
Abstract
Background
Although mixed infection by two Plasmodium species has been recognized, mixed infection by three different Plasmodium species within one individual has not been clarified. This study sought to determine the pooled prevalence and proportion of triple mixed Plasmodium spp. infection compared with double mixed infection.
Methods
Articles from PubMed, Scopus, and Web of Science were searched for cross-sectional studies of triple mixed infection by Plasmodium species and then were retrieved and extracted. The pooled proportion and prevalence of triple mixed infection by Plasmodium species were subjected to random-effects analysis. The secondary outcomes were differences in the pooled proportion between triple mixed infection and double mixed infection by Plasmodium species reported in the included studies.
Results
Of 5621 identified studies, triple mixed infection data were available for 35 records, including 601 patients from 22 countries. The overall pooled prevalence of triple mixed infection was 4% (95% Confidence Interval (CI) 3–5%; I2 = 92.5%). The pooled proportion of triple mixed infection compared with double mixed infection was 12% (95% CI 9–18; I2 = 91%). Most of the included studies (29/35; 82.9%) presented a lower proportion of triple mixed infection than double mixed infection. Subgroup analysis demonstrated that the proportion of triple mixed infection was the highest in Oceania (23%; 95% CI 15–36%) and Europe (21%; 95% CI 5–86%), but the lowest in the USA (3%; 95% CI 2–4%). Moreover, the proportion of triple mixed infection was higher in residents (20%; 95% CI 14–29%) than in febrile patients (7%; 95% CI 4–13%), when compared with the proportion of double mixed infection. Subgroup analysis of the age groups demonstrated that, compared with the proportion of double mixed infection, triple mixed infection was lower in patients aged ≤ 5 years (OR = 0.27; 95% CI 0.13–0.56; I2 = 31%) and > 5 years (OR = 0.09; 95% CI 0.04–0.25, I2 = 78%).
Conclusions
The present study suggested that, in areas where triple mixed infection were endemic, PCR or molecular diagnosis for all residents in communities where malaria is submicroscopic can provide prevalence data and intervention measures, as well as prevent disease transmission and enhance malaria elimination efforts.
Similar content being viewed by others

Background
Malaria remains a major disease of public health concern worldwide, particularly in sub-Saharan Africa [1]. In 2018, the World Health Organization (WHO) estimated 228 million cases and 405,000 deaths caused by malaria worldwide, mostly in children aged younger than 5 years [1]. Infections of the Plasmodium species usually present as monoinfection by one species; however, mixed infections by more than one species within one individual can occur [2,3,4,5,6]. The interactions between mixed infections are not well characterized, but may play roles in disease progression and outcomes [7]. Moreover, mixed infections by Plasmodium species are often not recognized or are underestimated by microscopists [8]. In Asia, mixed infections by Plasmodium species have occurred at a frequency of 2% to 30% [9]. Although mixed infection by two Plasmodium species has been recognized, mixed infection by three different Plasmodium species within one individual has not been clarified.
This study sought to determine the pooled prevalence and proportion of triple mixed infection by Plasmodium spp. compared with double mixed infection. This information is necessary to guide the progress of research on mixed infection and malaria management, as well as control strategies for strategic malaria diagnostic service choices and treatment options.
Methods
Search strategy
Articles from PubMed, Scopus, and Web of Science were searched for cross-sectional studies on triple mixed infection by Plasmodium species in patients with all species of malaria. Triple mixed infection were defined as infection with three Plasmodium species. Articles published between February 2, 1907, and February 24, 2020, in the English language were included in the analysis if they explicitly reported the presence of triple mixed infection by Plasmodium species. The search strategy included the search terms “(Plasmodium OR Malaria) AND (“Mixed infection” OR “Triple infection”)” (Additional file 1: Table S1).
