
Abstract
Background
Prior studies suggest a link between metabolic dysfunction-associated steatotic liver disease (MASLD) and incident arrhythmias, including atrial fibrillation (AF). However, robust data are lacking from cohorts with liver histology, which remains the gold standard for staging MASLD severity.
Methods
This population-based cohort included all Swedish adults with histologically-confirmed MASLD and without prior cardiac arrhythmias (1966–2016; n = 11,206). MASLD was defined from prospectively-recorded histopathology, and characterized as simple steatosis, non-fibrotic steatohepatitis (MASH), non-cirrhotic fibrosis, or cirrhosis. MASLD patients were matched to ≤ 5 controls without MASLD or arrhythmias, by age, sex, calendar year and county (n = 51,856). Using Cox proportional hazards modeling, we calculated multivariable-adjusted hazard ratios (aHRs) for incident arrhythmias (including AF, bradyarrhythmias, other supraventricular arrhythmias, ventricular arrhythmias/cardiac arrest).
Results
Over a median follow-up of 10.8 years, incident arrhythmias were confirmed in 1351 MASLD patients (10.3/1000 person-years [PY]) and 6493 controls (8.7/1000PY; difference = 1.7/1000PY; aHR = 1.30, 95%CI 1.22–1.38), and MASLD patients had significantly higher rates of incident AF (difference = 0.9/1000PY; aHR = 1.26, 95%CI 1.18–1.35). Rates of both overall arrhythmias and AF were significantly elevated across all MASLD histological groups, particularly cirrhosis (differences, 8.5/1000PY and 5.3/1000PY, respectively). In secondary analyses, MASLD patients also had significantly higher rates of incident ventricular arrhythmias/cardiac arrest (aHR = 1.53, 95%CI 1.30–1.80), bradyarrhythmias (aHR = 1.26, 95%CI 1.06–1.48), and other supraventricular arrhythmias (aHR = 1.27, 95%CI 1.00–1.62), compared to controls.
Conclusions
Compared to matched controls, patients with biopsy-confirmed MASLD had modest but significantly higher incidence of cardiac arrhythmias, including AF, bradyarrhythmias, other supraventricular arrhythmias and ventricular arrhythmias/cardiac arrest. Excess risk was observed across all stages of MASLD and was highest with cirrhosis.
Similar content being viewed by others


Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) represents a leading cause of chronic liver disease in the United States (U.S.) and Europe, where it affects over 100 million adults [1, 2]. Between 20 and 33% of patients with MASLD develop progressive steatohepatitis (MASH) with fibrosis, which in turn may progress to cirrhosis, decompensated liver disease, and liver-related mortality [3,4,5,6,7]. Observational data have also linked MASLD to the development of diverse cardiovascular complications, including coronary atherosclerosis [8, 9], cardiac diastolic dysfunction [10], and both subclinical [8], and overt cardiovascular (CV) events [11, 12]. Based on this body of evidence, both the American Association for the Study of Liver Disease (AASLD) and the European Association for the Study of the Liver (EASL) recommend that patients with MASLD undergo careful cardiovascular screening [13, 14].
Recent data further suggest that MASLD may adversely impact cardiac conduction and autonomic function, and could contribute to the development of cardiac arrhythmias [15, 16], including atrial fibrillation [17, 18], the most common arrhythmia and a cause of significant morbidity and mortality [19]. However, published data are limited and conflicting, with some observational studies reporting increased rates of atrial fibrillation and other arrhythmias in MASLD [20, 21], while others have found conflicting results [17, 22]. Among the few prior studies in this area, all have had substantial limitations, including a focus on prevalent – rather than incident – arrhythmias [23,24,25], or reliance upon surrogate, non-invasive definitions of MASLD [17, 20,21,22], which are prone to misclassification, and cannot identify MASH or fibrosis severity. To date, only one longitudinal study has included liver histology [24], but it derived from a single center and had a small sample size (N = 215), with very few events and limited generalizability.
Thus, we leveraged a nationwide histopathology cohort, comprised of all adults in Sweden with biopsy-confirmed MASLD, to examine the incidence of cardiac arrhythmias according to the presence and histological severity of MASLD.
Methods
Study population and MASLD ascertainment
Within the ESPRESSO (Epidemiology Strengthened by Histopathology Reports in Sweden) cohort, we conducted a population-based, matched cohort study. ESPRESSO encompasses prospectively-recorded liver histopathology submitted to all 28 pathology departments in Sweden between 1965 and 2016 [26]. Each liver biopsy report includes liver biopsy date and location, the unique personal identity number (PIN) assigned to all Swedish residents, and describes topography within the liver and morphology, using the Systematized Nomenclature of Medicine (SNOMED) system. We linked ESPRESSO to validated, nationwide registers that include comprehensive data regarding patient demographics, clinical comorbidities, prescription medications, incident cardiac arrhythmias and death. Informed consent was waived as the study was register-based [27].
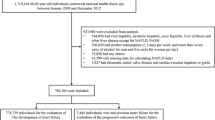
For the current study, we identified all adults aged ≥ 18 years with a liver biopsy between 1966–2016 that confirmed MASLD, as defined as at least one morphology code for steatosis (M5008x or M5520x) without another etiology of liver disease or cardiac arrhythmia, on or before the index date (i.e. date of liver biopsy), using a validated international classification of disease (ICD) algorithm (Additional file 1: Figure S1; eMethods) [12]. As in prior studies, we excluded anyone with another recorded etiology of liver disease, alcohol abuse/misuse, liver transplantation, cardiac arrhythmia or emigration from Sweden, on or before the index date (Additional file 1: Table S1).
