
Abstract
Aims
To examine the joint association of diabetes status and N-terminal pro-B-type natriuretic peptide (NT-proBNP) with subsequent risk of major adverse cardio-cerebral events (MACCEs) and all-cause mortality in patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS).
Methods
A total of 7956 NSTE-ACS patients recruited from the Cardiovascular Center Beijing Friendship Hospital Database Bank were included in this cohort study. Patients were divided into nine groups according to diabetes status (normoglycemia, prediabetes, diabetes) and NT-proBNP tertiles (< 92 pg/ml, 92–335 pg/ml, ≥ 336 pg/ml). Multivariable Cox proportional hazards models were used to estimate the individual and joint association of diabetes status and NT-proBNP with the risk of MACCEs and all-cause mortality.
Results
During 20,257.9 person-years of follow-up, 1070 MACCEs were documented. In the fully adjusted model, diabetes and a higher level of NT-proBNP were independently associated with MACCEs risk (HR 1.42, 95% CI: 1.20–1.68; HR 1.72, 95% CI: 1.40–2.11) and all-cause mortality (HR 1.37, 95% CI: 1.05–1.78; HR 2.80, 95% CI: 1.89–4.17). Compared with patients with normoglycemia and NT-proBNP < 92 pg/ml, the strongest numerical adjusted hazards for MACCEs and all-cause mortality were observed in patients with diabetes and NT-proBNP ≥ 336 pg/ml (HR 2.67, 95% CI: 1.83–3.89; HR 2.98, 95% CI: 1.48–6.00). The association between MACCEs and all-cause mortality with various combinations of NT-proBNP level, HbA1c, and fasting plasma glucose was studied.
Conclusions
Diabetes status and elevated NT-proBNP were independently and jointly associated with MACCEs and all-cause mortality in patients with NSTE-ACS.
Similar content being viewed by others
Introduction
Diabetes has become a major health concern in China, the prevalence of which increased from 9.7% in 2007 to 11.2% in 2017 among adults [1]. Besides being a risk factor for the development of coronary artery disease (CAD), diabetes is also strongly associated with an increased risk for subsequent adverse cardiovascular events in patients with acute coronary syndrome (ACS) [2,3,4]. In addition, diabetes is related to a high risk of multivessel coronary artery disease and has a rising prevalence in individuals with a non-ST-segment elevation ACS (NSTE-ACS) [5, 6]. Revascularization is one of the major treatments for NSTE-ACS, but the optimal revascularization strategy (percutaneous coronary intervention [PCI] vs. coronary artery bypass grafting [CABG]) remains controversial due to the lack of randomized comparison [7]. Thus, early and precise risk stratification, as one of the factors in the decision-making process, is essential for the prognosis of patients with NSTE-ACS.
Recently, N-terminal pro-B-type natriuretic peptide (NT-proBNP) has received attention as a biomarker of cardiac reserve and hemodynamic stress [8]. NT-proBNP has been found a strong and independent predictor of subsequent adverse cardiovascular events in the spectrum of ACS patients [9,10,11]. The current guideline from the European Society of Cardiology (ESC) has newly recommended that measuring NT-proBNP plasma concentrations should be considered to gain prognostic information for the risk assessment and management of patients with NSTE-ACS [12]. In addition, a few studies have indicated that NT-proBNP may help the cardiologist to select either PCI or CABG as the revascularization strategy in patients with left main CAD or three-vessel CAD [13,14,15]. However, fewer studies evaluated the prognostic value of NT-proBNP in patients with NSTE-ACS combined with glycemic status. One previous study has confirmed a similar extent of association between NT-proBNP and increased risk of mortality across the spectrum of diabetes status in a community population [16]. However, less is known about the joint association of diabetes status and NT-proBNP with mortality in the acute scenario of NSTE-ACS.
Thus, the present study aims to extend previous observations and comprehensively evaluate the joint association of diabetes status and NT-proBNP with subsequent risk of cardiovascular events in a large Chinses cohort of patients with NSTE-ACS. We hypothesized that patients with both diabetes and elevated NT-proBNP would be associated with an increased risk of adverse cardiac outcomes.