Selection criteria
Observational studies, prospective cohorts, and case–control designs were included if they reported triple mixed malaria infection among the included participants by polymerase chain reaction (PCR) or molecular methods. Studies were excluded if the numbers of triple mixed infection could not be extracted and if only one species of Plasmodium was studied or evaluated subsequently from microscopy or rapid diagnostic test (RDT). Animal studies, clinical drug trials, case reports, experimental studies, reviews, systematic reviews, and polymorphism studies were excluded because they were considered incompatible study designs for the present review and meta-analysis. Studies were selected and identified by two independent authors (MK and KUK), with discrepancies resolved following discussion with a third author (FM). The protocol of this analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Data extraction and definitions
The data extracted for individual studies included author names, year of publication, study area, year of study, details, and numbers of the participants, age ranges, blood collection methods, DNA extraction method, investigated gene, PCR method, malaria positivity status, number of double mixed infections, and number of triple mixed infections. The numbers of patients with four different Plasmodium species were also extracted for further discussions in the present study. Subgroup analyses were performed for the following parameters: publication year (before and after 2000), continent (Asia, Africa, America, Europe, or Oceania), participant group (febrile patients and residents from the same community), type of blood storage for PCR (EDTA blood or dried blood spots), and age group of patients with mixed infection.
Data analysis
The primary outcome was the pooled proportion and pooled prevalence of triple mixed infection by Plasmodium species, with random-effects meta-regression used to investigate these pooled analyses. The analyses were performed using Stata Statistical Software (Release 15; StataCorp LLC. USA). The secondary outcomes were differences in the pooled proportion between triple mixed infection and dual mixed infection by Plasmodium species reported in the included studies. Those differences were estimated using random-effects meta-analysis to calculate the odds ratio (ORs) and 95% confidence intervals (CI). The analyses were performed using Review Manager 5 (RevMan 5, Cochrane Community).
Potential bias related to individual studies was assessed using a tool developed by the Newcastle-Ottawa Scale (NOS) to assessing the quality of non-randomized studies in meta-analyses. The quality of included studies was rated if they qualified with a maximum of 7 stars. Publication bias related to study effects was assessed by funnel plot asymmetry. Between-study heterogeneity was assessed by the I2 statistic and was assessed using the random-effects statistic. Subgroup analysis of the baseline characteristics included continent (Asia, Africa, America, Europe, or Oceania), participants (residents and febrile individuals), type of blood storage for PCR (EDTA blood or dried blood spots), and age group. For the subgroup analyses of age groups and different mixed infections (double and triple infection), the age groups of patients were classified as ≤ 5 and > 5 years because children younger than 5 years are one of the most vulnerable groups affected by malaria [10].
Results
Characteristics of the included studies
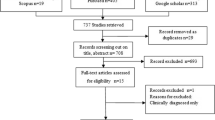
After screening the titles and abstracts of 5621 identified studies published between February 2, 1907, and February 24, 2020, the full texts of 344 (6.11%) potentially relevant studies were reviewed (Fig. 1). There were 309 studies that did not meet the inclusion criteria, mostly because they did not document triple mixed infection by Plasmodium species in their studies. Thirty-five (10.1%) of 344 studies could be extracted and were included in the analysis (Table 1). Of the 35 studies, 14 (40%) were from the Asia–Pacific region, 9 (25.7%) were from Africa, 5 (14.3%) were from Europe, 4 (11.4%) were from Oceania, and three (8.6%) were from the (Table 1). Among 35 included studies from 22 different countries, most (4/35, 11.4%) were from Papua New Guinea [11,12,13,14], Cambodia [15,16,17], India [6, 18, 19], Italy [4, 20, 21], and Uganda [2, 22, 23]. Most of the participants included among the studies were residents (16/35, 45.7%), febrile patients (11/35, 31.4%), and malaria-positive cases (6/35, 17.1%). Twenty-four studies (68.6%) reported age ranges, whereas others did not. One study used samples from doubtful microscopic examination [18], whereas another enrolled both febrile and asymptomatic patients to perform PCR analysis [6]. More than half of the included studies (18/35, 51.4%) used EDTA blood to extract the DNA for PCR analysis, whereas others used dried blood spots (15/35, 42.9%), and one study used thick smears for DNA extraction [24]. Most of the studies (28/35, 80%) used DNA commercial kits, while four studies (4/35, 11.4%) used 30% Chelex-100 and phenol–chloroform extraction for DNA extraction. All of the included studies used the 18S ribosomal RNA (rRNA) gene to identify the Plasmodium genus and species. Overall, 44,310 participants were enrolled in the included studies. Of those, most were residents (34,483, 77.8%), febrile patients (7797, 17.6%), and malaria-positive samples (1675, 3.78%).

