
Abstract
Background
Some reports suggest there are differences in health needs between the population affiliated to the subsidized health insurance scheme (SS) and those affiliated to the contributory health insurance scheme (CS) in Colombia. The objective of this study was to identify the epidemiological profile of the population affiliated to the SS in Colombia and to compare the main epidemiological features of the SS to the CS.
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) methodology, the search was carried out from 1993, with no other restriction. The information was synthesized into five categories according to the most important risk populations. We estimated combined incidences from epidemiological surveillance data, prevalence ratio, and other measures to estimate the difference between the studied groups. A 95% confidence interval was considered. A random effects model was used weighted by the inverse of the variance of the cumulative incidence calculated for each disease. The risk of bias was assessed using the Joanna Briggs Institute’s critical appraisal tools.
Results
A total of 16,236 articles were identified; 14,972 were excluded after title and abstract screening, 725 articles were verified as full text, and finally 268 articles were included. The relative risk of non-communicable and communicable diseases was lower in the SS than in the CS (RR: 0.37 and 0.72, respectively, p-value < 0.05). However, the risk of presenting obstetric and maternal conditions in the SS versus the CS was RR 1.55 for frequent conditions during early childhood, and for other diseases it was RR 1.28 with a p-value of < 0.05. The use of health services was different by scheme, with less demand, access, and provision being found in health services in the SS.
Conclusions
This study allowed us to conclude that there are differences in the incidence, prevalence, and use of health services between health affiliation schemes (SS and CS) in Colombia, thereby assisting in decision-making for stakeholders.
Trial registration
PROSPERO Registration number CRD42021279234.
Similar content being viewed by others

Background
The General System of Social Security in Health (SGSSS) in Colombia is the mechanism by which the public health service is regulated and creates the conditions for the access of the population to all levels of health care. The state integrates this system through the Ministry of Health and Social Protection (MHSP) and other government entities; it began its regulation through Law 100 of 1993, which is the current comprehensive social security system in the country [1]. This law, in order to guarantee access to health care, established that for each affiliated person a Capitation Payment Unit (CPU) is recognized for health-promoting entities (HPEs) [2]. The CPU is defined as the annual value recognized by each person affiliated to the SGSSS to cover the health technologies included in the Health Benefit Plan (HBP). Likewise, Law 100 of 1993 stipulated an insurance system through schemes that include the contributory scheme (CS) and the subsidized scheme (SS), in addition to other so-called “special schemes” (for employees of military forces, public universities, etc.) [3].
All persons linked through a labour contract, public servants, pensioners, and independent workers with the ability to pay can join the CS and, through a monthly contribution to an HPE, they can access health services through health service provider institutions (HSPIs). The people affiliated with this scheme can be dependent or independent workers with income who can guarantee the monthly contributions and, in turn, the additional payments that must be made for health matters, such as moderating fees and co-payments. These payments are proportional to each person’s income [1].
On the other hand, the subsidized scheme is characterized by affiliating people without the ability to pay and those who are vulnerable in the country – that is, those classified as level 1 or 2 in the Beneficiary Selection System (BSS) and priority special populations such as people in forced displacement, the abandoned child population, boys and girls disconnected through armed conflict, indigenous communities, elderly people in protection centres, people from the witness protection programme, street dwellers, and Romani people, among others (according to classification 3 of the BSS). This population can also choose the HPE that provides health-care services through an HSPI [1, 4].
Currently, the value of the financing that is allocated for health coverage in each of the schemes is different, as is provided in Resolution 2503 of 2020, which assigns the budget for the CPU for the year 2021 according to the scheme, either contributory or subsidized. The CPU estimate is the product of the technical-actuarial analysis of the information reported by the HPE to the Ministry of Health, where the main frequencies of use of the health services provided are identified. It is important to note that the quality of the information of the CS is superior to that of the SS. Additionally, government-certified sources are taken into account to consider factors such as demographic changes in the relevant population, the national epidemiological profile, health technologies available in the country, general illnesses and maternal conditions covered in the promotion of health and prevention phases of the disease, and the prevention, diagnosis and treatment of pathologies according to the use of services and levels of care and complexity. Particular characteristics of population subgroups such as the indigenous population are also taken into account, for whom a different percentage of CPU is available due to their socio-cultural, demographic, and epidemiological differences [5].
The analysis of these characteristics to define the monetary values of the CPU for each scheme is carried out in order to collect the differences that may occur in the risk of becoming ill and to present differential health results in the affiliated population. These differences, which are tangible, especially in health outcomes, have been described in the SGSSS in Colombia. In 2015, the Ministry of Health demonstrated the inequities in health in the country in terms of mortality, as well as a possible relationship of this with the population density indices. This analysis also evidenced a positive correlation between infant mortality rates and socio-economic inequity, indicating that the departments that presented improvements in the Gini coefficient maintained lower levels in those rates [6].
Other differences in the consumption of health resources and in the presentation of communicable diseases have also been reported. Mejía et al. [7] published an analytical study that analysed the equity in access to health services in the department of Antioquia, as well as its main determinants, finding that education, age, and type of affiliation to social security were the main factors that determine the access to preventive and curative services. On the other hand, Hilarion-Gaitán et al. [8] evaluated social inequalities in health in Colombia, using the type of affiliation to the health system as a representative parameter of the socio-economic condition. For this, they carried out a descriptive and retrospective study where the incidence rates for events were calculated. In the SS population, 82.31 more cases of Plasmodium falciparum malaria were reported per 100,000 affiliates than those reported in the CS population. Additionally, belonging to the SS was associated with a greater risk of dying from malnutrition in children under 5 years of age, specifically 31.74 times more than for those in the CS.
Although there are some reports and seminal studies that suggest there may be different health needs in the population affiliated to the SS compared to the needs of the CS population in Colombia, determined by differences in the burden of disease, health outcomes, and use of health services, it has not been proven whether these differences exist across the spectrum of diseases, nor is the magnitude of these dissimilarities recognized. Therefore, the objective of this study was to identify the epidemiological profile of the population affiliated to the SS in Colombia, establish if there are differences compared to the CS in terms of incident diseases, prevalent diseases, and use of health services, and estimate the magnitude of differences from statistical analyses of data retrieved in a systematic review of data published in the literature and other sources of information.
Methods
The protocol for this systematic review (SRL) was registered on PROSPERO (Registration number: CRD42021279234) before starting the literature search. A systematic and exhaustive literature search was carried out. The entire process followed the international quality standards used by the Cochrane Collaboration [9]. The review was guided by the following research question: What is the epidemiological profile and the features of the use of health services for the population affiliated to the SS of Colombia?
We took into account all the population linked to the SS as our target population and the main outcomes assessed were: I) the epidemiological profile of communicable and non-communicable diseases, obstetric and maternal conditions, frequent conditions during early childhood, and other conditions (external causes); and II) the use of health services by the population in each insurance scheme.
Inclusion and exclusion criteria
The search and selection of studies and other documents was guided by the elements of the structured question. All documents that presented information on i) the population affiliated to the SS in Colombia, ii) data such as incidence, prevalence, the absolute and relative distribution of communicable and non-communicable diseases, other conditions or pathologies, use of health services, and iii) exclusive information on the subsidized scheme or comparative analysis against the CS were included. This SRL was not limited by language or type of study, and the time frame considered was from 1993 to 2021.
Search strategy
Four bibliographical databases (MEDLINE, Embase, SciELO, and LiLacs) were systematically searched for studies published between January 1st 1993 and September 24th 2021. The threshold was considered to be from 1993 as Law 100 was issued then regarding the classification by health scheme in Colombia.
Relevant literature was identified following search algorithms summarized in Supplementary Table 1. MeSH, Emtree, and DeCS terms such as “epidemiology”, “health insurance”, “subsidized”, “subsidized health insurance scheme”, and “regimens” were used. Additionally, a non-indexed data search was performed on 22 websites related to this topic (Table 1). Studies identified through each database were imported to Mendeley, and then duplicates were identified and removed. The studies were then imported to the program Rayyan [10].
Study selection
The title and abstract screening was performed by two reviewers, LMM and KEO. Disagreements were resolved by consensus between the two reviewers using the Rayyan program and a new review of references.
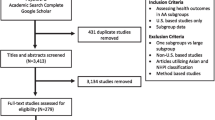
Those studies that met the eligibility criteria previously described were included. The full-text screening was carried out independently by the same two reviewers (LMM and KEO). Disagreements were resolved by consensus between both reviewers. No third reviewer was needed. The complete screening and selection process used was presented using the flow diagram proposed by the PRISMA statement [11].
Data extraction
The relevant data for this systematic review were extracted by one reviewer (LMM) and independently verified by a second reviewer (KEO), using a data extraction form designed in Excel®, which was adjusted after the pilot extraction carried out with two of the articles. The information was extracted by prioritizing studies with a cohort-type epidemiological design, cases and controls, cross-sectional and descriptive observational ones. Subsequently, the information was extracted from documents and epidemiological surveillance reports, and finally, the documents from repositories of academic databases and grey literature.
Quality assessment
The quality assessment was conducted by reviewing each study according to the critical appraisal tool made by the Joanna Briggs Institute [12]. These tools assess focus in different aspects, including: (i) type of design; (ii) how outcome variables were assessed; and (iii) if confounding variables were controlled. Quality assessment was performed by one researcher (LMM). Consensus was reached in consultation with a second author (KEO) as needed. The articles assessed were full-text only: event reports, theses, and non-full-text articles were not assessed.
Analysis of the systematized papers
The synthesis of the information of all the included studies and documents was carried out descriptively. Additionally, synthesis tables were elaborated for the relative frequency measures (incidence and prevalence), or absolute frequency reported in them. The incidences of health conditions were calculated according to five categories of interest: non-communicable diseases, communicable diseases, maternal and obstetric conditions, early childhood health conditions, and other diseases not classified in the previous ones. For each category, the following operational definition was used (Additional file 1: Table 1):
-
Non-communicable diseases: They result from a combination of genetic, physiological, environmental, and behavioural factors.
-
Communicable diseases: They are contagious or infectious diseases, caused by specific infectious agents or their toxic products in a susceptible host.
-
Maternal and obstetric conditions: They are a set of physiological events and pathophysiological alterations that affect women of reproductive age, including in the prenatal, natal, and postnatal periods.
-
Common conditions in early childhood: Group of diseases that frequently occur in boys and girls from 0 to 5 years old. In this group of diseases, perinatal conditions and congenital defects are considered.
-
Other diseases: This refers to external causes such as accidents, trauma, poisoning, and other events that affect the integrity and health of people that are not related to the health conditions already mentioned.
We presented the information according to each category previously mentioned categorized by affiliation scheme. Additionally, an analysis of “health services use” by scheme was performed.
The incidence estimator was calculated using as denominator the population affiliated to the CS or the SS according to the study period, and as a numerator, the number of cases identified. For example, the human immunodeficiency virus (HIV) report in 2020 identified 5167 cases belonging to the SS and the affiliated population for this scheme in the same year was 24,307,637 people, whilst the number of cases reported in the CS was 6213 out of a total of 21,796,582 affiliated. The number of affiliations by scheme were obtained from the Unique Affiliate Database [13].
On the other hand, combined incidence estimations were generated from data from epidemiological surveillance systems at the national level, using metaregressions considering a 95% confidence interval. In addition, random effects models were used weighted by the inverse of the variance of the cumulative incidence calculated for each pathology and each period of time to the data report, considering the high expected heterogeneity due to: incidence estimators for different health conditions grouped in five categories of analysis (non-communicable diseases, communicable diseases, maternal and obstetric conditions, early childhood health conditions, and other diseases not classified in the above) and different observation periods [14,15,16]. The heterogeneity values were confirmed by calculating the I2 estimate. These results are summarized in “forest plot” graphics. In total, 10 models were built using the statistical software STATA 14 [17].
Frequencies of use of health services were calculated for the people affiliated to each scheme, the SS prevalence ratio between the CS and the odds ratio as a measure of association was reported.
Results
Literature search results
In the indexed databases consulted, a total of 5235 references were found and 11,001 references were found in grey literature and official sources such as web pages of official national institutions, repositories of universities, and non-profit organizations. The details of the search results are presented in Table 1.
Of the 16,236 references found, 529 were excluded because they were duplicates, 15,707 were screened by title and abstract, and 735 references were evaluated in full text. Finally, 267 documents were included (see Additional file 1: Tables 2 and 3). The information flowchart is detailed in Fig. 1 (PRISMA).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram
The included studies contain information from 1993 to 2021; 42 articles were obtained from indexed databases [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59]. Of these, four have a retrospective design [24, 32, 33, 53], two are case series [40, 56], and there is one case-control study [39], five cohort studies [25, 30, 38, 52, 54], 27 prevalence studies (cross-sectional) [18, 20,21,22, 26, 27, 29, 31, 34,35,36,37, 41,42,43,44,45,46,47,48,49, 51, 55, 57, 58, 60], one descriptive study [19], and two ecological studies [23, 50]. Through Google Scholar, there are 20 references [61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80], 155 annual reports from the Colombian National Institute of Health (INS) [81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228], two reports from R4V [229, 230], one report from the website of the Ministry of Health and Social Protection [231], and two from the “Cuenta de Alto Costo” [232, 233]. The selected references whose sources were the academic repositories of the Colombian universities numbered 44 – 23 from the National University of Colombia [65, 234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255], 11 from the University of Rosario [81, 119, 153, 256,257,258,259,260,261,262,263], three from the University of Antioquia [264,265,266], three from the University of Andes [267,268,269], two from the University of Bosque [270, 271], and two from the University Javeriana [272, 273].
Of the documents found, 161 came from public and 105 from private sources. The references that contained information at the national level numbered 192, and there were 74 at the regional, departmental, or municipal level. In regard to the type of document, there were three poster summaries, 64 articles, three report summaries of notification events in PowerPoint format, six technical reports of outbreak studies, 22 infographics, 128 reports of epidemiological surveillance events, two press reports, and 38 academic theses. Among the main cities described in the analysed documents are Bogotá, Barranquilla, Medellín, Cali, Tunja, Cartagena, Chocó, Guainía, Pasto, Popayán, Santander, Villavicencio, Manizales, Bucaramanga, and Pereira.
