
Abstract
Background
Malaria rapid diagnostic tests based on histidine-rich protein-2 have played a vital role in improving malaria case management and surveillance particularly in Africa, where Plasmodium falciparum is predominant. However, their usefulness has been threatened by the emergence of gene deletion on P. falciparum histidine rich protein 2 (pfhrp2) and P. falciparum histidine rich protein 3 (pfhrp3). Use of standard and recommended methods is key for accurate investigation, confirmation and reporting of pfhrp2 and pfhrp3 gene deletion.
Methods
A systematic review was conducted to assess the status, methods and approaches that have been used for investigation, confirmation and reporting of pfhrp2 and pfhrp3 gene deletion in Africa. An online search was done using PubMed and MEDLINE Google Scholar for all articles published in English on pfhrp2/3 gene deletion in Africa. Relevant articles that met the inclusion criteria were summarized and assessed based on the protocol recommended by the World Health Organization for confirmation and reporting of pfhrp2/3 gene deletion.
Results
The search identified a total of 18 articles out of which 14 (77.7%) fulfilled the criteria for inclusion and were retained for review. The articles were distributed across 12 countries where the pfhrp2 and pfhrp3 gene deletion studies were conducted and reported. The level of pfhrp2/3 gene deletion across selected studies in Africa ranged from the highest 62% to the lowest 0.4%. There was wide variation in methods and approaches including study designs, size and sampling and whether both pfhrp2 and pfhrp3 double deletions or pfhrp2 single deletion were investigated, with a wide variation in laboratory methods.
Conclusion
Based on the review, there is evidence of the presence of pfhrp2/3 gene-deleted P. falciparum parasites in Africa. The approaches and methods used for investigation, confirmation and reporting of pfhrp2/3 deleted parasites have varied between studies and across countries. Countries that are considering plans to investigate, confirm and report pfhrp2/3 deletion should use recommended standard and harmonized methods to prevent unnecessary recommendations for costly switch of RDTs in Africa.
Similar content being viewed by others


Background
The World Health Organization (WHO) estimated that there were 219 million cases of malaria and 435,000 malaria deaths and nearly half of the world’s population was at risk of malaria infection in 2017 [1, 2]. The WHO African Region continues to carry a disproportionately high share of the global malaria burden contributing 92% (200 million) malaria cases and 91% of malaria deaths. Plasmodium falciparum is the most prevalent malaria species in the WHO African region, accounting for 99.7% of estimated malaria cases in 2017 [1, 2].
Efforts to reduce the burden of malaria in Africa have mostly included the use of long-lasting insecticide-treated nets (LLINs), indoor residual spraying (IRS) with insecticides, intermittent preventive therapy (IPT), diagnosis and treatment. Case management which involves testing and treatment with artemisinin-based combination therapy (ACT) is a major intervention for malaria control [1, 2]. The WHO recommends parasitological confirmation of malaria in all suspected cases prior to treatment with ACT. Nearly all countries in Africa adopted this as policy and have shifted from clinical to parasite-based diagnosis with microscopy or rapid diagnostic tests (RDTs) [1,2,3]. Due to systemic challenges associated with blood smear microscopy, RDTs are becoming increasingly the most used method to test for malaria among suspected malaria patients in sub-Saharan Africa [1, 2]. In 2017 alone, an estimated 75% of malaria tests were conducted using RDTs, up from 40% in 2010 and an estimated 276 million rapid diagnostic tests (RDTs) were sold globally [1, 2]. Due to the dominance of P. falciparum, over 90% of RDTs used for the diagnosis of malaria in sub-Saharan Africa are HRP2-based [1, 2]. Plasmodium falciparum specific RDTs specifically recognize HRP2 antigen that encodes for the pfhrp2 gene and whose antibodies cross-react with histidine-rich protein 3 (pfhrp3) antibodies due to high degree of similarity in amino acid sequence [3,4,5]. However, recent publications have indicated that a substantial number of malaria parasites in the Amazon region and some parts of Africa and Asia are lacking the pfhrp2 and pfhrp3 genes. Plasmodium falciparum parasites lacking the pfhrp2/3 gene do not express HRP2 protein antigen threatening the usefulness of HRP2 RDTs in malaria diagnosis [3, 4, 6]. The first P. falciparum parasites with pfhrp2 and pfhrp3 gene deletions were reported in the Amazon basin in 2010 by Gamboa et al. [4]. However recent evaluations of malaria parasites revealed the presence of pfhrp2/3 gene deletions outside the Amazon region in Africa and India [6]. The occurrence of P. falciparum with missing pfhrp2/3 genes pose a public health threat as a large number of malaria infected patients will go undetected by the HRP2 RDTs and, therefore, remain untreated leading to increased risk of malaria morbidity and mortality, and continued malaria transmission [3, 5, 6].
