
Abstract
Background
Myocardial infarction (MI) elicits an intense acute inflammatory response that is essential for cardiac repair. However, an excessive inflammatory response also favors myocardial apoptosis, cardiac remodeling, and cardiovascular mortality. Omega-3 polyunsaturated fatty acids (ω-3) bear anti-inflammatory effects, which may mitigate the inflammatory response during MI. This study investigated whether ω-3 intake is associated with attenuation of the MI-related inflammatory response and cardiac remodeling.
Methods
ST-elevation MI (STEMI) patients (n = 421) underwent clinical, biochemical, nutritional, 3D echocardiogram, Cardiac Magnetic Resonance imaging (CMRi) at 30 days and 3D echocardiogram imaging at six months after the MI. Blood tests were performed at day one (D1) and day five (D5) of hospitalization. Changes in inflammatory markers (ΔD5-D1) were calculated. A validated food frequency questionnaire estimated the nutritional consumption and ω-3 intake in the last 3 months before admission.
Results
The intake of ω-3 below the median (< 1.7 g/day) was associated with a short-term increase in hs-C-reactive protein [OR:1.96(1.24–3.10); p = 0.004], Interleukin-2 [OR:2.46(1.20–5.04); p = 0.014], brain-type natriuretic peptide [OR:2.66(1.30–5.44); p = 0.007], left-ventricle end-diastolic volume [OR:5.12(1.11–23.52)]; p = 0.036] and decreases in left-ventricle ejection fraction [OR:2.86(1.47–6.88); p = 0.017] after adjustment for covariates. No differences were observed in the extension of infarcted mass obtained by CMRi.
Conclusion
These findings suggest that a reduced daily intake of ω-3 may intensify outcome-determining mechanisms after STEMI, such as acute inflammatory response and late left ventricular remodeling.
Trial registration
Clinical Trial Registry number and website: NCT02062554.
Similar content being viewed by others

Introduction
Myocardial infarction (MI) elicits an intense acute inflammatory response due to mechanical stress and ischemia-reperfusion injury [1]. The generation of pro-inflammatory cytokines via activation of both Nuclear Factor κB (NF-κB) and Activator Protein-1 (AP-1) transcription factors represents a central step in the triggering of this response [2,3,4]. Although this phenomenon is involved for cardiac repair, excessive inflammation favors myocardial apoptosis and cardiac remodeling, thus leading to increased cardiovascular mortality [5,6,7].
Omega-3 (ω-3) are polyunsaturated fatty acids whose interactions with human physiology have been reported, particularly for α-linolenic acid (ALA), eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). EPA and DHA components bear anti-inflammatory effects through two complementary actions: (i) reducing the content of arachidonic acid products and (ii) downregulating the expression of pro-inflammatory cytokines via NF-κB and AP-1 inhibition [8,9,10,11,12]. The clinical impact of this set of mechanisms has been documented in several conditions involving the acute phase response. These included sepsis and chronic inflammatory conditions such as rheumatoid arthritis, multiple sclerosis, type 1 diabetes mellitus, end-stage renal disease, and Alzheimer disease [13,14,15,16,17,18,19]. Considering the abovementioned premises, we hypothesized that MI-related inflammatory response would be attenuated in individuals who had enhanced ω-3 intake prior the onset of the coronary event. This assumption is consistent with a previous randomized controlled trial that showed a decrease in cardiovascular death with dietary supplementation with ω-3 [20]. However, it is unclear whether the acute inflammatory response and cardiac remodeling may be further subsided by ω-3 intake that is already established at the time of the inciting event. Therefore, aiming to investigate whether ω-3 intake is associated with attenuation of the MI-related inflammatory response and cardiac remodeling, we analyzed a prospective cohort database originally designed to include the investigation of nutritional characteristics from 3 months prior to 3 months after ST-elevation MI (STEMI) manifestation.