The number of documents and references according to the category of analysis, i.e. health condition and use of health services, is presented in Table 2.
General description of the categories of disease in Colombia
Non-communicable diseases
Incidence data were collected from reports from the National Institute of Health (INS) for mandatory notification events classified as non-communicable diseases: cancer, rheumatoid arthritis, transplants (kidney, heart, liver, lung), rare diseases, malnutrition, and exposure to fluorine.
The data related to the incidence of the disease comprised 25 reports [100,101,102, 116,117,118, 130, 132, 137, 146, 147, 149, 150, 154, 194, 232, 233, 276, 277] and 33 with data on the distribution of diseases in morbid groups of patients [20, 26, 30, 32, 35,36,37,38, 41, 48, 52, 54, 61, 62, 65, 66, 70, 73, 235,236,237, 249, 251, 256, 266, 268, 270, 272, 274, 275, 278, 279, 292].
Communicable diseases
INS reports were the main source of information for this category, including data on diseases such as ophidian accidents, attacks by animals transmitting rabies, acute Chagas, chronic Chagas, chikungunya, dengue, chickenpox, malaria, diphtheria, equine encephalitis, meningococcal disease, yellow fever, typhoid and paratyphoid fever, hepatitis B, hepatitis A, infections associated with medical-surgical procedures, acute respiratory infections, leishmaniasis, leprosy, leptospirosis, bacterial meningitis, acute flaccid paralysis, mumps, congenital rubella, measles, congenital syphilis, accidental tetanus, whooping cough, tuberculosis, HIV AIDS, and Zika. Seventy-eight documents were included [9, 21, 29, 31, 35, 36, 46, 49,50,51,52, 58, 59, 77,78,79,80, 85, 88, 90, 92, 93, 95,96,97,98,99, 101,102,103,104, 108,109,110,111,112,113,114,115,116,117,118,119,120,121,122, 124,125,126,127, 130,131,132,133, 135,136,137,138, 142,143,144,145,146,147, 149,150,151,152,153,154, 156,157,158,159,160,161, 165, 170, 171, 175, 176, 180, 182, 183, 185, 187, 189, 192,193,194,195,196, 198, 199, 202, 205, 206, 208, 218, 221, 262,263,264,265,266,267,268,269,270,271,272,273] and 15 studies offered information on the distribution of the population in the subsidized scheme [22, 25, 40, 63, 69, 71, 103, 222, 242, 249, 258, 267, 269, 273, 286].
Maternal and obstetric conditions
For the conditions that affected women in a fertile period, 10 studies were taken into account that indicated the incidence of the following alterations, namely gestational syphilis, maternal mortality and extreme maternal morbidity [84, 87, 88, 93, 109,110,111, 113, 114, 145] and six [39, 55, 119, 243, 250, 259] showing the distribution of their population according to the affiliation scheme (CS and SS).
Common conditions in early childhood
This category included 11 references, nine from INS reports, and two articles resulting from indexed databases [72, 91, 94, 129, 162, 168, 178, 191, 219, 276, 277], reporting incidences of health conditions and early childhood illness as outcomes such as: underweight at birth, perinatal mortality, late neonatal mortality, and congenital malformations. Five studies showed the distribution of their population for the SS and CS [21, 53, 74, 244, 247].
Other diseases
For the category “other diseases”, 10 references were considered, of which eigth events’ data came from INS reports [101, 206, 221, 222, 288,289,290,291] and two results from other sources [76, 239]. The incidence of cases of pathologies was taken into account: violence from gender and domestic violence, external causes due to aesthetic procedures and consumption accidents, intoxications, sexual abuse, and maxillofacial trauma.
Epidemiological behaviour of disease categories according to insurance schemes (SS and CS)
Subsidiary scheme
Non-communicable diseases
The non-communicable diseases that had the highest incidence during the observation period (2016–2021) was cancer (all types) for the year 2020. Heart, lung, and kidney transplants with living donors represented the fewest incidents. Details of the data can be found in Additional file 2: Table 1.
The combined measure of cumulative incidence for non-communicable diseases in Colombia in the SS during the aforementioned period was 0.000197 (95% CI: 0.000191 to 0.000203). The details of the accumulated incidents by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 1.
From the studies that described the frequency distribution of non-communicable diseases according to the affiliation scheme and that were published between 2004 and 2020, information was obtained on different types of cancer, high blood pressure, asthma, cardiovascular diseases, chronic skin diseases, autoimmune joint inflammatory diseases, nutritional deficiencies, and diseases of the oral cavity. The conditions whose number of cases in the SS was higher than those in the CS were breast cancer, chronic diseases in general, and epilepsy. Details are presented in Additional file 3: Table 1.
Communicable diseases
For this category, 78 documents were considered including reports and studies. Thirty-two pathologies were included for the observation period 2012 to 2021, with chickenpox and chikungunya having the highest incidence and neonatal tetanus and diphtheria having the lowest incidence of cases (Additional file 2: Table 2). The cumulative incidence for SS was 0.000124 (95% CI: 0.000120 to 0.000127). The details of the cumulative incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 2.
From the studies that described the frequency distribution of communicable diseases according to the affiliation scheme and that were published between 2011 and 2021, information was obtained on vector-borne diseases, acute respiratory infection, tuberculosis, sexually transmitted infections, and intestinal parasitic infection. Except for acute respiratory infection, multi-drug-resistant tuberculosis, and Zika, all the other communicable conditions had a greater number of cases in the SS than in the CS in the cohorts studied. The conditions with the highest SS/CS ratio were Chagas disease, congenital syphilis, and gestational syphilis. Details are presented in Table 4 [22, 25, 40, 63, 69, 71, 103, 222, 242, 249, 258, 267, 269, 273, 286].
Maternal and obstetric conditions
The INS was the main source of information for this category, taking incident data from conditions such as extreme maternal morbidity between the years 2010 and 2021. Of the total number of 10 reports included, extreme maternal morbidity was the condition with the highest incidence, and maternal mortality was the one with the lowest incidence (Additional file 2: Table 3). The pooled incidence measure for the SS was 0.000166 (95% CI: 0.000131 to 0.000201). The details of the accumulated incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 3.
The studies that described the frequency distribution of obstetric and maternal conditions according to the affiliation scheme were published between 2010 and 2021. It can be seen that the conditions whose number of cases in the SS was higher than those in the CS were maternal mortality and extreme maternal morbidity [39, 55, 119, 243, 250, 259]. Those details are presented in Table 5.
Common conditions in early childhood
For this category, the information was obtained from nine INS reports and two studies from other sources [72, 91, 94, 129, 162, 168, 178, 191, 219, 276, 277]. Congenital malformations were the pathology with the largest number of new cases. The result of the combined incidence measure was 0.061682 (95% CI: 0.060620 to 0.062744) for the SS. The cumulative incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 4. Of the studies that described the frequency distribution of non-communicable diseases according to the affiliation scheme and that were published between 2014 and 2016, information was obtained on infant death and congenital malformations, with a ratio of 2.1 to 1 of cases in the SS to the CS [74, 244, 247]. Details are presented in Table 6.
Other diseases
This category comprised information from 11 references – nine from the INS between 2018 and 2021, and two studies published in 2015 and 2017 from the literature. For the SS, sexual abuse and intra-family and gender violence were the events with the highest incidence and injuries from external causes caused by accidents related to the consumption of psychoactive substances and aesthetic procedures had the lowest (Additional file 2: Table 5). The cumulative incidence for this scheme was 0.000397 (95% CI: 0.000374 to 0.000420). The details of the accumulated incidents by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 5.
Contributory scheme
Non-communicable diseases
For the CS, the non-communicable diseases with the highest incidence were cancer and rheumatoid arthritis, and those with the lowest incidence were kidney and pancreas transplantation and lung transplantation. The cumulative incidence was 0.000526 (95% CI: 0.000506 to 0.000546). The cumulative incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 6.
From the studies that described the frequency distribution of non-communicable diseases according to the affiliation scheme and that were published between 2004 and 2020, it is evidenced that dental conditions, cancer, and cerebrovascular disease presented a lower number of cases for the CS than for the SS (Additional file 2: Table 1).
Communicable diseases
Of the 32 pathologies analysed from 2012 to 2021, the cumulative incidence for the CS was 0.000171 (95% CI: 0.000165 to 0.000177) (Additional file 2: Table 2). Chickenpox, malaria, and dengue were the diseases with the highest incidence, while acute Chagas and equine encephalitis had the lowest incidence. The details of the accumulated incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 7.
Among the documents that characterized the distribution of pathologies by scheme, it was found that multi-drug-resistant tuberculosis and acute respiratory infections presented a higher ratio of cases to the SS (see Table 4).
Obstetric and maternal conditions
For this scheme, the obstetric and maternal condition with the highest incidence was extreme maternal morbidity, while maternal mortality had the lowest. The cumulative incidence was 0.000107 (95% CI: 0.000088 to 0.000127). The details of the accumulated incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 8.
From the studies that described the frequency distribution of non-communicable diseases according to the affiliation scheme, the ratio of cases of extreme maternal morbidity for the CS is 2.6 to 1 compared to the SS of the SIVIGILA data. For maternal mortality and morbidity and mortality combined, the number of cases is lower in the CS than in the SS [21, 39, 53, 55, 119, 243, 250, 259]. Details are presented in Table 5.
Common conditions in early childhood
The early childhood disorder with the highest incidence in the CS was neonatal death, and congenital defects had the lowest incidence. This scheme’s pooled incidence result of common conditions in early childhood was 0.048309 (95% CI: 0.047478 to 0.049141). These data came mostly from INS reports and information was identified between 2009 and 2021. The details of the cumulative incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 9. Infant mortality presented a ratio of 2.4 for the CS to the SS [39, 45, 69, 217], as identified in Additional file 2: Table 4.
Other diseases
In the CS, the cumulative incidence for this category was 0.000309 (95% CI: 0.000284 to 0.000333), with intra-family and gender violence having the highest incidence and alterations due to external causes secondary to cosmetic procedures having the lowest. The source of information was the mandatory reports of the INS SIVIGILA. The details of the cumulative incidences by affiliation scheme are presented in Table 3 and their graphic representation in the forest plot of Additional file 2: Illustration 10.
Comparison of disease burden between SS and CS
The relative risk for non-communicable and communicable diseases as categories was lower in the SS than in the CS (RR: 0.37 and 0.72, respectively, p-value < 0.05); however, for the other three categories, although differences are found, these represent a greater risk for the population affiliated to the SS, where it is found, for example, that the risk of presenting obstetric and maternal conditions in the SS versus the CS is RR 1.55, while for frequent conditions of early childhood it is RR 1.28, and for other conditions RR 1.28, with a p-value of < 0.05 in all cases. Details are presented in Table 3.
Non-comparative SS disease burden
This section presents descriptive information from the retrieved articles analysing morbid cohorts with data only for the SS or CS; the study designs do not allow for a formal statistical comparison. The information presented ranges between the years 1993 and 2021, with data related to pathologies such as infant malnutrition, pertussis infection, accidental tetanus, ophidian accident, leishmaniasis, gestational syphilis, maternal mortality, malaria, cancer (solid and haematological tumours), leptospirosis, leprosy, yellow fever, acute Chagas disease, Zika, congenital defects, dengue, puerperal endometritis, infections associated with medical-surgical procedures, chronic diseases, sexually transmitted diseases, maternal complications, HIV, intestinal parasites, perinatal death, and migraine.
Different type of documents: academic theses, reports of mandatory notification events, infographics, technical reports of outbreak studies, scientific articles, and poster summaries were identified, coming from both public and private entities.
Non-communicable diseases
The information presented contains data from between 1998 and 2021. The three reports presented by the INS corresponding to the pathology of cancer in children under 18 years of age and acute, moderate, and severe malnutrition in children under 5 years of age for 2021 and 2020, 33, 66, and 64% of cases occurred in the SS, respectively (Table 7).
Agudelo [234] carried out an ecological study published as an academic thesis whose objective was to establish the behaviour of mortality due to child malnutrition in children under 5 years of age in Colombia and its relationship with some social determinants of health; the data source came from the National Administrative Department of Statistics information bases. A total of 12,165 deaths were found and the results show that the correlation between the SS and mortality due to malnutrition in children under 5 years of age, children under 1 year, and children aged between one and four was 0.2057 (Spearman Rho) p-value: 0.0000; Rho 0.1933 p-value: 0.0000 and 0.2147 (Spearman Rho) p-value: 0.0000, respectively.
Afanador-Echeverri et al. [57] presented an abstract in which the current epidemiological situation of migraine in Colombia was analysed, estimating the general prevalence of migraine by geographic area, based on the data obtained from the individual records of provision of services (IRPS) database. This study included a total of 429,816 participants between the years 2014 and 2018, of which 68.8% of the diagnoses were in SS patients and 26.8% in CS patients.
On the other hand, Parra-Lara et al. [18] present a poster summary whose main objective was to analyse the five-year global survival of patients with gastric cancer concerning the health scheme and the place of residence (rural or urban) in a specialized health centre in the city of Cali. A total of 500 cases of gastric cancer were included, and the main outcome (five-year overall survival) was different for patients affiliated to the SS at 14.96% (95% CI: 4.61 to 30.95) versus 26.69% (95% CI: 19.9 to 33.94) for the CS patients (p-value: 0.0089).
Castañeda et al. [248] carried out an academic thesis (retrospective cohort) that aimed to describe the burden of disease due to acute paediatric leukaemia (APL) and identify its association with inequalities in terms of affiliation scheme and department of origin in Colombia during the period 2011–2012. The data sources used were the IRPS and vital statistics registered in the DANE of the participating institution. A total of 636 cases of children who died from APL were included. The prevalence of APL for the SS was 9.43 and for the CS it was 9.39, and the mortality rate per 100,000 inhabitants was 1.49 for the CS and 2.19 for the SS.