Methods
Study population
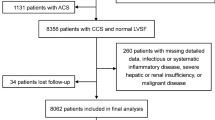
The CBDBANK (Cardiovascular Center Beijing Friendship Hospital Database Bank) is a prospective cohort study of 15,330 consecutive patients diagnosed with ACS from January 2013 to January 2021. A total of 12,946 patients were diagnosed with NSTE-ACS (including non-ST-segment elevation myocardial infarction [NSTEMI] and unstable angina [UA]) based on the guideline [12]. Of the 12,946 patients, 4990 were excluded according to the exclusion criteria, which were (1) lack of NT-proBNP, fasting plasma glucose (FPG), or glycosylated hemoglobin (HbA1c), (2) severe liver dysfunction (alanine ≥ 5 times the upper reference limits), severe renal insufficiency (estimated glomerular filtration rate [eGFR] < 30 ml/min/1.73m2), or kidney replacement treatment, (3) severe acute infection or malignancy, and (4) previous CABG, cardiogenic shock or heart failure with reduced ejection fraction (left ventricular ejection fraction [LVEF] ≤ 40%). Cardiogenic shock was defined as systolic blood pressure (SBP) < 90 mmHg for ≥ 30 min or catecholamines to maintain SBP > 90 mmHg, and clinical pulmonary congestion and impaired end-organ perfusion (altered mental status, cold/clammy skin and extremities, urine output < 30 ml/h, or lactate > 2.0 mmol/l), or a class IV rating according to the Killip classification [17, 18]. Overall, 7956 patients were included in this study (Fig. 1).

Study flow chart
The study was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University, and was following the Declaration of Helsinki.
Measurements of NT-ProBNP
Blood samples were drawn from patients during hospitalization and immediately measured using the Chemiluminescent Enzyme Immuno Assay (PATHFAST™ Immunoanalyzer, PHC Europe B.V.). The coefficients of variation for the assays range from 4.6% to 5.4%. The lower and upper limits of detection are 15 pg/ml and 30,000 pg/ml, respectively. This study used the peak values of NT-proBNP for further analyses as a continuous variable and as a category variable based on the NT-proBNP tertiles (T1 < 92 pg/ml, T2 = 92–335 pg/ml, T3 ≥ 336 pg/ml) following previous studies [19, 20].
Glycemic measures
Overnight fasting venous blood samples were collected and immediately transferred to the central laboratory (Beijing Friendship Hospital) for HbA1c and FPG testing using standard laboratory methods. The classifications of normoglycemia, prediabetes, and diabetes were based primarily on the American Diabetes Association (ADA) criteria [21]: diabetes was defined as previously diagnosed with diabetes, the use of anti-diabetic medications, FPG ≥ 7.0 mmol/l, or HbA1c ≥ 6.5%; prediabetes was as FPG 5.6–6.9 mmol/l or HbA1c 5.7–6.4%; and normoglycemia was as FPG < 5.6 mmol/l and HbA1c < 5.7%.
Outcome
The primary endpoint was major adverse cardio-cerebral events (MACCEs), including all-cause death, non-fatal myocardial infarction, non-fatal stroke, and ischemia-induced revascularization within 5 years after discharge. The secondary outcome was all-cause mortality. Non-fatal stroke was defined as signs of neurological dysfunction caused by cerebral vascular obstruction or sudden rupture confirmed by computed tomography or magnetic resonance imaging. Any revascularization was defined as percutaneous intervention or bypass surgery of the target vessel or non-target vessels. Incident cardiovascular events during hospitalization were confirmed by medical record review. Clinical follow-up was performed by telephone interview or outpatient follow-up.
