
Abstract
Background
Gaps remain in understanding the role of caregiver responses on time to seek appropriate care. The objective of this study was to describe caregiver responses to illness and the impact of these responses on time to seek appropriate care among children with malaria.
Methods
A case–control study of 325 children with severe (cases) and 325 children with uncomplicated (controls) malaria was conducted in Jinja, Uganda. Caregivers’ responses to their children’s illnesses and time to seek appropriate care were documented. Responses included staying at home, seeking care at drug shops, and seeking care at public health facilities classified into two types: (1) health facilities where caregiver initially sought care before enrollment, and (2) health facilities where children were provided appropriate care and enrolled in the study. Weighted Cox regression was used to determine risk factors for delays in time to seek appropriate care within 24 h of illness onset.
Results
Children staying home on self-medication was the most common initial response to illness among caregivers of controls (57.5%) and cases (42.4%, p < 0.001), followed by staying at home without medication (25.2%) and seeking care at drug shops (32.0%) for caregivers of controls and cases, respectively. Seeking care at drug shops was more common among caregivers of cases than of controls (32.0% vs. 12.3%; p < 0.001). However, compared to public health facilities, drug shops offered sub-optimal services with children less likely to have been examined (50.0% vs. 82.9%; p < 0.001) or referred to another facility (12.5% vs. 61.4%; p < 0.001). Upon adjustment for known risk factors for delay, initially seeking care at a drug shop (HR 0.37, p = 0.036) was associated with delay in seeking care at a health facility where appropriate care was provided. In contrast, those initially seeking care at public health facility before enrollment were more likely to subsequently seek care at another public health facility where appropriate care was provided (HR 5.55, p < 0.001).
Conclusion
Caregivers should be educated on the importance of promptly seeking care at a health facility where appropriate care can be provided. The role of drug shops in providing appropriate care to children with malaria needs to be reviewed.
Similar content being viewed by others


Background
The World Health Organization (WHO) emphasizes prompt (within 24 h of fever onset) treatment with effective anti-malarials as the main strategy for prevention of progression from uncomplicated to severe malaria [1, 2]. Concerted efforts by governments, international organizations, and partner institutions have resulted in increased availability of high quality and affordable artemisinin-based combination therapy (ACT) in both the public and private sectors of health [3,4,5,6]. Increased availability of ACT has likely contributed to reductions in malaria morbidity and mortality in sub-Saharan Africa [7,8,9]. However, despite progress, a large number of African children continue to die of malaria, partly due to delays in seeking appropriate care [10]; defined as prompt diagnosis by microscopy or RDTs for suspected malaria cases followed by treatment with ACT, if uncomplicated malaria is diagnosed, or parenteral artesunate and supportive care if severe malaria is diagnosed. For children with severe malaria, if appropriate care cannot be provided at the facility the child should be referred to a facility where care can be provided.
The proportion of African children with confirmed malaria receiving ACT has been reported to vary greatly, ranging from a low of 0.6% in Somalia to a high of 70.2% in Uganda [11]. Of concern, the proportion of children with confirmed malaria promptly receiving ACT is unacceptably low, ranging from 2 to 22% in 17 high burden countries in Africa [6]. Low provision of appropriate treatment for uncomplicated malaria is partly explained by preferential attention given to health system factors at the expense of focus on individual actions [12]. Time taken to seek appropriate care by caregivers of sick children is influenced by two important decisions: when to respond to illness and where to seek care [13]. These decisions determine the time to seek appropriate care. In sub-Saharan Africa, responses to seek care outside home are often delayed, and when a response is made, this response is often to seek care at a drug shop, rather than at a qualified health facility [14, 15].
Appreciation of the significance of caregiver responses to illness as determinants of promptly seeking appropriate care is increasing. However, despite their importance, the impact of these responses on time to seek appropriate care remains largely unexplored. As part of a case control study of risk factors for severe malaria, presented are caregivers’ responses to illness in children with uncomplicated and severe malaria. Predictors of different responses and impact of initial responses on time to seek appropriate care were also studied.