Communicable diseases
The information related to the SS was found in 37 documents, of which 30 came from the INS. These data report information from between 2010 and 2021. Neonatal trachoma and tetanus accounted for all cases in the SS for 2019 and 2020, and neonatal tetanus for 2020 and 2021. The information is detailed in Additional file 3: Table 2.
Cardona et al. (2014) [78], published a study on the prevalence of positive cytology results for bacterial vaginosis, candidiasis, and trichomoniasis between 2010 and 2012 in the city of Medellín. The study aimed to determine the prevalence of positive cytology results for bacterial vaginosis, candidiasis, and vaginal trichomoniasis. The main source of information was obtained from the cervical cancer detection and prevention programme at the Hospital Metrosalud de Medellín in the SS. A total of 206,035 records from the programme databases were included, with the prevalence of bacterial vaginosis being 18%, and that of candidiasis 4.7%, and trichomoniasis 0.8%. On the other hand, Cardona et al. [64] in another study carried out in the city of Medellín between 2010 and 2011, sought to determine the prevalence of bacterial vaginosis in women from Medellín and whose source of information came from 50 health centres and hospital units. It was found that only 41.48% of the women in the SS were users of family planning methods.
Arrivillaga [58] published a cross-sectional study that aimed to evaluate and analyse the association between adherence to treatment and the social position of women living with HIV. This study was carried out between 2006 and 2008 and was part of the project “Social perspective of adherence to treatment in Colombian women with HIV/acquired immunodeficiency syndrome (AIDS)”. A total of 269 women with HIV/AIDS were included in five cities of the country (Cali, Bogotá, Villavicencio, Pasto, and Medellín). The main results showed that the probability of remaining adhered to treatment is three times lower when the patient is affiliated with the SS (OR = 3478, 95% CI: 1957 to 6181) compared to the CS.
Pinzón-Rondón et al. [46], on the other hand, carried out a study aimed at establishing the relationship between intestinal parasitism in children under 6 years of age and living in environmentally protected areas, without an aqueduct service, in El Codito-Bogotá, Colombia. This cross-sectional study included 144 children aged between four and 70 months and demonstrated that, compared with affiliation to the CS, the children affiliated to the SS presented differences in the risk of intestinal parasitic diseases, although they were not statistically significant (OR = 1.49, 95% CI: 0.48 to 4.68).
Borrero et al. [50] published a study that aimed to evaluate the effect of decentralization in the context of the Colombian health system (SGSSS) on the incidence of malaria in Colombian municipalities. This was an ecological study that performed a univariate analysis between the affiliation scheme and the malaria incidence rate between the years 1998 and 2004. The primary source of information was the departmental and municipal health secretaries. A total of 145 cases met the inclusion criteria. In the bivariate analysis between the type of affiliation and the ratio of malaria incidence rates in the municipalities, it was shown that the proportion of the municipal population belonging to the CS was 0.27 (95% CI: 0.11 to 0.64), and the proportion of the municipal population belonging to the SS was 4.23 (95% CI: 1.98 to 9.00). This means that the higher the proportion of the population affiliated to the subsidized regime, the higher the incidence rates of malaria in the municipalities.
Maternal and obstetric conditions
Six reports from the INS are listed in Table 8 and show that 56.7% of the cases of gestational syphilis for the year 2021 were presented in the SS; likewise, for the year 2020, there was 54.3% of the same pathology in the SS population.
Díaz et al. [264] carried out an ambispective cohort study whose main objective was to determine the factors associated with complications during the third trimester of pregnancy, childbirth, and the puerperium of maternal women belonging to the SS treated in a second-level institution of complexity in Medellín during the year 2012. The cohort included a total of 506 maternal and among the main maternal complications prior to the current pregnancy of the included participants, the prevalence of abortion was 24.5%, pre-eclampsia 8.2%, premature delivery 4.3%, and intrauterine growth retardation 0.9%.
Bolaños et al. [68], in their cross-sectional study, had as their objective to evaluate factors associated with 28 cases of maternal mortality during 2008 in women affiliated to an HPE of the SS, calculating the maternal mortality ratio of 28 deaths per 29,944 live births.
Acevedo [255] carried out a study published as an academic thesis that aimed to identify contextual and individual factors related to maternal health between the years 2011 and 2015 in Vichada. The pregnant women affiliated to the administrative entities of benefit plans (AEBP) of the SS had a maternal mortality ratio of 715.26 deaths per 100,000 live births, and the risk of dying of the pregnant women affiliated to this scheme was five times higher (OR = 5.48; 95% CI: 0.8812 to 226.58) in uninsured pregnant women, although there were no statistically significant differences. There were no cases in women affiliated with the AEBP of the CS or with the exception scheme.
Rivillas et al. [23], in an ecological study whose objective was to measure socio-economic inequality and inequality related to health financing in maternal mortality in Colombia, as well as to identify the potential epicentres of this inequality, indicated that maternal mortality for the indicator of absolute inequity for expenses in health was, in the SS in the year 2012, −10,542, while in 2013 it was −13,979 and in the year 2014 it was −64,781; meanwhile for the CS it was −32,895 in 2012, −23,241 in 2013, and − 17,283 in 2014. This study concluded that there is high inequality in maternal mortality between the regions, and particularly in the SS.
Common conditions in early childhood
Cortés et al. [33], who published a retrospective descriptive study that characterized perinatal mortality in Manizales between 2009 and 2012 according to socio-demographic, clinical, and healthcare variables, affiliation scheme, and their relationships, showed that the perinatal mortality rate during the years mentioned was 8.9 per 1000 live births in the CS, and 9.8 per 1000 live births in the SS, while the frequency of perinatal mortality was similar in both affiliation schemes (CS = 50.9% and SS = 49.1%).
Behaviour in the use of health-care services according to affiliate schemes in Colombia
The use of health services in affiliation schemes in Colombia is described in studies and reports that informed the distribution of use differently. The number of references included was 21, which reported information between 2009 and 2021. Details are presented in Additional file 3: Table 3.
In this table, the rates of higher frequency of use of health services in the regimens were established, and it is found that the use of radiotherapy, chemotherapy, radiotherapy, and mastectomy, among others, is greater when exposed to the SS compared to the CS (Additional file 3: Table 3).
Additional file 3: Table 4 shows in greater detail a study developed by the MHSP evaluating the quality of care provided in Colombia in 2014. The data showed that there is a greater risk of consumption of services, specifically for drug delivery services, hospitalization, requesting procedures from the HPE in person, and not requesting procedures from the HPE when exposed to the SS than when exposed to the CS.
For the use of services concerning health promotion, prevention, and surgery there were no statistically significant differences between the SS and the CS, and it is notable that the risk of consuming resources for general medicine services, laboratory tests, specialized medicine, emergencies, dentistry, radiography and images, priority appointments, therapies, and requesting medical appointments via telephone or the Internet is lower when you are exposed to the SS compared to the CS.
Zúñiga [271] published an analytical observational study, conducted in 2018, which aimed to analyse inequality in prenatal care live births in Colombia by type of health insurance. The database of the registry of live births was analysed, with a total of 459,238 records, and within the results were found a mean number of prenatal controls for the SS of 6.04 (95% CI: 6.03 to 6.05) while for the CS it was 7.40 (95% CI: 7.39 to 7.41). Likewise, mothers affiliated to the SS were 3.5 times more likely (OR = 3.545; 95% CI: 3.479 to 3.611) to have four or fewer prenatal check-ups than those affiliated to the CS (OR = 0.288; 95% CI: 0.283 to 0.294).
Additional file 3: Table 5, on the other hand, shows the distribution of health services according to the affiliation scheme of the study population. Information was obtained from three studies, carried out between 2009 and 2019, where services such as delivery care and time of health-care attention were evaluated, with a ratio of between 5.41 and 1 cases in the SS to the CS.
Quality assessment
Thirty-seven original articles described previously were assessed according to the study design. Other documents included, such as event reports, academic theses, outbreak reports, news, infographics, and epidemiological reports, were not included. Twenty-nine articles were classified as cross-sectional studies. Eight articles [19, 21, 23, 29, 33, 41, 47, 50] were considered of high concern due to the risk of bias mainly because of the lack of information regarding the subject’s settings and the sample size. Three [32, 52, 54] out of seven cohort studies were flagged as being of high concern because of the risk of bias due to unclear information about exposure measures, whether control or exposed groups. One [56] study was evaluated with a case series tool and this was considered to be of low concern in terms of risk of bias. For more information see Additional file 4.
Discussion
The objective of this study was to identify the epidemiological profile of the population affiliated with the SS in Colombia, to establish whether there are differences compared to the CS in terms of prevalence and incidence of diseases, and use of health services, and to estimate the magnitude of the differences from statistical analyses of the data retrieved in a systematic review of data published in the literature and other sources of information. As a main result, it was determined that there are significant differences in the use of health services, and in the incidence and prevalence of diseases between the population affiliated to the SS and that affiliated to the CS in Colombia. The main differences found account for the existence of a greater burden of disease in terms of morbidity and mortality for the SS in the categories of obstetric and maternal conditions, which include maternal morbidity, extreme maternal morbidity, maternal and perinatal mortality (RR 1.5), the category of frequent childhood conditions with an RR of 1.27, and finally the category of other diseases or conditions, among which injuries due to violent causes stand out (RR 1.28).
These findings can be explained by the greater vulnerability of the population in these categories. The pregnant population, for example, is more vulnerable to access barriers in the provision of health services; these barriers translate into absent or incomplete prenatal controls, which increases the risk of detection, management, and prevention of complications typical of this physiological state with consequences that can be catastrophic for the mother and the product of the pregnancy.
Likewise, it is not unknown that the population affiliated to the SS presents vulnerability characteristics secondary to precarious access to essential public services, the quality of food, transportation, and restricted movement, either due to its location in dispersed areas or to difficult access when found within population centres. These characteristics, added to the existing biological vulnerability in children under 5 years of age, cause the risk of morbidity and mortality to be greater in this age group, while malnutrition, mortality associated with malnutrition, congenital malformations, and postnatal nutritional deficiencies, among others, are problems that occur more frequently in the population affiliated with the subsidized scheme and are mediated beyond the biological substrate by social determinants of health.
Also, the different forms of violence that are monitored in the national information systems were predominant in the population affiliated to the SS. This gender violence, intra-family violence, as well as sexual abuse, intoxication, and consumption accidents, can be understood as a manifestation of unsatisfied basic needs, gender inequalities, a lack of purchasing power, unemployment, inequality in income, level of education [292] and socio-cultural patterns and historical violence such as armed conflict, which demarcate differences in social positions [293].
Other important findings were the significant differences in the incidence of communicable and non-communicable diseases between those affiliated with the SS and CS, with a higher risk of incidence in the population affiliated with the CS. This finding, which is contrary to what is expected given the marked additional risk that has been described for the occurrence of these diseases in a population with a higher degree of vulnerability [55, 294, 295], has two explanations. The first is related to the quality of health information systems and registries at the national level, which constituted a primary source of information for this analysis. It is recognized that the information for the SS and the characterization of the use of health system resources, as well as the burden of disease in its affiliates, is deficient, not representative, and in most cases not available, which may mean in this case an under-reporting of the number of cases and the systematic deviation of these incidents towards an underestimation. Also, structural and intermediate problems of the health system, related to the location of residence of the population affiliated to the SS, deficiencies in transportation, limitations in mobility due to civil security problems, and the location and organization of service-providing institutions, constitute barriers that limit the access of this population to care, so that care is not received in the institutions and consequently they are not recorded in the information systems. This problem also generates a bias in incidence reports with a tendency to underestimate.
The characterization of the prevalence of communicable and non-communicable diseases in the country according to the scheme comes from more representative studies, albeit fragmented by regions or municipalities in many cases. The distribution of cases in the identified morbid cohorts shows a ratio greater than 1 in the cases of patients affiliated to the SS versus the CS who have chronic diseases such as cardiovascular disease and arterial hypertension (ratio 1.3:1), skin lesions, mortality due to nutritional deficiencies, and malnutrition that represent cases of the SS to the CS in a ratio of approximately 2:1, or in the case of epilepsy or other chronic diseases that represent cases of the SS to the CS in a ratio of > 3:1.
This same pattern was observed in communicable diseases such as the occurrence of acute Chagas disease, tuberculosis, sexually transmitted diseases, HIV, intestinal parasitic infection (> 1:1), congenital and gestational syphilis, and chronic Chagas disease (> 4:1). The relative risk of the occurrence of communicable diseases such as leprosy, congenital syphilis, whooping cough, Zika, leishmaniasis, equine encephalitis, malaria, trachoma, and neonatal tetanus is also higher in the population affiliated to the SS than in the CS.
It is especially noteworthy in this study that in the morbid cohorts with cancer in which there is a report in national databases, the largest number of affiliates are found in the CS. Another important finding in this study is related to the presentation of the disease in the population affiliated to the SS, its severity, and the differential behaviour of the clinical course of some of them. In one of the studies included in this analysis, it was evident, at least for the population in Cali, how screening services for malignant breast disease are provided in a 0.5:1 ratio in women from the SS compared to those from the CS, and in women who were diagnosed with breast cancer there was a 2.8 times higher risk of requiring mastectomy among women with this condition affiliated to the SS than in those affiliated to the CS, which may be a proxy for the severity of the disease at the time of diagnosis.
The differences found in the course of the disease are also relevant and induce a reflection on the process of care within the IPS for the population affiliated to one or other scheme. For example, in Bogotá, by 2020, it was found that the risk of having a patient with rheumatoid arthritis with high disease activity at the beginning of the two-year follow-up was lower in the SS than in the CS (OR 0.1); however, upon completing the follow-up time, the risk of presenting high disease activity was higher in the SS than in the CS (OR 1.8), reversing the trend observed at the beginning of follow-up in patients. Also, in delivery care, caesarean sections were more frequent in the CS than in the SS. These findings denote a possible differential approach and other factors that mediate the differential health outcomes in the population that demands and accesses health services in each of these schemes.