Flow chart for the study selection
Regarding the number of malaria-positive participants by PCR, 12,023 patients were infected by one of the five Plasmodium species (Plasmodium falciparum, Plasmodium vivax, Plasmodium malariae, Plasmodium ovale, and Plasmodium knowlesi). Among those positive patients, 3059 (25.4%) were infected with two different Plasmodium species. The most common types of mixed infection were P. falciparum and P. vivax (1318, 11%), P. falciparum and P. malariae (775, 6.4%), and P. vivax and P. malariae (645, 5.4%). Among those 12,023 positive patients, 601 (5%) were infected with three different Plasmodium species. The most common types of mixed infection were P. falciparum/P. malariae/P. vivax (355, 3%), P. falciparum/P. malariae/P. ovale (137, 1.1%), and P. falciparum/P. vivax/P. ovale (83, 0.7%). Fifty-three patients (0.44%) had quadruple mixed infection with P. falciparum/P. vivax/P. malariae/P. ovale.
Quadruple mixed infection was identified among the present studies and comprised of P. falciparum/P. vivax/P. malariae/P. ovale in one individual. Fifty-three patients (0.44%) had quadruple mixed infection. Most (40/53, 75.5%) were found in Papua New Guinea [11,12,13,14], followed by Cambodia (12/53, 22.6%) [15,16,17], Thailand (8/53, 15%) [24, 25], India (1/53, 1.9%) [18], China (1/53, 1.9%) [26], and Laos (1/53, 1.9%) [27].
Quality of the included studies
All of the included studies were rated with a maximum of 7 stars (Table 2). Sixteen studies received 7 stars, 12 received 6 stars, and 7 received 5 stars. The twelve studies rated with 6 stars used febrile controls, and the 7 studies rated with 5 stars used malaria-positive samples for PCR analysis.
The pooled prevalence of triple mixed infection
The numbers of triple mixed infection were available for 35 records that included 601 patients from 22 countries. The overall pooled prevalence of triple mixed infection (4%; 95% CI 3–5%; I2 = 92.5%) with no evidence of publication bias related to small study effects is shown in the funnel plot (Fig. 2). The highest prevalence of triple mixed infection for an individual study was 46% (95% CI 37–55) in a study by Zhou et al. [24].

Pooled prevalence of triple mixed infections by Plasmodium species
Comparison of the pooled proportion of triple and double mixed infections
The pooled proportion of triple mixed infection compared with double mixed infection was 12% (95% CI 9–18, I2 = 91%) (Fig. 3). Most of the included studies (29/35, 82.9%) presented a lower proportion of triple mixed infection than double mixed infection. Only one study demonstrated a higher proportion of triple mixed infection than double mixed infection [24]. Another included study by Peruzzi et al. could not input the present meta-analysis because it had only reported on triple mixed infection, not double mixed infection [21].

Pooled proportion of triple mixed infections by Plasmodium species compared with double mixed infections
Subgroup analysis
Subgroup analysis of the continents from 34 studies where triple mixed infection were reported in the included studies was available. The analysis demonstrated that the proportion of triple mixed infection was the highest in Oceania 23% (95% CI 15–36%) and Europe 21% (95% CI 5–86%) compared with that of double mixed infection (Fig. 4). However, the proportion of triple mixed infection was the lowest in America (3%; 95% CI 2–4%). A subgroup difference was found between continents with a high level of heterogeneity (P-value < 0.0001, I2 = 94.8%).

Subgroup analysis of triple mixed infections by Plasmodium species between areas of the included studies
Subgroup analysis of the febrile subjects and residents from 27 studies was available (Fig. 5). Compared with the proportion of double mixed infection, triple mixed infection was higher in residents (20%; 95% CI 14–29%) than in febrile patients (7%; 95% CI 4–13%). A subgroup difference was observed between febrile patients and residents with a high level of heterogeneity (P-value = 0.004, I2 = 88.2%). Subgroup analysis of the blood collection method for PCR from 32 studies was available. The proportion of triple mixed infection using EDTA blood was 13% (95% CI 8–21%) and dried blood spots was 10% (95% CI 7–17%), with no subgroup difference between the groups (P-value = 0.59; Fig. 6).