Methods
Study design
A matched case–control study was conducted to identify determinants of severe malaria in Ugandan children, as recently described [16]. In brief, 325 severe malaria cases and 325 uncomplicated malaria controls were enrolled. Severe malaria cases were enrolled at the Children’s Ward, Jinja Regional Referral Hospital (JRRH). Uncomplicated malaria controls were enrolled at a level III or higher public health facility, geographically matched (level of sub-county) to the residence of an age-matched case. Additionally, controls were matched to cases by calendar time (enrollment within 1 month of case). The latter two matching criteria were intended to result in selection of controls with an exposure distribution identical to that of the population that gave rise to the cases. Information concerning the child’s caregiver, head of household (relation to child, age, education level, employment status), and house characteristics and possessions were also documented and used to construct a wealth index for each child. GPS coordinates of participants’ homes were captured and used to determine distances between these homes and the nearest public health facility (Fig. 1). Information on caregivers’ responses to illness was systematically re-constructed into an itinerary detailing events that took place throughout the child’s illness reflecting progression of illness against response and actions taken from illness onset to the date and time when the child was enrolled. The itinerary was a comprehensive account of each caregiver’s pathway to seeking appropriate care.

Study site. Map demonstrating locations of residence’s for both severe malaria cases and uncomplicated malaria cases within the catchment area of Jinja Hospital
Responses
Caregiver responses to illness were categorized as staying at home or care seeking, defined as any care sought outside the home. If the caregiver provided the child medicine without having the child reviewed by a care-provider, this was referred to as staying home on self-medication. Public health facilities where caregiver sought care were categorized into two types, facilities where caregivers initially sought care before presenting to the facility where appropriate care was provided, and facilities where caregivers sought care leading to provision of appropriate care and enrollment in the study. Care seeking at private health facilities and non-biomedical sources of care were also captured. To distinguish drug shops from private clinics, drug shops were defined as facilities where caregivers could buy medicine without the need for the patient to be present. Private clinics were defined as facilities that offered care, with the patient required to pay a fee to be seen by a health worker and facilities for administering intravenous drugs.
Itinerary of events data
Each caregiver’s itinerary started on the date of illness onset and ended on the date when the child arrived at a public health facility where the child was provided appropriate care and enrolled in the study. To determine the date of illness onset, caregivers were asked to recall the date when the child was last well. Using that date as a reference point, interviewers probed the caregiver about the subsequent daily state of the child’s health. The day when the caregiver reported that the child’s health had deviated from normal was documented as the start date of illness. Starting from that date, caregivers were asked a standard set of questions (Additional file 1) concerning each day of illness, regarding observed symptoms including fever, signs, and response. If the response was care-seeking, caregivers were asked to specify where they sought care, what intervention was provided, and who made care decisions. Additional information related to health services offered by care-providers before enrollment was captured based on caregiver reports. Specifically, we asked if the provider: (1) examined the child, confirmed by having touched the child, and (2) performed laboratory tests for malaria testing and haemoglobin estimation. Provision of anti-malarials to children was also queried. Efforts were made to validate caregiver reports based on description of medicines, and available prescription notes. An event constituted reported symptoms, response, and intervention(s) given, and was defined by the response. Each event represented a step in the caregiver’s itinerary, with subsequent days representing distinct steps in the caregiver’s itinerary, even if the response did not change. Different responses on the same day were captured as distinct events.
Analysis
Data were entered using Microsoft Access (Microsoft Corporation) and analyzed using STATA (version 14; STATA Corp., College Station, TX, USA). Caregiver responses were grouped as follows: (1) stayed home; not on medication, (2) stayed home on medication, (3) sought care at a drug shop, (4) sought care at a non-biomedical provider, (5) sought care at a private clinic, and (6) sought care at public health facilities ranging from level II to hospitals. For analysis of association between initial response types and time to seek care, care-seeking at private health facilities and non-biomedical providers (< 1% of responses) were collapsed under the categories drug shops and stayed home not on medication, respectively. Time (in days) to seek appropriate care was calculated based on the duration between time when fever was first noted and time of arrival at the enrolling health facility. As cases and controls were matched, the Wilcoxon matched pair signed-rank and the Chi square tests were used for testing the significance of differences between continuous and categorical data in cases and controls, respectively. Caregiver actions were compared based on the initial response by the caregiver and the sum of responses throughout the itinerary of events. Additionally, frequencies of different responses at different time points (equivalent to steps in itineraries) on caregivers’ pathways to care were compared. Health services offered by providers’ were presented as proportion of children who receiving a specified service among those who sought care at the provider. This analysis was limited to children who had severe malaria, as they were more likely to have sought care at an initial facility. Risk factors for care seeking at drug shops as the initial response to illness were determined using logistic regression with a dichotomous outcome (seeking care at a drug shop vs. others). As this outcome was not the basis for the case–control study, weighted logistic regression analysis was performed to account for the biased representation of the outcome amongst cases, as has been described by others [17]. The population incidence of cases was estimated to be 2000 cases per 100,000 people per year (0.02) based on the World Health Organization Uganda malaria country profile [18]. A logistic regression backward stepwise approach (p = 0.2) was used to identify variables for inclusion in the final logistic regression model. Excluded variables that contributed to model fitness and interpretation were retained in the model. Variables were also excluded for collinearity.