Other greater risks that in turn determine a greater burden of disease in SS patients are related to a greater possibility of having failed tuberculosis treatments (OR 1.3) or fewer complete treatments (OR 0.4), and a greater possibility of having refractory epilepsy (OR 4.6), abandonment of breastfeeding (OR 1.3), fewer promotional and preventive activities such as vaginal cytology (OR 0.8), complete vaccination schedules (OR 0.4), or a higher risk of having complete but late vaccination schedules (OR 2.4).
In regard to the use of services offered in the health system, the trend was also evident in terms of relative frequencies towards less use of health services in the SS than in the CS. Such is the case for general medicine services, medication delivery, laboratory tests, specialized medicine, emergency service care, dentistry, radiology and imaging, priority appointment care, and therapies. However, the risk of requiring hospitalization in the population affiliated to the SS is greater than that among those affiliated to the CS (OR 1.65). The use of prevention and promotion health services (P&P) and the performance of surgical procedures do not imply an additional risk in any of the schemes (OR 1.0).
This trend in the differential use of health services, with a lower frequency of use and care in the SS, is understandable to the extent that the population affiliated to this scheme has greater barriers to accessing health services located beyond the provision of services and availability of health technologies. Among them, the characteristics of informality in the work activity generate competition between seeking care and obtaining income that guarantees subsistence. The lower availability of tools that facilitate the request for health-care services and their continuity, such as the telephone or Internet service or the lack of knowledge and appropriate use of this resource, is a fact that again impacts the need for transfers in person to the institutions or service points to request for healthcare services. This confronts them with access barriers generated by problems due to a lack of transportation, mobility, geographical areas and barriers, and the availability of economic resources to access the request for health services. This last phenomenon was also evident in this study, where it was found that the request for health services in person is 3.6 times higher in the SS, so it also occurs with procedures in person (OR 2.1) and in the worst cases the non-request for procedures or services is 1.7 times more frequent in the population affiliated with the SS.
This study, which sought to identify the differences in the incidence and prevalence of diseases and the use of health services between the affiliation schemes (subsidized and contributory) in Colombia, is the first of this nature, and integrates information available in the literature and sources from administrative bases and epidemiological surveillance in Colombia, combining advanced statistical methods for the estimation of combined measures of incidents and analysis of prevalences in each scheme. Additionally, formal statistical tests were carried out, which made it possible to find and quantify the magnitude of the existing differences in the occurrence of disease and the use of health services in Colombia for these two health affiliation schemes.
The sources of information in turn suppose important limitations – among them, the categories of diseases generated a priori could only be fed with information on health conditions and diseases with information available in the literature or the surveillance information bases, however they do not constitute all of the diseases that are part of these categories, and in some cases they are not the most frequently presented.
Conclusion
This study allowed us to conclude that there are differences in the incidence, prevalence, and use of health services between health affiliation schemes (SS and CS) in Colombia. For the categories configured in the framework of this study as communicable and non-communicable diseases, the data showed a greater risk of becoming ill from this cause in the population affiliated to the CS; however, the certainty in this estimate is very low given the potential biases of information, selection, and measurement detected in the information sources, which even allows an underestimation of the incidences and prevalences of the conditions reported in the SS. For the categories of obstetric and maternal conditions, frequent conditions in early childhood, and other diseases, the risk of occurrence was higher in those affiliated to the SS than among those in the CS. The use of health services is also different by scheme, with less demand, access, and provision in health services for general consultation, dentistry, drug delivery, and emergency consultation, among others, in the SS, probably mediated by social determinants of health, other than the availability of health technologies. However, the risk of requiring hospitalization is greater in those affiliated to the SS.
These results not only allow the differences that are presumed in the configuration of health in the populations belonging to the SS and CS in Colombia to be quantified and quantitatively demonstrated, but they can also guide decision-making regarding the aspects necessary for the actuarial estimation of values to be recognized by people according to the health insurer’s scheme. It is necessary that aspects such as the social characteristics of the population are taken into account in the planning, organization, and management of health risk, given that they are determinants of the burden of disease and health results, as well as the configuration of ways that health care services available are using, as well as barriers that impact the entire care process. There are many limitations in the recovered evidence, so it is necessary to promote studies that seek not only to overcome these limitations and reduce the risk of bias from the design but also to achieve a greater degree of representativeness at the national level.
Availability of data and materials
The data and materials will be made available if required.
Abbreviations
- AIDS:
-
Acquired immunodeficiency syndrome
- APL:
-
Acute paediatric leukaemia
- AEBP:
-
Administrative entities of benefit plans
- BSS:
-
Beneficiary Selection System
- CPU :
-
Capitation payment unit
- CI :
-
Confidence interval
- CS:
-
Contributory scheme
- SGSSS:
-
General System of Social Security in Health
- HBP:
-
Health benefit plan
- HPE :
-
Health-promoting entity
- HSPI:
-
Health service provider institution
- HIV:
-
Human immunodeficiency virus
- IRPS:
-
Individual Service Provision Registry
- R4V:
-
Interagency Coordination Platform for Refugees and Migrants from Venezuela
- MHSP:
-
Ministry of Health and Social Protection
- DANE:
-
National Administrative Department of Statistics
- INS:
-
National Institute of Health
- OR :
-
Odds ratio
- P&P:
-
Promotion of health services
- SIVIGILA:
-
Public Health Surveillance System
- SS :
-
Subsidized scheme
- SRL:
-
Systematic review of literature
- TB :
-
Tuberculosis
References
Ministerio de Salud y Protección Social. Aseguramiento al Sistema General de Seguridad Social: Minsalud; 2017. p. 63. Available from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VP/DOA/RL/cartillas-de-aseguramiento-al-sistema-general-de-seguridad-social-en-salud.pdf
Ministerio de Salud y Protección Social. Resolucion 2503 de 2020. Vol. 93, Acta Medica Scandinavica; 2009. p. 22–70.
Ministerio de Salud y Protección Social. Unidad de pago por capitación del regimen subsidiado; 2021. p. 1. Available from: https://www.minsalud.gov.co/salud/Paginas/UPC_S.aspx [cited 8 Sep 2021]
Nieto López E, Londoño FJ. Factores socioeconómicos y aseguramiento en salud en el área urbana de Colombia. Fac Nac Salud Pública El Escen para la salud pública desde la Cienc. 2001;19(1):2.
Ministerio de Salud y Protección Social. Resolucion 2503 del 2020. Acta Med Scand. 2009;93(S85):22–70.
Ministerio de Salud y Protección Social. La equidad en Salud para Colombia. Bogotá: Brechas internacionales y territoriales; 2015.
Mejía-Mejía A, Sánchez-Gandur AF, Tamayo-Ramírez JC. Equidad en el Acceso a Servicios de Salud en Antioquia, Colombia TT - Equity in access to health-services in Antioquia, Colombia. Rev Salud Publica (Bogota). 2007;9(1):26–38 Available from: http://www.scielosp.org/scielo.php?script=sci_arttext&.
Hilarión-Gaitán L, Díaz-Jiménez D, Karol Cotes-Cantillo CC-O. Vista de Desigualdades en salud según régimen de afiliación y eventos notificados al Sistema de Vigilancia (Sivigila) en Colombia, 2015. Biomedica. 2019; Available from: https://revistabiomedica.org/index.php/biomedica/article/view/4453/4274 [cited 12 Sep 2021].
Garritty C, Gartlehner G, Kamel C, King VJ, Nussbaumer-Streit B, Stevens A, et al. Interim guidance from the cochrane rapid reviews methods group. Cochrane Rapid Rev. 2020;2020:1–2 Available from: https://methods.cochrane.org/rapidreviews/sites/methods.cochrane.org.rapidreviews/files/public/uploads/cochrane_rr_-_guidance-23mar2020-final.pdf.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):1–10.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberatî A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. 2015; Available from: http://www.crd.york.ac.uk/prospero [cited 16 Sep 2021].
Adelaide. TU of. critical-appraisal-tools - Critical Appraisal Tools | Joanna Briggs Institute. The University of Adelaide. Available from: https://jbi.global/critical-appraisal-tools. [cited 3 Jan 2022]
ADRES. Base de Datos Unica de Afiliacos - BDUA. Bogotá: ADRES; 2021. [cited 2021 Dec 5]. Available from: https://www.adres.gov.co/eps/procesos/bdua.
Wang N. How to Conduct a Meta-Analysis of Proportions in R: A Comprehensive Tutorial. 2018. https://doi.org/10.13140/RG.2.2.27199.00161.
Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Heal. 2014;72(1):1–10.
Lipsey M. Practical meta-analysis. Thousand Oaks: Sage Publications; 2001. p. 247.
StataCorp. Stata: Software for Statistics and Data Science | Stata. 2021 Available from: https://www.stata.com/ [cited 5 Dec 2021].
Parra-Lara L, Falla-Martinez J, Bravo J, Zambrano A, Bravo L. Health disparities and gastric cancer survival in Cali, Colombia: a hospital-based study. Ann Oncol. 2019;30(Supplement 4). https://doi.org/10.1093/annonc/mdz155.340.
Mejía-Mejía A, Sánchez-Gandur AF, Tamayo-Ramírez JC. Equidad en el acceso a servicios de salud en Antioquia, Colombia. Rev Salud Publica. 2007;9(1):26–38.
Martínez-Pérez DC, Gómez-Wolff LR, Ossa-Gómez CA, Hernández-Herrera GN, Rivas-Bedoya Y, García-García HI. Association between delayed diagnosis and breast cancer in advanced clinical stage at the time of consultation in four oncology centers in Medellin-Colombia, 2017. Cross-sectional study. Rev Colomb Obstet Ginecol. 2020;71(2):9–24.
Briceño-Ayala LL, Pinzón-Rondón ÁMÁM, Zárate-Ardila CJCJ. Acceso, seguridad e integralidad en registros de gestantes colombianas entre los años 2007 al 2009. Ciencias Salud. 2015;13(3):355–67.
Ettenger A, Bärnighausen T, Castro A. Health insurance for the poor decreases access to HIV testing in antenatal care: evidence of an unintended effect of health insurance reform in Colombia. Health Policy Plan. 2014;29(3):352–8.
Rivillas JC, Devia-Rodriguez R, Ingabire M-G. Measuring socioeconomic and health financing inequality in maternal mortality in Colombia: a mixed methods approach. Int J Equity Health. 2020;19(1):98.
Hilarión-Gaitán L, Díaz-Jiménez D, Cotes-Cantillo K, Castañeda-Orjuela C. Desigualdades en salud según régimen de afiliación y eventos notificados al Sistema de Vigilancia (Sivigila) en Colombia, 2015. Biomedica. 2019;39(4):737–47.
Paniagua-Saldarriaga LA, Pelissari DM, Rueda ZV. Factors associated with unsuccessful outcomes of tuberculosis treatment in 125 municipalities in Colombia 2014 to 2016. Am J Trop Med Hyg. 2021;105:1326–34.
Hernández Bernal NE, Bulla AP, Mancilla López E, Peña Peña LV. Prevalencia de lesiones de piel asociadas a la dependencia física en geriátricos e instituciones de salud de Tunja. Gerokomos. 2021;32(1):51–6.
Díaz-Grajales C, Zapata-Bermúdez Y, Aristizábal-Grisales JC. Acceso y satisfacción con servicios curativos: Análisis de casos en afiliados al régimen contributivo y afiliados al régimen subsidiado en un barrio estrato 2 – Cali, Colombia. Rev Gerenc Polit Salud. 2015;14(29):155–78.
Lopera MM, Lemos Y. Factores socioeconómicos y clínicos asociados con infecciones oportunistas en pacientes con HIV afiliados al sistema de salud. Biomédica. 2019;39(1):186–204.
Gómez-De la Rosa F, Marrugo-Arnedo CA, Florez-Tanus Á, López-Pájaro K, Mazenett-Granados E, Orozco-Africano J, et al. Impacto económico y sanitario del control prenatal en embarazadas afiliadas al régimen subsidiado en Colombia durante 2014. Salud Publica Mex. 2017;59(2):176–82 Available from: http://www.saludpublica.mx/index.php/spm/article/view/7766 [cited 24 Sep 2021].
de Vries E, Uribe C, Pardo C, Lemmens V, Van de Poel E, Forman D. Gastric cancer survival and affiliation to health insurance in a middle-income setting. Cancer Epidemiol. 2015;39(1):91–6. https://doi.org/10.1016/j.canep.2014.10.012.
Cruz LF, Epidemiol M, Girón LN, Enf L, Velásquez R, García LM, et al. Coberturas de vacunación en el Valle del Cauca, 2002. Colomb Med. 2003;34:17–23.
Barahona-Correa JE, Flórez-Suárez J, Coral-Alvarado P, Méndez-Patarroyo P, Quintana-López G. Does healthcare regime affiliation influence the clinical outcomes of patients with rheumatoid arthritis? Clin Rheumatol. 2021;40(3):877–86.
Bernal Cortés DP, Cardona RD. Caracterización de la mortalidad perinatal en Manizales, Colombia 2009-2012. Hacia Promoc Salud. 2014;19(2):2009–12.
Díaz-Grajales C, Zapata-Bermúdez Y, Aristizábal-Grisales JC. Acceso a los servicios preventivos en los regímenes contributivo y subsidiado de salud en un barrio estrato dos de la ciudad de Cali. Rev Gerenc Polit Salud. 2011;10(21):153–75.
Gómez-Mercado CA, Segura-Cardona AM, Pájaro-Cantillo DE, Mesa-Largo M. Incidencia y determinantes demográficos de la leucemia linfoide aguda en pacientes con cáncer pediátrico, Antioquia. Univ Salud. 2020;22(2):112–9.
Pinilla A, Cano N, Granados C, Paez-Canro C, Eslava-Schmalbach J. Inequalities in prescription of hydrochlorothiazide for diabetic hypertensive patients in Colombia. Rev Salud Publica. 2011;13(1):27–40 Available from: http://www.scielosp.org/pdf/rsap/v13n1/v13n1a03.pdf.
