
Abstract
Background
Further reductions in malaria incidence as more countries approach malaria elimination require the identification and treatment of asymptomatic individuals who carry mosquito-infective Plasmodium gametocytes that are responsible for furthering malaria transmission. Assessing the relationship between total parasitaemia and gametocytaemia in field surveys can provide insight as to whether detection of low-density, asymptomatic Plasmodium falciparum infections with sensitive molecular methods can adequately detect the majority of infected individuals who are potentially capable of onward transmission.
Methods
In a cross-sectional survey of 1354 healthy children and adults in three communities in western Kenya across a gradient of malaria transmission (Ajigo, Webuye, and Kapsisywa–Kipsamoite), asymptomatic P. falciparum infections were screened by rapid diagnostic tests, blood smear, and quantitative PCR of dried blood spots targeting the varATS gene in genomic DNA. A multiplex quantitative reverse-transcriptase PCR assay targeting female and male gametocyte genes (pfs25, pfs230p), a gene with a transcriptional pattern restricted to asexual blood stages (piesp2), and human GAPDH was also developed to determine total parasite and gametocyte densities among parasitaemic individuals.
Results
The prevalence of varATS-detectable asymptomatic infections was greatest in Ajigo (42%), followed by Webuye (10%). Only two infections were detected in Kapsisywa. No infections were detected in Kipsamoite. Across all communities, children aged 11–15 years account for the greatest proportion total and sub-microscopic asymptomatic infections. In younger age groups, the majority of infections were detectable by microscopy, while 68% of asymptomatically infected adults (> 21 years old) had sub-microscopic parasitaemia. Piesp2-derived parasite densities correlated poorly with microscopy-determined parasite densities in patent infections relative to varATS-based detection. In general, both male and female gametocytaemia increased with increasing varATS-derived total parasitaemia. A substantial proportion (41.7%) of individuals with potential for onward transmission had qPCR-estimated parasite densities below the limit of microscopic detection, but above the detectable limit of varATS qPCR.
Conclusions
This assessment of parasitaemia and gametocytaemia in three communities with different transmission intensities revealed evidence of a substantial sub-patent infectious reservoir among asymptomatic carriers of P. falciparum. Experimental studies are needed to definitively determine whether the low-density infections in communities such as Ajigo and Webuye contribute significantly to malaria transmission.
Similar content being viewed by others

Background
Malaria remains a global public health burden with 229 million cases worldwide in 2019 [1]. Transmission of malaria requires that sexual-stage Plasmodium parasites, gametocytes, present in the blood of infected humans be ingested by female Anopheles mosquitoes during feeding. Strategies that combine effective control of the mosquito vector through use of insecticide-treated nets (ITNs) and indoor residual spraying alongside rapid diagnosis and effective treatment of malaria with artemisinin-based combination therapy (ACT) have reduced the prevalence of Plasmodium falciparum infection and the incidence of clinical malaria in endemic areas of Africa since 2000, albeit at a slower rate in recent years [1]. Further reductions in malaria incidence as more countries approach malaria elimination would require the identification and treatment of asymptomatic individuals, who carry mosquito-infective gametocytes that are responsible for furthering malaria transmission [2].
Detection of asymptomatically infected individuals has been a major challenge given that individuals residing in areas of high-transmission intensity often carry parasitaemia at densities below the detection limits of accessible field diagnostics, which currently includes microscopy and rapid diagnostic tests (RDTs) [3]. Moreover, the proportion of low-density infections among all malaria infections in a community increases with decreasing malaria transmission [2], suggesting that more sensitive diagnostics are required for detecting parasitaemia among individuals in low-transmission settings [4]. Several studies have examined whether low-density infections contribute to onward transmission using mosquito feeding assays [5,6,7,8,9,10,11]. A recent meta-analysis of eight such studies estimated that individuals with sub-patent parasitaemia were approximately one-third as infectious to mosquitoes as individuals with blood-smear positive infections [4]. In general, gametocyte density directly correlates with mosquito infectivity and thus transmission, with infections with parasite densities below the limit of detection of conventional molecular diagnostics being unlikely to contribute significantly to transmission [12]. Assessing the relationship between total parasitaemia and gametocytaemia in field surveys can provide insight as to whether detection of low-density, asymptomatic P. falciparum infections using sensitive molecular methods can identify the majority of infected individuals who are potentially capable of onward transmission.
In this study, quantitative molecular assays were used to determine the prevalence and density of asymptomatic P. falciparum infections among children and adults in three communities of western Kenya that differed in transmission intensities. To better estimate the relationship between asexual parasite densities and gametocyte densities, a multiplex quantitative reverse-transcriptase polymerase chain reaction (PCR) assay for detecting asexual stage-specific, female gametocyte-specific, and male gametocyte-specific genes in a single blood sample was developed and evaluated. Results were compared to microscopy and an established quantitative PCR-based diagnostic assay.
Methods
Ethics approval and consent to participate
The study was reviewed and approved by the Kenya Medical Research Institute Scientific and Ethics Review Unit and the Indiana University Institutional Review Board. Written informed consent was obtained from a parent or guardian of participants who were minors and from adult participants. Minors aged 13–17 years provided their own written informed assent, accompanied by written consent of a parent or guardian.