Life tables were used to demonstrate patterns of seeking appropriate care at different intervals by caregivers of cases and controls. Weighted Kaplan–Meier survival curves and the Cox regression model were used to determine the un-adjusted and adjusted association between initial caregiver responses and time taken to seek appropriate care within the first 24 h of illness onset, respectively.
Results
Care-seeking characteristics
Caregivers of children with severe malaria (cases) took longer to seek appropriate care (median 2.4 vs. 1.7 days; p < 0.001) and had more responses (median 4.0 vs. 3.0; p < 0.001) compared to caregivers of children with uncomplicated malaria (controls, Table 1). Considering initial responses, overall, staying home on self-medication (49.5%) was the most common response followed by staying at home not on medication (22.9%) and care-seeking at a drug shop (22.1%). Among controls, staying home on self-medication (57.3%) was the most common response followed by staying home not on medication (25.2%) and care-seeking at a drug shop (12.4%). For cases, staying home on self-medication (42.1%) was the most common response followed by care-seeking at a drug shop (32.0%) and staying at home not on medication (20.6%). By comparison, staying home on self-medication (57.2% vs. 42.1%; p < 0.001) was more common among caregivers of controls compared to those of cases. Additionally, initially care-seeking at public health facilities (4.6% vs. 0.6%, p < 0.001) where children were provided appropriate care and enrolled, was more common among controls than cases. In contrast, initially care seeking at drug shops (32.0% vs. 12.3%; p = 0.001) and care-seeking at a public health (4.0% vs. 0%, p < 0.001) before enrollment was more common among caregivers of cases than controls. When the sum of responses were considered, caregivers of controls were more likely to have stayed at home (on medication; 42.4% vs. 26.0%), compared to caregivers of cases. In contrast, caregivers of cases were more likely to have sought care at drug shops (18.3% vs. 6.8%, p < 0.001) and at a public health facility (12.3% vs. 0.7%, p < 0.001; Table 1), compared to caregivers of controls. Consideration of caregiver pathways to care showed that differences in frequencies of occurrence of staying at home (more frequent among controls) or seeking care at drug shops (more frequent among cases) were consistent throughout pathways (Fig. 2).

Frequency of responses at different points in caregiver pathways to care. The analysis was limited to the first six steps of caregiver itineraries, when most (> 80%) caregivers had sought appropriate care. The category stayed home included those on medication and not on medication
Health services provided to children at facilities before enrolment with severe malaria
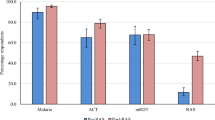
Compared to private clinics or public health facilities, drug shops provided sub-optimal health service (Table 2). Considering physical examination, drug shops examined fewer children compared to those seen at private clinics (50% vs. 78%, p < 0.001) or all public health facilities (50.0 vs. 82.9%, p < 0.001; Table 2). Malaria testing rates were low across all facilities, but highest at public hospitals (43.5%), private clinics (42.0%), and level IV public facilities (41.3%), and lowest at drug shops (8.9%, p < 0.001 compared to all other sites). Hemoglobin testing was not done at drug shops, but was provided at public facilities (26.8%; range 5.9% at health centre II to 43.5% at public hospitals) and private clinics (28.0%). Provision of anti-malarials to presenting children was highest at drug shops and level II public facilities and lowest at public hospitals (Table 2). Consider patient referral, drug shops were less likely to refer children compared to all public hospitals (12.5% vs. 61.4%, p < 0.001).
