
Abstract
Background
Plasmodium falciparum accounts for approximately 60% of malaria cases in Ethiopia and artemether–lumefantrine has been used as a first-line treatment for uncomplicated P. falciparum malaria since 2004. The aim of this study was to assess the therapeutic efficacy of artemether–lumefantrine (AL) for the treatment of uncomplicated P. falciparum malaria in north-western Ethiopia.
Methods
A 28-day one-arm, prospective evaluation of the clinical and parasitological response to the first-line treatment for uncomplicated P. falciparum malaria was conducted in Enfranze Health Centre in accordance with the 2009 WHO efficacy study guidelines. Patients were treated with a 3-day course of AL and clinical and parasitological parameters were monitored over a 28-day follow-up. All data from recruited patients were imported into an electronic data base and Kaplan–Meier survival analysis was used for analysing primary [early treatment failures (ETF), late clinical failure (LCF), late parasitological failures (LPF), and adequate clinical and parasitological response (ACPR)] and secondary (PCT, GCT and FCT) outcomes.
Results
Eighty patients were enrolled and all of them completed the 28-day follow-up period. The PCR-corrected cure rate was 95.0% (95% CI 87.0–98.4%) and there were two ETF, one LCF and three LPF. Two of the LPF were classified as re infections by PCR. Seventy three point seven five percent, 91.25 and 95% of patients had cleared their parasitaemia by days 1, 2, and 3, respectively, and 75, 91.25 and 96.25% of patients had cleared their fever by days 1, 2, and 3. All patients completely cleared their gametocytes by day 7.
Conclusion
The relatively high cure rate, low proportion of patients still positive on day 3 as well as parasite clearance times in this study would indicate no imminent threat of artemisinin resistance development in the region. However, the threat of spreading or de novo development of artemisinin resistance warrants regular monitoring of drug efficacy throughout the region.
Similar content being viewed by others


Background
Malaria is a disease caused by protozoan parasites of the genus Plasmodium and transmitted by female Anopheles mosquitoes. Plasmodium falciparum is by far the most important specie, responsible for nearly all severe malaria cases [1, 2]. About 198 million cases of malaria occurred globally in 2013 and the disease led to 584,000 deaths. The burden is heaviest in the WHO African Region, where an estimated 90% of all malaria deaths occur, and in children <5 years of age, who account for 78% of all deaths [3].
Malaria is the leading communicable disease in Ethiopia and an estimated 68% of the population of Ethiopia lives in areas at risk of malaria [4]. In the country, P. falciparum and Plasmodium vivax are the main species accounting for roughly 60 and 40% of malaria cases, respectively [5, 6]. Plasmodium falciparum causes severe malaria with a case fatality rate of about 10% in hospitalized adults and up to 33% in children less than 12 years old in Ethiopia [7].
Early diagnosis and prompt treatment is one of the main strategies in malaria prevention and control and it is also the key to reducing morbidity and preventing mortality [8]. However, efforts towards controlling malaria are greatly challenged by the increasing spread of anti-malarial drug resistance [3]. Use of ineffective anti-malarial drugs contributes to the difficulties in reducing malaria morbidity and mortality, leads to the spread of malaria to new areas, re-emergence of malaria in areas where the disease had been eliminated and it has also played an important role in the occurrence and severity of epidemics [9]. Anti-malarial drug resistance is observed in P. falciparum malaria, but has also been identified in P. vivax [10, 11].
In Ethiopia, high level resistance to chloroquine (CQ) in 1998 necessitated a change to sulfadoxine–pyrimethamine (SP) as first-line anti-malarial drug. However, high treatment failure rates with SP of up to 72% were reported in some areas which have led to increasing acceptance of using a combination of two or more drugs in an attempt to reduce malaria transmission and resistance development. Consequently, artemether–lumefantrine (AL) was adopted in 2004, which currently is being used as the first-line drug for the treatment of uncomplicated P. falciparum malaria [8]. A base-line study in 2004 showed that AL was a highly efficacious drug with a treatment success of 99.1% and with few reports of adverse effects [12, 13].