Study sites and study participants
The study was conducted from August to September 2016 at three sites in western Kenya that differed in malaria transmission intensity. This time period was specifically chosen as it was one month after the primary malaria transmission peak but before the secondary peak for all three sites and thus increased the likelihood of recruiting individuals who had not experience symptomatic malaria within the last 30 days. Ajigo is located in the lowland area of Siaya County, where malaria transmission is intense and perennial, but with a seasonal peak from May to July [13, 14]. The Webuye township is in Bungoma County, which exhibits moderate, perennial transmission with a primary seasonal peak in May to June and a smaller, second peak in October [15,16,17]. Kapsisywa and Kipsamoite are two adjacent highland communities in Nandi County with low and unstable malaria transmission. Transmission for these two sites is highly variable, with a typical primary peak in May to July and an occasional smaller peak in November to December that varies from year to year [18, 19]. Intended recruitment targets were 200 participants in each of the moderate-to-high-transmission sites (the Matulo sublocation of Webuye and Ajigo) and 450 participants in each of the low-transmission sites (Kapsisywa and Kipsamoite). Sample sizes of 200, 450, and 900 participants provided 95% confidence of detecting within 20% of the true proportion of asymptomatic infections if the unknown prevalence was estimated to be 43%, 25%, and 14%, respectively. Healthy participants aged 1 to 85 years were recruited from a randomized community census of households for each site in an age-stratified manner to ensure adequate sample sizes for each age group, with a maximum of two participants for any household. Recruitment and enrollment occurred over a -week period. A brief questionnaire that included gender, age, recent travel history within the last month, recent use of ITNs, and relevant medical history was administered. Exclusion criteria at enrollment were axillary temperature ≥ 37.5 °C or history of fever, acute symptomatic illness, underlying chronic disease, malaria in the last 30 days, use of anti-malarial or immunosuppressive medications in the last 30 days, or pregnancy.
Blood collection
Drops of blood were collected by fingerprick for Paracheck Pf RDT (Orchid Biomedical Systems), which detects the presence of P. falciparum histidine-rich protein 2 in blood specimens; whole-blood ribonucleic acid (RNA); thick and thin blood smears; and dried blood spots (DBS) on filter paper (903 Protein Saver; Whatman). Individuals who tested positive for asymptomatic P. falciparum infection by RDT were treated at the point-of-care using the standard regimen recommended by the Ministry of Health in Kenya. For whole-blood RNA, 200 μl of peripheral fingerprick blood was collected using capillary blood collection tubes containing Tris-ethylenediaminetetraacetic acid (EDTA; Microvette CB300 K2E; Sarstedt) and transferred immediately in cryotubes pre-filled with 400 μl Tempus solution (Applied Biosystems). Filled sample tubes were agitated vigorously per the manufacturer’s instructions and stored at − 80 °C within 24 h of collection until use.
Microscopy
Giemsa-stained blood smears were examined for the presence of asexual parasites in 200 fields using the 100× oil immersion objective lens by two trained microscopists. Independent verification was performed by a third reader for samples that were qualitatively discordant for positivity between the first two microscopists. For positive samples, the number of asexual parasites per 200 leukocytes was multiplied by 40 to convert to parasites per μl, assuming an average leukocyte count of 8000 leukocytes per μl of blood. The mean parasite density from the two concordant microscopists were used for analysis.
Parasite culture
To produce parasite genomic deoxyribonucleic acid (gDNA) for use in standard curves for parasite density determination, P. falciparum 3D7 parasites [Malaria Research and Reference Reagent Resource Center (MR4), BEI Resources] were cultured in vitro using standard techniques [20] with two rounds of synchronization by sorbitol treatment to achieve a high parasitaemia. Ring and early trophozoite stage P. falciparum parasites were tenfold serially diluted in whole blood of an uninfected North American donor to obtain a final density of 440,000 down to 0.44 parasites/µl and spotted on 903 Protein Saver cards. To produce parasite RNA for use in standard curves for gametocyte density estimates, P. falciparum NF54 (MR4) in vitro cultures were enriched for gametocytes by decreasing asexual parasitaemia [17]. Total gametocytes (without differentiating for sex) were counted and tenfold serially diluted in whole blood to obtain a final density of 2580 down to 0.00258 gametocytes/μl immediately prior to RNA stabilization with Tempus solution at a 1:2 ratio. Asexual parasites (rings, trophozoites, and schizonts) were also counted in the same culture to allow parasite quantification using asexual-stage specific targets.
DNA and RNA isolation
Total DNA was extracted from three 0.32 cm diameter circles punched from each DBS using the QIAamp 96 Blood Kit (Qiagen, Valencia, CA) per the manufacturer’s instructions and eluted in 50 µl EDTA buffer. RNA was extracted from whole-blood RNA in Tempus using Norgen RNA extraction kit (Norgen Biotek, Thorold, Ontario) and treated with RNase-Free DNase I Kit (Norgen Biotek) to a final elution volume of 50 µl, per manufacturer’s instructions. Extracted RNA samples were assessed for quality and quantity using automated parallel capillary electrophoresis (Fragment Analyzer System, Agilent).