Factors associated with care-seeking at a drug shop as the initial response to illness
With unadjusted analysis, increasing age of the head of the household (OR 0.94, p < 0.001) was protective against initially care seeking at a drug shop. Upon adjustment, employed caregivers were two times more likely to have sought care at a drug shop compared to those who were not employed (OR 2.33, p = 0.017). Older caretakers (OR 0.95, p = 0.043) and first decision by the child’s mother (OR 0.38, p = 0.026) were protective against care seeking at a drug shop. When the adjusted analysis was limited to caregivers with available GPS data, longer distance to the nearest public health facility (level III and above; OR 1.07; p = 0.397) was not a risk factor for care seeking at a drug shop as the initial response (Table 3).
Time to seeking appropriate care
Considering the entire itineraries, caregivers of controls were more likely to have sought appropriate care earlier compared to caregivers of cases (Table 4, log rank test 0.001). Differences in time to seek appropriate care were most significant during the first 24 h, when 30.4% of caregivers of controls (hazard 0.35, 95% CI 0.28, 0.42), but only 11.6% of caregivers of cases (hazard 0.12, 95% CI 0.08, 0.16) had sought appropriate care. By 48 h after illness onset, 60.0% of caregivers of controls had sought appropriate care compared to only 35.5% of caregivers of cases (hazards 0.53, 95% CI 0.43, 0.64 and 0.30, 95% CI 0.24, 0.37, respectively). Thereafter, probabilities of seeking appropriate care were similar.
Impact of care-seeking responses on time to seek appropriate care
Using Kaplan–Meier survival curves, initial responses (Cox test p = 0.003), socio-economic position (Cox test p = 0.002), and having a caregiver with post primary education (Coxtest p = 0.001) were significantly associated with prompt seeking of appropriate care within the first 24 h of fever onset (Fig. 3). Upon adjustment, caregivers who initially sought care at a drug shop (HR 0.37; 95% CI 0.14, 0.93, p = 0.036) were nearly three times more likely to delay in seeking appropriate care within the first 24 h. These findings contrast with those of caregivers who initially sought care at a public health facility (HR 5.55; 95% 2.12, 14.5, p < 0.001) prior to enrollment in the first 24 h, who were more likely to have sought care at a public health facility where appropriate care was provided within the same interval (Table 5). In the final model, compared to those with lower levels of education, caregivers with post-primary education were more likely to have sought care early (Table 5).

Kaplan Meier Curves for probability of caregivers seeking appropriate care based on different explanatory variables
Discussion
Caregiver responses to children with severe and uncomplicated malaria vary. Overall, staying at home was the most common response to illness by caregivers, followed by care seeking at a drug shop, which was more common among caregivers of children with severe malaria. At every interval following illness onset, compared to caregivers of children with uncomplicated malaria, caregivers of those with severe malaria were more likely to have delayed seeking of appropriate care. This difference was most pronounced in the initial 24 h following fever onset. During this interval, care seeking at a drug shop as the initial response to illness was significantly associated with delay in seeking appropriate care.
Staying home is a common initial response to illness among caregivers of children with fever, accounting for 68% to 83% of initial caregiver responses to illness in three prior studies in sub-Saharan Africa [19,20,21]. At home, majority of caregivers provide self-medication [22], as was observed in our study, in which half of the children initially stayed home and were provided with medication by their caregivers. Upon adjustment, a significant association between staying at home on self-medication and delayed care-seeking was not found. However, the practice has the potential to contribute to delays in seeking appropriate care. In 2000, in the interest of broadening access to care, the Roll Back Malaria Summit in Abuja passed a declaration allowing for treatment of malaria at home [23]. Since then, and based on experimental studies that demonstrated benefit [24, 25], the WHO has advocated for Home Management of Malaria (HMM) as an intervention to increase prompt access to effective anti-malarials [26]. However, despite being associated with prompt initiation of treatment, inappropriate treatment at home compromises the effectiveness of this approach [27,28,29]. Integration of HMM into community case management of childhood illness (iCCM), an enhanced version of HMM, has also been associated with high levels of inappropriate treatment [30, 31]. Despite limitations, HMM and iCCM, if effectively implemented, offer home and community based initiatives for providing prompt treatment to populations at risk of malaria.