Subgroup analysis of triple mixed infections by Plasmodium species between residents and febrile groups

Subgroup analysis of triple mixed infections by Plasmodium species between the two blood collection methods
Seven included studies reported the age groups, and different types of mixed infection (85 triple mixed infection and 581 double mixed infection). Subgroup analysis of age groups demonstrated that, compared with the proportion of double mixed infection, triple mixed infection was lower in patients aged ≤ 5 years (OR = 0.27; 95% CI 0.13–0.56; I2 = 31%) and > 5 years (OR = 0.09; 95% CI 0.04–0.25; I2 = 78%) (Fig. 7). Subgroup analysis demonstrated no statistical difference (P-value = 0.09, I2 = 64.7%).

Subgroup analysis of triple mixed infections by Plasmodium species between the two age groups
Publication bias
Publication bias related to study effects was assessed using funnel plot asymmetry, and no publication bias was demonstrated as evidenced by the symmetry of the funnel plot (Fig. 8).

Publication bias among the included studies as demonstrated by funnel plot analysis
Discussion
The pooled prevalence of triple mixed infection has not been clarified in the previous literature. The systematic review and meta-analysis of 12,023 malaria-positive patients demonstrated a high prevalence of triple mixed infection (4%). The most common triple mixed infection of Plasmodium species was P. falciparum, P. malariae, and P. vivax (59%). This finding agreed with those of previous studies in Papua New Guinea [11,12,13,14], India [18], Cambodia [15,16,17], and Thailand [24], but contradicts the findings of previous studies which included P. ovale in triple mixed infection in the Laos-Vietnam border (P. falciparum/P. vivax/P. knowlesi) [28], China (P. falciparum/P. vivax/P. ovale) [26], Thailand (P. falciparum/P. vivax/P. ovale) [25], and Zambia (P. falciparum/P. malariae/P. ovale) [29].
The mechanisms underlying the triple mixed parasitic infection are unknown; however, the course of an infection might be influenced by the simultaneous occurrence of several Plasmodium species [30, 31]. Another explanation is the immunosuppressive effects caused by chronic P. falciparum infection and differences in individual exposure [32]. Whether the simultaneous infections might be beneficial or adds further detriment to the infected individual is not well defined. Triple mixed infection may be caused by cross immunity-induced susceptibility to three infections or exposure to infective bites of a single vector that can transmit three Plasmodium species [33]. A previous study indicated that infection with one Plasmodium species increased susceptibility to infection by other Plasmodium species [34]. The apparent frequency of mixed infection is dependent on the technique used for parasite analyses. The results demonstrated a high proportion of triple mixed infection compared with double mixed infection only in studies using PCR analysis to detect the malaria parasite due to the high sensitivity and specificity of PCR compared with microscopy or RDTs. In areas where more than one Plasmodium species is present and transmission is stable, the adult populations often have parasite densities below the level of microscopic detection and called “submicroscopic infections”. These submicroscopic infections demonstrated more than one Plasmodium species.
The subgroup analysis demonstrated that the proportion of triple mixed infection was higher in residents than in febrile patients, indicating that residents in communities where malaria is endemic were exposed to malaria several times or to more than one species at a time [35]. These triple mixed infection were submicroscopic infection for which microscopy has insufficient sensitivity for their detection. It is well-documented that malaria patients in endemic areas develop immunity against malaria, resulting in symptom relief [35, 36]. A previous study demonstrated that age, geographical origin, and clinical manifestations were found to be associated with triple mixed infection [5]. The subgroup analysis of age ranges demonstrated that the proportion of triple mixed infection was significantly lower across a wide age range of ages compared to double mixed infection. Subgroup analysis demonstrated that no statistical difference in age groups and types of mixed infection. This result suggested that triple mixed infection can occur in both patients aged ≤ 5 years and > 5 years. However, a limited number of articles have reported on age and susceptibility to triple mixed infection. The included study by Camargo-Ayala et al. showed that patients tend to have a risk of triple mixed infection at an age range of 18–60 years than at ≤ 5 or 5–18 years, whereas patients tend to have a risk of double infection at age range greater than 60 years than at ≤ 5, 5–18 and 18–60 years [5]. However, small sample sizes of the triple and dual mixed infection were calculated for the risk estimate in the same study. Therefore, the association between age and different types of mixed infection (double and triple infection) should be analysed in further observational studies using the research gap in age and type of mixed infection.
