
Abstract
Background
Millions of tons of lead were added to gasoline worldwide beginning in 1922, and leaded gasoline has been a major source of population lead exposure. In 1960s, lead began to be removed from automotive gasoline. Removal was completed in 2021.
Objectives
To determine whether removal of lead from automotive gasoline is associated with declines in population mean blood lead levels (BPb).
Methods
We examined published studies that reported population blood leaded levels for two or more years, and we calculated average concentrations of lead in gasoline corresponding to the years and locations of the blood lead level measurements.
Results
Removal of lead from gasoline is associated with declines in BPb in all countries examined. In some countries, BPb continues to fall after lead has been eliminated from gasoline. Following elimination of lead from gasoline, BPb less than 1 μg/dL have been observed in several European and North American countries, and BPb less than 3 μg/dL have been documented in several studies from South America.
Discussion
There remain many countries for which no multi-year studies of populations BPb have been identified, including all of Central America, high population countries including Pakistan and Indonesia, and major lead producers including Australia and Russia.
Conclusion
Removal of lead from gasoline has been a public health success. Elimination of lead from gasoline has enabled many countries to achieve population mean BPb levels of 1 μg/dL or lower. These actions have saved lives, increased children’s intelligence and created great economic benefit in countries worldwide.
Similar content being viewed by others


Key messages
-
1.
The addition of lead to gasoline was a catastrophe for global health. It caused neurodevelopmental disability with diminished intelligence and disordered behavior in millions of children, as well as neurobehavioral deficits and premature deaths from cardiovascular and kidney disease in millions of adults, and great economic losses.
-
2.
WHO and UNEP deserve enormous credit for having successfully completed the removal of lead from automotive gasoline in all countries around the world. This work was accomplished under the leadership of the Partnership for Clean Fuels and Vehicles (PCFV) led by the United Nations Environment Programme and the World Health Organization [1].
-
3.
It is important to prevent the addition of other harmful substitutes to gasoline such as benzene or manganese in lieu of lead [2].
The lead pandemic provides an object lesson of the dangers of ignoring early warnings on potential danger [3] and of permitting wide use and dissemination of chemicals that have not been adequately tested for potential toxicity [4]. The use of lead in gasoline is a classic example of our society’s willingness to adopt a promising but unproven new technology without heed to its possible consequences. We made the same error with chlorofluorocarbon (CFCs), and we are at risk of making it again if we adopt fuel additives containing manganese, a known neurotoxicant [2]. For our children’s future [5], we must do better.
Introduction
In the past century, millions of tons of lead were added to gasoline worldwide [6]. The result has been a global pandemic of lead poisoning with damage to health, impairment of cognitive function, reduction in life expectancy, and premature death of millions of persons. This pandemic began in 1922 when lead in the form of tetraethyl lead was first added to motor fuels, accelerated after World War II, and peaked in the 1970s and 1980s. Neurodevelopmental impairment with IQ loss, shortened attention span, dyslexia, attention deficit/hyperactivity disorder, school failure, and increased future risk for drug abuse, criminal behavior and incarceration are the main health consequences in children [7,8,9,10,11]. Neurobehavioral impairment, hypertension, renal disease, cardiovascular disease, stroke and premature death are the health consequences in adults [12, 13]. It is now known that no level of lead is safe [14, 15].
The dangers of adding lead to gasoline first became evident in the 1920’s when a cluster of cases of acute neuropsychiatric disease appeared among workers occupationally exposed to tetraethyl lead at a refinery in Bayway, New Jersey, USA; 80% of the affected workers developed convulsions and five died [16]. These warnings were, however, ignored and after a brief pause in production, the addition of lead to gasoline resumed [3, 16]. At peak use in the 1970s and 1980s, virtually all countries around the world added lead to motor fuels [17]. Levels of lead were found to be elevated in cities and along roadways [18]. Geochemical studies conducted in the high Arctic documented an unprecedented increase in atmospheric deposition of lead into the Greenland ice cap [19]. These findings have been confirmed more recently by studies of lead deposition in Alpine glaciers [20].
Lead began to be removed from gasoline in the late 1960s, first in the Soviet Union, then in Japan and the United States [21]. The US Environmental Protection Agency mandated removal of lead from gasoline beginning in 1975 because of two discoveries – first, the recognition that lead released to the environment by the combustion of leaded gasoline was causing widespread lead poisoning in children [7, 8], and secondly, the realization that lead in gasoline was destroying the catalytic converters required on all new cars in compliance with the Clean Air Act Amendments of 1970 [22].