Covariates
Baseline characteristics on demographic and clinical information, including age, sex, medical history, lifestyles (smoking status [none, ever, current], body mass index [BMI]), laboratory results, and in-hospital therapy were collected from hospital records. Medical history, including previous hypertension, dyslipidemia, myocardial infarction, stroke, and PCI, was obtained according to the self-reported history of diagnosis. Trained staff measured systolic and diastolic blood pressure, heart rate, as well as weight and height. BMI was calculated as weight in kilograms divided by height in meters squared. Overnight fasting blood samples were obtained and examined for biomarkers including hemoglobin, serum creatinine, high-sensitivity C-reactive protein (hs-CRP), triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C). Elevated hs-CRP was defined as ≥ 3 mg/l according to the Centers for Disease Control and Prevention and the American Heart Association [22]. The eGFR was calculated using the MDRD (The Modification of Diet in Renal Disease) formula: eGFR (ml/min/1.73 m2) = 175 × (Scr)−1.154 × (Age)−0.203 × (0.742 if female) × (1.212 if African American) [23]. Furthermore, according to National Kidney Foundation criteria, patients were classified into two eGFR groups: eGFR ≥ 60 ml/min /1.73m2 and eGFR < 60 ml/min/1.73m2 [24]. Echocardiograms were performed by expert cardiologists or ultrasound specialists. The LVEF was measured using the Simpsons method, and patients were classified into LVEF categories (41–45%, 46–50%, 51–55%, 56–60%, 61–65%, 66–70%, or > 70%) [25]. The coronary angiography and PCI operation were implemented according to relevant guidelines by experienced cardiologists. Standard medications during hospitalization were obtained directly from the medical records, including antiplatelet therapy (aspirin, or clopidogrel/ticagrelor), β-blocker, angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB), and statins.
Statistical analysis
Continuous normally distributed variables were summarized as mean ± SD, while medians (P25-P75) were reported for non-normally distributed variables. Categorical variables were reported as frequency and percentage. Study participants were categorized by NT-proBNP tertiles, and baseline characteristics were compared using one-way ANOVA, Kruskal–Wallis H test, or Pearson’s χ2 test as appropriate.
We first calculated incidence rates of MACCEs and all-cause mortality (per 1000 person-years) by categories of diabetes status and NT-proBNP. We also graphically illustrated the cumulative incidence of MACCEs and all-cause mortality by categories of NT-proBNP according to diabetes status using the Kaplan–Meier method, and differences were compared by the Log-rank test.
Using multivariable Cox proportional hazards models and after stratification into subgroups of (1) diabetes status (normoglycemia, prediabetes, diabetes); (2) HbA1c categories (< 5.7%, 5.7–6.4%, ≥ 6.5%); or (3) FPG categories (< 5.6 mmol/l, 5.6–6.9 mmol/l, ≥ 7.0 mmol/l), we estimated the hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations of NT-proBNP (modeled as a categorical or continuous variable) with MACCEs and all-cause mortality. To explore the joint association of diabetes status and NT-proBNP, we created a new variable by combining diabetes status and NT-proBNP, which had nine categories representing nine (3 × 3) combinations of diabetes status (normoglycemia, prediabetes, and diabetes) and NT-proBNP level (low, medium, and high). A similar method was conducted to create two new variables representing the combinations of NT-proBNP level, HbA1c, and FPG categories. Multivariable models were adjusted for age, sex, BMI, NSTE-ACS status, previous hypertension, previous dyslipidemia, previous myocardial infarction, SBP, heart rate, LVEF, eGFR, hs-CRP, LDL-C, smoking status, and in-hospital treatments (PCI, antiplatelet therapy, β-blocker, ACEI or ARB, and statins). Separate Cox models were conducted according to the outcomes and glycemic measures for analysis of NT-proBNP. The reference groups were selected: (1) NT-proBNP < 92 pg/ml and normoglycemia; (2) NT-proBNP < 92 pg/ml and HbA1c < 5.7%; (3) NT-proBNP < 92 pg/ml and FPG < 5.6 mmol/L. The P values for trends were calculated based on the results of the Wald χ2 test on the linearity hypothesis of ordered NT-proBNP or glycemic categories. The P values for interactions between categories of NT-proBNP and diabetes status, HbA1c, or FPG categories for the association of outcomes were also estimated using the Wald χ2 test by adding an interaction term (i.e., NT-proBNP × glycemic categories) in the multivariable models. We also used restricted cubic spline analyses to examine the relationship between NT-proBNP as a continuous variable and the risk of outcomes according to each glycemic category.