Subjects and methods
Study design and participants
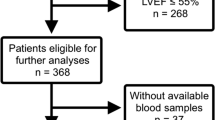
Participants from the Brasília Heart Study (BHS) database were used for this analysis (n = 421). BHS is a an ongoing prospective observational cohort composed of STEMI patients admitted to Hospital de Base do Distrito Federal (Brasília, Brazil) since 2006 [21]. Briefly, BHS inclusion criteria were: (i) < 24 h after onset of MI symptoms, (ii) ST-segment elevation of at least 1-mm (frontal plane) or 2-mm (horizontal plane) in 2 contiguous leads and (iii) increased myocardial necrosis markers above reference limit of creatine kinase-MB (CK-MB) (25 U/L) and troponin I (0.04 ng/mL) followed by a decline of both markers. Participants with new or presumed left bundle branch block, development of pathological Q waves without ST-elevation recording or exclusively with imaging evidence of MI were excluded. Diagram flow is showed in Fig. 1.

Diagram flow of study design
Patients enrolled into the study underwent therapies based on current guidelines for treatment of acute coronary disease, as indicated by Table 1 data [22]. Attending physicians, who were blind to the study evaluations, made all therapeutic decisions.
Clinical evaluation
Participants underwent a structured detailed clinical questionnaire, anthropometric measurements, blood collection for biochemical analysis, nutritional, and imagining evaluation. Ex-smoking status, diabetes and hypertension were previously defined elsewhere [23]. Coronary reperfusion therapy was assumed when the participant underwent to percutaneous coronary intervention (PCI) and/or fibrinolytic therapy to restore the blood flow during MI. Anthropometrical measurements obtained were body weight (kg), height (m), and waist circumference (WC). Killip and GRACE scores were evaluated in all enrolled patients. Briefly, the GRACE risk score is a well-validated multivariable algorithm for predicting 10-year death risk following an initial acute coronary syndrome (ACS) [24].
Biochemical analysis
Blood samples were obtained within the first 24 h of MI symptoms (D1) and at day five of hospitalization (D5). High-sensitivity C-reactive protein (hs-CRP), urea, creatinine, triglycerides, total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and glomerular filtration rate (GFR) were obtained as described elsewhere [23]. Interleukin-2 and B-type natriuretic peptide levels were quantified by ELISA.
Nutritional evaluation
A food frequency intake questionnaire (FFQ) was used to estimate nutritional composition and ω-3 intake [alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA)] within the previous 3-month period. The questionnaire was applied at admission and at the 3rd month of follow-up. The food intake was clustered in 62 items divided into 10 groups (dairy products, eggs and meats, oils, snacks and canned foods, cereals and vegetables, greens and fruits, desserts and candies, beverages, diet and light products and spices). Approximate portions of usual intake of each item was recalled by patients with the aid of a photographic record for dietary surveys and the portion size was, subsequently, quantified into weights [25]. Total caloric and ω-3 intake were calculated based on a food composition database of the Brazilian Table of Food Composition (TACO) [26]. Briefly, TACO is a 399-item nutritional database with the most consumed foods in Brazil. Sample of foods were collected in 9 cities in all 5 Brazilian regions. Sampling was performed by mixing and packing two units of each principal brand collected in each site. The total units were separated in three different composites of 100–200 g, and then analyzed by certified laboratories. Contents of total lipids, cholesterol, saturated, poly- and monounsaturated fatty acids and trans fats were entered in the database [27]. Quantification of ω-3 from the questionnaires was performed by an experienced nutritionist (A.P.R.C.) and values were omitted from all other study participants.
Echocardiography
Participants underwent 3D Echocardiography at the first- and sixth-month following MI (iE 33 system; Philips Medical Systems, Andover, MA) according to current guidelines [28]. Left ventricle end-diastolic diameter (LVEDD), end-systolic diameter (LVESD), septum diastolic thickness (SD), and posterior wall diastolic thickness (PD), left ventricle end-diastolic volume (LVEDV) and end-systolic volume (LVESV) were obtained in 3D mode, and Ejection fraction (EF) was derived from these volumes.
Cardiac magnetic resonance imagining
Cardiac Magnetic Resonance imaging (CMRi) and CMRi data analysis were performed according to descriptions shown in a previous study [29].