In the United States, the removal of lead from gasoline was followed by a more than 90% reduction in mean blood lead concentration between 1976 and 1995 [23]. This decline closely paralleled year-to year reductions in the amount of lead added to gasoline. The percentage of children in the United States aged 1–5 years with blood lead levels greater than or equal to 10 μg/dl fell from nearly 80% in the late 1970s to less than 5% in the early 1990s [24]. Other factors that may have contributed to the decline in blood lead levels in the United States were increased professional and public awareness of the dangers of low-level lead exposure and the banning of lead from domestic paint and plumbing supplies; however there is a close temporal parallel between the reduction of lead in gasoline and the decline in blood lead levels. The mean blood lead level in the United States today is less than 1 μg/dL [25].
Our data indicate that all countries, in all regions of the world have now eliminated lead from gasoline used in motor vehicles. Algeria, the last country to remove lead from automotive gasoline, did so in 2021. Declines in blood lead levels following removal of lead from gasoline have been reported in numerous countries and cities [26]. Lead is still used in racing cars and in aviation gasoline for small, piston-engine aircraft [27].
To assess the impact on global health of reducing lead levels in gasoline, Thomas et al. analyzed 17 studies from 5 continents and reported their findings in 1999 [28]. They compared reductions in blood lead levels in cities and countries with reductions in the mean concentration of lead in gasoline and found a strong linear correlation between the two with a median correlation coefficient of 0.94. Data on air lead concentrations were also available in some of the same locations, and in those places, correlations were observed between declining concentrations of lead in gasoline and reductions in air lead levels. In most locations that completely removed lead from gasoline, mean blood levels fell to approximately 3 μg/dL. Higher residual blood lead levels were observed in locations with widespread exposure to lead from sources other than leaded gasoline such as exposures to lead mining and smelting, lead battery recovery operations, lead-contaminated waste sites, e-waste recovery operations, lead-glazed pottery, and lead-containing cosmetics and medications [29,30,31,32,33,34].
Now to extend, update and corroborate the 1999 analysis by Thomas et al. [28], we have gathered 38 additional reports. For those reports as well as for earlier publications, we have systematically examined the relationships between reductions in levels of lead in gasoline and declines in population blood lead levels. This work was undertaken as a component of an effort led by the World Health Organization to develop guidelines on the prevention and management of lead exposure.
Methods
Search strategy for blood lead studies
The populations of interest are the general populations, children and adults, not known to be living near industrial lead sites or occupationally exposed, for which there are serial measurements of blood lead levels so that changes in blood lead levels can be observed over time as levels of lead in gasoline change. Comparison is provided both with time periods in which use of lead in gasoline lead did not change, as well as with time periods with quantitatively different changes in gasoline lead. Relevant outcomes include the amounts and rates of change in blood lead levels. In consultation with an experienced research librarian, we developed search strategies using the key words “lead blood level” and “gasoline.” We searched for full-text articles in the following databases: PubMed, Global Health in Ovid SP, EMBASE, and the Cochrane Library.
We developed and refined a data extraction sheet. One author extracted data from each study included in the analysis, and the second author checked the extracted data to ensure accuracy. Disagreements were resolved by discussion between the two review authors; if no agreement could be reached, a third author was available to adjudicate. However, all disagreements were resolved without the need for a third review. If an article identified through the databases could not be found, the corresponding author listed in the research article was contacted for the full-text article. If there was confusion about the contents of a research article, the corresponding author was contacted for further clarification. If the corresponding author was unable to be contacted, the principal investigator for the respective research article, subsequently followed by any additional authors listed, were contacted.
We included observational studies that measured serial blood lead levels (BLLs) in populations over a time span of at least 1 year. We also included studies that compared primary data with historical data. We included studies examining populations of both males and females, all age groups, and both urban and rural communities. Finally, studies in this systemic review had to include BLLs as their primary outcome.
Through this systematic search, we identified a total of 1696 records through database searching. After removing duplicates, 1264 records were screened and 874 articles were excluded based on the title and/or the abstract. Three hundred and ninety articles were then assessed for eligibility. Three hundred and fifty-one articles were excluded for reasons, including:
-
The article was published in a language not accessible to the reviewers.
-
The article was not available (only an abstract or poster was available).
-
The article was not relevant to the systematic review.
-
The article was a review paper and did not provide any original data.
-
The article provided no quantitative outcome data.
-
The article did not have data for at least two time periods separated by at least 1 year.
No evaluations of study quality or the possibility of bias other than the above criteria were applied. The criterion of providing blood lead measurements for more than one time period separated by at least 1 year is a significant marker of achievement, requiring ongoing laboratory and analysis capability. In sum, 38 articles were added to the systematic review of changes in blood lead levels related to changes in the lead content of gasoline published previously by Thomas et al. [28]. The data extracted from these articles was population blood lead level for each year reported, population location, and the population age range (Fig. 1).