The World Health Organization (WHO) recommends artemisinin-based combinations, such as AL, as first-line treatment forum complicated P. falciparum malaria in all endemic countries [14]. However, resistance of P. falciparum to artemisinin has been confirmed in western Cambodia and Thailand [15]. This resistance has spread from the Thai–Cambodia border to the Greater Mekong region, up to the border of Myanmar and India [16–19]. This resistance has the potential to spread to or develop de novo in other parts of the world [20] and drug efficacy may slowly deteriorate over time. The WHO recommends regular monitoring of drug efficacy for the first line anti-malarial drugs at defined sentinel sites at least once every 2 years in order to detect changes in their therapeutic efficacy [14]. The main focus of this study was to assess the therapeutic efficacy of AL in the treatment of uncomplicated P. falciparum malaria in north-western Ethiopia.
Methods
Study area
The study was conducted at Enfranze Health Centre. Enfranze is a sub-district, located in North Gondar administrative zone, Amhara Region, 675 km north of Addis Ababa and 60 km from Gondar town and at an elevation of 1,500 m above sea level. This area is malaria-endemic with a total population of about 45,686 (municipality report) and the majority of the population depends on subsistence farming.
Study design and period
The design was a one-arm, prospective evaluation of the clinical and parasitological response to directly observed treatment for uncomplicated P. falciparum malaria conducted between January and May 2013.
Study subjects
The study subjects were recruited among febrile patients attending Enfranze Health Centre using inclusion criteria as defined in the WHO guidelines for assessing the therapeutic efficacy of anti-malarial drugs against P. falciparum malaria [21].
Inclusion criteria and exclusion criteria
The following inclusion criteria were used for the study: mono-infection with P. falciparum, above 6 months of age, a parasitaemia of 1,000—100,000/μl, weight >5 kg, presence of axillary temperature (≥37.5°C) and no use of anti-malarial drugs 2 weeks prior to enrollment into the study. Patients with danger signs of severe and complicated malaria according to WHO criteria (including severe anaemia defined as haemoglobin <5 g/dl), history of allergic reactions to the study drug AL, mixed infection with another Plasmodium species, concomitant presence of febrile conditions with the potential to confound study outcome (e.g. acute respiratory infection, severe diarrhoea or other known underlying chronic or severe diseases (e.g. cardiac, renal or hepatic diseases, HIV/AIDS), severe malnutrition (defined as a child whose growth standard is below −3 z-score, has symmetrical oedema involving at least the feet or has a mid-upper arm circumference <110 mm for 6 month–18 years of age children and has a mid-upper arm circumference <170 mm, BMI <16 with or has a mid-upper arm circumference <180 mm with recent weight loss or underlying chronic illness for adults), as well as pregnant and lactating women, were not included in the study.
Sample size and sampling technique
The sample size was determined using a single population proportion formula according to the WHO guidelines: assuming a maximum of 25% clinical failures, 10% precision, and a confidence level of 95% with up to 10% losses to follow up a sample size of 80 was calculated [21].
Data collection procedures
A rapid screening procedure was used in an outpatient setting to identify patients who meet enrolment criteria. The typical screening data set included age, sex, temperature, body weight, pregnancy test, initial blood slide examination and haemoglobin. All patients meeting the basic enrolment criteria during the screening procedure were evaluated in greater depth by a member of the study team. Physical examination was performed at baseline (day 0 before dosing) and on days 1, 2, 3, 7, 14, 21 and 28. Body weight was determined on day 0 using a weight scale. The screening weight was used to calculate the dose (number of tablets) to be administered. Axillary temperature was measured at baseline (day 0 before dosing) and on days 1, 2, 3, 7, 14, 21 and 28. Female patients of child-bearing age (12–49 years) were asked to provide a urine sample for pregnancy testing before enrolment in the study and if sexually active were provided with condoms for the duration of the study.
Sample collection and processing
Finger-prick blood samples were collected from consenting patients for malaria parasite identification and haemoglobin level measurement. Patients that satisfied the criteria were enrolled into the study and followed up on days 1, 2, 3, 7, 14, 21, and 28 where finger-prick samples were taken for microscopic glass slides. Another drop of blood was collected on Whatman 903® filter paper on day 0 during enrollment and in case of recurrent parasitaemia. The filter paper was air dried and stored in a self-sealing plastic bag with desiccators for further molecular analysis.