The study demonstrated that vomiting and the intense brown colour of urine were associated with triple mixed infection. Regarding the geographical region analysed, triple mixed infection was mostly found at the Loretoyacu River in the Colombian Amazon region [5]. The high prevalence of triple mixed infection at the Loretoyacu River may be due to the occurrence of the mosquito Anopheles maculatus, which can serve as a single vector for P. falciparum/P. vivax/P. malariae [5]. Triple species infection of P. falciparum and P. malariae, followed by P. ovale delayed infection, were also observed in two adopted children from the Central African Republic and may be attributed to late therapeutic failure or the relatively insufficient dosage due to increased oral clearance of atovaquone in paediatric patients [37].
The subgroup analysis demonstrated that the proportion of triple mixed infection was the highest in Oceania (23%) and Europe (21%) but the lowest in America. A previous study indicated that, in Oceania, where intense transmission occurs in very small focal forests or forest fringe areas, mixed infection are common but require submicroscopic detection [9]. Malaria disease in Europe has been mostly eradicated, but the increase in the number of imported malaria due to tourism, as well as population migration, resulted in increased mortality, from 3.8 to 20% [38]. These imported cases have increased the number of malaria cases in places where its transmission was low or previously eradicated, such as in Europe [39].
Knowledge about mixed infection is important not only to develop appropriate control measures but also for therapeutic options. For example, if P. vivax infection is suppressed by mixed infection with P. falciparum, effective control of P. falciparum infection in an area will activate P. vivax transmission in the community, a condition that is more difficult to control [17]. The present study was limited by the heterogeneity of the included studies and should be interpreted cautiously. Thus, the findings of the present study might not necessarily apply to all co-endemic regions. The present study could not extract the age of patients with triple mixed infection due to the lack of data reported in the included studies. Moreover, the clinical data, laboratory data, and treatment data of individual patients with triple mixed infection were also unavailable to extract. These data should be included and declared in malaria studies for its apparent value in cases of review and meta-analyses. Future meta-analyses should assess the cases reported or case series to provide a greater understanding of the factors associated with triple mixed infection.
Conclusion
In summary, although mixed infection was recognized, the prevalence of triple mixed infection was high (4%). The proportion of triple mixed infection was the highest in Oceania and Europe but lower in America. Compared with the proportion of double mixed infection, triple mixed infection was higher in residents (20%) than in febrile patients (7%). The findings suggested that in some regions, co-endemic for triple mixed infection, PCR, or molecular diagnosis for all residents in communities where malaria is endemic can provide prevalence data and intervention measures, as well as prevent disease transmissions and enhance malaria elimination efforts.
Availability of data and materials
The datasets used during the current study are available without restriction.
Abbreviations
- CI:
-
Confidence interval
- DNA:
-
Deoxyribonucleic acid
- NOS:
-
Newcastle–Ottawa Scale
- OR:
-
Odds ratio
- PCR:
-
Polymerase chain reaction
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- RDT:
-
Rapid diagnostic test
- WHO:
-
World Health Organization
References
Malaria. https://www.who.int/news-room/fact-sheets/detail/malaria. Accessed 1 March 2020.
Asua V, Tukwasibwe S, Conrad M, Walakira A, Nankabirwa JI, Mugenyi L, et al. Plasmodium species infecting children presenting with malaria in Uganda. Am J Trop Med Hyg. 2017;97:753–7.