Real-time quantitative PCR using genomic DNA
To detect the presence of P. falciparum genomic DNA isolated from the DBS, primers targeting P. falciparum varATS that were originally designed for use in a Taqman-based qPCR assay [21] were adapted for use with the PowerUp SYBR Green Master Mix System (Thermo Fisher Scientific, Waltham, Massachusetts) (Additional file 1: Table S1). Samples were assayed in triplicate in 384-well plates on a QuantStudio 6 Flex Real Time PCR System (Thermo Fisher Scientific, Waltham, Massachusetts) using standard cycling conditions and a melt curve analysis. During assay development, PCR products were Sanger sequenced to verify that wells with a first calculated melt temperature (Tm1) > 71.14 °C contained varATS amplicons and wells with Tm1 < 71.14 °C contained primer dimers. Subsequently, the criteria for a P. falciparum positive sample were set as having ≥ 2 of 3 replicate wells with a Ct < 39 AND a Tm1 > 71.14 °C. Using these criteria, genomic DNA samples isolated from the blood of 20 of 20 (100%) healthy North American controls with no malaria exposure history were confirmed to be P. falciparum negative, and 86 of 87 (98.9%) samples positive by conventional P. falciparum 18s rRNA PCR [22, 23] were confirmed as positive with the modified varATS-based assay. The one discordant sample had only 1 of 3 replicate wells meeting the Ct and Tm1 criteria. A standard curve of gDNA extracted from serially diluted P. falciparum-spiked DBS samples (described above) and no-template negative controls were run on every plate, which allowed for estimation of parasite densities using Ct values.
Multiplex real-time quantitative reverse transcription PCR
An initial aim of the study was to develop a four-plex real-time quantitative reverse transcription PCR (RT-qPCR) that would detect female gametocytes, male gametocytes, and asexual parasites, as well as a human housekeeping gene glyceraldehyde 3-phosphate dehydrogenase (GAPDH), which served as a control for RNA extraction and relative quantification. The genes pfs25 [24] and pfs230p were used as the female- and male-specific gametocyte targets, respectively. The gene encoding for parasite-infected erythrocyte surface protein (piesp2, also called PFE60 and PF3D7_0501200) was chosen based on a transcriptional pattern restricted to asexual blood-stages, particularly trophozoites, in three P. falciparum gene expression datasets available on PlasmoDB (http://plasmodb.org) [25,26,27]. Primers and probes for pfs25 were adapted from Wampfler et al. [28]. Primers and probes for pfs230p and piesp2 were developed de novo using Primer 3 software [29] following standard guidelines for qPCR primer design. All primer and probes are listed in Additional file 1: Table S1.
After generation of complementary DNA (cDNA) from 50 ng RNA for each sample replicate using LunaScript RT Supermix (New England Biolabs) under standard cycling conditions, 20× triplex master mix was prepared from appropriate final concentrations of primers and probes for the three parasite targets and combined with 20× human GAPDH master mix (Applied Biosystems), Taqman multiplex master mix (Applied Biosystems), and cDNA to a final reaction volume of 10 μl. Field samples identified as positive for P. falciparum by varATS qPCR, no reverse transcriptase controls, amplification controls, and tenfold parasite RNA dilution standards were assayed in triplicate in 384-well MicroAMP Optical PCR plates (Applied Biosystems). The targets pfs25, pfs230p, piesp2, and human GAPDH were run in a QuantStudio6 Flex qPCR system (Applied Biosystems) with NFQ-MGB Quencher and VIC, FAM, ABY, and JUN reporter dyes, respectively (Additional file 1: Table S1). Mustang Purple was selected as the reference dye. Multiplex assay was run under standard cycling conditions: initial denaturation at 95.0 °C for 20 s (hold stage) followed by 40 cycles of 95.0 °C for 1 s and 60.0 °C for 20 s (PCR stage).
Statistical analysis
All statistical analyses were performed using R version 4.0.1 (https://www.r-project.org). Sample size estimates were performed using the epiR package. Multiple logistic regression was performed with PCR-confirmed gametocytaemia as the dependent variable and gender, age (in years), recent bed net use, recent travel, log10 transformed parasite density, and community as independent variables. Plots were rendered using the ggplot2 package. Statistical tests used to determine significance are indicated in tables and figure legends, and p values < 0.05 were considered significant.
Results
A total of 1354 participants were enrolled across all communities for this study (Table 1). The RDTs used for point-of-care diagnosis of asymptomatic infections demonstrated a 4.7% false positive rate using varATS qPCR as the reference standard. By contrast, microscopy showed no false positives. Given this, RDT data was not used for subsequent analyses. The prevalence of asymptomatic infections was greatest in Ajigo, followed by Webuye, regardless of diagnostic modality (Table 1). Only two asymptomatic infections were detected by PCR in Kapsisywa, and no infections were detected in Kipsamoite. Parasite densities were not statistically different across the four communities (Table 1) and did appear to vary with infection prevalence (Additional file 1: Fig. S1). The use of ITNs was higher in Ajigo and Webuye relative to Kapsisywa and Kipsamoite (Table 1). Given the similarities in prevalence of asymptomatic infections in the two highlands communities Kapsisywa and Kipsamoite, they were treated as a single community “Kap-Kip” for all subsequent analyses.