Microscopic diagnosis of malaria parasites
Thick and thin blood smears were prepared and stained with 10% Giemsa (pH 7.4) for 10 min and read by two senior microscopists. Blood films were taken at least eight times for each patient during the study period (day 0, 1, 2, 3, 7, 14, 21 and 28) and during any unscheduled visit. A blood film was considered negative when no parasites were seen after examining 100 high power fields on the thick film. Parasites were counted on thick films relative to 200 leukocytes by two microscopists blinded to each other’s results. Blood smears with discordant results (differences between the two microscopists in species diagnosis, or differences in parasite density of >50%) were re-examined by a third, independent microscopist, and parasite density was calculated by averaging the two closest counts.
Genotyping of malaria parasites
In order to differentiate a recrudescence from a newly acquired infection, blood spots were collected from all patients at day 0 (before drug intake) and in case of LPF on Whatman filter paper and sent to Medical University of Vienna for genotyping of merozoite surface protein 1 (MSP1), merozoite surface protein 2 (MSP2) and glutamate-rich protein (GLURP). To exclude mixed infections or infections with other human malaria parasites the samples were analysed with nested PCR for species classification as reported previously [22, 23]. Afterwards P. falciparum monoinfections were genotyped. Gene loci—glurp, msp1 and msp2—of these samples were compared by PCR as described previously [24].
Haematological assessment
Finger-prick blood samples were used to measure haemoglobin. Due to limited resources the actual haemoglobin concentration should be measured by hemocue. However, this study assessed the haematocrit value only. In healthy persons, the haematocrit (expressed as a percentage) is roughly three times the haemoglobin concentration (expressed in grams per decilitre). This ratio is maintained in normocytic anaemia, but in most of the tropical forms of chronic anaemia the ratio is 3.3:1.
Treatment and follow-up of patients
All eligible patients were treated with AL (Coartem®) (Novartis Pharmaceutical Corporation, Suffern, New York, USA for Novartis Pharma AG, Basel, Switzerland, and Bach No. F-2832) twice daily on days 0, 1, and 2. Study participants were advised to take the study drug with milk to improve absorption. Study medication was administered based on weight; the first and each morning dose were directly observed by the study staff [25]. The evening doses were given to the patient/guardian for self-administration in the presence of health extension workers. Patients were followed for 30 min post-treatment and if vomiting occurred, a second full dose was administered. If repeated vomiting occurred, patients were withdrawn from the study. Patients were asked to return to the health centre on days 1, 2, 3, 7, 14, 21, and 28 or whenever they did not feel well. Patients withdrawn or with complications were referred to the health centre for proper treatment. Patients experiencing a reemergence of P. falciparum parasitaemia were treated with quinine.
In vivo analysis and classification response
Patients were classified as early treatment failure (ETF), late clinical failure (LCF), and late parasitological failure (LPF, adequate clinical and parasitological response (ACPR) as per WHO definition [21].
Data analysis
After checking for completeness all data were imported into Excel and Kaplan–Meier survival analysis was used for analysing primary (ETF, LCF, LPF, and ACPR) and secondary (PCT, FCT, GCT) outcomes, Cox regression was used to identify predictor variables of secondary outcomes. P values <0.05 were considered statistically significant.
Ethical consideration
The study protocol was reviewed and approved by the Ethical Review Committee of the School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar. Written informed consent was obtained from all study participants or their legal representatives after being translated and read in the vernacular language.
Results
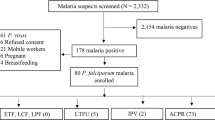
Study participants
A total of 80 patients (46 males and 34 females) were enrolled. Baseline demographics are presented in Table 1. Not a single participant was lost to follow-up. Headache, dizziness, cough, anorexia, and diarrhoea were the most commonly reported adverse events in 26, 15, 25, 12 and 8% of the patients, respectively. Across age groups participants had similar median parasite densities, proportion of gametocyte carriage and mean temperature (Table 1).
Cure rate of AL against uncomplicated Plasmodium falciparum malaria
The PCR-corrected cure rate by Kaplan–Meier analysis was 95.0% (95% CI 87.0–98.4%). Two participants developed ETF on days 2 and 3, respectively. One participant had a LCF on day 14 and three participants developed LPF on days 21 and 28, respectively, out of which two were classified as re-infections based on molecular analysis of paired samples. The remaining 74 patients completed the follow-up without recurrence of parasitaemia (Table 2).