Statistical analysis
Normally distributed data were presented as mean ± SD and skewed data as median and interquartile range (IQR). Participants were stratified into two groups according to daily consumption of ω-3 (below or above the median). Chi-square or two-tailed t tests were used for comparison of baseline data. Analyses of covariance (ANCOVA) was used to assess the association between ω-3 consumption and the change (Δ) of hs-CRP, IL-2 and BNP levels between D1 and D5. ANCOVA adjusted by covariates was also used to compare infarcted mass and the change in LVEF and LVEDV between 30 and 180 days. All analyses of the changes between D1 and D5 or between the 30th and the 180th day were additionally adjusted for the baseline levels in order to attenuate the effect of regression toward the mean. Multivariate binary logistic regression was used to evaluate the association between the dichotomous dependent variable ω-3 intake below or above the median and the independent variables Δhs-CPR, ΔIL-2, ΔBNP, ΔLVEF and ΔLVEDV. These dependent variables were categorized into below or above their respective medians to bypass the non-normal distribution and as a strategy to level their effects sizes, allowing direct comparability between variables. Stepwise selection of variables was used to reach the final model using the covariates. The following covariates were used for ANCOVA and regression analyses and were selected using bootstrapping based on t test analysis (Table 1): age, gender, diabetes mellitus, hypertension, coronary reperfusion therapy, and use of ACE inhibitors/ARBs. Restricted cubic spline models were used to assess the relationship between daily consumption of ω-3 and hs-CRP levels. Splines were adjusted by the GRACE score [24] and plasma peak CKMB levels. The GRACE score was chosen because its validity was confirmed as a predictive instrument in STEMI patients and due to the possibility of aggregating into a single index relevant covariate, thus reducing the saturation of the regression models. Statistical analysis was performed using SPSS®, version 21 for Mac (IBM) and STATA, version 15.0 for Mac. A two-sided p-value of 0.05 was considered statistically significant.
Results
Baseline characteristics are shown in Table 1. Participants who had a daily intake of ω-3 above the median (≥1.7 g/day) at admission had higher systolic blood pressure, higher levels of triglycerides and higher frequency of diabetes mellitus, hypertension, and coronary reperfusion therapy as well as the use of ACE inhibitors/ARBs than their counterparts.
Nutritional follow-up
Three months after STEMI, the food questionnaire was reapplied in order to evaluate the intake of ω-3 in this interlude. Participants who originally presented with ω-3 intake below the median (< 1.7 g/day) had no changes in their ω-3 intake during follow-up (from 1.0(0.7) to 1.1(0.9) g/day; p = 0.572). However, participants who originally had an intake of ω-3 above the median (≥1.7 g/day) reduced their ω-3 intake after STEMI (from 2.7(1.3) to 1.9(1.5) g/day; p < 0.001). Due to the natural limitation of the FFQ tool, it is not possible to specify the difference of 30% (0.8 g). Regardless, after 3 months, the higher intake group were still consuming significantly higher amounts of ω-3 (Table 1).
Inflammatory markers
Comparative analyses of inflammatory markers are shown in Table 2. Participants who consumed ω-3 above or below the median had equivalent levels of hs-CRP at D1. Participants who consumed ω-3 above the median had higher levels of IL-2 at D1 than their counterparts. The increase in both hs-CRP and IL-2 levels from D1 to D5 were smaller among those who consumed ω-3 above the median than their counterparts. All these comparative results remained significant after adjustment for covariates as indicated above.
Binary logistic regression models are shown in Table 3 and were used to assess the association between the intake of ω-3 and study endpoints. The intake of ω-3 was inversely associated with increase in hs-CRP and IL-2 levels (Δhs-CRP and ΔIL-2 – Model 1). Both associations remained significant after full adjustment for covariates (Model 2). The addition of smoking habit as covariate did not change the results.
Restricted cubic spline models were used to assess the relation between the daily consumption of ω-3 across changes in hs-CPR levels (Fig. 2). The consumption of ω-3 was inversely associated with the change in hs-CRP levels even after fully adjusted analysis (p = 0.01).