In a previous validation study [12], this methodology yielded a positive predictive value (PPV) of 92% for MASLD overall. All patients who met our criteria for MASLD were further classified at the time of their index biopsy into one of four mutually exclusive categories of histological severity (i.e. simple steatosis, MASH, without fibrosis, non-cirrhotic fibrosis and cirrhosis). Specifically, simple steatosis was defined by at least 1 code for steatosis and no additional codes for inflammation (i.e. M5400x or M4-) or fibrosis (i.e. M4900x) or cirrhosis (i.e. M4950x). MASH without fibrosis was defined broadly by the presence of at least 1 code for steatosis plus at least 1 code for inflammation (i.e. M5400x or M4-), without any codes for fibrosis or cirrhosis. Non-cirrhotic fibrosis (i.e. F1-F3 fibrosis, with or without MASH) was defined by the presence of at least 1 code for steatosis plus at least 1 code for fibrosis (i.e. M4900x), but no codes for cirrhosis. Cirrhosis was defined by at least 1 code for cirrhosis (i.e. M4950x). This algorithm has been validated and yielded high positive predictive values (PPV) for each subcategory: simple steatosis (PPV 90%), MASH without fibrosis (PPV 87%), non-cirrhotic fibrosis (PPV 93%), and cirrhosis (PPV 97%) [12]. Each MASLD patient was then subsequently matched to up to five general population controls without recorded MASLD or prior cardiac arrhythmia, according to age, sex, calendar year and county of residence. Population controls were derived from the Total Population Register [28], with identical exclusion criteria (Additional file 1: Figure S1).
Outcomes and covariates
Outcomes and covariates were ascertained from the validated Patient Register, which prospectively records data from all inpatient and outpatient medical facilities in Sweden, including hospital discharge diagnoses (since 1964) and specialty outpatient care (since 2001), with established PPVs for clinical diagnoses between 85 and 95% for liver-related and cardiovascular diseases [29], including PPV of 97% for atrial fibrillation in prior validation studies [30]. The two primary outcomes were: (1) incident overall arrhythmias (a composite defined by ≥ 1 primary or secondary inpatient or outpatient ICD diagnosis for atrial fibrillation or atrial flutter, bradyarrhythmia, other supraventricular arrhythmia, ventricular arrhythmias or cardiac arrest), and (2) incident atrial fibrillation (definitions in Additional file 1: Table S2). In prior validations, such ICD-based algorithms for identifying arrhythmias yield PPVs > 84% [31,32,33,34,35]. Secondary outcomes included other, individual arrhythmias (bradyarrhythmias, other supraventricular arrhythmias, and ventricular arrhythmias/cardiac arrest). In sensitivity analyses we also applied a more stringent definition of arrythmias (requiring ≥ 2 inpatient or outpatient diagnoses separated by > 6 months, with outcome diagnosis date defined by the last diagnosis). Mortality was ascertained from the Total Population Register, which records 93% of all deaths in Sweden within 10 days, and the remaining 7% within 30 days.
Detailed information was collected regarding demographics, education, comorbidities and prescription medication use (Additional file 1: Table S3; eMethods). Briefly, age at the index date (i.e. biopsy date among MASLD patients, or corresponding matching date among controls), sex, date of birth and emigration status were ascertained from the Total Population Register [28], and education level was obtained from the Longitudinal integrated database for health insurance and labour market studies. Data on education were missing for 3.1% of adults with an index date on or after January 1, 1990, which was the first year in which the LISA database was introduced [36]. We included a separate missing category for missingness on education level but did not impute any missing data.
Comorbidities were extracted from the Patient Register using established ICD algorithms [29] (Additional file 1: Table S3; eMethods), and we also identified the number of hospitalizations for each patient in the year preceding the index date. The Total Population Register also includes data from the Multigenerational Register regarding first-degree family members, which permitted us to ascertain a first-degree family history of early cardiovascular disease (CVD) diagnosed before age 50 years. Additionally, we collected detailed data regarding use of the following medications: statins, other lipid-lowering agents, low-dose aspirin (< 163 mg), other anti-platelets, anticoagulants, antidiabetic medications and anti-hypertensive agents [37]. Medication use was ascertained from the Prescribed Drug Register, a well-validated and virtually-complete nationwide register [37], that includes prospectively-recorded data for all dispensed prescriptions from Swedish pharmacies since July, 2005.
Statistical analysis
Our primary analyses examined rates of incident arrhythmias according to the presence and histological severity of MASLD, compared to matched controls. Follow-up began at the index date (or matching date for controls), and continued to the first recorded study outcome, death, emigration, or end of follow-up (December 31, 2016). For all outcomes, we calculated incidence rates and absolute rate differences, together with 95% confidence intervals (CIs). Using cause-specific Cox proportional hazard regression models, we estimated multivariable adjusted hazard ratios (aHRs) and 95%CIs for incident arrhythmias, and defined death due to non-cardiac causes as a potential competing event. The fully-adjusted multivariable model accounted for matching factors (i.e. age, sex, calendar year and county) and a priori-selected confounders defined up to and including the index date (i.e. diabetes, obesity, hypertension, dyslipidemia, chronic kidney disease, a first-degree family history of early CVD before age 50 years, education, number of inpatient hospitalizations in the year before the index date, and finally diagnoses of alcohol abuse/misuse recorded during study follow-up [12]) (eMethods; Additional file 1: Table S3). We did not adjust for heart failure or coronary artery disease since they constitute intermediates but are unlikely to be true confounders [38]. The proportional hazards assumption was assessed by examining the relationship between Schoenfeld residuals and time.