Effect of treatment with AL on parasite, fever, and gametocyte clearance rates
Seventy three point seven five percent, 91.25 and 96.2% of patients cleared their parasites by days 1, 2, and 3, respectively. The overall mean parasite clearance time was 33.6 ± 2.16 h. Seventy five percent, 91.25, and 97.5% of patients cleared their fever on day 1, 2, and 3, respectively. The overall mean fever clearance time was 33 ± 2.020 h. On day 1, all three patients ≤5 years old with gametocytes had cleared their gametocytes where as in the five patients >5 years old gametocytes progressively decreased and completely cleared by day 7 (Table 3).
Parasite densities and temperature at baseline, parasite, fever and gametocyte clearance
Based on parasite density at baseline participants had similar mean fever (P = 0.97) and gametocyte (P = 0.798) clearance times. There was statistically significant association between parasite density at baseline and mean parasite clearance time (P = 0.002) (Table 4).
Based on axillary temperatures at baseline participants had similar mean parasite (P = 0.760), fever (P = 0.329) and mean gametocyte (P = 0.498) clearance time (Table 5).
Discussion
This study suggests that with a cure rate of around 95% AL remains an efficacious treatment for uncomplicated P. falciparum malaria in the region. These results are consistent with studies reported from neighboring Kenya, 96% [25] and Burkina Faso, 96.6% [26] or Togo, 93% [27] and slightly lower than previously reported from e.g. India, 99.9% [28], Senegal, 100% [29], Congo, 100% [30], Tanzania, 100% [31], southern Ethiopia, 99.4% [32] and south-western Ethiopia, 97.5% [33]. Most of these results are well within the confidence intervals of this study and minor differences may be attributable to regional variations in the duration of deployment of AL before the studies were conducted, the age distribution of participants, levels of prevalence (and, therefore, immunity), as well as drug administration practices (e.g. in terms of administering with/without food).
Unlike previous reports from south-western Ethiopia [33], participants in this study ≤5 years old had a slightly, but not significantly (P = 0.18) lower cure rate than those >5 years. At least in part this may be attributable to the fact that the study explicitly did not interfere with the way children are fed and to a low-milk/fat diet typically given to children in the study region, which may have caused poorer absorption and cure rates in small children.
Unlike most previous studies, in this study there were two ETF [32–34]. The two ETF were one male participant 18 years old with parasite densities of 11,000/µl of blood and one male participant 17 years old with parasite densities 10,000/µl. Both had initial parasite densities above the mean and were classified as ETF based on development of severe malaria day 2 in the presence of parasitaemia and parasitaemia on day 3 with axillary temperature ≥37.5°C.
All except seven participants had cleared parasitaemia by day 2. However, four patients (5%; 95% CI 2.0–12.2) were still parasitaemic on day 3 (72 h) after initiation of treatment. All of these patients had initial parasite counts above average and one of them (a 5-year-old female participant with 18,000 parasites/µl) later developed a LCF. This is considered to be well below the threshold indicating potentially emerging resistance and is comparable to previous findings in southern Ethiopia [32] and Burkina Faso [26] and considerably lower than the 21.9% parasitaemic patients on day 3 reported from a trial conducted in western Cambodia as early as 2007 [15]. With only 33.6 h in spite of comparable initial parasite densities the parasite clearance times were also considerable shorter than those seen in Southeast Asia [35].
Clinical improvement was swift and fever clearance was similarly rapid in most of the participants with only three participants (3.75%; 95% CI 1.28–10.45) remaining febrile up to day 3. Fever clearance largely depends on inclusion criteria (e.g. febrile vs. only history of fever) and is, therefore, difficult to compare across study sites but seemed similar to fever clearance reported in previous studies across Africa [26, 30, 36, 37]. All eight participants with gametocytaemia on enrollment had cleared their gametocytes by day 7. Although this may seem faster than some previous reports from Africa, the relatively small number does not allow for conclusions of the potential influence of AL treatment on malaria transmission.
Conclusion
The relatively high cure rate, low proportion of patients still positive on day 3 as well as parasite clearance times in this study would indicate no imminent threat of artemisinin resistance development in the region. Artemether–lumefantrine remains highly efficacious in the treatment of uncomplicated falciparum malaria in small as well as older children and adults. However, the threat of spreading or de novo development of artemisinin resistance warrants regular monitoring of drug efficacy throughout the region.