The WHO recommends a policy switch to more effective alternative non-HRP2 RDTs, when the prevalence of pfhrp2-deleted parasites meets or exceeds the lower 90% confidence interval for 5% prevalence, or a plan for change over a longer time frame if deletions are present but < 5% [7]. In Africa, a number of studies have reported occurrence of pfhrp2 and pfhrp3 gene deletions [8,9,10,11,12,13,14,15,16,17,18]. Due to the high prevalence of pfhrp2/3 gene deletion, countries, such as Eritrea have introduced non-HRP2 alternative RDTs that are able to detect gene-deleted parasites [11]. However, the costs and resources associated with the switch of national malaria diagnostic strategies from HRP2 to alternative non-HRP2 based RDTs are enormous. In addition to the costs associated with training, non-HRP2 based RDTs have poor field stability and sensitivity compared to HRP2 based RDTs [3, 6]. The threat becomes real in view of the big volumes of HRP2 RDTs required for P. falciparum parasite confirmation in Africa and the limited options available of WHO approved non-HRP malaria RDTs [2, 3, 6, 7]. It is, therefore important that decisions to change pfhrp2 RDTs are based on quality data generated from well conducted studies using recommended methods to avoid unnecessary costly switch of RDTs [6]. However, the designs and methodologies used to investigate, confirm and report pfhrp2/3 gene deletion studies in Africa have varied. There have been variations in; (1) the size of the studies, (2) source of participants used (health facility versus survey data), (3) clinical classifications of the participants including symptomatic versus asymptomatic individuals, and (4) investigation of pfhrp2 deletion alone versus pfhrp2 and pfhrp3 double deletions and flanking genes and (5) the laboratory methods.
Due to this variability in study designs, methodologies and reporting, the WHO Global Malaria Programme published a standard protocol on the recommended approaches and methods required for investigation, confirmation and reporting of pfhrp2 and pfhrp3 gene deletion [7]. This review aims to assess the current status of pfhrp2 gene deletion and the methods and approaches being used for its estimation, confirmation and reporting in Africa.
Methods
Review question
The review aimed to (1) assess the status of pfhrp2 gene deletion in P. falciparum parasites in Africa since 2010 when the first deleted parasites were identified in clinical samples in the Amazon region, (2) assess the methodologies and approaches being used for pfhrp2/3 gene deletion estimation, confirmation and reporting in Africa.
Search strategy
A systematic search of literature was conducted electronically for published studies on pfhrp2/3 gene deletion in Africa between January 2010 and June 2019. Literature search was done using PubMed and MEDLINE google Scholar for all articles published in English about pfhrp2/3 gene deletion in Africa. The following were used as search words; ‘Malaria’, ‘Plasmodium falciparum’, ‘pfhrp2’, ‘pfhrp3’ ‘Gene deletion’, ‘Malaria Rapid diagnostic tests’, ‘Africa’. All searches were restricted to paper titles and abstracts.
Review period and selection criteria of articles
The review considered the period from January 2010, when Gamboa et al. first reported the occurrence of pfhrp2/3 gene deletion in clinical samples in Peru until June 2019 [4]. The articles were selected based on the following selection criteria: (1) Original publication, (2) containing primary data on pfhrp2 deletion, (3) conducted in Africa, and (4) published during the selected review period. In order to expand on the scope, the papers referenced or cited in the selected papers were also reviewed for additional evidence. The WHO recommended protocol for investigation, confirmation and reporting of pfhrp2/3 gene deletion (Table 1) was used to assess the designs, approaches and methodologies used in the selected relevant articles [7].
The status of gene deletion reported and the methods used for its investigations in every searched article were assessed and summarized based on the WHO protocol recommendation for investigation and confirmation of pfhrp2 and pfhrp3 gene deletions in P. falciparum. Searched material was excluded from the review if they were responses or correspondences to the editor, if they were conference presentations, if year of data collection was outside the review period and where retrieve full text for review was not possible.
In order to standardize methods for estimation and reporting of pfhrp2/3 gene deletion, the WHO Global Malaria Programme developed and published a pfhrp2/pfhrp3 gene deletion protocol [7].
The aim of the protocol is to provide guidance to countries on the recommended standard and harmonized methods required for confirmation and reporting of suspected pfhrp2/3 gene deletions in P. falciparum. In this systematic review, published papers were assessed against the WHO standard criteria (Table 1).
Results
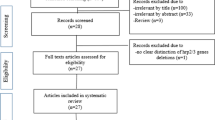
The review considered published articles on pfhrp2/3 gene deletion in Africa between Jan 2010 and June 2019 that satisfied our inclusion criteria. The initial search yielded 18 articles however only 14 (77.7%) fulfilled the criteria for inclusion and were retained for review (Fig. 1).