Garcés-Palacio IC, Altarac M, Kirby R, McClure LA, Mulvihill B, Scarinci IC. Contribution of health care coverage in cervical cancer screening follow-up: findings from a cross-sectional study in Colombia. Int J Gynecol Cancer. 2010;20(7):1232–9.
Egurrola-Pedraza JA, Gómez-Wolff LR, Ossa-Gómez CA, Sánchez-Jiménez V, Herazo-Maya F, García-García HI. Diferencias en supervivencia debidas al aseguramiento en salud en pacientes con cáncer de mama atendidas en un centro oncológico de referencia en Medellín, Colombia [Survival difference due to types of health coverage in breast cancer patients treated at a specialized cancer center in Medellín, Colombia]. Cad Saude Publica. 2018;34(12):e00114117. Spanish. https://doi.org/10.1590/0102-311X00114117.
Yepes FJ, Gómez JG, Zuleta JJ, Londoño JL, Acosta-Reyes JL, Sánchez-Gómez LH, et al. Healthcare and maternal morbidity and mortality: a hospital-based case-control study in two regions of Colombia (Bogotá and Antioquia), 2009-2011. Cad Saude Publica. 2016;32(11):e00080215.
Zabaleta A, Llerena C. Serie de casos: tuberculosis extremadamente resistente a drogas en Colombia, 2006-2016. Biomédica. 2019;39(4):707–14.
Osorio J. Prevalencia de caries e índice COP en población escolar de 12 años del municipio de Copacabana 2013-2014. Estomatologia. 2015;23(1):7–14.
Ortiz C, Rúa-Uribe GL, Rojas CA. Conocimientos, prácticas y aspectos entomológicos del dengue en Medellín, Colombia: un estudio comparativo entre barrios con alta y baja incidencia. Biomédica. 2018;38:106–16.
Houweling TAJ, Arroyave I, Burdorf A, Avendano M. Health insurance coverage, neonatal mortality and caesarean section deliveries: an analysis of vital registration data in Colombia. J Epidemiol Community Health. 2017;71(5):505–12 Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med14&NEWS=N&AN=27669713.
Rubio-Mendoza ML. Equidad en el Acceso a los Servicios de Salud y Equidad en la Financiación de la Atención en Bogotá. Rev Salud Pública. 2008;10(1):29–43.
Rocha M, Mendez Y, Giraldo M. Evaluation of emotional, Social and access needs of patients diagnosed with chronic myeloid leukemia in Colombia. Value Heal Reg Issues. 2019;19:S24. https://doi.org/10.1016/j.vhri.2019.08.125.
Pinzón-Rondón AM, Gaona MA, Bouwmans M, Chávarro LC, Chafloque J, Zuluaga C, et al. Acceso a agua potable, protección ambiental y parasitismo intestinal infantil en El Codito, Bogotá, Colombia. Rev Salud Pública. 2019;21(1):42–8.
Cardona D, Garzón MO, Calle M, Agudelo MC, Segura Á. Tendencia de la mortalidad y la morbilidad por tos ferina en Colombia, 2002-2012. Biomedica. 2016;36(3):397–405.
Salamanca MEC, Equidad. Equidad en la utilización de servicios de salud en el Sistema General de Seguridad Social en Salud en Colombia; 2011. p. 1–7.
Gutiérrez CC, Reyes-Ortiz C, Borda MG, Arciniegas A. El auto reporte de vacunación en los adultos mayores: Estudio SABE Bogotá, Colombia. Colomb Med. 2016;47(1):25–30.
Borrero E, Carrasquilla G, Alexander N. Decentralization and health system reform: what is their impact on malaria incidence in Colombian municipalities. Biomedica. 2012;32 Suppl 1:68–78.
Garcia-Subirats I, Vargas Lorenzo I, Mogollón-Pérez AS, De Paepe P, da Silva MRF, Unger JP, et al. Determinantes del uso de distintos niveles asistenciales en el Sistema General de Seguridad Social en Salud y Sistema Único de Salud en Colombia y Brasil. Gac Sanit. 2014;28(6):480–8.
Velásquez-De Charry LC, Carrasquilla G, Roca-Garavito S. Equidad en el acceso al tratamiento para el cáncer de mama en colombia. Salud Publica Mex. 2009;51(SUPPL.2):s246–53.
Catalán ÁV. Factors of accessibility related to perinatal death. Rev Investig Programa Enfermería UDES. 2010;1(1):26–34 Available from: http://www.scielo.org.co/pdf/cuid/v1n1/v1n1a05.pdf.
de Charry LC, Carrasquilla G, Roca S. Equidad en la detección del cáncer de seno en Colombia. Rev Salud Publica. 2008;10(4):571–82.
Alvarez-Sierra SP. Demoras en mortalidad materna en el departamento de Santander 2012 a 2015. Rev Salud Pública. 2018;20(6):699–706.
Agudelo Loaiza RD, Medina Arredondo MC, Cardona RD. Caracterización de la sífilis congénita y gestacional en Caldas, Colombia. Arch Med. 2016;16(2):326–34.
Afanador Echeverri GF, Ribero V. Current situation of migraine in Colombia: analysis based on the health services information system (RIPS). Value Health. 2019;22(Supplement 2):S286. https://doi.org/10.1016/j.jval.2019.04.1358 Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed20&NEWS=N&AN=2002156783.
Arrivillaga M, Ross M, Useche B, Alzate ML, Correa D. Social position, gender role, and treatment adherence among Colombian women living with HIV/AIDS: social determinants of health approach. Rev Panam Salud Publica. 2009;26(6):502–10. https://doi.org/10.1590/s1020-49892009001200005.
Benjumea Bedoya D, Arbeláez Montoya MP. Estudio y manejo clínico de menores que conviven con pacientes de tuberculosis pulmonar, Medellín 2010-2011. Iatreia. 2015;28(2):137–47.
Anaya Anichiarico A, Londoño Villaquiran F, Pérez Varela L, Ortiz MR. Caracterización de las pacientes llevadas a cesárea según modelo de Robson y exploración de factores asociados en gestantes atendidas en el hospital Universitario San José de la ciudad de Popayán-Colombia. 1 de enero de 2016 a 30 de junio de 2016. Rev Chil Obstet Ginecol. 2017;82(5):491–503.
Luis F, Jaramillo O. Mortalidad por cáncer en Colombia 2001. Rev CES Med. 2004;18(2):19–36.
Pastrán Alfonso O, Céspedes Nieves G, Ruiz Latriglia MF, Silva PS. Caracterización de personas con discapacidad del municipio de Sopó, Cundinamarca, Colombia. Rev Colomb Rehabil. 2017;7(1):15.
Farías-Curtidor LE, Mejía-Bernal CP, Osorio-Carmona GI, Pérez-Peña LJ, Preciado-Aponte C. Factores de riesgo para el desarrollo de Tuberculosis multidrogorresistente en Colombia, 2008 A 2011. Rev Salud Publica. 2016;18(6):845–57.
Antonio J, Arias C, Arredondo MV. Prevalencia de vaginosis bacteriana en usuarios de una institución prestadora de servicios de salud de Medellín Colombia. Investig Andin. 2015;17(30):1151–65.
Cardona-Arango D, Segura-Cardona Á, Espinosa-López AM. Mortalidad de adultos mayores por deficiencias nutricionales en los Departamentos de Colombia. Rev Salud Publica. 2012;14(4):584–95.
Borda MG, David-Pardo DG, Ríos-Zuluaga JD, López-Zea AI, Forero-Borda LM, Gutiérrez S, et al. Relationship between prostate cancer screening, linkage to the health system and associated factors in older adults from Bogotá, Colombia: secondary analysis of the SABE survey. Urol Colomb. 2018;27(1):35–41.
Emsanar E. Caracterización de pacientes afiliados a la Empresa Promotora de Salud del Régimen Subsidiado (EPS-S)“EMSSANAR”: EMSSANAR; 2015.
Bolaños ÁP, Cuevas AM, Díaz DI. Factores asociados con la mortalidad materna en las afiliadas a una EPS del régimen subsidiado, durante el año 2008. Cuad Latinoam Adm. 2010;6(10):103–18.
Ángel-Müller E, Rodríguez A, Núñez-Forero LM, Moyano LF, González P, Osorio E, et al. The prevalence of and factors associated with C. trachomatis, N. gonorrheae, T. vaginalis, C. albicans infection, syphilis, HIV and bacterial vaginosis in females suffering lower genital tract infection symptoms in three healthcare attention sites in Bogo. Rev Colomb Obstet Ginecol. 2012;63(1):14–24.
Herrera Marcano T, Cachada A, Rocha-santos T, Duarte AC, Roongtanakiat N. Lesiones intraepiteliales de alto grado en la población subsidiada, contributiva y pobre no asegurada en el municipio de Villavicencio, Colombia. 2008. Univ del Rosario. 2009; Available from: https://doi.org/10.1016/B978-0-12-849873-6.00001-7%0Ahttp://saber.ucv.ve/ojs/index.php/rev_venes/article/view/1112.
Sánchez MAE, Romero JAB. Vigilancia epidemiológica de la sífilis gestacional y congénita en el departamento de córdoba, Colombia, 2012- 2016. Rev Salud Pública. 2019;23:7–22.
García Ramírez JA, Vélez ÁC. Social determinants of health and quality of life of the adult population of Manizales, Colombia. Rev Cuba Salud Publica. 2017;43(2):191–203.
Yolanda I, Ávila C, Margarita K, Velasco A, Barón MM. Citología cervicovaginal. Hacia Promoc Salud. 2013;2:123–34.
Ruiz-Murcia FA, Fandiño-Losada A, Ramirez-Cheyne J, Isaza C, Saldarriaga W. Inequidades en el diagnóstico de anomalías congénitas mayores en recién nacidos en Cali, Colombia. Rev Chil Obstet Ginecol. 2014;79(6):481–8.
Lechuga EN, Martínez RP. de las S. Uso de la citología vaginal en mujeres afiliadas al régimen subsidiado atendidas en la unidad hospitalaria la manga de barranquilla (Colombia), 2006. Salud Uninorte. 2008;24(2):191–204.
Morán-Garreta LM, Pinzón-Gomez EM, Muñoz-Villa VH, Lesmes-Duque MC, Victoria-García MC. Abuso sexual en mujeres de 10 a 13 años en el Valle del Cauca, Colombia. Arch Med (Manizales) 2017;17(1):121–0.
Daza V, Jurado W, Duarte D, Gich I, Sierra-Torres CH, Delgado-Noguera M. Low birth weight: exploring of some risk factors at the San José teaching hospital in Popayán, Colombia. Rev Colomb Obstet Ginecol. 2009;60(2):124–34.
Cardona-Arias Jaiberth Antonio, Herrera-Posada Daniela, Valencia-Arredondo Marleny. Prevalencia de resultado positivo de la citología para vaginosis bacteriana, candidiasis y tricomoniasis en una Empresa Social del Estado de Medellín (Colombia), 2010-2012. Rev Colomb Obstet Ginecol [Internet]. 2014;65(3):206–14. [cited 2023 Jan 17]. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0034-74342014000300002&lng=en. https://doi.org/10.18597/rcog.47.
Rendón LF, Miyerlandi Torres GL. Caracterización de la población afiliada al Régimen Subsidiado en Cali. Colomb Med. 1996;27:146–9.
Piñeros M, Sánchez R, Perry F, García OA, Ocampo R, Cendales R. Demoras en el diagnóstico y tratamiento de mujeres con cáncer de mama en Bogotá, Colombia. Salud Publica Mex. 2011;53(6):478–85.
Varela SAGCAGAR. Niveles de actividad física de la población Colombiana: Análisis por sexo y condición socioeconómica. Inst Nac Salud. 2013;1:105–12.
Instituto Nacional de Salud (INS). Control en Vigilancia Publica. Instituto Nacional de Salud. 2015;12(22):1–10.
Instituto Nacional de Salud (INS), Paola S, Mora C. Accidente ofídico. Instituto Nacional de Salud. 2019;05(4):2–18.
Instituto Nacional de Salud (INS). Accidente ofídico. Instituto Nacional de Salud. 2020;04(01):2–20.
Instituto Nacional de Salud (INS). Accidente ofídico. Instituto Nacional de Salud. 2018;05(4):2–33.
Instituto Nacional de Salud (INS). Accidente ofídico. Instituto Nacional de Salud. 2021;01(01):1–2.
Instituto Nacional de Salud. Agresiones y contactos con Animales Potencialmente Transmisores de Rabia y Rabia Humana. Inst Nac Salud. 2019;05(31):1–4. Available from: http://www.ins.gov.co/buscador-eventos/Informesdeevento/VIGILANCIAINTEGRADADELARABIAPEXIII2018.pdf.
Instituto Nacional de Salud (INS). Aumento inusitado de casos de malaria en Guainía, Colombia 2015 -2017. Instituto Nacional de Salud. 2017;01:1–14.
Instituto Nacional de Salud (INS). Bajo peso al nacer a termino. Inst Nac Salud. 2020;3:0–1.
Instituto Nacional de Salud (INS). Bajo Peso Al Nacer a Término. Instituto Nacional de Salud. 2019;04(05):2–9 PRO-R02.00:13. Available from: http://www.dadiscartagena.gov.co/images/docs/saludpublica/vigilancia/protocolos/p2018/pro_bajo_peso_nacer_termino_2018.pdf.
Instituto Nacional de Salud (INS). Bajo Peso Al Nacer a Término. Instituto Nacional de Salud. 2021;01(01):1-2 PRO-R02.00:13. Available from: http://www.dadiscartagena.govco/images/docs/saludpublica/vigilancia/protocolos/p2018/pro_bajo_peso_nacer_termino_2018.pdf.
(INS) IN de S. Bajo Peso Al Nacer a Término. Inst Nac Salud. 2018; PRO-R02.00:13. Available from: http://www.dadiscartagena.gov.co/images/docs/saludpublica/vigilancia/protocolos/p2018/pro_bajo_peso_nacer_termino_2018.pdf.