Restricted cubic spline curves to assess for relationship between daily consumption of ω-3 and change in hs-CRP (a), IL-2 (b) and BNP levels (c) during acute phase of STEMI (ΔCRP = D5 – D1). Splines were adjusted by the Global Registry of Acute Coronary Events (GRACE) score and plasma peak CKMB level
Cardiac remodeling
Comparative analyses of BNP levels, infarcted mass, LVEF, LVEDV and SI are shown in Table 2. No difference in plasma levels of BNP was observed at D1. However, BNP levels significantly increased in both subgroups from D1 to D5 (p < 0.001 and p = 0.032 for subgroups below and above the median, respectively). In the subgroup analysis, those who consumed ω-3 levels above the median had lower levels of BNP at D5 than their counterparts. Accordingly, participants who consumed ω-3 levels above the median had a smaller change in BNP levels (ΔD5-D1) than their counterparts; this difference remained significant after adjustment.
No differences were observed in the extension of infarcted mass obtained by CMRi neither in the LVEF at first and sixth months after STEMI. However, participants who consumed ω-3 levels above the median had an increase of LVEF from the first to the sixth month after STEMI while their counterparts had a decrease of LVEF in this period of time. Also, LVEDV was not different between the groups at the first and sixth month after STEMI. Nevertheless, participants who consumed ω-3 levels above the median had a decrease in LVEDV from the first to the sixth month while their counterparts had an increase in LVEDV in the same period.
The associations between the intake of ω-3 and the changes in the levels of BNP, LVEF and LVEDV measures were tested by binary logistic regression models as shown in Table 3. The intake of ω-3 below the median was inversely associated with increase in BNP levels. Conversely, the intake of ω-3 below the median was directly associated with reduction in LVEF and decrease in LVEDV. Both associations remained significant after full adjustment for covariates.
Discussion
In short, this study indicates that an increased daily intake of ω-3 (at least 1.7 g) is associated with attenuated inflammatory response and ventricular remodeling after STEMI.
Excessive increase in pro-inflammatory cytokines secretion after MI have been associated with a higher risk for mortality [30]. Clinically, hs-CRP is a has been established as the preferred biomarker for inflammatory activity given its long half-life and its value in predicting both the incidence of cardiovascular events and mortality [31]. In STEMI patients, we previously observed a direct relationship between the activation of the innate and TH1 inflammatory response after post-reperfusion expansion of the peri-infarcted myocardial mass [29]. This finding has motivated us to verify the effect of such inflammatory attenuation of the left ventricle remodeling after STEMI. In fact, in line with prior studies in chronic and acute disease [13,14,15,16,17,18,19], individuals consuming at least 1.7 g ω-3 had a greater reduction of IL-2 (a classical marker for Th1 response) and hs-CRP (a marker for innate response) during the acute phase of MI.
Higher intake of ω-3 before MI was associated with higher late gain of LVEF and decreased late gain of LVEDV, indicating a lower degree of remodeling. As the nutritional reanalysis of these individuals three months after STEMI continued to point to a higher consumption of ω-3, we cannot rule out the possibility that persistently increased consumption also contributed to this outcome. We also cannot exclude the possibility of a play of chance due to the observational design of this study, precluding the balance between the groups for variables not measured or not known. Nevertheless, the treatment of high-dose of ω-3 after STEMI has been shown to be associated with a reduction in left ventricular remodeling, myocardial fibrosis, and systemic inflammation in a prospective randomized controlled trial [32]. This may result from the anti-inflammatory action of these fatty acids and may also result from direct effects of ω-3 on myocardial cells. For example, ω-3 protects the metabolic and functional properties of cardiomyocytes submitted to conditions prone to insulin resistance, such as STEMI [33]. Also, intake of certain types of fatty acids may modulate cardiomyocyte gene expression and, by this way, change myocardial bioenergetics; ω-3, for example, stimulates angiopoietin-like protein 4 resulting in decreased cardiac absorption of fatty acids and decreased oxidative stress induced by fatty acids and lipid peroxidation [34]. Thus, the toning down of both systemic inflammatory activation and ventricular remodeling after STEMI may result from a combination of direct and indirect effects of ω-3.