Categorization of the published articles identified in the search that fulfilled the criteria
The summary of findings from the reviewed articles on P. falciparum pfhrp2 gene deletion based on the WHO recommended methods for confirmation and reporting of pfhrp2 and pfhrp3 gene deletions is shown in Table 2. The distribution of reviewed studies of pfhrp2/3 gene deletion across Africa is shown in Fig. 2.

Distribution of reviewed pfhrp2/3 gene deletion studies across Africa
Discussion
The status, methods and approaches that have been used for confirmation and reporting of pfhrp2/3 gene deletions in Africa were assessed and reviewed where studies were conducted and reported between 2010 and June 2019. There was wide variation in methods and approaches used across studies (Table 2), as compared to those recommended in the WHO standard protocol for confirmation and reporting of pfhrp2 gene deletions (Table 1). Studies varied from the designs, size and sampling, whether they assessed both pfhrp2 and pfhrp3 double deletions or pfhrp2 single deletion alone with wide variation in laboratory methods.
Summary of results of studies on pfhrp2 gene deletion
A total of 14 research articles satisfied our criteria for inclusion in the review (Table 2). These articles provide unequivocal evidence of the existence and occurrence of pfhrp2 and pfhrp3 gene deletion in Africa where P. falciparum is the predominant parasite and where huge volumes of HRP2 based RDTs are used for malaria diagnosis [8,9,10,11,12,13,14,15,16,17,18]. Based on the articles included under this review, the current levels of pfhrp2/3 gene deletion across malaria endemic countries in Africa range from the highest 62% in Eritrea to the lowest 1.45% and 0.4% in Mozambique and Angola, respectively [11, 12, 20]. However, levels of gene deletions were as high as 80% at some hospitals in Eritrea [11]. Gene deletions were not detected in one of the studies in Kenya [16]. The observed differences in the levels of pfhrp2/3gene deletion in these studies could be due to selection pressure caused by exclusive use of HRP2 RDTs over time as suggested in previous studies [6, 11]. In Eritrea, HRP2-based RDTs had been widely used exclusively since 2006 and that provided ideal conditions for selection and spontaneous occurrence of pfhrp2/3 negative parasites that remained undetected and continued to increase [11]. This selection pressure and spontaneous occurrence of gene-deleted parasites has been predicted by recent mathematical modelling, that showed that exclusive use of HRP2-based RDTs exerts strong selection pressure for pfhrp2/3-negative parasite populations leading to their increase in frequency [22]. Low malaria transmission setting in Eritrea could have also contributed to selection of pfhrp2/3-negative parasites once they emerge [6, 11]. The extremely low prevalence of pfhrp2/3 deleted parasites reported by studies in Western Kenya and Southern Mozambique may be due to the absence of these ideal conditions for pfhrp2 selective pressure, such as are high transmission settings and use of malaria microscopy as the major diagnostic tool [12, 16]. Due to the high levels of pfhrp2/3 gene deletions above the 5% recommended WHO cut-off, Eritrea has introduced non-HRP2 RDTs to detect pfhrp2 and pfhrp3 deleted parasites [11].
Limitations of the studies and how they affect the results
There was wide variation in the approaches and methods used for investigation, confirmation and reporting of pfhrp2 and pfhrp3 gene deletion across all studies. The major differences and limitations in methods and approaches across the studies are highlighted below.
Study designs and participants
All the reviewed studies but one used a cross-sectional design as recommended by the WHO protocol for confirmation and reporting pfhrp2 and pfhrp3 gene deletion [8,9,10,11,12,13,14,15,16,17,18]. The WHO protocol recommends recruitment and enrolment of febrile symptomatic participants seeking treatment at health facility into pfhrp2 and pfhrp3 deletion studies [7]. The reason for preference of symptomatic to asymptomatic population for pfhrp2/3 gene deletion studies is because parasite density is generally higher in the former compared to the low-density infections in the latter and hence provide better quality samples for confirmation of gene deletions by molecular tests [6, 7]. However, a number of studies included in the current review collected and investigated samples from asymptomatic individuals for pfhrp2/3 gene deletion investigation including blood donors in Mali [9]. The DRC, Ethiopia and Mozambique studies estimated gene deletion in samples collected from Demographic Health Survey (DHS) and population-based surveys in asymptomatic individuals reporting the levels of pfhrp2 gene deletions as 6.4%, 4.8% and 1.45%, respectively [12, 16, 21]. These levels of deletions are relatively lower compared to the Eritrea and the Rwanda studies that recruited febrile symptomatic individuals and reported very high levels of pfhrp2 gene deletions up to 62% and 23%, respectively [8, 11]. The WHO standard protocol recommends symptomatic individuals as the preferred study participants for pfhrp2/3 gene deletion studies. The Mali study however gives contrary findings and reports a significant association between asymptomatic population and pfhrp2/3 gene deletion [9]. These variations in methodologies call for standardization of methods, approaches and reporting of pfhrp2/3 gene deletion studies across malaria endemic countries in Africa as the use of appropriate study participants is fundamental for the gene deletion study outcomes.