To better characterize the gradient of risk associated with MASLD histological severity, and to minimize potential confounding from misclassification of non-MASLD controls, we restricted the cohort to patients with MASLD, with simple steatosis as the comparator [12]. In stratified analyses, we examined the associations between MASLD and incident arrhythmias according to sex, and categories of age, follow-up duration, and calendar year of index biopsy, and we tested the significance of effect modification between J groups using the contrast test statistic, which approximates a chi-squared distribution with J-1 degrees of freedom under the null. [39]
To assess potential confounding related to shared genetic or early environmental factors, including a first-degree family history of early CVD, we identified all MASLD patients with ≥ 1 full sibling without recorded MASLD or arrhythmia before the start of follow-up, and otherwise applied identical exclusion criteria. We then compared each MASLD patient with his or her full sibling(s), after conditioning on matching set within family, and further adjusting for all covariates in the multivariable model.
We conducted several sensitivity analyses to test the robustness of our results. First, because a widely-used histological scoring system was published in 2005 [40], the same year that comprehensive prescription medication data was first available in Sweden, we restricted the cohort to patients with index date ≥ January 1, 2006, and constructed models further accounting for relevant medication use (i.e. aspirin, other antiplatelets, statins, other lipid-lowering agents, antidiabetic agents and/or anti-hypertensive medications). Second, because we lacked detailed data regarding smoking, we also constructed models further adjusting for chronic obstructive pulmonary disease (COPD), as a proxy for heavy smoking. Third, we computed an “E-value” [41], which is the minimum strength of the association that an unmeasured confounder would need to have with both the exposure and the outcome, to fully attenuate the observed association between MASLD and the study outcome. Fourth, because a diagnosis of underlying CVD might mediate an association between MASLD and incident cardiac arrhythmias, we constructed separate multivariable models focused on primary arrhythmias, by excluding patients with prior, underlying CVD, and further censoring patients during follow-up at the time of a CVD diagnosis. Finally, to address potential reverse causation, we repeated our analysis after excluding patients with incident arrhythmias recorded within < 90 days or within < 2 years of follow-up (with follow-up therefore starting at day 90 or at 2 years, respectively).
Analyses were conducted using R software (version 3.6.1, R Foundation for Statistical Computing, Vienna, Austria; survival package version 2.44 [Therneau, 2015, https://CRAN.R-project.org/package=survival]). A two-sided P < 0.05 was considered statistically significant.
Role of the funding source
No funding organization had any role in the design and conduct of the study; in the collection, management, and analysis of the data; or in the preparation, review, and approval of the manuscript.
Results
Table 1 outlines the baseline characteristics of 11,206 adults with histologically-confirmed MASLD and 51,856 matched general population controls. Among MASLD patients, the average age at index biopsy was 53 years, and 45% were female. Simple steatosis was found in 7,642 (68.2%), while 1,257 (11.2%) had MASH without fibrosis, 1695 (15.1%) had non-cirrhotic fibrosis, and 612 (5.5%) had cirrhosis. MASLD patients were more likely than controls to have diabetes, obesity, hypertension, dyslipidemia and chronic kidney disease.
Overall arrhythmias
Over 10.8 years of median follow-up, we confirmed 1,351 incident arrhythmias among MASLD patients (10.3/ 1000 person-years (PY)), and 6,493 incident arrhythmias among controls (8.7/1000PY; absolute rate difference, 1.7/1000PY, 95%CI 1.1–2.2)(Fig. 1; Table 2). After multivariable adjustment, MASLD patients had a significant, 1.30-fold higher rate of developing an incident arrhythmia, compared to controls (95%CI = 1.22–1.38), and significantly higher rates were observed across all MASLD histological categories (Fig. 1; Table 2). Specifically, compared to controls, the absolute rate differences and corresponding aHRs were significantly higher in patients with simple steatosis (1.1/1000PY; aHR = 1.28, 95%CI 1.19–1.38), non-fibrotic MASH (1.3/1000PY; aHR = 1.33, 95%CI 1.09–1.61), non-cirrhotic fibrosis (3.3/1000PY; aHR = 1.25, 95%CI 1.05–1.48) and cirrhosis (8.5/1000PY; aHR 1.60, 95%CI 1.21–2.12).

Cumulative Incidence of Arrhythmias According to the Presence and Histologic Severity of MASLD. MASLD metabolic dysfunction-associated steatotic liver disease; MASH metabolic dysfunction-associated steatohepatitis *Incident arrhythmias was a composite endpoint that included incident atrial fibrrillation or atrial flutter, bradyarrhythmias, other supraventricular arrhythmias, or ventricular arrhythmias or cardiac arrest (for definitions and details, see Additional file 1: Table S3)
In stratified analyses, the association between MASLD and incident overall arrhythmias was significantly higher in patients diagnosed with MASLD < 40 years of age (aHR = 2.22, 95%CI 1.80–2.74), compared to those diagnosed later in adulthood (aHR for 40–59 years = 1.30, 95%CI 1.18–1.42; aHR for > = 60 years = 1.23, 95%CI 1.13–1.34; p-interaction < 0.001)( Additional file 1: Table S4). Otherwise, associations did not differ significantly by sex, duration of follow-up, or between patients with and without underlying metabolic comorbidities (p-interactions all > 0.05).
Atrial fibrillation
Compared to controls, MASLD patients had modest but significantly higher rates of incident atrial fibrillation (difference, 0.9/1000PY; aHR = 1.26, 95%CI 1.18–1.35)(Table 2). These differences were observed across all MASLD histological categories, when compared to controls, including for simple steatosis (aHR = 1.24, 95%CI 1.14–1.35), non-fibrotic MASH (aHR = 1.34, 95%CI 1.07–1.68), non-cirrhotic fibrosis (aHR = 1.24, 95%CI 1.03–1.50) and cirrhosis (aHR = 1.59, 95%CI 1.15–2.19).
Individual arrhythmia outcomes
Compared to controls, MASLD patients also had significantly higher rates of developing incident bradyarrhythmias (difference, 0.2/1000PY; aHR = 1.26, 95%CI 1.06–1.48), other supraventricular arrhythmias (difference, 0.1/1000PY; aHR = 1.27, 95%CI 1.00–1.62) and ventricular arrhythmias/cardiac arrest (difference, 0.6/1000PY; aHR = 1.53, 95%CI 1.30–1.80) (Additional file 1: Table S5). In further exploratory analyses, we assessed those individual arrhythmia outcomes according to MASLD histological categories (Additional file 1: Table S5); however, those findings merit cautious interpretation, given the small numbers in each subgroup.