Some limitations must be considered when reading this study. Firstly, as commented above, our findings must be considered as hypothesis generating due to the observational design and hence the impossibility to exclude selection bias. Randomized controlled trials (RCT) are required to exclude unbalance between the arms and the healthy cohort effect. However, consistency with RCT and mechanistic data deem this finding plausible. Other limitation that should be considered is the recall bias due to FFQ application, since participants are asked to report their food intake retrospectively in a prolonged period of time.
Conclusion
In conclusion, the findings of the present study suggest that a reduced daily intake of ω-3 may intensify outcome-determining mechanisms after STEMI, such as acute inflammatory response and late left ventricular remodeling.
Abbreviations
- ACEi:
-
Angiotensin-converting enzyme inhibitors
- ANCOVA:
-
Analysis of covariance
- AP-1:
-
Activator Protein-1
- ARB:
-
Angiotensin II receptor blockers
- BHS:
-
Brasília Heart Study
- BNP:
-
B-type natriuretic peptide
- CK-MB:
-
Creatine kinase myocardial bound
- CMRi:
-
Cardiac Magnetic Resonance imaging
- D1:
-
First day of hospitalization
- D5:
-
Fifth day of hospitalization
- FFQ:
-
Food frequency questionnaire
- hs-CRP:
-
High-sensitivity C-reactive protein
- IL-2:
-
Inteleucin-2
- LVEDD:
-
Left ventricle end-diastolic diameter
- LVEDV:
-
Left ventricle end-diastolic volume
- LVEF:
-
Left ventricle ejection fraction
- LVESD:
-
End-systolic diameter
- LVESV:
-
Left ventricle end-systolic volume
- MI:
-
Myocardial infarction
- NF-κB:
-
Nuclear Factor κB
- PD:
-
Posterior wall diastolic thickness
- SD:
-
Septum diastolic thickness
- STEMI:
-
ST-elevation myocardial infarction
- ΔD5-D1:
-
Change from fifth to first day of hospitalization
- ω-3:
-
Omega-3
References
Frangogiannis NG, Smith CW, Entman ML. The inflammatory response in myocardial infarction. Cardiovasc Res [Internet] 2002 [cited 2017 Sep 20];53(1):31–47. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11744011.
Irwin MW, Mak S, Mann DL, et al. Tissue expression and Immunolocalization of tumor necrosis factor-α in Postinfarction dysfunctional myocardium. Circulation [Internet] 1999 [cited 2017 Sep 20];99(11). Available from: http://circ.ahajournals.org/content/99/11/1492.
Gwechenberger M, Mendoza LH, Youker KA, et al. Cardiac myocytes produce interleukin-6 in culture and in viable border zone of reperfused infarctions. Circulation [Internet] 1999 [cited 2017 Sep 20];99(4):546–551. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9927402.
Valen G, M. van den D, D.J. D, P.D. V, D.K. D, T.F. L. Unstable angina activates myocardial heat shock protein 72, endothelial nitric oxide synthase, and transcription factors NFκB and AP-1. Cardiovasc Res [Internet] 2000 [cited 2017 Sep 26];47(1):49–56. Available from: https://academic.oup.com/cardiovascres/article/47/1/49/320725.
Pietilä KO, Harmoinen AP, Jokiniitty J, Pasternack AI. Serum C-reactive protein concentration in acute myocardial infarction and its relationship to mortality during 24 months of follow-up in patients under thrombolytic treatment. Eur Heart J [Internet] 1996 [cited 2017 Sep 17];17(9):1345–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8880019.
Saraste A, Pulkki K, Kallajoki M, Henriksen K, Parvinen M, Voipio-Pulkki LM. Apoptosis in human acute myocardial infarction. Circulation [Internet] 1997 [cited 2017 Sep 20];95(2):320–323. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9008443.
Elmas E, Popp T, Lang S, Dempfle CE, Kälsch T, Borggrefe M. Sudden death: do cytokines and prothrombotic peptides contribute to the occurrence of ventricular fibrillation during acute myocardial infarction? Int J Cardiol [Internet] 2010 [cited 2017 Sep 20];145(1):118–119. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19570584.