Because NT-proBNP level is strongly associated with sex, age, and BMI [26,27,28], analyses stratified by sex (male, female), age group (< 60, ≥ 60 years), and BMI category (< 25, ≥ 25 kg/m2) were also conducted. We also evaluated the risk of MACCEs and all-cause mortality by cross-categories of NT-proBNP tertiles and diabetes status—including further categorization according to glycemic control (HbA1c < 7% vs HbA1c ≥ 7%), with NT-proBNP < 92 pg/ml and no diabetes as the reference.
Analysis was performed using Stata software, version 17.0 (StataCorp LP, College Station, TX, USA), and R software, version 4.1.2 (R Foundation for Statistical Computing). A 2-sided P-value < 0.05 was considered to be statistically significant.
Results
Baseline characteristics
Of the 7956 patients in the current study, the mean ± SD age of the study population was 65.4 ± 10.5 years, and 62.7% were male. The median (IQR) levels of NT-proBNP of the whole cohort were 165.0 (65.8, 527.5). Table 1 presents the baseline characteristics according to NT-proBNP tertiles. Participants with higher NT-proBNP were more likely to be older and NSTEMI; have diabetes, previous hypertension, previous myocardial infarction, previous stroke, and previous PCI; have higher levels of FPG, HbA1c and hs-CRP; have lower levels of BMI, diastolic blood pressure, LVEF, hemoglobin, triglyceride, and eGFR; and have a higher rate of receiving clopidogrel or ticagrelor, β-Blocker, ACEI/ARB and PCI during hospitalization.
During 20,257.9 person-years of follow-up, 13.5% of the study population experienced a first MACCEs (n = 1070; 52.8 per 1000 person-years). This included 461 incidents of all-cause death (21.3 per 1000 person-years), 253 incidents of non-fatal myocardial infarction (12.0 per 1000 person-years), 111 incidents of non-fatal stroke (5.2 per 1000 person-years), and 434 incidents of ischemia-induced revascularization (21.0 per 1000 person-years). Approximately, 17.6% of MACCEs occurred in patients with normoglycemia (n = 1848) and 16.9% in patients with NT-proBNP < 92 pg/ml (n = 2653). In contrast, 56.0% of those with baseline NT-proBNP ≥ 336 pg/ml (n = 2648) experienced a MACCEs during follow-up.
Independent association of NT-ProBNP, diabetes status, and outcomes
In the whole cohort, patients with diabetes were associated with a higher risk of MACCEs and all-cause mortality, with adjusted HRs of 1.42 (95% CI: 1.20–1.68) and 1.37 (95% CI: 1.05–1.78), respectively (Table 2). In addition, a higher level of NT-proBNP was significantly related to a higher risk of MACCEs and all-cause mortality. The adjusted HRs were 1.00 (reference), 1.24 (95% CI: 1.02–1.50) and 1.72 (95% CI: 1.40–2.11) for MACCEs, and 1.00 (reference), 1.47 (95% CI: 0.98–2.21) and 2.80 (95% CI: 1.89–4.17) for all-cause mortality across the NT-proBNP tertiles, respectively (Table 2). Besides, patients with higher levels of NT-proBNP also had an elevated risk of cardiovascular mortality, non-fatal MI, and revascularization (Additional file 1: Figure S1).