Barber BE, William T, Dhararaj P, Anderios F, Grigg MJ, Yeo TW, et al. Epidemiology of Plasmodium knowlesi malaria in north-east Sabah, Malaysia: family clusters and wide age distribution. Malar J. 2012;11:401.
Calderaro A, Gorrini C, Peruzzi S, Piccolo G, Dettori G, Chezzi C. An 8-year survey on the occurrence of imported malaria in a nonendemic area by microscopy and molecular assays. Diagn Microbiol Infect Dis. 2008;61:434–9.
Camargo-Ayala PA, Cubides JR, Niño CH, Camargo M, Rodríguez-Celis CA, Quiñones T, et al. High Plasmodium malariae prevalence in an endemic area of the colombian amazon region. PLoS ONE. 2016;11:e0159968.
Dhangadamajhi G, Kar SK, Ranjit MR. High prevalence and gender bias in distribution of Plasmodium malariae infection in central east-coast India. Trop Biomed. 2009;26:326–33.
May J, Falusi AG, Mockenhaupt FP, Ademowo OG, Olumese PE, Bienzle U, et al. Impact of subpatent multi-species and multi-clonal plasmodial infections on anaemia in children from Nigeria. Trans R Soc Trop Med Hyg. 2000;94:399–403.
Mbakilwa H, Manga C, Kibona S, Mtei F, Meta J, Shoo A, et al. Quality of malaria microscopy in 12 district hospital laboratories in Tanzania. Pathog Glob Health. 2012;106:330–4.
Mayxay M, Pukrittayakamee S, Newton PN, White NJ. Mixed-species malaria infections in humans. Trends Parasitol. 2004;20:233–40.
Malaria in children under five. https://www.who.int/malaria/areas/high_risk_groups/children/en/. Accessed 2 March 2020.
Kasehagen LJ, Mueller I, McNamara DT, Bockarie MJ, Kiniboro B, Rare L, et al. Changing patterns of Plasmodium blood-stage infections in the Wosera region of Papua New Guinea monitored by light microscopy and high throughput PCR diagnosis. Am J Trop Med Hyg. 2006;75:588–96.
Mehlotra RK, Lorry K, Kastens W, Miller SM, Alpers MP, Bockarie M, et al. Random distribution of mixed species malaria infections in Papua New Guinea. Am J Trop Med Hyg. 2000;62:225–31.
Mehlotra RK, Kasehagen LJ, Baisor M, Lorry K, Kazura JW, Bockarie MJ, et al. Malaria infections are randomly distributed in diverse holoendemic areas of Papua New Guinea. Am J Trop Med Hyg. 2002;67:555–62.
Mueller I, Widmer S, Michel D, Maraga S, McNamara DT, Kiniboro B, et al. High sensitivity detection of Plasmodium species reveals positive correlations between infections of different species, shifts in age distribution and reduced local variation in Papua New Guinea. Malar J. 2009;8:41.
Sluydts V, Heng S, Coosemans M, Van Roey K, Gryseels C, Canier L, et al. Spatial clustering and risk factors of malaria infections in Ratanakiri Province. Cambodia. Malar J. 2014;13:387.
Steenkeste N, Incardona S, Chy S, Duval L, Ekala MT, Lim P, et al. Towards high-throughput molecular detection of Plasmodium: new approaches and molecular markers. Malar J. 2009;8:12.
Steenkeste N, Rogers WO, Okell L, Jeanne I, Incardona S, Duval L, et al. Sub-microscopic malaria cases and mixed malaria infection in a remote area of high malaria endemicity in Rattanakiri province, Cambodia: implication for malaria elimination. Malar J. 2010;9:11.
Krishna S, Yadav A, Bhandari S, Vishwakarma AK, Bharti PK, Mandavi PL, et al. Prevalence of malaria in two highly endemic Community Health Centers in the Bastar district, Chhattisgarh showing mixed infections with Plasmodium species. Sci Rep. 2017;7:16860.
Pati P, Rana RK, Khuntia HK, Bal MS, Ranjit MR. The prevalence of P. malariae in Odisha, India. Trop Biomed. 2017;34:607-14.