Across all communities, children aged 11–15 years account for the greatest prevalence of sub-microscopic (1.1%; 95% confidence interval [CI], 0.65% to 1.9%) and total PCR-detectable (3.0%; 95% CI 2.2% to 4.0%) asymptomatic infections (Fig. 1A). In contrast to the younger age groups, in which the majority of infections are detectable by microscopy, 68% of asymptomatically infected adults > 21 years of age have sub-microscopic parasitaemia (Fig. 1A), which suggests acquisition of blood-stage immunity [30, 31]. Similar findings were observed in Ajigo and Webuye when asymptomatic infection prevalence was separated by community with the notable observation that in individuals aged 6–20 years the majority of asymptomatic infections in Ajigo were detectable by microscopy, whereas in Webuye, the majority of infections in this age range were sub-microscopic (Fig. 1B). Multiple logistic regression confirmed that being a child aged 11–15 years and residence in the high-transmission settting of Ajigo were independent predictors for varATS-detectable parasitaemia after adjusting for gender, ITN use, and recent travel (Additional file 1: Table S2).

Prevalence of asymptomatic P. falciparum infections. Iceberg plot showing microscopy-detectable (above x axis) and sub-microscopic, PCR-detectable (below x axis) P. falciparum infections as a proportion of all individuals tested stratified by age group at A all sites or B by community. Numbers above and below each bar represent proportion of microscopy-detectable and sub-microscopic infections in each age group, respectively
For individuals identified as parasitemic by varATS qPCR, both asexual parasite densities and sexual parasite densities were quantified within the same sample by four-plex RT-qPCR (see “Methods”). Female and male gametocytes were quantified using qRT-PCR targeting pfs25 and pfs230p, respectively, and identified 122 of 1354 (9.0%; 95% CI 7.6% to 10.7%) as having gametocytaemia based on the quantifiable expression of either gene. Among individuals with varATS-detectable parasitaemia (n = 122), there were no significant differences in gender distribution, age, use of ITNs, history of recent travel, or site distribution between those with and without gametocytes by univariate analysis (Table 2). To determine the relationship between gametocytaemia and total parasitaemia, female and male gametocyte densities estimated by RT-qPCR were plotted against corresponding estimated asexual parasite densities. The initial plan was to use parasite densities estimated from piesp2 Ct values obtained from the same multiplex RT-qPCR assay, which would maintain internal consistency for each sample. However, piesp2-derived parasite densities demonstrated poorer correlation with microscopy-determined parasite densities in patent infections and less sensitivity than gDNA-based detection using varATS (Additional file 1: Fig. S2). Thus, total parasite densities derived from the varATS-based assay were used to approximate asexual parasite densities for the remainder of the study. Inclusion of varATS-estimated total parasite densities in a multiple logistic regression model revealed a decreased risk of gametocytaemia in the lower transmission communities relative to the high-transmission community of Ajigo and among individuals who reported recent travel (Table 3). As expected, increased total parasite densities greatly increased the likelihood of gametocytaemia independent of site (Table 3).
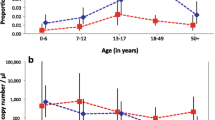
In general, both male and female gametocytaemia increased with increasing total parasitaemia (Fig. 2A, B). However, some individuals with very low total parasite densities were noted to have unexpectedly high gametocyte densities. Indeed, individuals with > 5 gametocytes/µl were bimodally distributed across a wide range of total parasitemia, which was more marked for pfs230p (Fig. 2C, D). Among individuals with low-density infections (total parasite densities < 40 parasites/μl), 28.3% (95% CI 17.2% to 42.6%) had > 5 gametocytes/μl estimated by pfs230p, and 20.8% (95% CI 11.3% to 34.5%) had > 5 gametocytes/μl estimated by pfs25 (Fig. 2E).

Relationship between total parasitaemia and gametocytemia. Spearman’s rank correlations between parasites/μl estimated by varATS and gametocytes/μl estimated by A pfs230p or B pfs25. Density plots of parasites/μl by number of gametocytes/μl estimated by C pfs230p or D pfs25. E Numbers (row proportions) of varATS-PCR positive individuals by number of gametocytes/μl
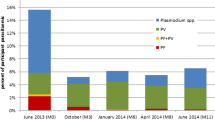
A substantial proportion (41.7%; 95% CI 29.3% to 55.1%) of individuals with potential for onward transmission, defined in our study as having at least 1.25 female and four male gametocytes per 2.5 µl of blood (thresholds adapted from a prior study [12] to account for sex-specific gametocytaemia overestimation), had qPCR-estimated parasite densities above the detectable limit of conventional, 18s ribosomal RNA-based nested PCR (1 parasite per µl) [22] and below the limit of detection of microscopy (40 parasites per µl), which corresponded well to the actual proportion potential transmitters with submicroscopic infections (40.0%; 95% CI 27.8% to 53.5%; Fig. 3A, B).

Distribution of individuals with potential for onward transmission. A Density plots by potential for onward transmission. Limit of detection for conventional molecular diagnostics and microscopy are shown as dashed black and red vertical lines, respectively. B Numbers (row proportions) of potential and unlikely transmitters by parasite density and blood smear positivity. Individuals with potential for onward transmission are defined in as having at least 1.25 female and four male gametocytes per 2.5 µl of blood, which are increased thresholds adapted from a prior study [12] to account for sex-specific gametocytaemia overestimation
Discussion
The current descriptive study provides a cross-sectional assessment of asymptomatic P. falciparum infections of three communities in western Kenya with differing malaria transmission intensities from August to September 2016. [12]. Similar to prior assessments, transmission intensity remained low in Kap-Kip [18, 32], where asymptomatic P. falciparum parasitaemia was rarely detected by varATS qPCR (0.22% prevalence). High malaria transmission was observed in Ajigo, where 42% of individuals had asymptomatic parasitaemia. Webuye demonstrated moderate transmission with 10% prevalence of asymptomatic parasitaemia, which is lower than what has been previously described at this site [33, 34], possibly reflecting micro-heterogeneity or seasonal differences, as the current study was performed during months when rainfall is historically lower in western Kenya.