Study selection flow chart
Database development for gasoline lead use
Measures of gasoline lead levels were calculated using data from Octel Ltd. [35], the world’s principal manufacturer of tetraethyl lead. Octel reports are available for the years 1968, 1969, 1971, 1975, 1976, 1978, 1979, 1981, 1982, 1983, 1984, 1991, 1992/3, 1994, 1995, and 1996. 1995 is the last year in which Octel included gasoline lead concentrations in its reports. The Octel reports provide data at the national level, and usually include the amount of gasoline and the concentration of lead in both premium and in regular gasoline grades. We use the weighted average of the concentration in premium and regular grades of gasoline. The Octel data were supplemented and cross-checked with data available from other sources, including data reported in the blood lead studies. For years after 1995 we used data developed from extensive literature review.
To characterize the use of lead in gasoline we consider two metrics, the total amount of lead used in gasoline, and the average concentration of lead in gasoline, calculated as the consumption-weighted average lead concentration of all gasoline grades sold, including unleaded gasoline.
Table S1 in the Supplemental Material summarizes the data on blood lead and gasoline lead included in this study.
Statistical analysis
Each included study reports data on population blood lead concentrations for at least 2 years for the same or similar location and for a similar population group. For each year with a reported population blood lead level, we calculated the average gasoline lead level, including both leaded and unleaded gasoline, on a national level. In cases in which the reported population blood lead levels covered a combined two-year period, in which case we use the average gasoline lead concentration over the two-year period.
Studies are from different countries and locations, and the population cohorts differ by age and location, and thus we do not combine results from different studies, and we do not extrapolate or fit the data. There are measurement errors in both the blood lead values and the gasoline lead values. We estimate the error in the gasoline lead values as 10-20%.
Results
Results are shown by continent.
Figures 2 and 3 show results for Europe, for which there have been more studies in different countries of blood level levels over time than for any other continent. Studies from several countries – Germany [36], Sweden [37], and Spain [38]– show blood lead concentrations of less than 2 μg/dL. All of the European studies show decreased blood lead concentrations over time. Figure 3 shows that in the majority of locations, blood lead concentrations fell in close temporaal concordance with gasoline lead concentrations [39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]. In Istanbul blood lead levels fell without a reduction in gasoline lead; Furman [61] reports that there had been a substantial decrease in gasoline lead levels several years before the reported measurements were made. Also to some extent in Venice and Zagreb, blood lead levels fell without a reduction in gasoline lead [62, 63]. This may indicate reduction in other sources of exposure, as well as uncertainty in the use of lead in gasoline. The data for several countries show continued blood lead reduction after the complete phase out of gasoline lead; this is expected, as lead remains in the body for years [64].

Population blood lead levels by year in Europe. Twenty-eight studies are shown; each marker is one data point; each line connects the data for a single study

Population blood lead levels versus gasoline lead concentrations in Europe. Twenty-eight studies are shown; each marker is one data point; each line connects the data for a single study
Even though there are numerous European studies, there are countries for which there are no data on how blood lead concentrations have changed over time. There are no studies over time from Russia, Ukraine, Romania, Netherlands, Czech Republic, and others. Russia is a major lead producer, but nonetheless took early action to eliminate lead from gasoline in major cities [65].
Figures 4 and 5 show data from North America. The data for the United States are the most extensive in North America [66, 67], and show that US blood lead concentrations have fallen below 1 μg/dL as of 2011. Canadian data from Ontario and specifically Toronto are less extensive and somewhat higher than the results from the US overall [68,69,70]. Studies from Mexico show higher blood lead levels, decreasing over time and decreasing as gasoline lead concentrations decreased [71,72,73,74].

Population blood lead levels by year in North America. Five studies are shown; each marker is one data point; each line connects the data for a single study

Population blood lead levels versus gasoline lead concentrations in North America. Five studies are shown; each marker is one data point; each line connects the data for a single study
Figures 6 and 7 show data from South America. There are no studies in our data set from Central America. The South American studies are from Venezuela, Chile, Uruguay, Argentina, and Peru [75,76,77,78,79,80]. There are no studies on blood lead concentrations over time from Brazil, Columbia, Ecuador, and others. The lowest population blood lead concentrations reported in these studies is 2.6 μg/dL, in Cordoba, Argentina from 2010. The trajectories shown across the studies suggest that current blood lead levels in Lima, Santiago, and Montevideo may now be lower.