Perandin F, Manca N, Calderaro A, Piccolo G, Galati L, Ricci L, et al. Development of a real-time PCR assay for detection of Plasmodium falciparum, Plasmodium vivax, and Plasmodium ovale for routine clinical diagnosis. J Clin Microbiol. 2004;42:1214–9.
Peruzzi S, Gorrini C, Piccolo G, Calderaro A, Dettori G, Chezzi C. Prevalence of imported malaria in Parma during 2005-2006. Acta Biomed Ateneo Parmense. 2007;78:170–5.
Hopkins H, Gonzalez IJ, Polley SD, Angutoko P, Ategeka J, Asiimwe C, et al. Highly sensitive detection of malaria parasitemia in a malaria-endemic setting: performance of a new loop-mediated isothermal amplification kit in a remote clinic in Uganda. J Infect Dis. 2013;208:645–52.
Subissi L, Kanoi BN, Balikagala B, Egwang TG, Oguike M, Verra F, et al. Plasmodium malariae and Plasmodium ovale infections and their association with common red blood cell polymorphisms in a highly endemic area of Uganda. Trans R Soc Trop Med Hyg. 2019;113:370–8.
Zhou M, Liu Q, Wongsrichanalai C, Suwonkerd W, Panart K, Prajakwong S, et al. High prevalence of Plasmodium malariae and Plasmodium ovale in malaria patients along the Thai-Myanmar border, as revealed by acridine orange staining and PCR-based diagnoses. Trop Med Int Health. 1998;3:304–12.
Putaporntip C, Hongsrimuang T, Seethamchai S, Kobasa T, Limkittikul K, Cui L, et al. Differential prevalence of Plasmodium infections and cryptic Plasmodium knowlesi malaria in humans in Thailand. J Infect Dis. 2009;199:1143–50.
Zhou X, Huang JL, Njuabe MT, Li SG, Chen JH, Zhou XN. A molecular survey of febrile cases in malaria-endemic areas along China-Myanmar border in Yunnan province. People’s Republic of China. Parasite. 2014;21:7.
Toma H, Kobayashi J, Vannachone B, Arakawa T, Sato Y, Nambanya S, et al. A field study on malaria prevalence in southeastern Laos by polymerase chain reaction assay. Am J Trop Med Hyg. 2001;64:257–61.
Pongvongsa T, Culleton R, Ha H, Thanh L, Phongmany P, Marchand RP, et al. Human infection with Plasmodium knowlesi on the Laos-Vietnam border 11 Medical and Health Sciences 1108 Medical Microbiology. Trop Med Health. 2018;46:33.
Sitali L, Chipeta J, Miller JM, Moonga HB, Kumar N, Moss WJ, et al. Patterns of mixed Plasmodium species infections among children six years and under in selected malaria hyper-endemic communities of Zambia: population-based survey observations. BMC Infect Dis. 2015;15:6.
Yoeli M, Sklarsh J. The course of simultaneously inoculated, concomitant infections with Plasmodium vinckei and Plasmodium berghei in white mice. Trans R Soc Trop Med Hyg. 1970;64:271–5.
Snounou G, Bourne T, Jarra W, Viriyakosol S, Wood JC, Brown KN. Assessment of parasite population dynamics in mixed infections of rodent Plasmodia. Parasitology. 1992;105:363–74.
Butcher G. Cross-species immunity in malaria. Parasitol Today. 1998;14:166.
Collins WE, Jeffery GM. A retrospective examination of sporozoite-induced and trophozoite-induced infections with Plasmodium ovale: development of parasitologic and clinical immunity during primary infection. Am J Trop Med Hyg. 2002;66492-502.
de Arruda-Mayr M, Cochrane AH, Nussenzweig RS. Enhancement of a simian malarial infection (Plasmodium cynomolgi) in mosquitoes fed on rhesus (Macaca mulatta) previously infected with an unrelated malaria (Plasmodium knowlesi). Am J Trop Med Hyg. 1979;28:627–33.
Coura JR, Suarez-Mutis M, Ladeia-Andrade S. A new challenge for malaria control in Brazil: asymptomatic Plasmodium infection–a review. Mem Inst Oswaldo Cruz. 2006;101:229–37.