Campo Carey AR, Benavides Ocampo M, Martínez Durán ME, Caro Núñez OA, Gómez Amaya JA, Nieto Sánchez DL, et al. Brote de chikungunya en el municipio de Mahates, Bolivar, 2014. IQEN Inf Quinc Epidemiol Nac. 2014;19(21):342–67.
Campo A, Martínez M, Benavides M, Cuellar N. Brote de chikungunya en el municipio de San Juan Nepomuceno, Bolivar, Colombia 2014. Inf Quinc Epidemiol Nac. 2015;20(1):2–20 Available from: https://www.ins.gov.co/buscador-eventos/IQEN/IQENvol202015num1.pdf.
Martinez M, Tolosa N, Salas P, Benitez J, Santos M, Malo DC, et al. Brote de enfermedad por virus Zika en el municipio de Turbaco. Inf Quinc Epidemiol Nac. 2016;21(17):391-403. Available from: https://www.ins.gov.co/buscador-eventos/IQEN/IQENvol212016num17.pdf.
Instituto Nacional de Salud (INS). Brote de evento de etiología desconocida en el municipio de El Carmen de Bolívar, Bolívar, 2014. Inst Nac Salud. 2014;2(441):1–40.
Instituto Nacional de Salud (INS). Brote de leishmaniasis visceral en área periurbana en el municipio de Neiva, Huila. Situación de en ero a julio de 2017. Instituto Nacional de Salud. 2012;05(1):1–12.
Bonilla M, Campo A, Martínez M. Brote de malaria en el municipio de Quibdó Departamento del Chocó, Noviembre de 2015. Inf Quinc Epidemiológico Nac. 2016;21:17.
Instituto Nacional de Salud (INS). Brote de malaria en los municipios de Guapi y Timbiquí, Cauca, Colombia, 2014 Antecedentes. Inst Nac Salud. 2014;2013:634 Available from: https://hsgm.saglik.gov.tr/depo/birimler/saglikli-beslenme-hareketli-hayat-db/Yayinlar/kitaplar/diger-kitaplar/TBSA-Beslenme-Yayini.pdf.
Instituto Nacional de Salud (INS). Situación del cáncer en la población pediátrica 2016. Instituto Nacional de Salud. 2016;01(01):15–67.
Instituto Nacional de Salud. Cáncer En Menores De 18 Años. Protoc Vigil Salud Publica. 2017;1:19 Available from: https://www.ins.gov.co/buscador-eventos/Lineamientos/PROCáncerenmenoresde18años-.pdf.
Instituto Nacional de Salud (INS). Cáncer en menores de 18 años Colombia, 2019. Instituto Nacional de Salud. 2019;1(3):1-2
Instituto Nacional de Salud (INS). Caso confirmado de Chagas agudo, Rio Iro, Chocó. Instituto Nacional de Salud. 2018;04(1):1–6.
Instituto Nacional de Salud (INS). Chagas (Agudo). Instituto Nacional de Salud. 2021;3(10):8–9.
Instituto Nacional de Salud (INS). Chikungunya. Instituto Nacional de Salud. 2018;2(31):2-16
Instituto Nacional de Salud (INS). Chikungunya. Instituto Nacional de Salud. 2020;5(31):2-24
Instituto Nacional de Salud (INS). Comportamiento de Infección Respiratoria Aguda Semanas epidemiológicas 1 a 52 de 2012. Instituto Nacional de Salud. 2012;5(1):1-26
Instituto Nacional de Salud (INS). Comportamiento Variables de interés. Instituto Nacional de Salud. 2019;01(3):1-3
Instituto Nacional de Salud (INS). Defectos congénitos. Instituto Nacional de Salud. 2020;2(3):0–1.
Instituto Nacional de Salud (INS). Defectos congénitos. Instituto Nacional de Salud. 2018;5(31):2–19.
Instituto Nacional de Salud (INS). Defectos congénitos. Instituto Nacional de Salud. 2021;7(1):1–3.
Instituto Nacional de Salud (INS). Dengue. Instituto Nacional de Salud. 2018;12(2):2–21.
Instituto Nacional de Salud (INS). Dengue. Instituto Nacional de Salud. 2019;12(2):1–24.
Instituto Nacional de Salud (INS). Dengue. Instituto Nacional de Salud. 2021;2(1):19–22.
Instituto Nacional de Salud (INS). Dengue y COVID-19. Instituto Nacional de Salud. 2020;8(1):1–3.
Instituto Nacional de Salud (INS). Desnutrición aguda moderada y severa en menores de cinco años. Instituto Nacional de Salud. 2020;1(4):18–9.
Instituto Nacional de Salud (INS). Desnutrición aguda moderada y severa en menores de cinco años. Instituto Nacional de Salud. 2019;12(1):2–15.
Instituto Nacional de Salud (INS). Desnutrición aguda, moderada y severa en menores de cinco años. Instituto Nacional de Salud. 2020;2(5):5–7.
Zuluaga GPA, Alvarez-Lerma F. Determinantes económicos, sociales y de salud que inciden en la lactancia materna exclusiva en Colombia para el año 2010. Vol. 3. Bogotá: Universidad del Rosario; 2015.
Instituto Nacional de Salud (INS). Difteria. Instituto Nacional de Salud. 2018;12(2):2–12
Instituto Nacional de Salud (INS). Difteria. Instituto Nacional de Salud. 2020;12(2):2–13.
Instituto Nacional de Salud (INS). Difteria. Instituto Nacional de Salud. 2019;12(2):2–10.
Instituto Nacional de Salud (INS). Encefalitis equinas Colombia, 2018. Instituto Nacional de Salud. 2018;12(2):2–11.
Instituto Nacional de Salud (INS). Endometritis puerperal. Instituto Nacional de Salud. 2020;02(1):1–3.
Instituto Nacional de Salud (INS). Enfermedad de Chagas. Inst Nac Salud. 2019;14(1):9–13.
Instituto Nacional de Salud (INS). Enfermedad por virus Zika. Inst Nac Salud. 2021;84(2):17–9.
Instituto Nacional de Salud (INS). Enfermedad por virus Zika. Inst Nac Salud. 2018;84(2).
Organización Panamericana de la Salud(OPS), Instituto Nacional de Salud. Enfermedad por virus Zika. Instituto Nacional de Salud. 2019;01(01):1–4.
Instituto Nacional de Salud (INS). Enfermedad por virus Zika (OPS/OMS). Instituto Nacional de Salud. 2019;12(01):1–18
Instituto Nacional de Salud (INS). Enfermedades huérfanas - raras. Instituto Nacional de Salud. 2020;21(02)1–3.
Instituto Nacional de Salud. Enfermedades huérfanas y raras. Instituto Nacional de Salud. 2021;21(01):1–3.
Instituto Nacional de Salud (INS). Enfermedades huérfanas y raras. Instituto Nacional de Salud. 2021;1(1):1–5.
Instituto Nacional de Salud (INS). Evento adverso grave relacionado a inmunizaciones. Instituto Nacional de Salud. 2020;04(31):0–1.
Instituto Nacional de Salud (INS). Evento adverso posterior a la vacunación - grave. Instituto Nacional de Salud. 2021;4(3):3–6.
Instituto Nacional de Salud (INS). Eventos graves supuestamente atribuidos a la vacunación o inmunización. Instituto Nacional de Salud. 2018;8(1):1–3.
Instituto Nacional de Salud (INS). Eventos graves supuestamente atribuidos a la vacunación o inmunización, Colombia. Instituto Nacional de Salud. 2020;12(1):1–3.
Instituto Nacional de Salud (INS). Exposición a Flúor. Instituto Nacional de Salud. 2018;12(1):2–17.
Instituto Nacional de Salud (INS). Fiebre amarilla. Instituto Nacional de Salud. 2021;8(1):1–3.
Instituto Nacional de Salud (INS). Fiebre tifoidea y embarazo. Inst Nac Salud. 2021;3(2):112–8.
Instituto Nacional de Salud (INS). Hepatitis A. Instituto Nacional de Salud. 2018;04(05):1–13.
Instituto Nacional de Salud (INS). Hepatitis B, hepatitis C y B delta. Inst Nac Salud. 2018;99(8):475.
Instituto Nacional de Salud (INS). Infección Por Virus Del Zika En El Embarazo. Inst Nac Salud. 2017;15:35 Available from: https://uvadoc.uva.es/bitstream/handle/10324/24455/TFG-H886.pdf;jsessionid=8E0A6FD6E5C860F094BB8243AD8758D0?sequence=1.
Instituto Nacional de Salud (INS). Infección Respiratoria Aguda. Instituto Nacional de Salud. 2016;2(1):1-3 Available from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/infeccion-respiratoria-aguda-ira-2016-.pdf.
Rivera S. Infecciones Asociadas a Dispositivos Colombia 2019. Instituto Nacional de Salud. 2019;12(1):2-17. Available from: https://www.ins.gov.co/buscadoreventos/Informesdeevento/INFECCIONESASOCIADASADISPOSITIVOS_2019.pdf#search=INFECCIONESASOCIADASADISPOSITIVOSENUCI.
Instituto Nacional de Salud (INS). Infecciones asociadas a procedimientos médico – quirúrgicos. Bol Epidemiol Sem. 2019;25:32 Available from: https://www.ncbi.nlm.nih.gov/books/NBK536395/.
Instituto Nacional de Salud (INS). Información receptores trasplantados de riñón con donante cadavérico (DC), Colombia 2016. Instituto Nacional de Salud. 2017;1(12):1–14.
Instituto Nacional de Salud (INS). Informe anual red de donación y transplantes de Colombia, 2019. Instituto Nacional de Salud. 2019;01(09):2–76 Available from:https://www.ins.gov.co/Direcciones/RedesSaludPublica/DonacionOrganosYTejidos/Estadisticas/infografia_red_nacional_de_donacion_y_trasplantes_2019.pdf.
Instituto Nacional De Salud., Dirección Redes En Salud Pública., Subdirección Red Nacional De Trasplantes Y Bancos De Sangre., Coordinación Nacional Red Donación Y Trasplantes. Informe anual red de donación y trasplantes. Instituto Nacional de Salud. 2018;01(01):4–76 Available from: https://www.ins.gov.co/Direcciones/RedesSaludPublica/DonacionOrganosYTejidos/Estadisticas/Informe-Anual-Red-Donacion-Trasplantes-2018.pdf.
Instituto Nacional de Salud (INS). Informe anual Red de Donación y Trasplantes Colombia, 2008. Instituto Nacional de Salud. 2009;1(3):1–15. Available from: https://www.ins.gov.co/Direcciones/RedesSaludPublica/DonacionOrganosYTejidos/Estadisticas/INFCOORDNALMINPROTORGANOS2008.pdf.
Instituto Nacional de Salud (INS). Informe de Evento Desnutrición Aguda Moderada y Severa En Menores De Cinco Años. Inf del Evento. 2018;13:1–5 Available from: https://www.ins.gov.co/buscadoreventos/Informesdeevento/DESNUTRICIÓNAGUDAENMENORESCINCOAÑOSSEMESTREI2018.pdf.
Instituto Nacional de salud (INS). Informe De Evento VIH/SIDA, Colombia, Año 2018. Instituto Nacional de Salud. 2018;16:1–5.
Espitia NCC. Informe del comportamiento de VIH-SIDA en Colombia, 2015. Instituto Nacional de Salud. 2015;1(2):1–18.
Espitia NCC. Informe del comportamiento de VIH-SIDA, Colombia periodo epidemiológico del año 2016. Instituto Nacional de salud. 2019;3(1):2–16.
Instituto Nacional de Salud (INS). Informe ejecutivo. Red de donación y trasplantes de Colombia, 2018. Instituto Nacional de Salud. 2019;8(1):1–79.
Botero DS. Informe final del evento leptospirosis, Colombia, 2015. Inst Nac Salud. 2015;3:103–11.
Instituto Nacional de Salud (INS). Intoxicaciones. Instituto Nacional de Salud. 2018;12(1):1–17.
Instituto Nacional de Salud. Intoxicaciones por sustancias químicas. Instituto Nacional de Salud. 2018;01(01):51–104 Available from: http://www.vertic.org/media/assets/nim_docs/InternationalImplementationAssistanceProgram(IAP)pdfs-CW/Chemicalproducts/Chemicalproducts-Spanish.pdf.
Instituto Nacional de Salud (INS). Leishmaniasis Cutánea, Mucosa Y Visceral, Colombia 2018. Inst Nac Salud. 2019;05(31):28.
Instituto Nacional de Salud (INS). Leishmaniasis mucosa. Instituto Nacional de Salud. 2021;1(8):1–2.
Aranda-Torrelio E. Leishmaniasis visceral. Inst Nac Salud. 2021;53(5):246–9.
Instituto Nacional de Salud (INS). Lepra. Instituto Nacional de Salud. 2018;12(1):2–17.
Instituto Nacional de Salud (INS). Lepra. Instituto Nacional de Salud. 2019;1(1):2–16.
Instituto Nacional de Salud (INS). Lepra. Instituto Nacional de Salud. 2021;01(01):0–1.
Instituto Nacional de Salud (INS). Leptospirosis. Instituto Nacional de Salud. 2021;8(2):1–2.
Instituto Nacional de Salud (INS). Leptospirosis. Instituto Nacional de Salud. 2018;5(03):1–13.
Instituto Nacional de Salud (INS). Leptospirosis. Instituto Nacional de Salud. 2020;1(12):1–12.
Instituto Nacional de Salud (INS). Leptospirosis, 2019. Instituto Nacional de Salud. 2019;01(04):1–12.
Instituto Nacional de Salud (INS). Leptospirosis Colombia, 2019. Instituto Nacional de Salud. 2019;12(1):1–10.
Moreno SL, Carreño PA. Lesiones de causa externa. Colombia 2011. Inst Nac Salud. 2012;13(1):11–64.
Instituto de Medicina Legal y Ciencias Forenses. Lesiones De Causa Externa. Colombia, 2006. Instituto Nacional de Salud. 2018;04(01):11–34 Available from: https://www.medicinalegal.gov.co/documents/20143/49496/Contenido.pdf.