Population blood lead levels by year in South America. Five studies are shown; each marker is one data point; each line connects the data for a single study

Population blood lead levels versus gasoline lead concentration in South America. Five studies are shown; each marker is one data point; each line connects the data for a single study
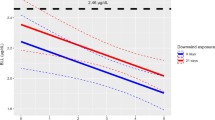
Figures 8 and 9 show the data for Asia. Figure 8 shows that blood lead concentrations have decreased over time in all of the Asian data sets. Figure 9 shows that in most of the countries, decreasing blood lead concentration is associated with decreasing concentrations of lead in gasoline [81,82,83,84]. For Mumbai, India, there was substantial decrease in the concentration of lead in gasoline while blood lead levels remained roughly constant. However, between 1985 and 1995, while the concentration of lead in gasoline decreased by approximately a factor of two, the amount of gasoline consumed rose by approximately a factor of [85] two. All of the data sets from China show falling blood lead concentrations with gasoline lead levels already at low levels [86,87,88,89]. While data on use of lead in gasoline in China are sparse, there is no indication of heavy use of lead in gasoline. The decreasing blood lead concentrations in China may reflect decreases in other sources of lead exposure. The lowest levels from these studies is 1.4 μg/dL, from Japan in 2008 (Fig. 9) [90,92,93].

Population blood lead levels by year in Asia. Twelve studies are shown; each marker is one data point; each line connects the data for a single study

Population blood lead levels versus gasoline lead concentrations in Asia. Twelve studies are shown; each marker is one data point; each line connects the data for a single study
Figures 10 and 11 show result for Africa, for South Africa, Nigeria, and the Democratic Republic of Congo [94,95,96,97,98]. Although lead was phased out of gasoline in many African countries by 2006, there are ongoing exposures from other sources [31, 99]. The data in Figs. 10 and 11 show consistent slopes, with decreases corresponding to reduced use of lead in gasoline and over time. All of the African studies show relatively lower blood lead concentrations for the gasoline lead concentrations, compared to the results from South America, North American and Europe, while similar to the results from Asia. These may indicate comparatively low consumption of gasoline in the African cities studied, compared to the studies from North and South America and Europe. Further studies of lead exposure in more locations in Africa would be welcome to further examine population lead exposures and trends.

Population blood lead levels by year in Africa. Four studies are shown; each marker is one data point; each line connects the data for a single study

Population blood lead levels versus gasoline lead concentrations in Africa. Four studies are shown; each marker is one data point; each line connects the data for a single study
Figures 12 and 13 show data from Oceania. This region includes Australia, New Zealand, Melanesia, Micronesia, and Polynesia. There has only been a one published study of blood lead concentration trends in a general population: the study shown from Christchurch New Zealand [100,102,103]. Australia has been one of the world’s largest producers of lead since the 1800’s, and has the world’s largest lead reserves. Yet there has been no study of population exposure trends. The Christchurch New Zealand study shows a significant decrease in blood lead concentrations from 1978 to 1984, a time during which the gasoline lead concentrations did not change. This may indicate reductions in other sources of lead exposure, or improvements in laboratory measurement techniques. After 1984 the relative values of blood lead versus gasoline lead are similar to those in Europe and in North and South America.

Population blood lead levels versus year in New Zealand. One study is shown; each marker is one data point

Population blood lead levels versus gasoline lead concentrations in New Zealand. One study is shown; each marker is one data point
Discussion
Lead has now been removed from gasoline in all countries in the world. Algeria, the last country to still use lead in motor vehicle gasoline, completed removal in 2021, 99 years after the commercial introduction of tetraethyl lead. These findings corroborate and extend the previous work of Thomas et al., [28] and they confirm that removal of lead from gasoline has been a highly effective strategy for reducing population lead levels. These data show that the reduction in blood lead levels that followed removal of lead from gasoline has been lasting and that the health benefits of lead removal have now been extended to more than two generations of children.
In some cities and countries lead levels have not fallen as sharply as in others. This may speak to widespread population exposure in these locations to lead sources other than gasoline such as lead-based paint, plumbing containing lead (Flint, MI), industrial lead emissions, or lead-containing household and consumer products, for example, widespread use of lead pottery in Mexico, as well as the possibility of systematic measurement errors [29].
There are some cases in which blood lead levels decreased during a time with no known decrease in gasoline lead levels. We see this in the data from Istanbul; Furman [61] reports that there had been a substantial decrease in gasoline lead levels several years before the reported measurements were made. Also, in the United States and several other countries, blood lead levels have continued to fall in the years since the complete phase out of lead in gasoline. These may be due both to decreases in residual exposure to lead from gasoline, and to decreases in other sources of exposure.