Size of the studies
The WHO protocol for investigation of pfhrp2/3 deletion recommends the recruitment of a minimum of 370 or 318 symptomatic individuals with suspected P. falciparum infection to estimate a prevalence of 3.2% and 8.0%, respectively per sampling region or province [7]. However, the articles included under this review showed wide variation in size with regard to number of participants recruited. In some cases, extremely low sample sizes were used such as the Eritrean study that enrolled a total sample of 51 individuals to report a pfhrp2 gene deletion of > 80% at one of the study hospitals [11]. The Zambian study reported a gene deletion of up to 10.7% (3/28) based on a total of 28 P. falciparum DNA samples [19]. Based on the WHO protocol, even when the recommended sample is used, it should be distributed and spread across all regions to provide a representation of a country’s malaria epidemiology and P. falciparum population [7]. However, these criteria on sample size and its distribution across different malaria epidemiological setting were not complied with in a number of articles reviewed. The effect and challenges associated with the use of inadequate sample size on study outcomes in prevalence studies are widely published [23, 24]. Non-uniformity and non-compliance to the recommended methods may pose challenges in reporting and comparability of findings on pfhrp2/3 gene deletion across countries.
Reporting of pfhrp2 and pfhrp3 double deletion versus pfhrp2 single deletion alone: The WHO protocol for pfhrp2/3 studies recommends estimation and reporting of both pfhrp2 and pfhrp3 in P. falciparum gene deletion studies [3, 6, 7]. This is because P. falciparum-based RDTs are designed to specifically recognize HRP2 antigen, however pfhrp2 and pfhrp3 are homologous genes whose antigens may cross-react due to high degree of similarity in their amino acid sequence [5, 25, 26]. A number of studies elsewhere have reported a possible association between pfhrp2 and pfhrp3 gene deletions warranting investigation of both genes. Evidence from the Eritrean study showed that every sample that was pfhrp2 deleted was also pfhrp3 deleted suggesting a possible association [11]. However, the studies considered under this review exhibited variation in approaches with some investigating and reporting pfhrp2 and pfhrp3 double deletion while others reported pfhrp2 deletion alone. Gene deletions studies in Ghana, Mali and Rwanda investigated and reported single pfhrp2 deletion alone [8, 9, 17], while those conducted in DRC, Mozambique, Kenya, Eritrea and Nigeria investigated and reported pfhrp2 and pfhrp3 double deletions [11,12,13,14,15,16, 18]. The effect of investigating single pfhrp2 gene deletion alone is a possible underestimation as some of the samples may test positive with HRP2 RDT even when parasites are pfhrp2 deleted due to cross-reactivity with HRP3 antibodies. These observations and variations in methods call for harmonization and standardization of investigative and reporting approaches for pfhrp2/3 gene deletions.
Laboratory methods
The recommended laboratory-based testing methods required for confirmation of suspected pfhrp2/3 gene deletion in P. falciparum parasites have been previously published [4, 6, 25,26,27,28,29,30,31,32,33,34,35]. At the minimum, the suspected sample for pfhrp2/3 deletion should be negative by HRP2 based RDT and positive with expert microscopy or Pf-pLDH RDT [6, 33, 35]. From a suspected deleted sample, a dried blood spot is collected for PCR to confirm P. falciparum mono-infection and exclude other non-P. falciparum species. Samples that are PCR confirmed as P. falciparum are amplified in the exon1 and exon 2 regions of the pfhrp2/3 gene to detect the presence or absence of the gene [25, 33,34,35]. Samples that fail to amplify pfhrp2 or pfhrp3 in the exon region are considered pfhrp2 and pfhrp3 deleted after ascertaining the quality of parasite DNA by amplification of MSP1 and MSP1 single copy genes [4, 6, 7]. However, not all articles considered under this review performed the minimum recommended laboratory testing required for confirmation of parasite gene deletion. The study in Ghana extracted and used blood sample left-overs from used RDT test cassettes for pfhrp2/3 gene deletion study as opposed to the use of dried blood spots as preferred samples [17]. The effect of using wrong samples on the final pfhrp2/3 gene deletion outcome is poorly understood. Four of the reviewed articles that reported pfhrp2 deletion in four countries missed an essential procedural requirement of demonstrating the quality of parasite DNA by PCR amplification of MSP1 and MSP2 single copy genes of P. falciparum [8, 14, 15, 17]. One study reported MSP1 alone and the reason for not amplifying MSP2 was not indicated [9]. Detailed laboratory methods for one of the articles could not be accessed [16]. Failure to demonstrate the presence of P. falciparum MSP1 and MSP1 single copy genes as an essential confirmation of P. falciparum DNA quality in suspected pfhrp2/3 deleted samples is a major methodological flaw that creates uncertainty on the validity and correctness of the reported deletion estimates [6, 7]. The investigation of deletions in flanking genes located upstream and downstream of pfhrp2/3 in the subtelomeric region is optional and not essential requirement for confirmation and reporting of P. falciparum parasite gene deletion [6, 7]. However whole genome sequencing studies have showed that deletion is not restricted in the pfhrp2 and pfhrp3 gene regions and can extend in the neighbouring flanking genes [6, 36]. Under the current review, all the articles except one did not investigate or report deletions in the flanking genes.