Instituto Nacional de Salud (INS). Malaria. Instituto Nacional de Salud. 2021;1(1):1–3.
Instituto Nacional de Salud (INS). Malaria. Instituto Nacional de Salud. 2018;04(1):1–14.
Instituto Nacional de Salud (INS). Malaria Y COVID-19. Instituto Nacional de Salud. 2021;1(1):1–3.
Instituto Nacional de Salud (INS). Meningitis Bacteriana Y enfermedad meningocócica. Instituto Nacional de Salud. 2020;12(05):2–18.
Instituto Nacional de Salud. Ministerio de Salud de Colombia. Meningitis Bacteriana Y Enfermedad Meningocócica. Inst Nac Salud. 2019:1–17 Available from: http://www.dadiscartagena.gov.co/images/docs/saludpublica/vigilancia/protocolos/p2018/pro_meningitis_2018.pdf.
Instituto Nacional de Salud (INS). Morbilidad Materna Extrema 2018. Boletín Epidemiológico. 2018;12(1):1–22.
Instituto Nacional de Salud (INS). Morbilidad Materna Extrema 2019. Boletín Epidemiológico. 2019;12(1):1–20.
Instituto Nacional de Salud (INS). Mortalidad asociada a anomalías congénitas en Alcance y fuentes de esta conferencia. Instituto Nacional de Salud. 2010;02(01):1998–2010.
Jimenez MAC. Mortalidad asociada a anomalías congénitas en Alcance y fuentes de esta conferencia; 2010.
Instituto Nacional de Salud (INS). Mortalidad materna temprana. Instituto Nacional de Salud. 2020;01(01):0–3.
(INS) IN de S. Mortalidad materna. Inst Nac Salud. 2019;100(6):555–63.
Alvarez-Bravo A. Mortalidad materna. Gac Med Mex. 1970;100(6):555–63.
Instituto Nacional de Salud. Mortalidad Perinatal y Neonatal. Boletín Epidemiologico Semanal. 2019;30:1–4 Available from: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2019Boletínepidemiológicosemana12.pdf.
Equipo maternidad segura - subdirección prevención vigilancia y control en salud pública. Mortalidad Perinatal y Neonatal Tardía. Protocolo de Vigilancia en salud pública. 2018;01(05):1–19. Available from: https://www.ins.gov.co/buscador-eventos/Lineamientos/PROMortalidadperinatalneonatal.pdf.
Instituto Nacional de Salud (INS). Mortalidad materna temprana. Instituto Nacional de Salud. 2021;01(02):1–3.
Instituto Nacional de Salud (INS). Parálisis flácida aguda. Instituto Nacional de Salud. 2018;13(02):1–14.
Instituto Nacional de Salud (INS). Parálisis flácida Aguda. Instituto Nacional de Salud. 2020;12(1):1–15.
Instituto Nacional de Salud (INS). Parálisis flácida aguda. Instituto Nacional de Salud. 2021;3(2):1–18
Instituto Nacional de Salud (INS). Parálisis flácida aguda Colombia, 2019. Instituto Nacional de Salud. 2019;12(2):2–13.
Instituto Nacional de Salud (INS). Parotiditis. Instituto Nacional de Salud. 2018;01(08):2–17.
Instituto Nacional de Salud (INS). Parotiditis. Instituto Nacional de Salud. 2019;12(08):2–17.
Instituto Nacional de Salud (INS). Procedimientos estéticos. Instituto Nacional de Salud. 2021;01(01):1–4.
Instituto Nacional de Salud (INS). Protocolo Violencia de género e intrafamiliar. Instituto Nacional de Salud. 2019;02(05):1–13.
Instituto Nacional de Salud (INS). Red de Donación y Trasplantes. Instituto Nacional de Salud. 2020;12(01):1–15.
Instituto Nacional de Salud (INS). Sarampión y rubeola. Instituto Nacional de Salud. 2018;6(1):2–18.
Instituto Nacional de Salud (INS). Sarampión y rubeola Instituto Nacional de Salud. 2018;12(1):2–18.
Instituto Nacional de Salud (INS). Sarampión y rubeola. Instituto Nacional de Salud. 2020;12(1):2–13.
Instituto Nacional de Salud (INS). Sarampión y Rubéola. Bol Epidemiol Sem 49. 2019:1–31 Available from: https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2019_Boletin_epidemiologico_semana_49.pdf.
Instituto Nacional de Salud (INS). Sífilis congénita. Instituto Nacional de Salud. 2021;01(01):2–4.
Instituto Nacional de Salud (INS). Sífilis gestacional. Instituto Nacional de Salud. 2021;08(1):1–2.
Instituto Nacional de Salud (INS). Sífilis gestacional. Instituto Nacional de Salud. 2020;01(03):0–2.
Instituto Nacional de Salud. Sífilis Gestacional y Congénita 2018. Protocolo de Vigilancia en Salud Pública. 2018;02(01):1–17. Available from: https://www.ins.gov.co/buscador-eventos/Lineamientos/PROSifilis_.pdf.
Instituto Nacional de Salud (INS). Sífilis Gestacional y Congénita 2018. Protocolo de Vigilancia en Salud Pública. 2018;01(03):1–26. Available from: https://www.ins.gov.co/buscador-eventos/Lineamientos/PROSifilis_.pdf.
Instituto Nacional de Salud. Sífilis Gestacional y Congénita 2019. Protocolo de Vigilancia en Salud Pública. 2019;04(05):1–27. Available from: https://www.ins.gov.co/buscador-eventos/Lineamientos/PROSifilis_.pdf.
Instituto Nacional de Salud (INS). Síndrome de rubeola congénita. Instituto Nacional de Salud. 2019;12(1):2–11.
Instituto Nacional de Salud (INS). Síndrome de rubeola congénita. Instituto Nacional de Salud. 2020;12(1):1–11.
Instituto Nacional de Salud (INS). Síndrome de rubeola congénita. Instituto Nacional de Salud. 2018;12(1):2–11.
Instituto Nacional de Salud (INS). Tétanos accidental. Instituto Nacional de Salud. 2020;12(2):2–10.
(Instituto Nacional de Salud (INS). Tétanos accidental. Instituto Nacional de Salud. 2019;12(2):2–14.
Instituto Nacional de Salud (INS). Tétanos accidental. Instituto Nacional de Salud. 2021;01(01):12–14.
Instituto Nacional de Salud (INS). Tétanos accidental. Instituto Nacional de Salud. 2020;2020;6(2):2–10.
Instituto Nacional de Salud (INS). Tétanos Accidental Colombia 2018. Instituto Nacional de Salud. 2018;17(1):2–10.
(INS) IN de S. Tetanos Neonatal. Inst Nac Salud. 2017;3(4):473–85.
(INS) IN de S. Tetanos Neonatal. Inst Nac Salud. 2019;3(4):473–85.
(INS) IN de S. Tetanos Neonatal. Inst Nac Salud. 2020;3(4):473–85.
Instituto Nacional de Salud (INS). Tétanos Neonatal Colombia 2018. Instituto Nacional de Salud. 2018;12(1):2–9.
Instituto Nacional de Salud INS. Tos ferina. Instituto Nacional de Salud. 2021;8(1):1–3.
Instituto Nacional de Salud (INS). Tos ferina. Instituto Nacional de Salud. 2018;12(1):2–18.
Instituto Nacional de Salud (INS). Tos ferina Colombia, 2019. Instituto Nacional de Salud. 2019;12(2):2–18.
Instituto Nacional de Salud (INS). Tracoma. Instituto Nacional de Salud. 2019;12(1):2–10.
Instituto Nacional de Salud (INS). Tracoma. Inst Nac Salud. 2020;1:105–12.
Instituto Nacional de Salud (INS). Tracoma colombia 2017-2018. Inst Nac Salud. 2018;13 Available from: https://www.ins.gov.co/buscador-eventos/Informesdeevento/TRACOMA_2018.pdf.
Instituto Nacional de Salud (INS). Tuberculosis. Instituto Nacional de Salud. 2019;12(02):2–31.
Instituto Nacional de Salud (INS). Tuberculosis farmacorresistente. Instituto Nacional de Salud. 2019;02(01):0–1 Available from: https://www.ins.gov.co/buscador-eventos/Informesdeevento/TUBERCULOSISFARMACORRESISTENTEPEII2021.pdf.
Andrea L, Pinzón B. Tuberculosis Farmacorresistente Colombia, 2019. Instituto Nacional de Salud. 2018;05(04):1–33 Available from: https://www.ins.gov.co/buscador-eventos/Informesdeevento/TUBERCULOSISFARMACORRESISTENTE_2019.pdf.
Instituto Nacional de Salud (INS). Varicela. Instituto Nacional de Salud. 2019;12(01):2–16.
Instituto Nacional de Salud (INS). Varicela. Instituto Nacional de Salud. 2018;12(01):2–18.
Instituto Nacional de Salud. VIH, sida y muerte por SIDA. Colombia 2019. Inst Nac Salud. 2019;22:1-14 Available from: https://www.ins.gov.co/buscador-eventos/Informesdeevento/VIH-SIDA_2019.pdf.
R4V. Situación y respuesta del fenómeno migratorio en salud. Bogotá: R4V; 2021. p. 3–7.
R4V. Afiliaciones a la Salud de Refugiados y Migrantes Venezolanos – Antioquia. Bogotá: R4V; 2021.
Ministerio de Salud y Protección Social. Informe de resultados: Estudio de evaluación de los servicios de las EPS por parte de los usuarios, en el régimen contributivo y subsidiado. Ministerio de Salud y Protección Social. 2014;01(01):7–24.
Cuenta de Alto Costo. Artritis reumatoide, una enfermedad que afecta la productividad laboral | Cuenta de Alto Costo. Bogotá: Cuenta de Al to Costo; 2021. [cited 20 Nov 2021]. Available from: https://cuentadealtocosto.org/site/artritis/artritis-reumatoide-una-enfermedad-que-afecta-la-productividad-laboral/.
Costo C de alto. Día mundial contra el cáncer 2020. Bogotá: Cuenta de Alto Costo; 2021. [cited 20 Nov 2021]. Available from: https://cuentadealtocosto.org/site/cancer/dia-mundial-contra-el-cancer-2020/.
Agudelo Ibañez, D Mortalidad por desnutrición infantil en menores de 5 años y sus determinantes a nivel municipal en Colombia 1998 - 2016. [Internet]. [citado: 2023, enero]. 2019:1–128.
Torres Ibargüen, M Caracterización de la calidad del proceso de atención de pacientes con cáncer colorrectal atendidos en los años 2014 y 2015 en el Instituto Nacional de Cancerología E. S. E. [Internet]. [citado: 2023, enero]. 2020:1–149.
Atehortúa S, Palacio-Mejía L. Impacto del seguro subsidiado en el acceso y el uso de servicios de salud: el caso de Medellín, Colombia. Lect Econ. 2015;16(82):522–33.
Rodríguez AYR. Caracterización de la mortalidad en personas de 30 y más años por enfermedades cardio-cerebrovasculares y su relación con aspectos socio-económicos y de vinculación al sistema general de seguridad social en salud. Colombia (2005-2013). Rev Fac Med. 2017;26(4):219–27.
Almario-Barrera AJ, Villarreal-Neira C, Concha-Sánchez SC. Aspectos relacionados con el número de citas odontológicas a las que asisten las mujeres embarazadas en Santander. Rev Fac Med. 2017;65(1):73–9.
Pineda CA. Caracterización del trauma maxilofacial en el Hospital la Samaritana de Bogotá entre los años 2008 a 2013. Univ Nac Colomb. 2015;3(7):59–78.
Ruiz-Rodríguez M, Vera-Cala LM, López-Barbosa N. Seguro de salud y cobertura de vacunación en población infantil con y sin experiencia de desplazamiento forzado en Colombia. Rev Salud Publica. 2008;10(1):49–61.
Por T, Vez P, Centros EN, En O, Periodo EL. Supervivencia de los pacientes con cáncer escamocelular bucal, tratados por primera vez, en centros oncológicos en el periodo 2000 a 2011, Medellín- Colombia. Rev Fac Odontol Univ Antioquia. 2016;27:245–61.
Gómez-Suárez, M Comparación de dos modelos de asesoría en anticoncepción para mujeres VIH positivas desde una perspectiva de equidad en salud. Colombia 2015-2017. [Internet]. [citado: 2023, enero]. 2019:1–166.
Trabajo MSB. Factores asociados a la morbilidad materna extrema a nivel individual y entre las comunas y corregimientos de Medellín, 2013-2015. Occup Med (Chic Ill). 2017;53(4):130.
Romero Acosta, D Factores asociados a la desigualdad de la mortalidad infantil en las localidades de Bogotá, 2013. [Internet]. [citado: 2023, enero]. 2017:1–128.
Vergara Escobar, O Intervención de enfermería para el automanejo en adultos con cáncer colorrectal en tratamiento quirúrgico. [Internet]. 2020. [citado: 2023, enero] doscientas once.
Calderón Ramirez, V Desigualdad en carga de enfermedad por Infección respiratoria aguda (IRA) y enfermedad diarreica aguda (EDA) menores de 5 años, Colombia 2010. [Internet]. 2016. [citado: 2023, enero]. Universidad Nacional de Colombia Sede Bogotá Facultad de Medicina Departamento de Salud Pública.
Córdoba González, L Determinantes sociales y mortalidad en menores de 5 años en el departamento del Chocó. [Internet]. [citado: 2023, enero]. Universidad Nacional de Colombia Sede Bogotá Facultad de Medicina Departamento de Pediatría. 2016:1–106.
Castañeda Rodríguez, C Asociación de la carga de enfermedad por Leucemia pediátrica aguda y las desigualdades en salud por régimen de afiliación y departamento de procedencia en Colombia durante el periodo 2011-2012. [Internet]. [citado: 2023, enero]. Universidad Nacional de Colombia Sede Bogotá Facultad de Medicina Instituto de Salud Pública. 2017.