The great strength of this study lies in the availability of well curated data sets from multiple cities and countries around the world. The principal weakness is the lack of data from certain areas. There is an ongoing need for measurements of population lead exposure, in low- and middle-income countries [104] as well as in higher income countries. In addition, continuing lead exposures in communities due to legacy or ongoing uses of lead are not reflected in aggregated studies have not received systematic study [105].
Availability of data and materials
All data are available in the supplementary information.
References
(UNEP), U.N.E.P. The lead campaign. 2022. Available from: https://www.unep.org/explore-topics/transport/what-we-do/partnership-clean-fuels-and-vehicles/lead-campaign.
Landrigan P, et al. The Declaration of Brescia on prevention of the neurotoxicity of metals June 18, 2006. Am J Ind Med. 2007;50(10):709–11.
Harremoës P, et al. Late lessons from early warnings: the precautionary principle 1896-2000. Copenhagen: European Environmental Agency; 2001.
Landrigan PJ, Goldman LR. Children’s vulnerability to toxic chemicals: a challenge and opportunity to strengthen health and environmental policy. Health Aff (Millwood). 2011;30(5):842–50.
Reuben A, et al. Association of childhood blood lead levels with cognitive function and socioeconomic status at age 38 years and with IQ change and socioeconomic mobility between childhood and adulthood. JAMA. 2017;317(12):1244–51.
Organisation for Economic Co-operation Development. and United Nations Environment Programme. Phasing lead out of gasoline: an examination of policy approaches in different countries. Paris: OECD; 1999.
Landrigan PJ, et al. Neuropsychological dysfunction in children with chronic low-level lead absorption. Lancet. 1975;1(7909):708–12.
Needleman HL, et al. Deficits in psychologic and classroom performance of children with elevated dentine lead levels. N Engl J Med. 1979;300(13):689–95.
Needleman HL, et al. Bone lead levels in adjudicated delinquents. A case control study. Neurotoxicol Teratol. 2002;24(6):711–7.
Needleman HL, et al. The long-term effects of exposure to low doses of lead in childhood. An 11-year follow-up report. N Engl J Med. 1990;322(2):83–8.
Nevin R. Understanding international crime trends: the legacy of preschool lead exposure. Environ Res. 2007;104(3):315–36.
Pirkle JL, et al. The relationship between blood lead levels and blood pressure and its cardiovascular risk implications. Am J Epidemiol. 1985;121(2):246–58.
G. B. D. DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603–58.
Lanphear BP, et al. Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environ Health Perspect. 2005;113(7):894–9.
World Health Organization. Childhood lead poisoning. Geneva: WHO; 2010.
Rosner D, Markowitz G. A ‘gift of God’?: The public health controversy over leaded gasoline during the 1920s. Am J Public Health. 1985;75(4):344–52.
Fewtrell LJ, et al. Estimating the global burden of disease of mild mental retardation and cardiovascular diseases from environmental lead exposure. Environ Res. 2004;94(2):120–33.
Caprio RJ, Margulis HL, Joselow MM. Lead absorption in children and its relationship to urban traffic densities. Arch Environ Health. 1974;28(4):195–7.
Murozumi M, Chow TJ, Patterson C. Chemical concentrations of pollutant lead aerosols, terrestrial dusts and sea salts in Greenland and Antarctic snow strata. Geochim Cosmochim Acta. 1969;33(10):1247–94.
More AF, et al. Next-generation ice core technology reveals true minimum natural levels of lead (Pb) in the atmosphere: Insights from the Black Death. GeoHealth. 2017;1(4):211–19.
Thomas VM. The Elimination of Lead in Gasoline. Annu Rev Energy Environ. 1995;20(1):301–24.
Newell RG, Rogers K. The US Experience with the phasedown of lead in gasoline; 2003.
Annest JL, et al. Chronological trend in blood lead levels between 1976 and 1980. N Engl J Med. 1983;308(23):1373–7.
CDC. Blood lead levels--United States, 1999-2002. MMWR Morb Mortal Wkly Rep. 2005;54(20):513–6.
Tsoi MF, et al. Continual decrease in blood lead level in Americans: United States national health nutrition and examination survey 1999-2014. Am J Med. 2016;129(11):1213–18.
Landrigan PJ. The worldwide problem of lead in petrol. Bull World Health Organ. 2002;80(10):768.
Federal Aviation Administration and US DOT. Aviation gasoline. 2017. Available from: https://www.faa.gov/about/initiatives/avgas/.
Thomas VM, et al. Effects of reducing lead in gasoline: an analysis of the international experience. Environ Sci Technol. 1999;33(22):3942–8.