NT-ProBNP, diabetes status, and outcomes
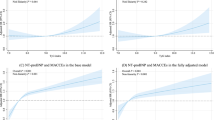
Incidence rates of MACCEs and all-cause mortality (for 1000 person-years) by cross categories of NT-proBNP tertiles and diabetes status were shown in Fig. 2. Event rates for MACCEs and all-cause mortality were lowest in those with NT-proBNP < 92 pg/ml and normoglycemia. The cumulative incidence of first MACCEs and all-cause mortality was higher in patients with baseline NT-proBNP ≥ 336 pg/ml compared to those with NT-proBNP < 92 pg/ml across each diabetes category (Log-rank P < 0.001 for all; Fig. 3). Using restricted cubic spline analyses, we observed an approximately positive linear relationship between NT-proBNP on a continuous scale and MACCEs as well as all-cause mortality across each diabetes status, after adjustment for possible confounders (Fig. 4).

Incidence rate per 1000 person-years of MACCEs and mortality in different subgroups of diabetes status and NT-proBNP categories

Kaplan–Meier estimated event rates of MACCEs and all-cause mortality by NT-proBNP tertiles across different diabetes statuses

Restricted cubic spline analysis for association of the NT-proBNP and risk of MACCEs and all-cause mortality across different diabetes statuses. Adjusted model included age, sex, BMI, NSTE-ACS status, previous hypertension, previous dyslipidemia, previous myocardial infarction, systolic blood pressure, heart rate, LVEF, eGFR, hs-CRP, LDL-C, smoking status, and in-hospital treatments (PCI, antiplatelet therapy, β-blocker, ACEI or ARB, and statins)
Table 3 and Fig. 5 show the joint associations between diabetes status and NT-proBNP categories with incident MACCEs and all-cause mortality. After adjustment of potential confounders, increasing levels of NT-proBNP were associated with higher incidents of MACCEs and all-cause mortality across each diabetes status. Compared with patients with normoglycemia and a low NT-proBNP level, the strongest numerical hazards for MACCEs and all-cause mortality were seen in patients with diabetes and NT-proBNP ≥ 336 pg/ml (HR 2.67, 95% CI: 1.83–3.89; HR 2.98, 95% CI: 1.48–6.00; Table 3, Fig. 5). However, there was no significant interaction between diabetes status and NT-proBNP for risk of MACCEs and all-cause mortality (Additional file 1: Table S1). We also observed similar results in subgroup analyses stratified by sex, age, and BMI (Additional file 1: Table S2).

Forest plots of the adjusted hazard ratios of MACCEs and all-cause mortality across diabetes status and NT-proBNP categories. The HR was calculated using Cox proportional hazards model adjusted for age, sex, BMI, NSTE-ACS status, previous hypertension, previous dyslipidemia, previous myocardial infarction, systolic blood pressure, heart rate, LVEF, eGFR, hs-CRP, LDL-C, smoking status, and in-hospital treatments (PCI, antiplatelet therapy, β-blocker, ACEI or ARB, and statins)
When further stratified by glycemic control, among patients with elevated NT-proBNP (≥ 336 pg/ml), the adjusted HRs of MACCEs were 2.62 (95% CI: 1.77–3.89) and 2.72 (95% CI: 1.84–4.02) for diabetes with HbA1c < 7% and HbA1c ≥ 7%, respectively. Similarly, the HRs of all-cause mortality were 2.95 (95% CI: 1.44–6.03) for those with diabetes and HbA1c < 7%, and 3.02 (95% CI: 1.48–6.16) for those with diabetes and HbA1c ≥ 7% (Additional file 1: Table S3). We observed no clear interaction between the two variables for MACCEs (P for interaction = 0.088) and all-cause mortality (P for interaction = 0.364).
NT-ProBNP, HbA1c, and outcomes
Increased NT-proBNP categories (≥ 336 pg/ml vs. < 92 pg/ml) demonstrated consistently higher event rates and significantly increased hazards for MACCEs and all-cause mortality across HbA1c strata (Table 4). Compared with patients with NT-proBNP < 92 pg/ml and HbA1c < 5.7%, the adjusted HRs of MACCEs and all-cause mortality were 2.72 (95% CI: 1.89–3.91) and 2.92 (95% CI: 1.53–5.57) for those with NT-proBNP ≥ 336 pg/ml and HbA1c ≥ 6.5%, respectively. We observed no clear interaction between HbA1c and NT-proBNP for outcomes (Additional file 1: Table S1). HbA1c ≥ 6.5% (vs. HbA1c < 5.7%) was associated with an increased risk of incident MACCEs in each NT-proBNP category, whereas the association was not observed for all-cause mortality in patients with NT-proBNP < 92 pg/ml (HR 0.92; 95% CI: 0.40–2.09; Table 4).
