherosclerosis. 2009;204:483–90.
Koh KK, Quon MJ, Sakuma I, Lee Y, Lim S, Han SH, Shin EK. Effects of simvastatin therapy on circulating adipocytokines in patients with hypercholesterolemia. Int J Cardiol. 2011;146:434–7.
Krysiak R, Zmuda W, Okopien B. The effect of simvastatin-ezetimibe combination therapy on adipose tissue hormones and systemic inflammation in patients with isolated hypercholesterolemia. Cardiovasc Ther. 2014;32:40–6.
Moezzi A, Parizadeh SM, Tavallaie S, Mazidi M, Afzali F, Adab A, Ferns G, Ghayour Mobarhan M. Effects of simvastatin treatment on serum adiponectin concentrations in patients with dislipidemia. Iran Red Crescent Med J. 2014;16:e6915.
Koh KK, Oh PC, Sakuma I, Kim EY, Lee Y, Hayashi T, Han SH, Park YM, Shin EK. Vascular and metabolic effects of ezetimibe combined with simvastatin in patients with hypercholesterolemia. Int J Cardiol. 2015;199:126–31.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. 2011. http://handbook.cochrane.org/.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Gasbarrino K, Gorgui J, Nauche B, Cote R, Daskalopoulou SS. Circulating adiponectin and carotid intima-media thickness: a systematic review and meta-analysis. Metabolism. 2016;65:968–86.
Carter AA, Gomes T, Camacho X, Juurlink DN, Shah BR, Mamdani MM. Risk of incident diabetes among patients treated with statins: population based study. BMJ. 2013;346:f2610.
Arnaboldi L, Corsini A. Could changes in adiponectin drive the effect of statins on the risk of new-onset diabetes? The case of pitavastatin. Atheroscler Suppl. 2015;16:1–27.
Yin X, Tu L, Yang H. Effect of simvastatin on IL-6 and adiponectin secretion and mRNA expression in 3 T3-L1 adipocytes. J Huazhong Univ Sci Technolog Med Sci. 2007;27:248–51.
Lobo SM, Quinto BM, Oyama L, Nakamichi R, Ribeiro AB, Zanella MT, Dalboni MA, Batista MC. TNF-alpha modulates statin effects on secretion and expression of MCP-1, PAI-1 and adiponectin in 3 T3-L1 differentiated adipocytes. Cytokine. 2012;60:150–6.
Acknowledgements
Not applicable.
Funding
This study was supported by a grant from the Natural Science Foundation of Fujian Province, China (no. 2013D011), and Natural Science Foundation of Xiamen City, China (no. 3502Z20154011). The funding bodies did not play a role in the design of the study, collection, analysis, or interpretation of data, or in writing the manuscript.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on request.
Authors’ contributions
WC and NZ designed the study. WC and ZH performed statistical analysis, and drafted the manuscript. MB and XX collected data and assisted with statistical analysis and manuscript drafting. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chen, W., Huang, Z., Bi, M. et al. Effects of simvastatin on serum adiponectin: a meta-analysis of randomized controlled trials. Lipids Health Dis 16, 53 (2017). https://doi.org/10.1186/s12944-017-0439-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-017-0439-0