Diaz-Ruiz A, et al. Glazed clay pottery and lead exposure in Mexico: current experimental evidence. Nutr Neurosci. 2017;20(9):513–18.
Caravanos J, et al. The burden of disease from pediatric lead exposure at hazardous waste sites in 7 Asian countries. Environ Res. 2013;120:119–25.
Ericson B, Landrigan P, Taylor MP, Frostad J, Carabanos J, Keith J, et al. The global burden of lead toxicity attributable to informal used lead-acid battery sites. Ann Glob Health. 2016;82(5):686–99.
Heacock M, et al. Prevention-intervention strategies to reduce exposure to e-waste. Rev Environ Health. 2018;33(2):219–28.
Caravanos J, et al. Blood lead levels in Mexico and pediatric burden of disease implications. Ann Global Health. 2014;80(4):269.
Horiuchi T, Narimatsu K, Hokari R. Imported ayurvedic medicine and lead poisoning. Intern Med. 2022;61:3313.
Associated Octel Company, World wide survey of motor gasoline quality, May, 1968. 1968.
Lermen D, et al. Long-term time trend of lead exposure in young German adults – Evaluation of more than 35 Years of data of the German Environmental Specimen Bank. Int J Hyg Environ Health. 2021;231:113665–72.
Strömberg U, Lundh T, Skerfving S. Yearly measurements of blood lead in Swedish children since 1978: the declining trend continues in the petrol-lead-free period 1995-2007. Environ Res. 2008;107(3):332–5.
Ordonez-Iriarte JM, et al. Economic appraisal of the impact of the ban on the use of lead in gasoline on the intellectual quotient of 7-8 years old in the community of Madrid. Rev Esp Salud Publica. 2015;89(5):487–96.
Chartsias B, et al. The impact of gasoline lead on man blood lead: first results of the Athens lead experiment. Sci Total Environ. 1986;55:275–82.
Kapaki EN, et al. Blood lead levels of traffic- and gasoline-exposed professionals in the city of Athens. Arch Environ Health. 1998;53(4):287–91.
Rodamilans M, et al. Effect of the reduction of petrol lead on blood lead levels of the population of Barcelona (Spain). Bull Environ Contam Toxicol. 1996;56(5):717–21.
Ducoffre G, Claeys F, Bruaux P. Lowering time trend of blood lead levels in Belgium since 1978. Environ Res. 1990;51(1):25–34.
Guberti E, et al. Trends in blood lead levels in the population of the city of Bologna. Ann Ist Super Sanita. 1998;34(1):67–73.
Bitto A, Horvath A, Sarkany E. Monitoring of blood lead levels in Hungary. Cent Eur J Public Health. 1997;5(2):75–8.
Meyer I, et al. Temporal changes in blood lead levels of children in east Germany. Int J Hyg Environ Health. 2003;206(3):181–92.
Huel G, et al. Evolution of blood lead levels in urban French population (1979-1995). Rev Epidemiol Sante Publique. 2002;50(3):287–95.
Kolossa-Gehring M, et al. German Environmental Survey for Children (GerES IV)--first results. Int J Hyg Environ Health. 2007;210(5):535–40.
Pönkä A, Salminen E, Ahonen S. Lead in the ambient air and blood specimens of children in Helsinki. Sci Total Environ. 1993;138:301–8.
Pönkä A. Lead in the ambient air and blood of children in Helsinki. Sci Total Environ. 1998;219:1–5.
Neri R, Palmieri F. Blood lead levels in the population of La Spezia. Ann Ist Super Sanita. 1998;34(1):51–7.
Piccinini R, et al. Lead absorption in an Umbrian population from 1982 to 1992. Ann Ist Super Sanita. 1998;34(1):81–90.
Jarosinska D, Biesiada M, Muszynska-Graca M. Environmental burden of disease due to lead in urban children from Silesia, Poland. Sci Total Environ. 2006;367(1):71–9.
Roma-Torres J, et al. Lead exposure of children and newborns in Porto, Portugal. Int J Hyg Environ Health. 2007;210(3-4):411–4.
Elinder CG, et al. Decreased blood lead levels in residents of Stockholm for the period 1980-1984. Scand J Work Environ Health. 1986;114–20.
Wietlisbach V, et al. Time Trend and Determinants of Blood Lead Levels in a Swiss Population over a Transition Period (1984-1993) from Leaded to Unleaded Gasoline Use. Environ Res. 1995;68:82–90.
Schuhmacher M, et al. Impact of reduction of lead in gasoline on the blood and hair lead levels in the population of Tarragona Province, Spain, 1990–1995. Sci Total Environ. 1996;184:203–9
Bono R, et al. Updating about Reductions of Air and Blood Lead Concentrations in Turin, Italy, Following Reductions in the Lead Content of Gasoline. Environ Res. 1995;70:30–34.