The substantial reservoir observed among 6–15 year old children in Ajigo and Webuye is consistent with a prior study in the Kakamega district of western Kenya that showed PCR-confirmed asymptomatic P. falciparum infections were more prevalent in younger children age 5–14 years (~ 34%) relative to older children > 14 years (~ 9%) [35]. However, this observation contrasts with a study conducted in a high transmission area (Suba district) that demonstrated the prevalence of blood-smear positive asymptomatic infections was greater in young children < 5 years (74%) compared to older children (30–50%) [36]. The differences in relative contribution to the asymptomatic infectious reservoir by age groups may be attributable to intense malaria transmission in Suba, where clinical immunity may be acquired more rapidly, and differences in assay sensitivity.
To determine whether sensitive molecular assays can sufficiently detect the majority of individuals carrying low-density P. falciparum infections who are also potentially capable of onward transmission, the relationship between asexual parasitaemia and gametocytaemia was assessed. The initial goal was to correlate gametocyte densities with asexual parasite densities using a multiplex RT-qPCR that would contain targets specific to female gametocytes, male gametocytes, and asexual blood-stage parasites in a single assay, which would facilitate comparisons as this strategy eliminates both within subject differences in template preparation and assay variability. However, parasite densities determined using the chosen asexual-specific target piesp2, which encodes for parasite-infected erythrocyte surface protein and previously shown to be maximally transcribed in the trophozoite stage in laboratory isolates [25,26,27, 37], showed weaker correlation with microscopy-determined parasite density than densities derived from varATS qPCR using gDNA (Additional file 1: Fig. S2). The weaker correlation for piesp2 could be due to lower piesp2 expression in ring stages, which had previously been thought to be the predominant asexual form of P. falciparum found in peripheral circulation. However, a recent study in Mali revealed that more developed trophozoite stages were commonly found in asymptomatic P. falciparum infections [38]. Expression of piesp2 could also vary among the field isolates, perhaps due to differential transcriptional regulation related to precise stage at the time of collection or host immune pressure. Although speculative, these potential explanations are intriguing given that antibodies against PIESP2 associate with protection from malaria [39], and PIESP2 has recently been observed to bind to brain microvascular endothelial cells in vitro to induce an inflammatory response [40]. The current data, combined with these prior findings, suggest that piesp2 is a poor target for quantifying asexual parasite densities.
Nevertheless, using varATS-derived parasite densities, asexual parasitaemia and residence in a high-transmission setting independently predicted gametocytaemia, consistent with a recent longitudinal analysis of gametocyte carriage in Kilifi, Kenya [41]. On the surface, this might suggest that treating high-density infections in high-transmission settings, especially with ACT that is highly effective against early stage gametocytes (e.g. artemether–lumefantrine or artesunate/mefloquine) [42], would contribute to the overall reduction of gametocyte carriage. However, such a strategy neglects the potential contribution of sub-microscopic infections. The observation that a sizable proportion of low-density infections (< 40 parasites/μl) had estimated gametocyte densities that would favour onward transmission is also consistent with prior studies that demonstrated a considerable sub-microscopic infectious reservoir [4, 10, 43, 44]. Although the presence of gametocytaemia was only determined among individuals who were parasitaemic by varATS qPCR, which had a limit of detection of ~ 0.4 parasites/μl using dried blood spots, the proportion of individuals with potential for onward transmission drops off below 10 parasite/μl. This finding is in line with recent studies suggesting that mosquito infectivity occurs primarily when parasitaemia is > 1 parasite/μl [12, 45], which is the limit of detection of standard molecular diagnostics. Taken together, the main implication is that ultra-sensitive molecular diagnostics capable of detecting infections < 1 parasite/μl may not be necessary to achieve significant reductions in malaria transmission using a screen-and-treat strategy. However, experimental studies are needed to definitively determine whether the low-density infections in communities such as Ajigo and Webuye contribute significantly to malaria transmission.
There are several limitations to the current study. Although the study excluded individuals who endorsed symptoms of acute illness at the time of enrollment and sample collection, clinical or laboratory examinations that may have uncovered a more subacute or indolent disease process beyond self-reported symptoms were not performed. No short-term follow-up was conducted to assess whether asymptomatic individuals progressed to symptomatic malaria as other studies have done [46, 47]. By including potentially pre-symptomatic individuals, the prevalence of true asymptomatic infections may have been overestimated. Additionally, the cross-sectional study design provides only a snapshot of infection prevalence in these communities during the relatively dry season and the current findings may not be generalizable to the rainy season when malaria transmission is more intense. Gametocyte densities were estimated using molecular quantification of male and female gametocyte-specific gene expression as a surrogate of potential for onward transmission and did not directly measure mosquito infectivity using direct or indirect feeding assays. Such a surrogate based solely on gametocyte density ignores the relative contribution of anti-gametocyte immunity in reducing malaria transmission [48]. Although male and female gametocyte targets were used for gametocyte quantification, sex was not differentiated when determining gametocyte densities by microscopy for standard curves, which would lead to overestimates of sex-specific gametocytaemia. This is especially true for male-specific gametocytaemia given that natural infections are biased towards females, with 3–5 times more females [49]. However, no assessments using sex ratio were conducted in this study. Furthermore, gametocytaemia overestimates would affect all samples consistently and thus would not affect the ranked correlation analyses. Importantly, in determining the number of individuals capable of onward transmission, the effect of overestimating sex-specific gametocytaemia was reduced by using higher thresholds for minimum male and female gametocyte densities.