MASLD-only subgroup
When compared to patients with simple steatosis, those with more advanced MASLD fibrosis had significantly higher rates of incident arrhythmias (absolute differences for non-cirrhotic fibrosis and for cirrhosis, 2.3/1000PY and 7.5/1000PY, respectively; Table 3). After multivariable adjustment, this corresponded to a 32% higher rate of incident arrhythmias in patients with cirrhosis, compared to those with simple steatosis (aHR = 1.32, 95%CI 1.04–1.66). Findings were similar in analyses focused on incident atrial fibrillation (differences for non-cirrhotic fibrosis and cirrhosis, each compared to simple steatosis: 2.3/1000PY and 7.5/1000PY, respectively). In contrast, no significant differences in either overall arrhythmias or in atrial fibrillation were observed, when non-fibrotic MASH was compared directly with simple steatosis.
Sibling analyses
To address potential residual confounding related to shared genetic and intrafamilial factors, we re-matched 4,686 MASLD patients to 8,736 full-sibling comparators who were alive at the index date and had no diagnoses of MASLD or arrhythmia (Additional file 1: Table S6). Consistent with our primary analysis, MASLD patients again demonstrated significantly higher rates of incident overall arrhythmias, compared to matched full siblings (difference, 2.3/1000PY; aHR = 1.34, 95%CI 1.15–1.56), including higher rates of incident atrial fibrillation (difference, 1.6/1000PY; aHR = 1.32, 95%CI 1.11–1.58). In analyses of the individual arrhythmia outcomes, we found that MASLD patients had significantly higher rates of incident ventricular arrhythmias/cardiac arrest, compared to full sibling controls (difference, 0.6/1000PY; aHR = 1.89, 95%CI 1.25–2.86), but no significant differences were observed for bradyarrhythmias or other supraventricular arrhythmias.
Sensitivity Analyses
Our findings were robust across all sensitivity analyses, including after restricting the cohort to MASLD patients with index biopsy ≥ January 1, 2006 (n = 2375) and matched controls (n = 9757), and further adjusting for use of relevant medications (differenceoverall arrhythmias for MASLD vs. controls = 3.5/1000PY; aHR = 1.47, 95%CI 1.20–1.81]; Additional file 1: Table S7). Similarly, our findings persisted after further adjusting for COPD as a proxy for smoking (aHRoverall arrhythmias = 1.29, 95%CI 1.21–1.37), and also after excluding any patient with a cardiac arrhythmia outcome within < 90 days of follow-up (aHRoverall arrhythmias = 1.28, 95%CI 1.20–1.36; Additional file 1: Table S8) or within < 2 years (aHRoverall arrhythmias = 1.27; 95%CI 1.19–1.36; Additional file 1: Table S9). Moreover, our results were similar in analyses focused on primary cardiac arrhythmias (i.e. after excluding any patient with underlying CVD at baseline, and further censoring patients with incident CVD diagnosed during follow-up: aHRoverall arrhythmias = 1.29, 95%CI 1.19–1.40 Additional file 1: Table S10). Finally, we estimated the “E-value” using the approach by VanderWeele et al [41], and found that an unmeasured confounder would need to have a multivariable-adjusted HR of at least 1.92 or more for both the exposure and outcome, to attenuate the observed association between MASLD and incident arrhythmias to 1.0. For cirrhosis, this E-value would need to be at least 2.58 or more.
Discussion
In this population-based cohort comprised of all Swedish adults with biopsy-confirmed MASLD and matched general population controls, MASLD was associated with significantly higher rates of both fatal and non-fatal cardiac arrhythmias, including atrial fibrillation, bradyarrhythmias, other supraventricular arrhythmias and ventricular arrhythmias/cardiac arrest. Compared to controls, MASLD patients had a 30% higher relative risk of developing an arrhythmia, and an absolute excess rate of 1.7 per 1000PY, which corresponds to one additional, incident cardiac arrhythmia per each 29 patients diagnosed with MASLD over 20 years. Rates of incident overall arrhythmias and atrial fibrillation were significantly elevated across all MASLD histological categories, and they were highest in patients with cirrhosis, who demonstrated striking, 17-fold higher rates of developing an incident cardiac arrhythmia—including 12-fold higher rates of incident atrial fibrillation—compared to controls. Importantly, these findings were robust across numerous sensitivity analyses, including after accounting for cardiometabolic risk factors, use of relevant medications, other causes of death, and after comparing MASLD patients with full siblings, to address important, shared genetic, intrafamilial and socioeconomic factors.
Currently, longitudinal evidence linking MASLD to the development of incident cardiac arrhythmias, including atrial fibrillation, is limited. While a recent meta-analysis of six longitudinal studies found a significant, 19% higher risk of incident atrial fibrillation in patients with MASLD compared to non-MASLD controls (pooled HR = 1.19, 95%CI 1.07–1.31) [18], a prior meta-analysis and recent observational community-based cohort [17, 22] found null associations. However, all prior studies have been significantly limited by small sample sizes, cross-sectional design [24], or reliance upon surrogate definitions of MASLD, including laboratory-based algorithms [42], ultrasound [20, 21] or computed tomography [22], which lack precision and cannot identify MASH or stage fibrosis. In fact, the largest studies to date have identified people with MASLD using the fatty liver index—an algorithm based on BMI, waist circumference, triglycerides and GGT—which is not specific for MASLD but rather reflects the association with obesity. In contrast, the current study derived from a large, nationwide cohort with detailed liver histology, and long follow-up for incident arrhythmia events. Thus, our data provide strong evidence that MASLD is associated with modest albeit significantly increased rates of developing incident arrhythmias, including atrial fibrillation.