Quinn MJ. Factors Affecting Blood Lead Concentrations in the UK: Results of the EEC Blood Lead Surveys, 1979–1981. Int J Epidemiol. 1985;14(3):420–31.
UK Department of the Environment. UK Blood lead monitoring programme 1984-1987. London; 1987.
Delves HTDSJ, Oppert S, Prescott-Clarke P, Periam J, Gompertz D. Blood lead concentrations in United Kingdom have fallen substantially since 1984. Br Med J. 1996;313:883–4.
Furman A, Laleli M. Maternal and umbilical cord blood lead levels: an Istanbul study. Arch Environ Health. 2001;56(1):26–8.
Bortoli A, et al. Environmental lead exposure in the Venetian population from 1976-1992. Ann Ist Super Sanita. 1998;34(1):59–65.
Zorana KG, Alica P, Jasna J. Influence of abatement of lead exposure in Croatia on blood lead and ALAD activity. Environ Sci Pollut Res Int. 2016;23(1):898–907.
Skerfving S, et al. Late effects of low blood lead concentrations in children on school performance and cognitive functions. NeuroToxicology. 2015;49:114-–20.
Thomas VM, Orlova AO. Soviet and post-soviet environmental management: lessons from a case study of lead pollution. Ambio. 2001;30(2):104–11.
Centers for Disease Control and Prevention. Blood Lead (2011 - 2018), National Health and Nutrition Examination Survey, cgroup2_LBXBPB_2011-p (2018).
Brody DJ, et al. Blood Lead Levels in the US Population. JAMA. 1994;272(4):277–83.
Wang ST, et al. Decline in blood lead in Ontario children correlated to decreasing consumption of leaded gasoline, 1983-1992. Clin Chem. 1997;43(7):1251–2.
Langlois P, et al. Blood lead levels in Toronto children and abatement of lead-contaminated soil and house dust. Arch Environ Health. 1996;51(1):59–67.
Loranger S, Zayed J. Manganese and lead concentrations in ambient air and emission rates from unleaded and leaded gasoline between 1981 and 1992 in Canada: A comparative study. Atmos Environ. 1994;28(9):1645–51.
Santos-Guzman J, et al. A decade of lead monitoring in schoolchildren in the metropolitan area of Monterrey NL, Mexico. Salud Publica Mex. 2014;56(6):592–602.
Rothenberg SJ et al. Secular Trend in Blood Lead Levels in a Cohort of Mexico City Children. Arch Environ Health. 1998;53(3):231–5.
Driscoll W et al. Reducing lead in gasoline. Mexico’s experience. Environ Sci Technol. 1992;26(9):1702–5.
Program to control atmospheric pollution in Mexico City. Mexico City: Commission for Prevention and Control of Pollution; 1993.
Cedeno ALAA, Lombardi C. Comparative study of the levels of lead in the air and blood part II; technical report, S.A. Intevep, Editor. Los Teques: Filial de Petroleos de Venezuela; 1990.
Romero A. The environmental impact of leaded gasoline in Venezuela. J Environ Dev. 1996;5(4):434–8.
Martinez SA, et al. Blood lead levels and enzymatic biomarkers of environmental lead exposure in children in Cordoba, Argentina, after the ban of leaded gasoline. Hum Exp Toxicol. 2013;32(5):449–63.
Pino P, et al. Rapid drop in infant blood lead levels during the transition to unleaded gasoline use in Santiago, Chile. Arch Environ Health. 2004;59(4):182–7.
Mormontoy W, Gastanaga C, Gonzales GF. Blood lead levels among police officers in Lima and Callao, 2004. Int J Hyg Environ Health. 2006;209(6):497–502.
Cousillas A, et al. Impacts of multidisciplinary actions on environmental lead exposure in Uruguay. Environ Geochem Health. 2012;34(2):207–11.
Senanayake MP, Rodrigo MD, Malkanthi R. Blood lead levels of children before and after introduction of unleaded petrol. Ceylon Med J. 2004;49(2):60–1.
Kim D-S, Ahn S, Cha J-H. Unleaded gasoline use and lead level change in human blood. Toxicol Environ Heal Sci. 2011;3(1):22–9.
Neo KS, Goh KT, Sam CT. Blood lead levels of a population group not occupationally exposed to lead in Singapore. Southeast Asian J Trop Med Public Health. 2000;31(2):295–300.
Hwang YH, et al. Transition of cord blood lead level, 1985-2002, in the Taipei area and its determinants after the cease of leaded gasoline use. Environ Res. 2004;96(3):274–82.