In this study, drug shops were the most common initial service provider sought, particularly among caregivers of children with severe malaria. Previous studies in Uganda indicated that more than half of caregivers (range 51.7–56.6%) used private outlets to treat childhood fevers [32]. Similar findings were reported in Ghana, where half of patients visiting a health facility with severe malaria had previously sought care at a drug shop [33]. Employed caregivers were more likely to seek care at drug shops, potentially attributed to their ability to afford these services or the advantages of physical accessibility or flexible opening hours.
However, despite their popularity drug shops have been associated with sub-optimal services for children suffering from malaria [34,35,36]. The results of this study linked drug shops with sub-optimal practices, as reported by caregivers, including low rates of physical examination of sick children, malaria diagnostic testing, and referral. These findings are consistent with reports from Tanzania indicating that children with confirmed malaria are less likely to receive an ACT from a drug shop as compared to a public facility [12]. In Uganda and Kenya, surveys of health facilities indicate that most drug shops stocked poor quality anti-malarials in addition to stocking non-recommended monotherapies [37, 38]. Low testing rates at drug shops indicate that most children were managed for malaria presumptively, thus not following WHO guidelines.
Due to their close proximity and popularity among rural populations [34, 39, 40], there is growing interest in utilizing drug shops to extend health care services [41, 42]. However, despite their potential to provide prompt treatment [43, 44], because treatment may be inappropriate, drug shops may actually delay access to appropriate care [45, 46], increasing the risk of progression of uncomplicated to severe malaria. Regrettably, the findings of this study point to this problem, evidenced by the observation that, despite seeking care promptly, caregivers who initially sought care at drug shops were likely to delay seeking appropriate care within the first 24 h of illness onset. This finding is substantiated by caregiver reports, which indicated that drug shops as compared to public health facilities were significantly less likely to refer patients to another facility. Indeed, a recent study conducted in Uganda suggested that providers at drug shops are not motivated to refer patients, presumably due to economic benefits to shopkeepers of providing care [14]. Surprisingly, compared to drug shops that frequently prescribed anti-malarials, prescription of anti-malarials by public health facilities was low, especially at public hospitals. This paradox may be explained by the fact that public health facilities were caring for children who had probably received treatment prior to presenting at the facility. Additionally, public facilities were more likely to refer patients’ unlike drug shops that did not. Despite limitations, by providing medicines promptly, drug shops provide vital services close to communities at risk. Indeed, through training and price subsidies [4, 47] the quality of services offered at drug shops has been improved [35]. However, it remains unclear if acceptable standards of managing children with malaria can be attained and gains sustained at drug shops [48,49,50,51].
This study had some limitations inherent to the case–control study design. First, cases were enrolling from a referral hospital, excluding cases that were not hospitalized at this facility, limiting the representativeness of the study population. For example, children who died at home from severe malaria were not represented. Second, recall by caregivers, including interventions by different facilities, could have been a source of bias influenced by the state of the child at the time of enrolment. Third, despite assuring respondents of confidentiality, caregivers may have been reluctant to report unconventional choices of care for fear of perceived rebuke. Fourth, the estimated population incidence of severe malaria used to adjust for biased representation among cases in the study population may have resulted in inaccurate population estimates, compromising validity of the study findings related to secondary outcomes. Lastly, recording of caregiver responses in a sequential manner limited the ability to study the influence of concurrent responses on outcomes.
Conclusion
Findings from this study provide useful insights about caregiver responses to illness and the impact of these responses on time to seek appropriate care for children with malaria. Caregivers preferred to stay at home as the initial response to illness, and if they sought care outside the home, drug shops were preferred. Unfortunately, visits to drug shops led to delay in seeking appropriate care, probably due to in-appropriate care provided. Albeit limitations, drug shops provide an opportunity to bridge the gap and by promptly providing effective anti-malarial treatment to children with malaria, drug shops could provide benefit. However, for benefits to be realized and sustained, the role of drug shops in providing care to sick children needs to be re-defined, appropriate care protocols established, and effective mechanisms of regulating drug shops instituted. Finally, prioritizing and directing limited resources to holistically strengthening the existing public health system may be a more rational approach.
References
WHO. Managment of severe Malaria, practical handbook. 3rd ed. Geneva: World Health Organization; 2012.
WHO. Global Technical Strategy for Malaria 2016–2030. Geneva: World Health Organization; 2016.