Hu C, Yang M, Zhu X, et al. Effects of Omega-3 fatty acids on markers of inflammation in patients with chronic kidney disease: a controversial issue. Ther Apher Dial. 2018;22(2):124–32.
Allaire J, Couture P, Leclerc M, et al. A randomized, crossover, head-to-head comparison of eicosapentaenoic acid and docosahexaenoic acid supplementation to reduce inflammation markers in men and women: the comparing EPA to DHA (ComparED) study. Am J Clin Nutr. 2016;104(2):280–7.
Haghiac M, Yang X, Presley L, et al. Dietary Omega-3 fatty acid supplementation reduces inflammation in obese pregnant women: a randomized double-blind controlled clinical trial. PLoS One. 2015;10(9):e0137309.
Di Nunzio M, Danesi F, Bordoni A. N-3 PUFA as regulators of cardiac gene transcription: a new link between PPAR activation and fatty acid composition. Lipids [Internet] 2009 [cited 2017 Sep 20];44(12):1073–1079. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19859757.
Babcock T, Kurland A, Helton W, Rahman A, Anwar K, Espat N. Inhibition of activator protein-1 transcription factor activation by omega-3 fatty acid modulation of mitogen-activated protein kinase signaling kinases. J Parenter Enter Nutr [Internet] 2003 [cited 2017 Sep 25];27(3):176–180. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12757110.
Canhada S, Castro K, Perry IS, Luft VC. Omega-3 fatty acids’ supplementation in Alzheimer’s disease: A systematic review. Nutr Neurosci [Internet] 2017 [cited 2017 Sep 25];1–10. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28466678.
Martin JM, Stapleton RD. Omega-3 fatty acids in critical illness. Nutr Rev [Internet] 2010 [cited 2017 Sep 25];68(9):531–541. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20796218.
Rajaei E, Mowla K, Ghorbani A, Bahadoram S, Bahadoram M, Dargahi-Malamir M. The effect of Omega-3 fatty acids in patients with active rheumatoid arthritis receiving DMARDs therapy: double-blind randomized controlled trial. Glob J Health Sci [Internet] 2015 [cited 2017 Sep 25];8(7):18. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26925896.
Gan RW, Young KA, Zerbe GO, et al. Lower omega-3 fatty acids are associated with the presence of anti-cyclic citrullinated peptide autoantibodies in a population at risk for future rheumatoid arthritis: a nested case-control study. Rheumatology [Internet] 2016 [cited 2017 Sep 25];55(2):367–376. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26370400.
Bi X, Li F, Liu S, et al. ω-3 polyunsaturated fatty acids ameliorate type 1 diabetes and autoimmunity. J Clin Invest [Internet] 2017 [cited 2017 Sep 25];127(5):1757–1771. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28375156.
Noori N, Dukkipati R, Kovesdy CP, et al. Dietary omega-3 fatty acid, ratio of omega-6 to omega-3 intake, inflammation, and survival in long-term hemodialysis patients. Am J Kidney Dis [Internet] 2011 [cited 2017 Sep 25];58(2):248–256. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21658827.
Kiecolt-Glaser JK, Epel ES, Belury MA, et al. Omega-3 fatty acids, oxidative stress, and leukocyte telomere length: a randomized controlled trial. Brain Behav Immun [Internet] 2013 [cited 2017 Sep 25];28:16–24. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23010452.
Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet (London, England) [Internet] 1999 [cited 2018 Jan 10];354(9177):447–55. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10465168.
Sposito AC, Alvarenga BF, Alexandre AS, et al. Most of the patients presenting myocardial infarction would not be eligible for intensive lipid-lowering based on clinical algorithms or plasma C-reactive protein. Atherosclerosis [Internet] 2011 [cited 2018 Jan 10];214(1):148–150. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21115179.
Wright RS, Anderson JL, Adams CD, et al. 2011 ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction. J Am Coll Cardiol 2011;57(19):e215–367.
Campos AM, Placido-Sposito A, Freitas WM, et al. ST-elevation myocardial infarction risk in the very elderly. BBA Clin [Internet] 2016 [cited 2016 Sep 26];6:108–12. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27635386.
Granger CB, Goldberg RJ, Dabbous O, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345.