NT-ProBNP, FPG, and outcomes
Table 5 shows the joint associations of NT-proBNP and FPG categories with incident MACCEs and all-cause mortality, selecting patients with a low NT-proBNP and FPG level as the reference. Within each FPG category, a higher category of NT-proBNP was associated with significantly increased risk for incident MACCEs and all-cause mortality (Table 5). Patients with the highest NT-proBNP (≥ 336 pg/ml) and FPG (≥ 7.0 mmol/l) had the highest numerical hazards for MACCEs (HR 2.33; 95% CI: 1.74–3.12) and all-cause mortality (HR 3.27; 95% CI: 1.92–5.57) compared with patients with NT-proBNP < 92 pg/ml and FPG < 5.6 mmol/l (Table 5). There was a marginally significant interaction between FPG and NT-proBNP for MACCEs, but not for all-cause mortality (Additional file 1: Table S1).
Discussion
To our knowledge, this is the first study that prospectively evaluated the joint association of diabetes status and NT-proBNP with the subsequent risk of MACCEs and all-cause mortality in patients with NSTE-ACS. Compared with individuals with normoglycemia and NT-proBNP < 92 pg/ml, individuals with NT-proBNP ≥ 336 pg/ml and diabetes, HbA1c ≥ 6.5%, or FPG ≥ 7.0 mmol/l, were at higher risk of first MACCEs and all-cause mortality. We did not observe a significant interaction between diabetes status and NT-proBNP for incident MACCEs and all-cause mortality.
The prognostic value of NT-proBNP for adverse cardiovascular outcomes is increasingly identified in patients with diabetes. One recent study of a community-based cohort of 5861 individuals provided compelling evidence that NT-proBNP alone was superior to conventional risk factors for the prediction of cardiovascular events [29]. In addition, Prausmüller et al. evaluated the predictive performance of NT-proBNP with the recently published ESC/European Association for the Study of Diabetes (EASD) risk stratification model and the Systemic Coronary Risk Evaluation (SCORE) in patients with type 2 diabetes [30]. In this study, compared to the ESC/EASD and SCORE risk model, NT-proBNP remained a robust predictor for predicting 10-year cardiovascular disease and all-cause mortality in individuals with type 2 diabetes [30]. One case-cohort study within the European Prospective Investigation Into Cancer and Nutrition (EPIC)-Potsdam cohort indicated that NT-proBNP was positively associated with diabetes-related microvascular and macrovascular complications, which could be useful in monitoring the risk of vascular complications [31]. In general, these studies highlighted the extremely high prognostic value of NT-proBNP to identify high-risk patients with diabetes. However, none of these studies analyzed the joint association of diabetes status and NT-proBNP in patients with existing cardiovascular diseases. Our study extended these findings to patients with NSTE-ACS and found that patients with both a higher glycemic category and NT-proBNP level were associated with worse outcomes.
The association of increased NT-proBNP levels with adverse outcomes was observed among numerous studies regarding the NSTE-ACS population [11, 32, 33]. It has been reported that plasma NT-proBNP would rise rapidly from the onset of myocardial ischemia due to acute left ventricular dysfunction [34]. The increased magnitude of NT-proBNP level is proportional to the severity of myocardial ischemia and subsequent left ventricular systolic and diastolic dysfunction [35]. In addition, prior studies also indicated that the prognostic value of NT-proBNP was on top of cardiac troponin [33]. Similar results were observed in the present study that NT-proBNP was independently associated with a higher risk of MACCEs and all-cause mortality in the whole cohort. Moreover, no significant interaction between diabetes status and NT-proBNP was observed, suggesting that NT-proBNP was also useful for further risk stratification within each diabetes status for patients with NSTE-ACS.