Opiyo N, Yamey G, Garner P. Subsidising artemisinin-based combination therapy in the private retail sector. Cochrane Database Syst Rev. 2016;3:CD009926.
Tougher S, Mann AG, Group AC, Yess Y, Kourgueni IA, Thomson R, et al. Improving access to malaria medicine through private-sector subsidies in seven African countries. Health Aff (Millwood). 2014;33:1576–85.
Ye Y, Arnold F, Noor A, Wamukoya M, Amuasi J, Blay S, et al. The affordable medicines facility-malaria (AMFm): are remote areas benefiting from the intervention? Malar J. 2015;14:398.
Galactionova K, Tediosi F, de Savigny D, Smith T, Tanner M. Effective coverage and systems effectiveness for malaria case management in sub-Saharan African countries. PLoS One. 2015;10:e0127818.
Camponovo F, Bever CA, Galactionova K, Smith T, Penny MA. Incidence and admission rates for severe malaria and their impact on mortality in Africa. Malar J. 2017;16:1.
Korenromp E, Mahiane G, Hamilton M, Pretorius C, Cibulskis R, Lauer J, et al. Malaria intervention scale-up in Africa: effectiveness predictions for health programme planning tools, based on dynamic transmission modelling. Malar J. 2016;15:417.
Chuma J, Abuya T, Memusi D, Juma E, Akhwale W, Ntwiga J, et al. Reviewing the literature on access to prompt and effective malaria treatment in Kenya: implications for meeting the Abuja targets. Malar J. 2009;8:243.
WHO. World Malaria Report. Geneva: World Health Organization; 2016.
Bennett A, Bisanzio D, Yukich JO, Mappin B, Fergus CA, Lynch M, et al. Population coverage of artemisinin-based combination treatment in children younger than 5 years with fever and Plasmodium falciparum infection in Africa, 2003–2015: a modelling study using data from national surveys. Lancet Glob Health. 2017;5:e418–27.
Ensor T, Cooper S. Overcoming barriers to health service access: influencing the demand side through purchasing. HNP Discussion Paper. 2004;1:69–79.
Mackian S, Bedri N, Lovel H. Up the garden path and over the edge: where might health-seeking behaviour take us? Health Policy Plan. 2004;19:137–46.
Mbonye AK, Buregyeya E, Rutebemberwa E, Clarke SE, Lal S, Hansen KS, et al. Referral of children seeking care at private health facilities in Uganda. Malar J. 2017;16:76.
Kolola T, Gezahegn T, Addisie M. Health care seeking behavior for common childhood illnesses in Jeldu District, Oromia Regional State, Ethiopia. PLoS One. 2016;11:e0164534.
Mpimbaza A, Ndeezi G, Katahoire A, Rosenthal PJ, Karamagi C. Demographic, socioeconomic, and geographic factors leading to severe malaria and delayed care seeking in Ugandan children: a case-control study. Am J Trop Med Hy. 2017;97:1513–23.
Sommerfelt H, Steinsland H, van der Merwe L, Blackwelder WC, Nasrin D, Farag TH, et al. Case/control studies with follow-up: constructing the source population to estimate effects of risk factors on development, disease, and survival. Clin Infect Dis. 2012;55(Suppl 4):S262–70.
WHO. Uganda: country profile, World Health Organization. http://www.who.int/malaria/publications/country-profile_uga.en.pdf. Accessed 21 June 2017.
Romay-Barja M, Cano J, Ncogo P, Nseng G, Santana-Morales MA, Valladares B, et al. Determinants of delay in malaria care-seeking behaviour for children 15 years and under in Bata district, Equatorial Guinea. Malar J. 2016;15:187.
Kassile T, Lokina R, Mujinja P, Mmbando BP. Determinants of delay in care seeking among children under five with fever in Dodoma region, central Tanzania: a cross-sectional study. Malar J. 2014;13:348.
Nonvignon J, Aikins MK, Chinbuah MA, Abbey M, Gyapong M, Garshong BN, et al. Treatment choices for fevers in children under-five years in a rural Ghanaian district. Malar J. 2010;9:188.
McCombie SC. Treatment seeking for malaria: a review of recent research. Soc Sci Med. 1996;43:933–45.