References
Marcus B, Babcock H (2009) Deadly diseases and epidemics: malaria. Chelsea house, New York, pp 12–13
MMV website (2008) Curing malaria together. [http://www.mmv.org]. Accessed Oct 16
World Health Organization (2014) World malaria report. Available at http://www.who.int/malaria/publications/world_malaria_report_2014/en/. Accessed 27 May 2015
President’s malaria initiative (2013) Malaria operational plan FY 2013. President’s malaria initiative, Ethiopia
Federal Ministry of Health (2006) National five-year strategic plan for malaria prevention and control in Ethiopia 2006–2010. Federal Ministry of Health, Addis Ababa
Adugna A Malaria in Ethiopia. Available at http://www.ethioDemographyAndhealth.org. Accessed 10 Dec 2012
Mitikie G, Addissie M, Admassu M, Tadesse A, Feleke A, Alebachew H (2005) Malaria for the Ethiopian Health Center Team. Gondar College of Medicine and Health Sciences: In: Collaboration with the Ethiopia Public Health Training Initiative, the Carter Center, the Ethiopia Ministry of Health and the Ethiopia Ministry of Education, p 17
Federal Ministry of Health of Ethiopia (2004) Malaria diagnosis and treatment a guideline for health workers in Ethiopia. Federal Ministry of Health, Addis Ababa
Bloland PB (2001) Drug resistance in malaria. World Health Organization. WHO/CDS/CRS/DRS/2001.4
Waller KL, Muhle RA, Ursos LM, Horrocks P, Verdier-Pinard D, Sidhu AB et al (2003) Chloroquine resistance modulated in vitro by expression levels of the Plasmodium falciparum chloroquine resistance transporter. Biol Chem 278:33593–33601
Rosenthal PJ (2001) Antimalarial chemotherapy: mechanism of action, resistance, and new directions in drug discovery. Springer Science + Business Media LLC, Humana Press, New Jersey
World Health Organization (2003) Assessment and monitoring of antimalarial drug efficacy for the treatment of uncomplicated falciparum malaria. World Health Organization, Geneva. http://malaria.who.int/docs/ProtocolWHO.pdf
Makanga M, Krudsood S (2009) The clinical efficacy of artemether/lumefantrine (Coartem®). Malar J 8(Suppl 1):S5
Alemu A, Tsegaye W, Golassa L, Abebe G (2011) Urban malaria and associated risk factors in Jimma town, south-west Ethiopia. Malar J 10:173
Noedl H, Se Y, Schaecher K, Smith BL, Socheat D, Fukuda MM (2008) Artemisinin resistance in Cambodia 1 (ARC1) study consortium. Evidence of artemisinin-resistant malaria in western Cambodia. N Engl J Med 359:2619–2620
Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J (2009) Artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med 361:455–467
Tun KM, Imwong M, Lwin KM, Win AA, Hlaing TM, Hlaing T et al (2015) Spread of artemisinin-resistant Plasmodium falciparum in Myanmar: a cross-sectional survey of the K13 molecular marker. Lancet Infect Dis 15:415–421
Takala-Harrison S, Jacob CG, Arze C, Cummings MP, Silva JC, Dondorp AM et al (2015) Independent emergence of artemisinin resistance mutations among Plasmodium falciparum in Southeast Asia. J Infect Dis 211:670–679
Ashley EA, Dhorda M, Fairhurst RM, Amaratunga C, Lim P, Suon S et al (2014) Spread of artemisinin resistance in Plasmodium falciparum malaria. N Engl J Med 371:411–423
Breman JG (2012) Resistance to artemisinin-based combination therapy. Lancet Infect Dis 12:820–822
WHO (2009) Methods for surveillance of antimalarial drug efficacy. World Health Organization, Geneva
Snounou G, Singh B (2002) Nested PCR analysis of Plasmodium parasites. Methods Mol Med 72:189–203
Fuehrer HP, Stadler MT, Buczolich K, Bloeschl I, Noedl H (2012) Two techniques to simultaneously identify Plasmodium ovale curtisi and P. ovale wallikeri using the small subunit rRNA gene. J Clin Microbiol 50:400–402
Snounou G, Viriyakosol S, Zhu XP (1993) High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol Biochem Parasitol 61:315–320
Worldwide Anti-malarial Resistance Network (WWARN), AL Dose Impact Study Group (2015) The effect of does on the anti-malarial efficacy of artemether–lumefantrine: a systematic review and pooled analysis of individual patient data. Lancet Infect Dis 15:692–702