Forero, L Escala de vulnerabilidad de muerte por infección respiratoria aguda, en menores de un año, en Bogotá según determinantes sociales de la salud. [Internet]. [citado: 2023, enero] Universidad Nacional de Colombia Sede Bogotá Facultad deMedicina Instituto de Investigaciones Clínicas. 2017:1–69.
Soto Mora, B Análisis cualitativo de las muertes maternas en Buenaventura 2010 - 2012 con enfoque de determinantes sociales y equidad. [Internet]. [citado: 2023, enero] Universidad Nacional de Colombia Sede Bogotá Facultad de Medicina Departamento deSalud Pública. 2016:1–188.
Peñafiel Ruiz, J Caracterización de los pacientes con diagnóstico de cáncer de mama, en el Hospital de La Samaritana, Bogotá 2010 - 2018. [Internet]. [citado: 2023, enero]. 2020:1–66.
Barragan MM. Equidad en salud: estudio de caso en el distrito capital de Bogotá. Univ Nac Colomb. 2006;3:313–23.
Enrique I, Puerta P, Enrique I, Cortés P, Caballero AD. Investigaciones originales research articles. Res Artic. 2018;8(1):60–74.
Becerra Muñoz, M Barreras de acceso al programa ampliado de inmunizaciones, de la población infantil asistente a las casas vecinales de Tibabitá y horizontes de la localidad de Usaquén, Bogotá D.C., año 2008. [Internet]. [citado: 2023, enero] Universidad Nacional de Colombia Sede Bogotá Facultad de Medicina. 2011:1–188.
Acevedo Jaimes, J Caracterización sociodemográfica de la salud materna en el Vichada, 2011-2015: una mirada desde la morbimortalidad. [Internet]. [citado: 2023, enero]. 2019;110.
Garcia CS. Asociación entre condiciones sociodemográficas y epilepsia no controlada en poblaciones con acceso limitado a servicios de neurología. Univ del Rosario. 2019;8(5):55.
Garcia-Subirats I, Vargas I, Mogollón-Pérez AS, De Paepe P, da Silva MRF, Unger JP, et al. Barriers in access to healthcare in countries with different health systems. A cross-sectional study in municipalities of Central Colombia and North-Eastern Brazil. Soc Sci Med. 2014;106:204–13. https://doi.org/10.1016/j.socscimed.2014.01.054.
Bouwmans M, Gaona MA, Chenault MN, Zuluaga C, Pinzon Rondon AM. Prevalence of intestinal parasitic infections in preschool-children from vulnerable neighborhoods in Bogotá. Rev Univ Ind Santander Salud. 2016;48(2):178–87.
Palacios MS. Caracterización y perfiles de pacientes con morbilidad materna extrema, unidad de cuidados intensivos, hospital la samaritana, 2008-2014. Univ del Rosario. 2017:2008–14.
Agudelo YRO. Salud sexual y reproductiva: aspectos de análisis para el departamento de Casanare. Appl Microbiol Biotechnol. 2016;85(1):2071–9.
Mora PED. Determinantes socio-económicas de la desnutrición global infantil en la localidad de ciudad Bolívar (Bogotá, Colombia) en el año 2011. Vol. 1. Bogotá: Universidad del Rosario; 2019.
Saboyá ELS, Giraldo MMLRFG. Determinantes sociales y su asociación con la no toma de citología cérvico vaginal en la población rural de Colombia. Univ del Rosario 2020;4(1):1–9. Available from: https://pesquisa.bvsalud.org/portal/resource/en/mdl-20203177951%0Ahttp://dx.doi.org/10.1038/s41562-020-0887-9%0Ahttp://dx.doi.org/10.1038/s41562-020-0884-z%0Ahttps://doi.org/10.1080/13669877.2020.1758193%0Ahttp://sersc.org/journals/index.php/IJAST/article
Rincón JMS. Factores asociados de la pobreza multidimensional con la toma de citología en Colombia. Univ del Rosario. 2020;9:6 Available from: https://www.slideshare.net/maryamkazemi3/stability-of-colloids%0Ahttps://barnard.edu/sites/default/files/inline/student_user_guide_for_spss.pdf%0Ahttp://www.ibm.com/support%0Ahttp://www.spss.com/sites/dm-book/legacy/ProgDataMgmt_SPSS17.pdf%0Ahttps://www.n.
Díaz BLM, Chávez GBM. Complicaciones maternas en adolescentes y adultas afiliadas al régimen subsidiado, 2012. Rev Fac Nac Salud Pública. 2015;33(2):206–14.
Barrientos MS. Factores asociados a la morbilidad materna extrema a nivel individual y entre las comunas y corregimientos de Medellín, 2013-2015. Occup Med (Chic Ill). 2017;53(4):130.
Cifuentes MAP. Características sociales, demográficas y de morbilidad de los pacientes atendidos por enfermedades crónicas no transmisibles en la E.S.E Hospital Pedro Claver Aguirre del municipio de Toledo-Antioquia 2015-2019. [Internet]. [citado: 2023, enero]. Universidad de Antioquia; 2021:1–95.
Hernández Ruiz, S Caracterización de las gestantes con zika virus del municipio de Villavicencio, 2016 : abordaje sociodemográfico y perinatal incluyendo elementos de aproximación a los determinantes sociales de la salud. [Internet]. [citado: 2023, enero]. Uniandes; 2017:1–27.
Arenas Duque A, Lucumí DI. Caracterización del accidente cerebrovascular en Colombia. Ser Doc Trab. 2019;78116(63):1–30.
Murcia Urrego, L Determinantes sociales de la morbimortalidad infantil por Infección Respiratoria Aguda en Bogotá 2015-2016. [Internet]. [citado: 2023, enero]. Uniandes; 2019:1–44.
García, S. Análisis descriptivo de la morbimortalidad por leucemia linfoide aguda en menores de 20 años según departamento y régimen de aseguramiento en Colombia 2010-2015. [Internet]. 2020. [citado: 2023, enero] Disponible en: http://hdl.handle.net/20.500.12495/2864.
Núñez MAZ. Desigualdades del aseguramiento en salud de la atención prenatal en Colombia Insurance health disparities in antenatal care in Colombia Autor: Univ del Bosque; 2018. p. 22.
Echavarría N. Acceso a los servicios curativos de salud oral en escolares de la localidad de Fontibón de Bogotá D.C., 2009. [Internet]. [citado: 2023, enero]. Disponible en: 2011:1-109. http://hdl.handle.net/10554/1478.
Arrivillaga Quintero M, Zapata Ossa H, Tovar Cuevas LM, Correa Sánchez DE, Varela Arévalo MT, Hoyos Hernández PA. Infecciones de transmisión sexual en Colombia: análisis basado en la encuesta nacional de salud: año 2007. Vol. 10. Bogotá: Gerencia y Políticas de Salud; 2011.
Vergara ÓJ. Intervención de enfermería para el automanejo de adultos con cáncer colorrectal en tratamiento quirúrgico; 2020. p. 211. Available from: https://repositorio.unal.edu.co/bitstream/handle/unal/78593/TesisFinalOscarVergara5Noviembre-2020.pdf?sequence=1&isAllowed=y
Posada López A, Palacio MA, Salas ZC, Álvarez ME, Grisales H. Supervivencia de los pacientes con cáncer escamocelular bucal, tratados por primera vez, en centros oncológicos en el periodo 2000 a 2011, Medellín-Colombia. Rev Fac Odontol. 2016;27(2):245–61.
Instituto Nacional de Salud (INS). Red de Donación y Trasplantes. Informe ejecutivo 2021. Instituto Nacional de Salud. 2021;05(1):1–15.
Instituto Nacional De Salud. Informe anual red de donación y trasplantes. Instituto Nacional de Salud. 2018;01(01):4–76 Available from: https://www.ins.gov.co/Direcciones/RedesSaludPublica/DonacionOrganosYTejidos/Estadisticas/Informe-Anual-Red-Donacion-Trasplantes-2018.pdf.
Casallas JL, Novoa Garzón YTM. Evaluacion del tiempo libre de cisis de asma en niños de 4 a 11 años con relacion a factores sociales. Univ del Rosario. 2019;9(1):148–62. https://doi.org/10.1155/2015/420723%0A. Available from: http://jurnal.globalhealthsciencegroup.com/index.php/JPPP/article/download/83/65%0Ahttp://www.embase.com/search/results?subaction=viewrecord&from=export&id=L603546864%5Cnhttp://link.springer.com/10.1007/978-3-319-76.
Mora PED. Determinantes socio-económicas de la desnutrición global infantil en la localidad de ciudad bolívar (Bogotá, Colombia) en el año 2011. Univ del Rosario. 2012;13:15–38.
Instituto Nacional de Salud (INS). Leptospirosis. Instituto Nacional de Salud. 2015;(01):1–18.
Instituto Nacional de Salud (INS). Tracoma. Instituto Nacional de Salud. 2020;01(01):1–2.
Instituto Nacional de salud (INS). Síndrome de rubeola congénita. 2018;
Instituto Nacional de Salud (INS). Fiebre amarilla. Inst Nac Salud. 2018;11(216):45.
Instituto Nacional de Salud (INS). Encefalitis equinas colombiana, 2020. Instituto Nacional de Salud. 2020;01(01):1–4.
Instituto Nacional de Salud. Infección Respiratoria Aguda. Hnrg; 2016. p. 2. Available from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/infeccion-respiratoria-aguda-ira-2016-.pdf
Instituto Nacional de Salud (INS). Enfermedad de Chagas. Prensa Med Mex. 1949;14(1):9–13.
Instituto Nacional de Salud (INS). Sífilis congénita. Instituto Nacional de Salud. 2020;2(3):0–1.
Instituto Nacional de Salud (INS). Lesiones de causa externa. Instituto Nacional de Salud. 2021;01(01):12–4.
Instituto de Medicina Legal y Ciencias Forenses. Lesiones De Causa Externa. Colombia, 2006. 2018;01(03):11–34. Available from: https://www.medicinalegal.gov.co/documents/20143/49496/Contenido.pdf.
Instituto Nacional de Salud (INS). Intoxicaciones por sustancias químicas. Instituto Nacional de Salud. 2019;02(01):51–104 Available from: http://www.vertic.org/media/assets/nim_docs/InternationalImplementationAssistanceProgram(IAP)pdfs-CW/Chemicalproducts/Chemicalproducts-Spanish.pdf.
Moreno SL, Carreño PA. Lesiones de causa externa. Colombia, 2011. Forensis. 2012;13(1):11–64.
López JEB. Características de los cuidadores asociadas a la consulta odontológica de niños colombianos menores de 5 años. Univ del Rosario. 2019;1:105–12.
Española OMC. La pobreza es uno de los factores claves en violencia doméstica, según psiquiatras | Médicos y Pacientes [Internet]. Organización Médica Colegial Española. 2021. [cited 2021 Dec 30]. Available from: http://www.medicosypacientes.com/articulo/la-pobreza-es-uno-de-los-factores-claves-en-violencia-doméstica-según-psiquiatras.
Emadi M, Delavari S, Bayati M. Global socioeconomic inequality in the burden of communicable and non-communicable diseases and injuries: an analysis on global burden of disease study 2019. BMC Public Health [Internet]. 2021;21(1):1–13. [cited 2021 Dec 6]. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-11793-7.
Sommer I, Griebler U, Mahlknecht P, Thaler K, Bouskill K, Gartlehner G, et al. Socioeconomic inequalities in non-communicable diseases and their risk factors: An overview of systematic reviews. BMC Public Health [Internet]. 2015;15(1):1–12. [cited 2021 Dec 6]. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-015-2227-y.
Acknowledgements
Not applicable.
Funding
This study is funded by the Ministerio de Hacienda y Crédito Público of Colombia and the Instituto de Evaluación Tecnológica en Salud, through inter-administrative agreement No. 7008-2021.
Author information
Authors and Affiliations
Contributions
LMM and KEO defined the scope of the research subject and developed the search strategy. LMM and KEO undertook the search, reviewed the literature, and summarized the search findings. LMM and KEO drafted the manuscript. LMM, KEO, OE, and LM provided substantial input in the design stages of the review, critically reviewed the manuscript, and helped shape the final version of the manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors agree with the content of this manuscript.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Diagnostic codes. Table 2. Search strategy. Table 3. References included.
Additional file 2: Table 1.
Noncommunicable diseases. Table 2. Communicable diseases. Table 3. Obstetric and maternal conditions. Table 4. Frequent conditions in early childhood. Table 5. Other diseases. Illustration 1. Forest plot of cumulative incidence of noncommunicable diseases in the SS, 2016-2021. Illustration 2. Forest Plot of cumulative incidence of communicable disease. Illustration 3. Forest plot of cumulative incidence of obstetric and maternal conditions in the SS, 2018-2021. Illustration 4. Forest plot of cumulative incidence of common conditions in early childhood in the SS, 2009-2021. Illustration 5. Forest plot of cumulative incidence of other diseases in SS, 2015-2021. Illustration 6. Forest plot of cumulative incidence of non-communicable diseases in the CS, 2016-2021. Illustration 7. Forest plot of cumulative incidence of CS communicable diseases, 2012-2021. Illustration 8. Forest plot of cumulative incidence of obstetric and maternal conditions in CS, 2018-2021. Illustration 9. Forest plot of cumulative incidence of common conditions in early childhood in the CS, 2009-2021. Illustration 10. Forest plot of cumulative incidence of others in CS, 2015-2021.
Additional file 3: Table 1.
Distribution of cases by regimen in morbid cohorts of non-communicable diseases between 2004 and 2020. Table 2. Description of studies with information on communicable diseases from the SS, 2018-2021. Table 3. Distribution of cases between regimens. Health services. 2009-2021. Table 4. Use of health services. Table 5. Distribution of cases by regimen in morbid cohorts in health services. 2009-2019.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mora-Moreo, L., Estrada-Orozco, K., Espinosa, O. et al. Characterization of the population affiliated to the subsidized health insurance scheme in Colombia: a systematic review and meta-analysis. Int J Equity Health 22, 28 (2023). https://doi.org/10.1186/s12939-022-01818-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-022-01818-x