Zabotto CB, Viana RP de T, Gil M de F. Registro fotográfico para inqueritos dietéticos: utensilios e porçöes [Internet]. Regist. fotográfico para inqueritos dietéticos Utens. e porçöes, vol. 76; 1996. Available from: https://www.fcm.unicamp.br/fcm/sites/default/files/2016/page/manual_fotografico.pdf.
NEPA N de E e P em A, UNICAMP UE de C. Tabela brasileira de composição de alimentos [Internet]. Campinas: UNICAMP/NEPA: 2011. Available from: http://www.cfn.org.br/wp-content/uploads/2017/03/taco_4_edicao_ampliada_e_revisada.pdf.
Galeazzi MAM, Lima DM, Colugnati FAB, Padovani RM, Rodriguez-Amaya DB. Sampling plan for the Brazilian TACO poject. J Food Compos Anal. 2002.
Lang RM, Badano LP, Tsang W, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur Heart J Cardiovasc Imaging. 2012.
Quinaglia e Silva JC, Coelho-Filho OR, Andrade JM, et al. Peri-Infarct Zone Characterized by Cardiac Magnetic Resonance Imaging is Directly Associated with the Inflammatory Activity During Acute Phase Myocardial Infarction. Inflammation [Internet] 2013 [cited 2017 Sep 27];37(3):678–85. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24282109.
Hamzic-Mehmedbasic A. Inflammatory Cytokines as Risk Factors for Mortality After Acute Cardiac Events. Med Arch (Sarajevo, Bosnia Herzegovina) [Internet] 2016 [cited 2017 Sep 26];70(4):252–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27703283.
Calabrò P, Golia E, Yeh ETH. Role of C-reactive protein in acute myocardial infarction and stroke: possible therapeutic approaches. Curr Pharm Biotechnol [Internet] 2012 [cited 2017 Sep 27];13(1):4–16. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21470166.
Heydari B, Abdullah S, Pottala J V., et al. Effect of Omega-3 acid ethyl esters on left ventricular remodeling after acute myocardial InfarctionClinical perspective. Circulation [Internet] 2016 [cited 2017 Oct 5];134(5). Available from: http://circ.ahajournals.org/content/134/5/378.
Franekova V, Angin Y, Hoebers NTH, et al. Marine omega-3 fatty acids prevent myocardial insulin resistance and metabolic remodeling as induced experimentally by high insulin exposure. Am J Physiol - Cell Physiol [Internet] 2015 [cited 2017 Nov 3];308(4):C297–307. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25472960.
Georgiadi A, Lichtenstein L, Degenhardt T, et al. Induction of cardiac Angptl4 by dietary fatty acids is mediated by peroxisome proliferator-activated receptor / and protects against fatty acid-induced oxidative stress. Circ Res [Internet] 2010 [cited 2017 Nov 3];106(11):1712–1721. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20378851.
Acknowledgements
Not applicable.
Ethical approval and consent to participate
BHS proceedings were in accordance with the Helsinki Declaration and the study was approved by the local Ethics Committee (083/06). Participants were only enrolled after signing informed consent. BHS is registered at ClinicalTrials.org (NCT02062554).
Funding
This work was supported by a grant from the Brazilian National Research Council (CNPq) grant number 308550/2010–2. Prof. Sposito is recipient of a Research Career Awards from the CNPq.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to ongoing proprietary work but are available from the corresponding author on reasonable request. The authors had full access to all of data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Consortia
Contributions
AMCS, APRC and SNS collected outpatient data, conducted data analyses and prepared the manuscript. LSFC, FAM, ORCF, WN, JQS and ACS reviewed the manuscript. ACS is the guarantor of this work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
All authors consent the submission of the manuscript as it is.
Competing interests
There are no financial and non-financial competing interests for all authors, who declare that they do not have a conflict of interest regarding the study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Campos-Staffico, A.M., Costa, A.P.R., Carvalho, L.S.F. et al. Omega-3 intake is associated with attenuated inflammatory response and cardiac remodeling after myocardial infarction. Nutr J 18, 29 (2019). https://doi.org/10.1186/s12937-019-0455-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-019-0455-1