Currently, little is known about the impact of MASLD histological severity on risk of developing incident cardiac arrhythmias [17]. In the current study, we found that the incidence of arrhythmias including atrial fibrillation were significantly elevated across all MASLD histological groups, including in patients with earlier stages of non-fibrotic MASLD. Nevertheless, among patients with MASLD, we found that patients with non-cirrhotic fibrosis or cirrhosis had markedly higher absolute rates of developing incident arrhythmias, when compared to simple steatosis (absolute differences, 2.3 and 7.5 per 1000PY, respectively). Over 20 years, those rate differences correspond to one additional, incident cardiac arrhythmia diagnosis per each 22 patients with non-cirrhotic fibrosis, and one additional arrythmia diagnosis per each 7 patients with cirrhosis. In contrast, rates of incident arrhythmias did not appear to differ between patients with non-fibrotic MASH and simple steatosis. Collectively, these data suggest that advanced MASLD fibrosis is an important predictor of incident arrhythmias, including atrial fibrillation.
Although the precise mechanism is undefined, preclinical and preliminary clinical studies suggest that MASLD may contribute to cardiac arrhythmia risk by promoting cardiac remodeling [10], autonomic dysfunction [43,44,45], and/or electrical remodeling [46]. For example, MASLD has been linked to cardiac sympathetic/parasympathetic dysregulation [47], impaired heart rate variability [45], and also to QTc interval [48,49,50] and cardiac conduction abnormalities [48, 51], and a higher risk of recurrent atrial fibrillation after ablation [52]. Furthermore, advanced liver disease at the stage of cirrhosis is known to considerably impair cardiac function via a hyperdynamic circulation and vasodilation, what has been termed “cirrhotic cardiomyopathy” [53]. In addition, MASLD represents a complex, multi-system disease, and it is still unclear whether MASLD represents a causal driver of cardiac arrhythmias, or whether it might simply reflect other, shared cardiometabolic risk factors. Importantly, we lacked data on BMI for the current study, which is an established risk factor for both MASLD and atrial fibrillation; however, evidence suggests that each 5-unit increase in BMI above the normal range confers a 19%-29% increased relative risk of incident atrial fibrillation [54]. Thus, our sensitivity analysis for unmeasured confounding (E-value = 1.92) would suggest that the association between MASLD and incident arrhythmias is unlikely to be fully explained by obesity; nevertheless, future large-scale cohorts with detailed assessments of adiposity are needed, to fully characterize this relationship.
Strengths of this study include a large, nationwide population with comprehensive and prospectively-recorded histopathology data, and strict, validated definitions of both MASLD [12] and confounding variables, in registers with near-complete follow-up for the entire Swedish population. Our large sample size permitted calculation of more precise risk estimates across the MASLD histological spectrum, which was not possible in previous, smaller studies, and allowed us to account for cardiometabolic risk factors and potential confounders. We also applied robust techniques to address potential residual confounding, misclassification of non-MASLD controls, and potential competing events.
Study limitations
We acknowledge several limitations. First, this was a retrospective study of biopsy-confirmed MASLD, which could introduce selection bias. However, our risk estimates are highly consistent with the largest meta-analysis to date [18], which was comprised of smaller cohorts that defined MASLD using non-invasive approaches, highlighting the generalizability of our findings. Second, while it is possible that our controls could have included patients with undiagnosed MASLD, our findings were consistent in the MASLD-only subgroup. Third, despite careful matching, residual confounding is possible, and we lacked detailed laboratory data or information regarding smoking status, alcohol consumption, or BMI. Nevertheless, our findings were robust after multivariable adjustment for important risk factors, including clinical comorbidities, subsequent alcohol use disorders and COPD − as a proxy for heavy smoking, relevant medication use, and even a first-degree family history of cardiovascular disease. Moreover, after re-matching MASLD patients with full siblings to address shared intrafamilial and early-life factors, the associations were confirmed. Finally, the Swedish population is primarily Caucasian, highlighting the need for additional research in more diverse, large-scale histology cohorts.
In conclusion, within this large nationwide cohort of 11,206 adults with biopsy-confirmed MASLD and matched population controls, MASLD was associated with modest but significantly higher incidence of both fatal and non-fatal arrhythmias, including atrial fibrillation, bradyarrhythmias, other supraventricular arrhythmias and ventricular arrhythmias/cardiac arrest. Our study provides quantitative estimates regarding rates of incident arrhythmias according to the presence and histological severity of MASLD, for the first time on a nationwide scale. The incidence of arrhythmias, including atrial fibrillation, was significantly elevated across all stages of MASLD, particularly in cirrhosis. Thus, our results provide strong support for additional research to understand the mechanisms that link MASLD and fibrosis to the development of arrhythmias, and also to identify which high-risk patients with MASLD might benefit from increased surveillance or early interventions.
Availability of data and materials
No additional data are available due to Swedish regulations.
Abbreviations
- aHR:
-
Adjusted hazard ratio
- AF:
-
Atrial fibrillation
- CV:
-
Cardiovascular
- CVD:
-
Cardiovascular disease
- CI:
-
Confidence interval
- ESPRESSO:
-
Epidemiology Strengthened by histoPathology Reports in Sweden
- ICD:
-
International classification of diseases
- MASLD:
-
Metabolic dysfunction-associated steatotic liver disease
- MASH:
-
Metabolic dysfunction-associated steatohepatitis
- NAFLD:
-
Nonalcoholic fatty liver disease
- NASH:
-
Nonalcoholic steatohepatitis
- PPV:
-
Positive predictive value
- PY:
-
Person-Years
References
Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. https://doi.org/10.1002/hep.28431[publishedOnlineFirst:20160222].