Conclusion
In summary, this cross-sectional survey of the prevalence and densities of P. falciparum infections among asymptomatic individuals in western Kenya provides an assessment of the relationship between parasitaemia and gametocytaemia in three communities with different transmission intensities. These data provide evidence of a substantial sub-patent infectious reservoir among asymptomatic carriers in these communities and supports prior findings that conventional molecular diagnostics may be capable of detecting the vast majority of infections capable of onward transmission [12]. Development of field-deployable molecular diagnostics to be used for the identification and treatment of asymptomatic carriers of P. falciparum could accelerate progress towards malaria elimination by reducing the infectious reservoir.
Availability of data and materials
Data and material used in this study will be made available upon request.
Abbreviations
- cDNA:
-
Complementary deoxyribonucleic acid
- CI:
-
Confidence interval
- DBS:
-
Dried blood spot
- EDTA:
-
Ethylenediaminetetraacetic acid
- gDNA:
-
Genomic deoxyribonucleic acid
- ITN:
-
Insecticide-treated net
- MR4:
-
Malaria Research and Reference Reagent Resource Center
- PCR:
-
Polymerase chain reaction
- RDT:
-
Rapid diagnostic test
- RNA:
-
Ribonucleic acid
- RT-qPCR:
-
Real-time quantitative reverse transcription PCR
References
WHO. World malaria report 2020. Geneva: World Health Organization; 2020.
malERA Refresh Consultative Panel. malERA: an updated research agenda for characterising the reservoir and measuring transmission in malaria elimination and eradication. PLoS Med. 2017;14:e1002452.
Bousema T, Okell L, Felger I, Drakeley C. Asymptomatic malaria infections: detectability, transmissibility and public health relevance. Nat Rev Microbiol. 2014;12:833–40.
Slater HC, Ross A, Felger I, Hofmann NE, Robinson L, Cook J, et al. The temporal dynamics and infectiousness of subpatent Plasmodium falciparum infections in relation to parasite density. Nat Commun. 2019;10:1433.
Githeko AK, Brandling-Bennett AD, Beier M, Atieli F, Owaga M, Collins FH. The reservoir of Plasmodium falciparum malaria in a holoendemic area of western Kenya. Trans R Soc Trop Med Hyg. 1992;86:355–8.
Coleman RE, Kumpitak C, Ponlawat A, Maneechai N, Phunkitchar V, Rachapaew N, et al. Infectivity of asymptomatic Plasmodium-infected human populations to Anopheles dirus mosquitoes in western Thailand. J Med Entomol. 2004;41:201–8.
Ouedraogo AL, Bousema T, Schneider P, de Vlas SJ, Ilboudo-Sanogo E, Cuzin-Ouattara N, et al. Substantial contribution of submicroscopical Plasmodium falciparum gametocyte carriage to the infectious reservoir in an area of seasonal transmission. PLoS ONE. 2009;4:e8410.
Gaye A, Bousema T, Libasse G, Ndiath MO, Konate L, Jawara M, et al. Infectiousness of the human population to Anopheles arabiensis by direct skin feeding in an area hypoendemic for malaria in Senegal. Am J Trop Med Hyg. 2015;92:648–52.
Ouedraogo AL, Goncalves BP, Gneme A, Wenger EA, Guelbeogo MW, Ouedraogo A, et al. Dynamics of the human infectious reservoir for malaria determined by mosquito feeding assays and ultrasensitive malaria diagnosis in Burkina Faso. J Infect Dis. 2016;213:90–9.
Goncalves BP, Kapulu MC, Sawa P, Guelbeogo WM, Tiono AB, Grignard L, et al. Examining the human infectious reservoir for Plasmodium falciparum malaria in areas of differing transmission intensity. Nat Commun. 2017;8:1133.
Tadesse FG, Slater HC, Chali W, Teelen K, Lanke K, Belachew M, et al. The relative contribution of symptomatic and asymptomatic Plasmodium vivax and Plasmodium falciparum infections to the infectious reservoir in a low-endemic setting in Ethiopia. Clin Infect Dis. 2018;66:1883–91.
Gruenberg M, Hofmann NE, Nate E, Karl S, Robinson LJ, Lanke K, et al. qRT-PCR versus IFA-based quantification of male and female gametocytes in low-density Plasmodium falciparum infections and their relevance for transmission. J Infect Dis. 2020;221:598–607.
Zhou Z, Mitchell RM, Kariuki S, Odero C, Otieno P, Otieno K, et al. Assessment of submicroscopic infections and gametocyte carriage of Plasmodium falciparum during peak malaria transmission season in a community-based cross-sectional survey in western Kenya, 2012. Malar J. 2016;15:421.