Spread and distribution of study sites
The WHO recommends the design of pfhrp2/3 surveys that aims to achieve representativeness of a country’s malaria parasites population across all epidemiological settings [7]. The importance of spreading the sample across the country to achieve geographical representation is emphasized in the Indian and DRC studies that showed a wide variation in frequency and occurrence of pfhrp2 and pfhrp3 gene deletion in parasites collected across the various states and provinces [15, 31]. However, under the current review, apart from one study that used a national representative sample of parasites collected under the Health Demographic Survey (DHS), the rest of the reported studies had relatively limited geographical coverage that may not be representative of the entire country’s P. falciparum parasites population [8,9,10,11,12,13,14, 16,17,18]. The direct effect of this methodological approach is the difficulty it presents in determining the correct estimate and extent of spread of parasite gene deletion that is representative of a country’s parasite population.
Denominators used for computation of pfhrp2 gene deletion estimates
Across all the reviewed studies, there were differences in the denominators used in the final computation of gene deletion estimates. While others used total P. falciparum infections as measured by microscopy, others used PCR confirmed or number of RDT-/microscopy + discordant samples that is a smaller denominator [8,9,10,11,12,13,14,15,16,17,18]. The use of these different denominators leads to different pfhrp2/3 gene deletion estimates with possible overestimation or underestimation. The WHO standard protocol recommends the use of total P. falciparum infections measured by microscopy the suitable denominator to avoid overestimation of gene deletion estimates [7]. However, this has limitations for erroneous inclusion of non-P. falciparum species and false positives that are misclassified by poor quality microscopy. This potentially inflates the denominator leading to under estimation of deletions [6, 12, 13].
Implications for future research and future perspectives
Our review found a wide variation in methodologies and approaches for investigation of pfhrp2/3 gene deletion across studies in malaria endemic countries in Africa. The direct implication of the use of non-Standardised and non-harmonized methods for confirmation and reporting of parasite gene deletion is the risk of unnecessary recommendations for a costly switch from HRP2 based RDTs to non-P. falciparum RDTs. Non-HRP2 RDTs are more expensive, less sensitive with poor field thermal stability [3, 6]. Unnecessary switch of current diagnostic strategies may potentially undermine the current gains and improvement in parasite-based diagnosis especially in Africa where P. falciparum is predominant and where large volumes of HRP2 based RDTs are used for malaria diagnosis [1, 2]. However, future research could consider establishment of the actual costs associated with the process of switching diagnostic tools and the public health benefit of deploying non-P. falciparum RDTs in the context of gene deletions.
Despite the high burden and dominance of P. falciparum, the search identified only 13 published articles on pfhrp2/3 gene deletion in Africa. This observation could explain the limited data available on the occurrence and status of pfhrp2/3 gene deletion in malaria endemic countries in Africa. The WHO recommends initiation of surveys and surveillance systems to allow early detection and containment of pfhrp2/3 gene-deleted parasites in countries at risk of this threat [3, 7]. Specifically the high risk countries are those located in regions where gene deletions have been confirmed, where there are concerns of false negative RDTs results and where discordance rate between microscopy and RDT is high [3, 7]. However, the direct implication for continued use of HRP2 RDTs in countries at risk without deliberate surveillance systems to allow early detection of gene-deleted parasites is a potential risk for selection pressure and continued spread of these parasites [3, 11, 37]. Even when there is initial confirmed presence of pfhrp2/3 gene deletion, the WHO recommends the need for periodic monitoring to assess if levels are increasing or exceeded the 5% prevalence cut-off required for change of diagnostic policies [7]. However, future research could consider generating additional evidence on the actual contribution of gene-deleted parasites to transmission, malaria morbidity and mortality if left to spread undetected.