Adams LA, Lindor KD. Nonalcoholic fatty liver disease. Ann Epidemiol. 2007;17(11):863–9. https://doi.org/10.1016/j.annepidem.2007.05.013[publishedOnlineFirst:2007/08/31].
Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 2011;34(3):274–85. https://doi.org/10.1111/j.1365-2036.2011.04724.x[publishedOnlineFirst:20110530].
Taylor RS, Taylor RJ, Bayliss S, et al. Association between fibrosis stage and outcomes of patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Gastroenterology. 2020. https://doi.org/10.1053/j.gastro.2020.01.043[publishedOnlineFirst:2020/02/07].
Dulai PS, Singh S, Patel J, et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology. 2017;65(5):1557–65. https://doi.org/10.1002/hep.29085[publishedOnlineFirst:20170331].
Kleiner DE, Brunt EM, Wilson LA, et al. Association of histologic disease activity with progression of nonalcoholic fatty liver disease. JAMA Netw Open. 2019;2(10): e1912565. https://doi.org/10.1001/jamanetworkopen.2019.12565[publishedOnlineFirst:2019/10/05].
McPherson S, Hardy T, Henderson E, et al. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol. 2015;62(5):1148–55. https://doi.org/10.1016/j.jhep.2014.11.034[publishedOnlineFirst:20141201].
Mellinger JL, Pencina KM, Massaro JM, et al. Hepatic steatosis and cardiovascular disease outcomes: an analysis of the Framingham heart study. J Hepatol. 2015;63(2):470–6. https://doi.org/10.1016/j.jhep.2015.02.045[publishedOnlineFirst:2015/03/18].
Salvi P, Ruffini R, Agnoletti D, et al. Increased arterial stiffness in nonalcoholic fatty liver disease: the cardio-GOOSE study. J Hypertens. 2010;28(8):1699–707. https://doi.org/10.1097/HJH.0b013e32833a7de6[publishedOnlineFirst:2010/05/15].
Simon TG, Bamira DG, Chung RT, et al. Nonalcoholic steatohepatitis is associated with cardiac remodeling and dysfunction. Obesity. 2017;25(8):1313–6. https://doi.org/10.1002/oby.21879[publishedOnlineFirst:2017/07/27].
Targher G, Byrne CD, Lonardo A, et al. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol. 2016;65(3):589–600. https://doi.org/10.1016/j.jhep.2016.05.013[publishedOnlineFirst:2016/05/24].
Simon TG, Roelstraete B, Khalili H, et al. Mortality in biopsy-confirmed nonalcoholic fatty liver disease: results from a nationwide cohort. Gut. 2021;70(7):1375–82. https://doi.org/10.1136/gutjnl-2020-322786[publishedOnlineFirst:20201009].
Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American association for the study of liver diseases. Hepatology. 2018;67(1):328–57. https://doi.org/10.1002/hep.29367[publishedOnlineFirst:20170929].
European Association for the Study of the L, European Association for the Study of D, European Association for the Study of O. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol 2016; 64(6):1388–402. doi: https://doi.org/10.1016/j.jhep.2015.11.004
Mantovani A, Rigamonti A, Bonapace S, et al. Nonalcoholic fatty liver disease is associated with ventricular arrhythmias in patients with type 2 diabetes referred for clinically indicated 24-hour holter monitoring. Diabetes Care. 2016;39(8):1416–23. https://doi.org/10.2337/dc16-0091[publishedOnlineFirst:20160523].
Mantovani A, Csermely A, Taverna A, et al. Association between metabolic dysfunction-associated fatty liver disease and supraventricular and ventricular tachyarrhythmias in patients with type 2 diabetes. Diabetes Metab. 2023;49(2): 101416. https://doi.org/10.1016/j.diabet.2022.101416[publishedOnlineFirst:20221228].
Mantovani A, Dauriz M, Sandri D, et al. Association between non-alcoholic fatty liver disease and risk of atrial fibrillation in adult individuals: an updated meta-analysis. Liver Int. 2019;39(4):758–69. https://doi.org/10.1111/liv.14044[publishedOnlineFirst:2019/01/19].
Cai X, Zheng S, Liu Y, et al. Nonalcoholic fatty liver disease is associated with increased risk of atrial fibrillation. Liver Int. 2020;40(7):1594–600. https://doi.org/10.1111/liv.14461[publishedOnlineFirst:2020/04/13].
Lip GY, Tse HF, Lane DA. Atrial fibrillation. Lancet. 2012;379(9816):648–61. https://doi.org/10.1016/S0140-6736(11)61514-6[publishedOnlineFirst:2011/12/15].
Targher G, Valbusa F, Bonapace S, et al. Non-alcoholic fatty liver disease is associated with an increased incidence of atrial fibrillation in patients with type 2 diabetes. PLoS ONE. 2013;8(2): e57183. https://doi.org/10.1371/journal.pone.0057183[publishedOnlineFirst:2013/03/02].
Karajamaki AJ, Patsi OP, Savolainen M, et al. Non-alcoholic fatty liver disease as a predictor of atrial fibrillation in middle-aged population (OPERA study). PLoS ONE. 2015;10(11): e0142937. https://doi.org/10.1371/journal.pone.0142937[publishedOnlineFirst:2015/11/17].
Long MT, Yin X, Larson MG, et al. Relations of liver fat with prevalent and incident atrial fibrillation in the Framingham heart study. J Am Heart Assoc. 2017. https://doi.org/10.1161/JAHA.116.005227.
Markus MR, Meffert PJ, Baumeister SE, et al. Association between hepatic steatosis and serum liver enzyme levels with atrial fibrillation in the general population: the study of health in Pomerania (SHIP). Atherosclerosis. 2016;245:123–31. https://doi.org/10.1016/j.atherosclerosis.2015.12.023[publishedOnlineFirst:2016/01/02].