African Heads of State and Government; World Health Organization. The Abuja Declaration and the Plan of Action. An extract from the African Summit on Roll Back Malaria, Abuja, 25 April 2000 (WHO/CDS/RBM/2000.17). http://apps.who.int/iris/bitstream/handle/10665/67816/WHO_CDS_RBM_2003.46.pdf. Accessed 14 Mar 2010.
Kidane G, Morrow RH. Teaching mothers to provide home treatment of malaria in Tigray, Ethiopia: a randomised trial. Lancet. 2000;356:550–5.
Sirima SB, Konate A, Tiono AB, Convelbo N, Cousens S, Pagnoni F. Early treatment of childhood fevers with pre-packaged antimalarial drugs in the home reduces severe malaria morbidity in Burkina Faso. Trop Med Int Health. 2003;8:133–9.
WHO. Lessons learned in home management of malaria. Geneva: World Health Organization; 2007.
Hopkins H, Talisuna A, Whitty CJ, Staedke SG. Impact of home-based management of malaria on health outcomes in Africa: a systematic review of the evidence. Malar J. 2007;6:134.
Okwundu CI, Nagpal S, Musekiwa A, Sinclair D. Home- or community-based programmes for treating malaria. Cochrane Database Syst Rev. 2013;5:CD009527.
Staedke SG, Mwebaza N, Kamya MR, Clark TD, Dorsey G, Rosenthal PJ, et al. Home management of malaria with artemether-lumefantrine compared with standard care in urban Ugandan children: a randomised controlled trial. Lancet. 2009;373:1623–31.
Ameh S, Welaga P, Kabiru CW, Ndifon W, Ikpeme B, Nsan E, et al. Factors associated with appropriate home management of uncomplicated malaria in children in Kassena-Nankana district of Ghana and implications for community case management of childhood illness: a cross-sectional study. BMC Public Health. 2015;15:458.
Ferrer BE, Webster J, Bruce J, Narh-Bana SA, Narh CT, Allotey NK, et al. Integrated community case management and community-based health planning and services: a cross sectional study on the effectiveness of the national implementation for the treatment of malaria, diarrhoea and pneumonia. Malar J. 2016;15:340.
Kassam R, Collins JB, Liow E, Rasool N. Caregivers’ treatment-seeking behaviors and practices in Uganda—a systematic review (Part II). Acta Trop. 2015;152:269–81.
Ansah EK, Gyapong M, Narh-Bana S, Bart-Plange C, Whitty CJ. Factors influencing choice of care-seeking for acute fever comparing private chemical shops with health centres and hospitals in Ghana: a study using case–control methodology. Malar J. 2016;15:290.
Awor P, Wamani H, Bwire G, Jagoe G, Peterson S. Private sector drug shops in integrated community case management of malaria, pneumonia, and diarrhea in children in Uganda. Am J Trop Med Hyg. 2012;87:92–6.
Kioko U, Riley C, Dellicour S, Were V, Ouma P, Gutman J, et al. A cross-sectional study of the availability and price of anti-malarial medicines and malaria rapid diagnostic tests in private sector retail drug outlets in rural Western Kenya, 2013. Malar J. 2016;15:359.
Buregyeya E, Rutebemberwa E, LaRussa P, Lal S, Clarke SE, Hansen KS, et al. Comparison of the capacity between public and private health facilities to manage under-five children with febrile illnesses in Uganda. Malar J. 2017;16:183.
Nakalembe L. Survey of antimalarial medicines and pharmacopoeial quality of artemether-lumefantrine tablets sold in private pharmacies and drug shops in Tororo district. Dissertation Master of Science in Pharmacology of Makerere University. 2017.
Group AC, Musuva A, Ejersa W, Kiptui R, Memusi D, Abwao E. The malaria testing and treatment landscape in Kenya: results from a nationally representative survey among the public and private sector in 2016. Malar J. 2017;16:494.
Sudhinaraset M, Ingram M, Lofthouse HK, Montagu D. What is the role of informal healthcare providers in developing countries? A systematic review. PLoS One. 2013;8:e54978.
Rutebemberwa E, Pariyo G, Peterson S, Tomson G, Kallander K. Utilization of public or private health care providers by febrile children after user fee removal in Uganda. Malar J. 2009;8:45.