Previous studies have demonstrated the possible occurrence and survival of pfhrp2 and pfhrp3 gene-deleted parasites in all malaria epidemiological setting including low and high transmission zones [9, 11, 15, 31]. However, the extent to which these undetected and unreported gene-deleted parasites affect surveillance and disease burden estimates is glaringly missing and remains subject of further research. From the review, there is evidence of the ability of pfhrp2/3 gene-deleted parasites to spread and cause disease [6, 9, 11]. However, their role and actual contribution in causing severe disease and deaths needs to be studied further. There are key questions on whether pfhrp2/3 deleted parasites are drug sensitive compared to gene harbouring parasites and whether current treatment is effective for pfhrp2/3 deleted parasites.
Studies have shown the failure of HRP2 based and the ability of non-HRP2 RDTs to detect pfhrp2/3 gene-deleted parasites in P. falciparum infected samples [6, 11, 12]. Indeed, the advance in the development of robust diagnostic tools to detect gene-deleted parasites is enormous [4, 21, 25, 32,33,34,35, 38, 39]. In addition to the current molecular and serological tools, Plucinski et al. have developed a bead-based multiplex assay that simultaneously detects parasite aldolase, parasite lactate dehydrogenase and histidine rich protein 2 increasing the possibility of detecting gene-deleted parasites [20]. However, false deletions due to unamplified pfhrp2/3 could still occur due to low quality parasite DNA particularly in low parasitaemia samples. Missed deletions could occur if an infection with a deleted parasite occurs subsequent to an infection with a wild type parasite, since circulating HRP2 can persist for up to a month [6]. In high transmission settings, such as many parts of Africa, polyclonal infection that involves host co-infection with two or more parasite strains is common. Co-infection may involve a non-deleted strain masking a gene-deleted strain that presents a challenge for the current diagnostic tools. This calls for future research into more robust diagnostic tools to detect masked gene-deleted parasites.
Conclusion
Based on the review, there is evidence of the presence of pfhrp2/3 gene-deleted P. falciparum parasites in Africa. The approaches and methods used for investigation, confirmation and reporting of pfhrp2/3 deleted parasites have varied between studies and across countries. The available evidence on the occurrence of pfhrp2/3 deletion comes from a limited number of countries leaving it largely unknown and unreported in many malaria endemic countries in Africa. Countries that are considering plans to confirm and report pfhrp2/3 deletion should use recommended standard and harmonized methods to prevent unnecessary recommendations for costly switch of RDTs in Africa.
Availability of data and materials
Not applicable.
Change history
10 February 2022
Following the original publication of this article, the name of author Bosco B. Agaba has been corrected: previously, the name had been miswritten as Agaba B. Bosco.
Abbreviations
- HRP2:
-
histidine rich protein 2
- pfhrp2 :
-
Plasmodium falciparum histidine rich protein 2
- RDTs:
-
rapid diagnostic tests
- ACT:
-
artemisinin-based combination therapy
- MSP1:
-
merozoite surface antigen 1
- MSP2:
-
merozoite surface antigen 2
- PCR:
-
polymerase chain reaction
- WHO:
-
World Health Organization
- ITNs:
-
insecticide-treated mosquito nets
- LLINs:
-
long-lasting insecticide-treated nets
- IRS:
-
indoor residual spraying
References
WHO. World Malaria Report. Geneva: World Health Organization; 2017. http://www.who.int/malaria/publications/world-malaria-report-2017/report/en/.
WHO. World malaria report. Geneva: World Health Organization; 2018.
WHO. Malaria Policy Advisory Committee Meeting, 14–16 September 2016, Background document for Session 7; P. falciparum hrp2/3 gene deletions, conclusions and recommendations of a technical consultation. Geneva: World Health Organization, 2016. http://www.who.int/malaria/mpac/mpac-sept2016-hrp2-consultation-short-report-session7.pdf.
Gamboa D, Ho MF, Bendezu J, Torres K, Chiodini PL, Barnwell JW, et al. A large proportion of P. falciparum isolates in the Amazon region of Peru lack pfhrp2 and pfhrp3: implications for malaria rapid diagnostic tests. PLoS One. 2010;5:e8091.
CDC, FIND, PAHO. Molecular surveillance for HRP2 and HRP3 gene expression in Plasmodium falciparum parasites from South and Central America. Centers for Disease Control and Prevention, P. falciparum pfhrp2 and pfhrp3 surveillance project. 2012.
Cheng Q, Gatton ML, Barnwell J, Chiodini P, McCarthy J, Bell D, et al. Plasmodium falciparum parasites lacking histidine-rich protein 2 and 3: a review and recommendations for accurate reporting. Malar J. 2014;13:283.