Whitsett M, Wilcox J, Yang A, et al. Atrial fibrillation is highly prevalent yet undertreated in patients with biopsy-proven nonalcoholic steatohepatitis. Liver Int. 2019;39(5):933–40. https://doi.org/10.1111/liv.14018[publishedOnlineFirst:2018/12/12].
Zhang Y, Li P, Miao M, et al. Nonalcoholic fatty liver disease is associated with increased atrial fibrillation risk in an elderly Chinese population: a cross-sectional study. Biomed Res Int. 2018;2018:5628749. https://doi.org/10.1155/2018/5628749[publishedOnlineFirst:2018/08/17].
Ludvigsson JF, Lashkariani M. Cohort profile: ESPRESSO (epidemiology strengthened by histopathology reports in Sweden). Clin Epidemiol. 2019;11:101–14. https://doi.org/10.2147/CLEP.S191914[publishedOnlineFirst:20190114].
Ludvigsson JF, Haberg SE, Knudsen GP, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491–508. https://doi.org/10.2147/CLEP.S90589[publishedOnlineFirst:20151123].
Ludvigsson JF, Almqvist C, Bonamy AK, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125–36. https://doi.org/10.1007/s10654-016-0117-y[publishedOnlineFirst:20160114].
Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450. https://doi.org/10.1186/1471-2458-11-450[publishedOnlineFirst:20110609].
Smith JG, Platonov PG, Hedblad B, et al. Atrial fibrillation in the malmo diet and cancer study: a study of occurrence, risk factors and diagnostic validity. Eur J Epidemiol. 2010;25(2):95–102. https://doi.org/10.1007/s10654-009-9404-1[publishedOnlineFirst:2009/11/26].
Antani MR, Beyth RJ, Covinsky KE, et al. Failure to prescribe warfarin to patients with nonrheumatic atrial fibrillation. J Gen Intern Med. 1996;11(12):713–20. https://doi.org/10.1007/BF02598984[publishedOnlineFirst:1996/12/01].
Brass LM, Krumholz HM, Scinto JM, et al. Warfarin use among patients with atrial fibrillation. Stroke. 1997;28(12):2382–9. https://doi.org/10.1161/01.str.28.12.2382[publishedOnlineFirst:1997/12/31].
Flaker GC, McGowan DJ, Boechler M, et al. Underutilization of antithrombotic therapy in elderly rural patients with atrial fibrillation. Am Heart J. 1999;137(2):307–12. https://doi.org/10.1053/hj.1999.v137.91403[publishedOnlineFirst:1999/01/30].
Shen AY, Yao JF, Brar SS, et al. Racial/Ethnic differences in ischemic stroke rates and the efficacy of warfarin among patients with atrial fibrillation. Stroke. 2008;39(10):2736–43. https://doi.org/10.1161/STROKEAHA.107.508580[publishedOnlineFirst:2008/07/19].
Jensen PN, Johnson K, Floyd J, et al. A systematic review of validated methods for identifying atrial fibrillation using administrative data. Pharmacoepidemiol Drug Saf. 2012;21(Suppl 1):141–7. https://doi.org/10.1002/pds.2317[publishedOnlineFirst:2012/01/25].
Ludvigsson JF, Svedberg P, Olen O, et al. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34(4):423–37. https://doi.org/10.1007/s10654-019-00511-8[publishedOnlineFirst:20190330].
Wettermark B, Hammar N, Fored CM, et al. The new Swedish prescribed drug register–opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf. 2007;16(7):726–35. https://doi.org/10.1002/pds.1294.
Rothman KJ, Greenland S, Lash TL. Modern Epidemiology: Wolters Kluwer Health/Lippincott Williams & Wilkins 2015.
Wang M, Spiegelman D, Kuchiba A, et al. Statistical methods for studying disease subtype heterogeneity. Stat Med. 2016;35(5):782–800. https://doi.org/10.1002/sim.6793[publishedOnlineFirst:2015/12/02].
Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–21. https://doi.org/10.1002/hep.20701.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–74. https://doi.org/10.7326/M16-2607[publishedOnlineFirst:20170711].
Roh JH, Lee JH, Lee H, et al. Association between non-alcoholic fatty liver disease and risk of new-onset atrial fibrillation in healthy adults. Liver Int. 2020;40(2):338–46. https://doi.org/10.1111/liv.14236[publishedOnlineFirst:2019/09/04].
Liu YC, Hung CS, Wu YW, et al. Influence of non-alcoholic fatty liver disease on autonomic changes evaluated by the time domain, frequency domain, and symbolic dynamics of heart rate variability. PLoS ONE. 2013;8(4): e61803. https://doi.org/10.1371/journal.pone.0061803[publishedOnlineFirst:2013/04/30].
Cho KI, Jo EA, Cho SH, et al. The influence of epicardial fat and nonalcoholic fatty liver disease on heart rate recovery in metabolic syndrome. Metab Syndr Relat Disord. 2017;15(5):226–32. https://doi.org/10.1089/met.2016.0132[publishedOnlineFirst:2017/03/28].
Houghton D, Zalewski P, Hallsworth K, et al. The degree of hepatic steatosis associates with impaired cardiac and autonomic function. J Hepatol. 2019;70(6):1203–13. https://doi.org/10.1016/j.jhep.2019.01.035[publishedOnlineFirst:2019/02/16].
Ozveren O, Izgi C, Eroglu E, et al. Doppler tissue evaluation of atrial conduction properties in patients with non-alcoholic fatty-liver disease. Ultrason Imaging. 2016;38(3):225–35. https://doi.org/10.1177/0161734615595015[publishedOnlineFirst:2015/07/15].