Apat DO, Gachohi JM, Karama M, Kiplimo JR, Sachs SE. Temporal variation in confirmed diagnosis of fever-related malarial cases among children under-5 years by community health workers and in health facilities between years 2013 and 2015 in Siaya County, Kenya. Malar J. 2017;16:454.
Obala AA, Mangeni JN, Platt A, Aswa D, Abel L, Namae J, et al. What is threatening the effectiveness of insecticide-treated bednets? A case-control study of environmental, behavioral, and physical factors associated with prevention failure. PLoS ONE. 2015;10:e0132778.
Mangeni JN, Menya D, Obala A, Platt A, O’Meara WP. Development and validation of a rapid assessment tool for malaria prevention. Malar J. 2016;15:544.
Roncales M, Vidal-Mas J, Leroy D, Herreros E. Comparison and optimization of different methods for the in vitro production of Plasmodium falciparum gametocytes. J Parasitol Res. 2012;2012:927148.
Hamre KES, Hodges JS, Ayodo G, John CC. Lack of consistent malaria incidence hotspots in a highland Kenyan area during a 10-year period of very low and unstable transmission. Am J Trop Med Hyg. 2020;103:2198–207.
Hamre KES, Ayodo G, Hodges JS, John CC. A mass insecticide-treated bed net distribution campaign reduced malaria risk on an individual but not population level in a highland epidemic-prone area of Kenya. Am J Trop Med Hyg. 2020;103:2183–8.
Trager W, Jensen JB. Human malaria parasites in continuous culture. Science. 1976;193:673–5.
Hofmann N, Mwingira F, Shekalaghe S, Robinson LJ, Mueller I, Felger I. Ultra-sensitive detection of Plasmodium falciparum by amplification of multi-copy subtelomeric targets. PLoS Med. 2015;12:e1001788.
Snounou G, Viriyakosol S, Zhu XP, Jarra W, Pinheiro L, do Rosario VE, Thaithong S, Brown KN. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol Biochem Parasitol. 1993;61:315–20.
Tran TM, Aghili A, Li S, Ongoiba A, Kayentao K, Doumbo S, Traore B, Crompton PD. A nested real-time PCR assay for the quantification of Plasmodium falciparum DNA extracted from dried blood spots. Malar J. 2014;13:393.
Kaslow DC, Quakyi IA, Syin C, Raum MG, Keister DB, Coligan JE, et al. A vaccine candidate from the sexual stage of human malaria that contains EGF-like domains. Nature. 1988;333:74–6.
Le Roch KG, Johnson JR, Florens L, Zhou Y, Santrosyan A, Grainger M, et al. Global analysis of transcript and protein levels across the Plasmodium falciparum life cycle. Genome Res. 2004;14:2308–18.
Otto TD, Wilinski D, Assefa S, Keane TM, Sarry LR, Bohme U, et al. New insights into the blood-stage transcriptome of Plasmodium falciparum using RNA-Seq. Mol Microbiol. 2010;76:12–24.
Lopez-Barragan MJ, Lemieux J, Quinones M, Williamson KC, Molina-Cruz A, Cui K, Barillas-Mury C, et al. Directional gene expression and antisense transcripts in sexual and asexual stages of Plasmodium falciparum. BMC Genom. 2011;12:587.
Wampfler R, Mwingira F, Javati S, Robinson L, Betuela I, Siba P, et al. Strategies for detection of Plasmodium species gametocytes. PLoS ONE. 2013;8:e76316.
Koressaar T, Lepamets M, Kaplinski L, Raime K, Andreson R, Remm M. Primer3_masker: integrating masking of template sequence with primer design software. Bioinformatics. 2018;34:1937–8.
Okell LC, Bousema T, Griffin JT, Ouedraogo AL, Ghani AC, Drakeley CJ. Factors determining the occurrence of submicroscopic malaria infections and their relevance for control. Nat Commun. 2012;3:1237.
Tran TM, Li S, Doumbo S, Doumtabe D, Huang CY, Dia S, et al. An intensive longitudinal cohort study of Malian children and adults reveals no evidence of acquired immunity to Plasmodium falciparum infection. Clin Infect Dis. 2013;57:40–7.
John CC, McHugh MM, Moormann AM, Sumba PO, Ofulla AV. Low prevalence of Plasmodium falciparum infection among asymptomatic individuals in a highland area of Kenya. Trans R Soc Trop Med Hyg. 2005;99:780–6.
Mangeni JN, Ongore D, Mwangi A, Vulule JM, Prudhomme O’Meara W, Obala A. Prevalence, heterogeneity of asymptomatic malaria infections and associated factors in a high transmission region. East Afr Med J. 2017;94:1.
Taylor SM, Sumner KM, Freedman B, Mangeni JN, Obala AA, Prudhomme OW. Direct estimation of sensitivity of Plasmodium falciparum rapid diagnostic test for active case detection in a high-transmission community setting. Am J Trop Med Hyg. 2019;101:1416–23.
Baliraine FN, Afrane YA, Amenya DA, Bonizzoni M, Menge DM, Zhou G, et al. High prevalence of asymptomatic Plasmodium falciparum infections in a highland area of western Kenya: a cohort study. J Infect Dis. 2009;200:66–74.