Rutebemberwa E, Buregyeya E, Lal S, Clarke SE, Hansen KS, Magnussen P, et al. Assessing the potential of rural and urban private facilities in implementing child health interventions in Mukono district, central Uganda-a cross sectional study. BMC Health Serv Res. 2016;16:268.
Liu J, Prach LM, Treleaven E, Hansen M, Anyanti J, Jagha T, et al. The role of drug vendors in improving basic health-care services in Nigeria. Bull World Health Organ. 2016;94:267–75.
Awor P, Wamani H, Tylleskar T, Jagoe G, Peterson S. Increased access to care and appropriateness of treatment at private sector drug shops with integrated management of malaria, pneumonia and diarrhoea: a quasi-experimental study in Uganda. PLoS One. 2014;9:e115440.
Rutta E, Liana J, Embrey M, Johnson K, Kimatta S, Valimba R, et al. Accrediting retail drug shops to strengthen Tanzania’s public health system: an ADDO case study. J Pharm Policy Pract. 2015;8:23.
Dixit A, Lee MC, Goettsch B, Afrane Y, Githeko AK, Yan G. Discovering the cost of care: consumer, provider, and retailer surveys shed light on the determinants of malaria health-seeking behaviours. Malar J. 2016;15:179.
Rutebemberwa E, Kallander K, Tomson G, Peterson S, Pariyo G. Determinants of delay in care-seeking for febrile children in eastern Uganda. Trop Med Int Health. 2009;14:472–9.
Awor P, Wamani H, Tylleskar T, Peterson S. Drug seller adherence to clinical protocols with integrated management of malaria, pneumonia and diarrhoea at drug shops in Uganda. Malar J. 2015;14:277.
Boyce MR, O’Meara WP. Use of malaria RDTs in various health contexts across sub-Saharan Africa: a systematic review. BMC Public Health. 2017;17:470.
Webster P. Drug shops as primary point of care-the case of Nigeria. Lancet. 2017;390:15–7.
Mackintosh M, Channon A, Karan A, Selvaraj S, Cavagnero E, Zhao H. What is the private sector? Understanding private provision in the health systems of low-income and middle-income countries. Lancet. 2016;388:596–605.
Group AC, Tougher S, Hanson K, Goodman C. What happened to anti-malarial markets after the Affordable Medicines Facility-malaria pilot? Trends in ACT availability, price and market share from five African countries under continuation of the private sector co-payment mechanism. Malar J. 2017;16:173.
Authors’ contributions
AM, CK, PJR conceived the idea. AM, CK contributed to data collection. AM, CK, led the analysis and interpretation of the data. AM, PJR, CK, AK, and GN contributed to interpretation of results. AM, AK, PJR wrote the first draft of the paper. All authors read and approved the final manuscript.
Acknowledgements
We thank the clinical study team of Yasin Kisambira, Jessica Tagobera, Annet Nabweteme, Prossy Ewinyo, Azizz Kiwanuka, Rose Nabirye, Peter Wambi, Ronald Bayisuka, William Ambayo, Juliet Nabunjje, Fiona Kassana, David Katikati, Sally Opus and Benjamin Buyi. We also thank health workers in Jinja Hospital and other participating health facilities for supporting the study team. We thank the staff of the Infectious Diseases Research Collaboration for providing administrative support and Kelly Wilson and Grant Guyen from the University of Washington for providing guidance in the mapping analysis. We also thank Sarah Staedke and Grant Dorsey for providing methodological and statistical advice to the study team. Finally, we are grateful to the parents, guardians, and caretakers who agreed to take part in this study.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable to this study.
Ethics approval and statement
Informed consent was obtained from the parents or guardians of all study participants. The study protocol was approved by the Uganda National Council of Science and Technology and the Institutional Review Boards of the School of Medicine, Makerere University-College of Health Sciences, and the University of California, San Francisco.
Funding
This research was supported by two training awards from the NIH Fogarty International Center, the University of California Global Health Institute GloCal Health Fellowship (TW009343) and the Training in Malaria Research in Uganda program (TW007375). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1.
Itinerary of events.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mpimbaza, A., Katahoire, A., Rosenthal, P.J. et al. Caregiver responses and association with delayed care-seeking in children with uncomplicated and severe malaria. Malar J 17, 476 (2018). https://doi.org/10.1186/s12936-018-2630-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-018-2630-9