Alves FP, Durlacher RR, Menezes MJ, Krieger H, Silva LH, Camargo EP. High prevalence of asymptomatic Plasmodium vivax and Plasmodium falciparum infections in native Amazonian populations. Am J Trop Med Hyg. 2002;66:641–8.
Bichara C, Flahaut P, Costa D, Bienvenu AL, Picot S, Gargala G. Cryptic Plasmodium ovale concurrent with mixed Plasmodium falciparum and Plasmodium malariae infection in two children from Central African Republic. Malar J. 2017;16:339.
Rubio JM, Benito A, Berzosa PJ, Roche J, Puente S, Subirats M, et al. Usefulness of seminested multiplex PCR in surveillance of imported malaria in Spain. J Clin Microbiol. 1999;37:3260–4.
Rubio JM, Benito A, Roche J, Berzosa PJ, García ML, Micó M, et al. Semi-nested, multiplex polymerase chain reaction for detection of human malaria parasites and evidence of Plasmodium vivax infection in Equatorial Guinea. Am J Trop Med Hyg. 1999;60:183–7.
Dormond L, Jaton-Ogay K, de Valliere S, Genton B, Bille J, Greub G. Multiplex real-time PCR for the diagnosis of malaria: correlation with microscopy. Clin Microbiol Infect. 2011;17:469–75.
Fuehrer HP, Starzengruber P, Swoboda P, Khan WA, Matt J, Ley B, et al. Indigenous Plasmodium ovale malaria in Bangladesh. Am J Trop Med Hyg. 2010;83:75–8.
Gabrielli S, Bellina L, Milardi GL, Katende BK, Totino V, Fullin V, et al. Malaria in children of Tshimbulu (Western Kasai, Democratic Republic of the Congo): epidemiological data and accuracy of diagnostic assays applied in a limited resource setting. Malar J. 2016;15:81.
Jiang N, Chang Q, Sun X, Lu H, Yin J, Zhang Z, et al. Co-infections with Plasmodium knowlesi and other malaria parasites, Myanmar. Emerg Infect Dis. 2010;16:1476–8.
Lorenzetti A, Fornazari PA, Bonini-Domingos AC, de Souza Rodrigues Penhalbel R, Fugikaha E, Bonini-Domingos CR, et al. Mixed Plasmodium falciparum infections and its clinical implications in four areas of the Brazilian Amazon region. Acta Trop. 2008;107:8–12.
Marques PX, Saute F, Pinto VV, Cardoso S, Pinto J, Alonso PL, et al. Plasmodium species mixed infections in two areas of Manhica district, Mozambique. Int J Biol Sci. 2005;1:96–102.
Nino CH, Cubides JR, Camargo-Ayala PA, Rodriguez-Celis CA, Quinones T, Cortes-Castillo MT, et al. Plasmodium malariae in the Colombian Amazon region: you don't diagnose what you don't suspect. Malar J. 2016;15(1):576.
Woldearegai TG, Lalremruata A, Nguyen TT, Gmeiner M, Veletzky L, Tazemda-Kuitsouc GB, et al. Characterization of Plasmodium infections among inhabitants of rural areas in Gabon. Sci Rep. 2019;9(1):9784.
May J, Mockenhaupt FP, Ademowo OG, Falusi AG, Olumese PE, Bienzle U, et al. High rate of mixed and subpatent malarial infections in southwest Nigeria. Am J Trop Med Hyg. 1999;61:339–43.
Acknowledgements
The authors would like to acknowledge all of the published research that contributed to the data used in this study.
Funding
This research was partially supported by the new strategic research (P2P) project, Walailak University, Thailand. The funders had a role in the collection, analysis, and interpretation of the data.
Author information
Authors and Affiliations
Contributions
MK and KUK participated in the study design, data analysis, and writing of the paper. GDM and FRM participated in the writing of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest regarding the publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Table S1.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kotepui, M., Kotepui, K.U., Milanez, G.D. et al. Prevalence and proportion of Plasmodium spp. triple mixed infections compared with double mixed infections: a systematic review and meta-analysis. Malar J 19, 224 (2020). https://doi.org/10.1186/s12936-020-03292-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-020-03292-8