Targher G, Mantovani A, Grander C, et al. Association between non-alcoholic fatty liver disease and impaired cardiac sympathetic/parasympathetic balance in subjects with and without type 2 diabetes-the cooperative health research in south tyrol (CHRIS)-NAFLD sub-study. Nutr Metab Cardiovasc Dis. 2021;31(12):3464–73. https://doi.org/10.1016/j.numecd.2021.08.037[publishedOnlineFirst:2021/10/11].
Anstee QM, Mantovani A, Tilg H, et al. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2018;15(7):425–39. https://doi.org/10.1038/s41575-018-0010-0[publishedOnlineFirst:2018/05/02].
Targher G, Tilg H, Byrne CD. Non-alcoholic fatty liver disease: a multisystem disease requiring a multidisciplinary and holistic approach. Lancet Gastroenterol Hepatol. 2021;6(7):578–88. https://doi.org/10.1016/S2468-1253(21)00020-0[publishedOnlineFirst:2021/05/08].
Targher G, Valbusa F, Bonapace S, et al. Association of nonalcoholic fatty liver disease with QTc interval in patients with type 2 diabetes. Nutr Metab Cardiovasc Dis. 2014;24(6):663–9. https://doi.org/10.1016/j.numecd.2014.01.005[publishedOnlineFirst:20140121].
Mantovani A, Rigolon R, Pichiri I, et al. Nonalcoholic fatty liver disease is associated with an increased risk of heart block in hospitalized patients with type 2 diabetes mellitus. PLoS ONE. 2017;12(10): e0185459. https://doi.org/10.1371/journal.pone.0185459[publishedOnlineFirst:20171005].
Donnellan E, Cotter TG, Wazni OM, et al. Impact of nonalcoholic fatty liver disease on arrhythmia recurrence following atrial fibrillation ablation. JACC Clin Electrophysiol. 2020;6(10):1278–87. https://doi.org/10.1016/j.jacep.2020.05.023[publishedOnlineFirst:2020/10/24].
Moller S, Wiese S, Barlose M, et al. How non-alcoholic fatty liver disease and cirrhosis affect the heart. Hepatol Int. 2023. https://doi.org/10.1007/s12072-023-10590-1[publishedOnlineFirst:20230928].
Wong CX, Sullivan T, Sun MT, et al. Obesity and the risk of incident, post-operative, and post-ablation atrial fibrillation: a meta-analysis of 626,603 individuals in 51 studies. JACC Clin Electrophysiol. 2015;1(3):139–52. https://doi.org/10.1016/j.jacep.2015.04.004[publishedOnlineFirst:2015/06/01].
Acknowledgements
None.
Transparency statement
Dr. Simon affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding
Open access funding provided by Karolinska Institute. TGS was supported by NIH K23 DK122104. FE was supported by the Swiss National Science Foundation (SNSF) P500PM_210866. HH was supported by Grants from Region Stockholm (CIMED), The Swedish Research Council, Radiumhemmet Research Foundation and The Swedish Cancer Society. JFL was supported by the Karolinska Institutet. No funding organization had any role in the design and conduct of the study; in the collection, management, and analysis of the data; or in the preparation, review, and approval of the manuscript.
Author information
Authors and Affiliations
Contributions
Guarantor: The corresponding author (JFL) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: All co-authors. Acquisition of data: JFL. Analysis: BR. Interpretation of data: All co-authors. Writing first draft of the manuscript: TGS and JFL. Critical revision of the manuscript for important intellectual content and approval of final version: All co-authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Review Board in Stockholm, Sweden (2014/1287-31/4, 2018/972-32 and 2022-05774-02).
Consent for publication
Not applicable.
Competing interests
All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work. TGS has received research funding from Amgen and has received consulting fees from Aetion, for work unrelated to this manuscript. FE has served as advisory board member for Boehringer Ingelheim. HH reports research grants to his institution from Astra Zeneca, Pfizer, Merck, EchoSens, Intercept and Gilead, and board advisory for Bristol-Myers Squibb and Gilead. JS reports ownership in companies providing services to Itrim, Amgen, Janssen, Novo Nordisk, Eli Lilly, Boehringer, Bayer, Pfizer and AstraZeneca, outside the submitted work. JFL coordinates an unrelated study on behalf of the Swedish IBD quality register (SWIBREG), that has received funding from Janssen corporation. The remaining authors have no disclosures and no conflicts of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Study Exclusion Criteria. Table S2. Definitions of Primary and Secondary Outcomes. Table S3. Definitions of Covariates and Prescription Medications. Table S4. Stratified Models for the Primary Overall Arrhythmia Outcome. Table S5. Secondary Arrhythmia Outcomes among Adults with Histologically-Confirmed MASLD and Matched Population Controls. Table S6. Incident Overall Arrhythmias and Atrial Fibrillation among MASLD Patients and Matched Full Sibling Comparators. Table S7. Incident Arrhythmia Outcomes among Adults with Histologically-Confirmed MASLD and Matched Population Controls from 2006-2016 with Comprehensive Prescription Medication Use Data. Table S8. Incident Cardiac Arrhythmias among MASLD Patients and Matched Population Controls, after Excluding Patients with a Primary Outcome Within <90 Days. Table S9.Incident Cardiac Arrhythmias among MASLD Patients and Matched Population Controls, after Excluding Patients with a Primary Outcome Within <2 years. Table S10. Incident Primary Cardiac Arrhythmias among MASLD Patients and Matched Population Controls, after Excluding Patients with Underlying CVD and Censoring at the Date of CVD Diagnoses in Follow-up. Figure S1. Cohort Construction
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Simon, T.G., Ebrahimi, F., Roelstraete, B. et al. Incident cardiac arrhythmias associated with metabolic dysfunction-associated steatotic liver disease: a nationwide histology cohort study. Cardiovasc Diabetol 22, 343 (2023). https://doi.org/10.1186/s12933-023-02070-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-02070-5