WHO. Protocol for estimating the prevalence of pfhrp2/pfhrp3gene deletions among symptomatic falciparum patients with false-negative RDT results. Geneva: World Health Organization; 2018.
Kozycki CT, Umulisa N, Rulisa S, Mwikarago EI, Musabyimana JP, Habimana JP, et al. False-negative malaria rapid diagnostic tests in Rwanda: impact of Plasmodium falciparum isolates lacking hrp2 and declining malaria transmission. Malar J. 2017;16:123.
Koita OA, Doumbo OK, Ouattara A, Tall LK, Konare A, Diakite M, et al. False-negative rapid diagnostic tests for malaria and deletion of the histidine-rich repeat region of the hrp2 gene. Am J Trop Med Hyg. 2012;86:194–8.
Menegon M, L’Episcopia M, Nurahmed AM, Talha AA, Nour BYM, Severini C. Identification of Plasmodium falciparum isolates lacking histidine-rich protein 2 and 3 in Eritrea. Infect Genet Evol. 2017;55:131–4.
Berhane A, Anderson K, Mihreteab S, Gresty K, Rogier E, Mohamed S, et al. Major threat to malaria control programs by Plasmodium falciparum lacking histidine-rich protein 2, Eritrea. Emerg Infect Dis. 2018;24:462–70.
Gupta H, Matambisso G, Galatas B, Cistero P, Nhamussua L, Simone W, et al. Molecular surveillance of pfhrp2 and pfhrp3 deletions in Plasmodium falciparum isolates from Mozambique. Malar J. 2017;16:416.
Funwei R, Nderu D, Nguetse CN, Thomas BN, Falade CO, Velavan TP, et al. Molecular surveillance of pfhrp2 and pfhrp3 genes deletion in Plasmodium falciparum isolates and the implications for rapid diagnostic tests in Nigeria. Acta Trop. 2019;196:121–5.
Wurtz N, Fall B, Bui K, Pascual A, Fall M, Camara C, et al. Pfhrp2 and pfhrp3 polymorphisms in Plasmodium falciparum isolates from Dakar, Senegal: impact on rapid malaria diagnostic tests. Malar J. 2013;12:34.
Parr JB, Vity R, Doctor SM, Janko M, Carey-Ewend K, et al. Pfhrp2-deleted Plasmodium falciparum parasites in the Democratic Republic of the Congo: a national cross-sectional survey. J Infect Dis. 2017;216:36–44.
Nderu D, Kimani F, Thiong’o K, Akinyi M, Karanja E, Meyer CG, et al. PfHRP2-PfHRP3 diversity among Kenyan isolates and comparative evaluation of PfHRP2/pLDH malaria RDT with microscopy and nested PCR methodologies. Parasitol Int. 2018;67:793–9.
Amoah LE, Abankwa J, Oppong A. Plasmodium falciparum histidine rich protein-2 diversity and the implications for PfHRP 2- based malaria rapid diagnostic tests in Ghana. Malar J. 2016;15:101.
Beshir KB, Sepulveda N, Bharmal J, Robinson A, Mwanguzi J, Busula AO, et al. Plasmodium falciparum parasites with histidine-rich protein 2 (pfhrp2) and pfhrp3 gene deletions in two endemic regions of Kenya. Sci Rep. 2017;7:14718.
Kobayashi T, Sikalima J, Parr JB, Chaponda M, Stevenson JC, Thuma PE, et al. Central Africa International Centers Of Excellence For Malaria R: the Search for Plasmodium falciparum histidine-rich protein 2/3 deletions in Zambia and implications for Plasmodium falciparum histidine-rich protein 2-based rapid diagnostic tests. Am J Trop Med Hyg. 2019;100:842–5.
Plucinski MM, Herman C, Jones S, Dimbu R, Fortes F, Ljolje D, et al. Screening for Pfhrp2/3-deleted Plasmodium falciparum, non-falciparum, and low-density malaria infections by a multiplex antigen assay. J Infect Dis. 2019;219:437–47.
Girma S, Cheaveau J, Mohon AN, Marasinghe D, Legese R, Balasingam N, et al. Prevalence and epidemiological characteristics of asymptomatic malaria based on ultrasensitive diagnostics: a cross-sectional study. Clin Infect Dis. 2019;69:1003–10.
Watson OJ, Slater HC, Verity R, Parr JB, Mwandagalirwa MK, Tshefu A, et al. Modelling the drivers of the spread of Plasmodium falciparum hrp2 gene deletions in sub-Saharan Africa. Elife. 2017;6:25008.
Noordzij M, Dekker FW, Zoccali C, Jager KJ. Sample size calculations. Nephron Clin Pract. 2011;118:c319–23.