Bousema JT, Gouagna LC, Drakeley CJ, Meutstege AM, Okech BA, Akim IN, et al. Plasmodium falciparum gametocyte carriage in asymptomatic children in western Kenya. Malar J. 2004;3:18.
Liu X, Wang Y, Liang J, Wang L, Qin N, Zhao Y, et al. In-depth comparative analysis of malaria parasite genomes reveals protein-coding genes linked to human disease in Plasmodium falciparum genome. BMC Genom. 2018;19:312.
Andrade CM, Fleckenstein H, Thomson-Luque R, Doumbo S, Lima NF, Anderson C, et al. Increased circulation time of Plasmodium falciparum underlies persistent asymptomatic infection in the dry season. Nat Med. 2020;26:1929–40.
Crompton PD, Kayala MA, Traore B, Kayentao K, Ongoiba A, Weiss GE, et al. A prospective analysis of the Ab response to Plasmodium falciparum before and after a malaria season by protein microarray. Proc Natl Acad Sci USA. 2010;107:6958–63.
Liu X, Wu Y, Zhao Y, Huang Y, Xu K, Wang J, et al. Identification of Plasmodium falciparum-specific protein PIESP2 as a novel virulence factor related to cerebral malaria. Int J Biol Macromol. 2021;177:535–47.
Muthui MK, Mogeni P, Mwai K, Nyundo C, Macharia A, Williams TN, et al. Gametocyte carriage in an era of changing malaria epidemiology: a 19-year analysis of a malaria longitudinal cohort. Wellcome Open Res. 2019;4:66.
WWARN Gametocyte Study Group. Gametocyte carriage in uncomplicated Plasmodium falciparum malaria following treatment with artemisinin combination therapy: a systematic review and meta-analysis of individual patient data. BMC Med. 2016;14:79.
Kobayashi T, Kanyangarara M, Laban NM, Phiri M, Hamapumbu H, Searle KM, et al. Characteristics of subpatent malaria in a pre-elimination setting in Southern Zambia. Am J Trop Med Hyg. 2019;100:280–6.
Thanh PV, Van Hong N, Van Van N, Van Malderen C, Obsomer V, Rosanas-Urgell A, et al. Epidemiology of forest malaria in Central Vietnam: the hidden parasite reservoir. Malar J. 2015;14:86.
Kiattibutr K, Roobsoong W, Sriwichai P, Saeseu T, Rachaphaew N, Suansomjit C, et al. Infectivity of symptomatic and asymptomatic Plasmodium vivax infections to a Southeast Asian vector, Anopheles dirus. Int J Parasitol. 2017;47:163–70.
Njama-Meya D, Kamya MR, Dorsey G. Asymptomatic parasitaemia as a risk factor for symptomatic malaria in a cohort of Ugandan children. Trop Med Int Health. 2004;9:862–8.
Tran TM, Guha R, Portugal S, Skinner J, Ongoiba A, Bhardwaj J, et al. A molecular signature in blood reveals a role for p53 in regulating malaria-induced inflammation. Immunity. 2019;51:750-765.e10.
Ouedraogo AL, Eckhoff PA, Luty AJF, Roeffen W, Sauerwein RW, Bousema T, et al. Modeling the impact of Plasmodium falciparum sexual stage immunity on the composition and dynamics of the human infectious reservoir for malaria in natural settings. PLoS Pathog. 2018;14:e1007034.
Tadesse FG, Meerstein-Kessel L, Goncalves BP, Drakeley C, Ranford-Cartwright L, Bousema T. Gametocyte sex ratio: the key to understanding Plasmodium falciparum transmission? Trends Parasitol. 2019;35:226–38.
Acknowledgements
We are grateful to all the study participants. We thank Brian Grimberg (Case Western Reserve University) for his assistance with developing the multiplex qPCR assay and Erik Gaskin for his careful review of the literature.
Funding
This project was funded with support from the Indiana Clinical and Translational Sciences Institute funded, in part by Grant #’s UL1TR001108 and KL2TR001106 from the National Institutes of Health, National Center for Advancing Translational Sciences, Clinical and Translational Sciences Award. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. TMT is also supported by the National Institute of Allergy and Infectious Diseases (Grant# 5K08AI125682) and the Doris Duke Charitable Foundation (Grant # 2018091).
Author information
Authors and Affiliations
Contributions
GA, WPO, CCJ, and TMT designed the study. GA, EOO, AO, and TMT coordinated and conducted the field studies. CS, MDM, and MPG designed and performed the experiments. MDM, SN, and TMT processed and analyzed the data. CS, WPO, CCJ, and TMT wrote the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the Kenya Medical Research Institute Scientific and Ethics Review Unit and the Indiana University Institutional Review Board. Written informed consent was obtained from a parent or guardian of participants who were minors and from adult participants. Minors aged 13–17 years of age provided their own written informed assent, accompanied by written consent of a parent or guardian.
Consent for publication
All authors read and approved the final version of this manuscript for publication.
Competing interests
None of the authors have competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Supplementary tables and figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salgado, C., Ayodo, G., Macklin, M.D. et al. The prevalence and density of asymptomatic Plasmodium falciparum infections among children and adults in three communities of western Kenya. Malar J 20, 371 (2021). https://doi.org/10.1186/s12936-021-03905-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-021-03905-w