Tripathi RM, et al. Atmospheric and children’s blood lead as indicators of vehicular traffic and other emission sources in Mumbai, India. Sci Total Environ. 2001;267(1):101–8.
Luo W, et al. Effects of chronic lead exposure on functions of nervous system in Chinese children and developmental rats. Neurotoxicology. 2012;33(4):862–71.
Wang L, et al. A systematic assessment of blood lead level in children and associated risk factors in China. Biomed Environ Sci. 2015;28(8):616–9.
Luo W, Zhang Y, Li H. Children's blood lead levels after the phasing out of leaded gasoline in Shantou, China. Arch Environ Health. 2003;58(3):184–7.
Huang P-C, et al. Childhood blood lead levels and intellectual development after ban of leaded gasoline in Taiwan: A 9-year prospective study. Environ Int. 2012;40:88–96.
Zhang ZW, et al. Further reduction in lead exposure in women in general populations in Japan in the 1990s, and comparison with levels in east and south-east Asia. Int Arch Occup Environ Health. 2000;73(2):91–7.
Niisoe T, et al. Environmental ecological modeling of human blood lead levels in East Asia. Environ Sci Technol. 2011;45(7):2856–62.
Ikeda M, et al. Cadmium, chromium, lead, manganese and nickel concentrations in blood of women in non-polluted areas in Japan, as determined by inductively coupled plasma-sector field-mass spectrometry. Int Arch Occup Environ Health. 2011;84(2):139–50.
Sugiyama SNH, Tatsumi S, Yamaguchi M, Furutani A, Yasui M, Yoshimura M. Comparison of heavy metal concentrations in human umbilical cord in 1980 and 1990. Nihon Hoigaku Zasshi. 1996;50(6):412–15.
Maresky LS, Grobler SR. Effect of the reduction of petrol lead on the blood lead levels of South Africans. Sci Total Environ. 1993;136(1-2):43–8.
Mathee A, et al. Reductions in blood lead levels among school children following the introduction of unleaded petrol in South Africa. Environ Res. 2006;100(3):319–22.
Naicker N, Mathee A, Barnes B. A follow-up cross-sectional study of environmental lead exposure in early childhood in urban South Africa. S Afr Med J. 2013;103(12):935–8.
Ojo JO, et al. Influence of nutritional status on some toxic and essential elements in the blood of women exposed to vehicular pollution in Ile-Ife, Nigeria. Environ Sci Pollut Res Int. 2014;21(2):1124–32.
Tuakuila J, et al. Blood lead levels in children after phase-out of leaded gasoline in Kinshasa, the capital of Democratic Republic of Congo (DRC). Arch Public Health. 2013;71(1):5.
World Health Organization. Lead exposure in African children: contemporary sources and concerns. World Health Organization, Regional Office for Africa. Brazzaville: Republic of Congo; 2015.
Hinton D, et al. Trends in blood lead levels in Christchurch (NZ) and environs 1978-85. J Epidemiol Community Health. 1986;40:244–8.
Walmsley TAS, J. A, Hinton D. Blood lead levels population data base: trace elements in New Zealand: environmental, human and animal. In: New Zealand Trace Elements Group conference. Canterbury: Lincoln College; 1998.
Walmsley T, et al. Trends in adult blood lead levels in New Zealand, 1974-1994. Public Health Rep. 1995;2(10):81-82
Grant S. in New Zealand Institute of Medical Laboratory Science annual conference. Auckland: New Zealand Institute of Medical Laboratory Science; 1996.
Ericson B, Hu H, Nash E, Ferraro G, Sinitsky J, Taylor MP. Blood lead levels in low-income and middle-income countries: a systematic review. Lancet Planet Health. 2021;5:e145–53.
Landrigan PJ, et al. The Lancet Commission on pollution and health. Lancet. 2018;391(10119):462–512.
Acknowledgements
We thank O. Bukharin and the Energy Institute Library for data access.
Funding
There was no external funding for this study.
Author information
Authors and Affiliations
Contributions
All authors, G.C., R.C.A., P.J.L. and V.M.T, wrote the main manuscript text. G.C., R.C.A. and V.M.T searched the literature and developed the database. V.M.T calculated the gasoline lead emissions and prepared the figures. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable. All population data used in this study are from previously published studies.
Consent for publication
All authors have reviewed the final submitted manuscript and have consented to publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Angrand, R.C., Collins, G., Landrigan, P.J. et al. Relation of blood lead levels and lead in gasoline: an updated systematic review. Environ Health 21, 138 (2022). https://doi.org/10.1186/s12940-022-00936-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-022-00936-x