Juma EA, Obonyo CO, Willis S, Akhwale WS, Ogutu BR (2008) A randomized, open-label, comparative efficacy trial of artemether–lumefantrine suspension versus artemether–lumefantrine tablets for treatment of uncomplicated Plasmodium falciparum malaria in children in western Kenya. Malar J 7:262
Zongo I, Dorsey G, Rouamba N, Dokomajilar C, Séré Y, Rosenthal PJ et al (2007) Randomized comparison of amodiaquine plus sulfadoxine–pyrimethamine, artemether–lumefantrine, and dihydroartemisinin–piperaquine for the treatment of uncomplicated Plasmodium falciparum malaria in Burkina Faso. Clin Infect Dis 45:1453–1461
Dorkenoo MA, Barrette A, Agbo YM, Bogreau H, Kutoati S, Sodahlon YK (2012) Surveillance of the efficacy of artemether–lumefantrine and artesunate–amodiaquine for the treatment of uncomplicated Plasmodium falciparum among children under five in Togo, 2005–2009. Malar J 11:338
Valecha N, Srivastava P, Mohanty SS, Mittra P, Sharma SK, Tyagi PK et al (2009) Therapeutic efficacy of artemether–lumefantrine in uncomplicated falciparum malaria in India. Malar J 8:107
Faye B, Ndiaye JL, Ndiaye D, Dieng Y, Faye O, Gaye O (2007) Efficacy and tolerability of four antimalarial combinations in the treatment of uncomplicated Plasmodium falciparum malaria in Senegal. Malar J 6:80
Van den Broek I, Kitz C, Attas SA, Libama F, Balasegaram M, Guthmann JP (2006) Efficacy of three artemisinin combination therapies for the treatment of uncomplicated Plasmodium falciparum malaria in the Republic of Congo. Malar J 5:113
Kabanywanyi AM, Mwita A, Sumari D, Mandike R, Mugittu K, Abdulla S (2007) Efficacy and safety of artemisinin-based antimalarial in the treatment of uncomplicated malaria in children in southern Tanzania. Malar J 6:146
Eshetu T, Abdo N, Bedru KH, Fekadu S, Wieser A, Pritsch M et al (2012) Open-label trial with artemether–lumefantrine against uncomplicated Plasmodium falciparum malaria three years after its broad introduction in Jimma Zone, Ethiopia. Malar J 11:240
Assefa A, Kassa M, Tadese G, Mohamed H, Animut A, Mengesha T (2010) Therapeutic efficacy of artemether/lumefantrine (Coartem®) against Plasmodium falciparum in Kersa, South West Ethiopia. Parasit Vectors 3:1
Kinfu G, Gebre-Selassie S, Fikrie N (2012) Therapeutic efficacy of artemether–lumefantrine for the treatment of uncomplicated Plasmodium falciparum malaria in northern Ethiopia. Malar Res Treat 2012:548710
Noedl H, Se Y, Sriwichai S, Schaecher K, Teja-Isavadharm P, Smith B et al (2010) Artemisinin resistance in Cambodia: a clinical trial designed to address an emerging problem in Southeast Asia. Clin Infect Dis 51:82–89
Sagara I, Rulisa S, Mbacham W, Adam I, Sissoko K, Maiga H (2009) Efficacy and safety of a fixed dose artesunate–sulphamethoxypyrazine–pyrimethamine compared to artemether–lumefantrine for the treatment of uncomplicated falciparum malaria across Africa: a randomized multi-centre trial. Malar J 8:63
Authors’ contributions
GG, AA and SG conceived the study, contributed in blood sample collection, microscopic diagnosis of malaria slides and patient follow up. HFP and HN undertook molecular analysis of the samples. All authors contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We are grateful to the University of Gondar and MARIB (Malaria Research Initiative Bandarban) for funding this study. The authors wish to thank data collectors at the study site and the study participants for their cooperation in providing the necessary information and blood samples. Furthermore we wish to thank Ingrid Blöschl for their excellent technical support during molecular analysis.
Compliance with ethical guidelines
Competing interests The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Getnet, G., Fola, A.A., Alemu, A. et al. Therapeutic efficacy of artemether–lumefantrine for the treatment of uncomplicated Plasmodium falciparum malaria in Enfranze, north-west Ethiopia. Malar J 14, 258 (2015). https://doi.org/10.1186/s12936-015-0775-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-015-0775-3