Anderson SF, Kelley K, Maxwell SE. Sample-size planning for more accurate statistical power: a method adjusting sample effect sizes for publication bias and uncertainty. Psychol Sci. 2017;28:1547–62.
Baker J, McCarthy J, Gatton M, Kyle DE, Belizario V, Luchavez J, et al. Genetic diversity of Plasmodium falciparum histidine-rich protein 2 (PfHRP2) and its effect on the performance of PfHRP2-based rapid diagnostic tests. J Infect Dis. 2005;192:870–7.
Verma AK, Bharti PK, Das A. HRP-2 deletion: a hole in the ship of malaria elimination. Lancet Infect Dis. 2018;18:826–7.
Dorado EJ, Okoth SA, Montenegro LM, Diaz G, Barnwell JW, Udhayakumar V, et al. Genetic characterisation of Plasmodium falciparum isolates with deletion of the pfhrp2 and/or pfhrp3 genes in Colombia: the Amazon region, a challenge for malaria diagnosis and control. PLoS One. 2016;11:e0163137.
Kumar N, Pande V, Bhatt RM, Shah NK, Mishra N, Srivastava B, et al. Genetic deletion of HRP2 and HRP3 in Indian Plasmodium falciparum population and false negative malaria rapid diagnostic test. Acta Trop. 2013;125:119–21.
Pati P, Dhangadamajhi G, Bal M, Ranjit M. High proportions of pfhrp2 gene deletion and performance of HRP2-based rapid diagnostic test in Plasmodium falciparum field isolates of Odisha. Malar J. 2018;17:394.
Kinnaird JH, Maitland K, Walker GA, Wheatley I, Thompson FJ, Devaney E. HRP-2, a heterogeneous nuclear ribonucleoprotein, is essential for embryogenesis and oogenesis in Caenorhabditis elegans. Exp Cell Res. 2004;298:418–30.
Bharti PK, Chandel HS, Ahmad A, Krishna S, Udhayakumar V, Singh N. Prevalence of pfhrp2 and/or pfhrp3 gene deletion in Plasmodium falciparum population in eight highly endemic states in India. PLoS One. 2016;11:e0157949.
Palani B. Quantification of histidine-rich protein 3 of Plasmodium falciparum. Monoclon Antib Immunodiagn Immunother. 2018;37:87–90.
Rubio JM, Benito A, Roche J, Berzosa PJ, Garcia ML, Mico M. Semi-nested, multiplex polymerase chain reaction for detection of human malaria parasites and evidence of Plasmodium vivax infection in Equatorial Guinea. Am J Trop Med Hyg. 1999;60:183–7.
Parr JB, Anderson O, Juliano JJ, Meshnick SR. Streamlined, PCR-based testing for pfhrp2- and pfhrp3-negative Plasmodium falciparum. Malar J. 2018;17:137.
Padley D, Moody AH, Chiodini PL, Saldanha J. Use of a rapid, single-round, multiplex PCR to detect malarial parasites and identify the species present. Ann Trop Med Parasitol. 2003;97:131–7.
Sepulveda N, Phelan J, Diez-Benavente E, Campino S, Clark TG, Hopkins H, et al. Global analysis of Plasmodium falciparum histidine-rich protein-2 (pfhrp2) and pfhrp3 gene deletions using whole-genome sequencing data and meta-analysis. Infect Genet Evol. 2018;62:211–9.
Akinyi S, Hayden T, Gamboa D, Torres K, Bendezu J, Abdallah JF, et al. Multiple genetic origins of histidine-rich protein 2 gene deletion in Plasmodium falciparum parasites from Peru. Sci Rep. 2013;3:2797.
Jang IK, Das S, Barney RS, Peck RB, Rashid A, Proux S, et al. A new highly sensitive enzyme-linked immunosorbent assay for the detection of Plasmodium falciparum histidine-rich protein 2 in whole blood. Malar J. 2018;17:403.
Das S, Peck RB, Barney R, Jang IK, Kahn M, Zhu M, et al. Performance of an ultra-sensitive Plasmodium falciparum HRP2-based rapid diagnostic test with recombinant HRP2, culture parasites, and archived whole blood samples. Malar J. 2018;17:118.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
AB and MP independently conducted the article search and literature; AB conceived the original idea and drafted the manuscript; MK shaped the concept and positive criticism; AY, NS, JIN, JK, CSL, JO, MK reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Agaba, B.B., Yeka, A., Nsobya, S. et al. Systematic review of the status of pfhrp2 and pfhrp3 gene deletion, approaches and methods used for its estimation and reporting in Plasmodium falciparum populations in Africa: review of published studies 2010–2019. Malar J 18, 355 (2019). https://doi.org/10.1186/s12936-019-2987-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-019-2987-4