Remarkably, the latest ESC guideline has recommended using NT-proBNP to gain more prognostic information in patients with NSTE-ACS (Class of Recommendation: IIa) [12]. In addition, a recent consensus report of the ADA also suggested that an initial assessment of NT-proBNP could be used as a first-line screening tool [36]. The relationship between diabetes and NT-proBNP was described as a “partners in crime” relationship by one previous study [37]. Consistently, our study emphasized the joint effect of diabetes and NT-proBNP on the cardiovascular risk in patients with NSTE-ACS, with the highest hazards for MACCEs and all-cause mortality shown in patients with diabetes and NT-proBNP ≥ 336 pg/ml. Furthermore, among patients with diabetes and elevated NT-proBNP, higher HRs were observed in patients with unsatisfactory glycemic control (HbA1c ≥ 7%). These results highlighted the importance of glycemic control and the detection of NT-proBNP. We assumed that our findings could help improve the early identification of high-risk patients and lead to the application of the most appropriate treatments as soon as possible.
The potential underlying mechanisms of the joint effect of diabetes status and NT-proBNP remains unknown. Several longitudinal observational studies of population-based cohorts have shown that heart failure risk was enhanced two- to fivefold in patients with diabetes or prediabetes compared with those without [38, 39]. In the diabetes community, heart failure was widely recognized as one of the main complications, the frequency of which was second only to peripheral arterial disease [40]. Individuals with diabetes may develop “diabetic cardiomyopathy,” defined as left ventricular systolic or diastolic dysfunction in the absence of coronary artery disease and hypertension [41]. The mechanisms are complex and include several dysregulated pathways such as mitochondrial dysfunction, altered insulin signaling, oxidative stress, and increased formation of advanced glycation end products, all leading to functional and structural changes in the diabetic heart [41]. Therefore, cardiac dysfunction may be accelerated in the presence of diabetes in NSTE-ACS patients. Our results indicated that patients with baseline diabetes and NT-proBNP ≥ 336 pg/ml should be alert for further decline of cardiac function.
The strengths of this study included the large population, prospective design, long follow-up period, and the wide variety of adjustments of covariates. However, several limitations need to be addressed. Overnight fasting venous blood samples for FPG testing were obtained on the second day after admission and the diagnosis of diabetes may be overestimated due to stress hyperglycemia. Second, only a single measurement of NT-proBNP was used in the study, and potential bias due to measurement error should be considered. Thus, further longitudinal analyses should be performed to confirm these findings. Furthermore, details on the severity of myocardial ischemia or infarct size were failed to obtain in this study, thus residual or unmeasured confounders may exist.
Conclusions
Diabetes status and higher levels of NT-proBNP were significantly associated with a higher risk of MACCEs and all-cause mortality in patients with NSTE-ACS. Detection of NT-proBNP would be useful to the prognostic evaluation and risk stratification, especially for patients with prediabetes and diabetes. Further randomized controlled trials are required to confirm whether intensification of treatment based on the joint association of diabetes status and NT-proBNP might improve the prognosis of patients with NSTE-ACS.
Availability of data and materials
The datasets used for the present analysis may be made available upon reasonable request by contacting the corresponding author.
References
Li Y, Teng D, Shi X, Qin G, Qin Y, Quan H, Shi B, Sun H, Ba J, Chen B, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ (Clinical research ed). 2020;369: m997.
Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, Antman EM. Diabetes and mortality following acute coronary syndromes. JAMA. 2007;298(7):765–75.
Dotevall A, Hasdai D, Wallentin L, Battler A, Rosengren A. Diabetes mellitus: clinical presentation and outcome in men and women with acute coronary syndromes. Data from the Euro Heart Survey ACS. Diabetic Med. 2005;22(11):1542-1550.
Fan HL, Zeng LH, Chen PY, Liu YH, Duan CY, He WF, Tan N, Chen JY, He PC. Association of baseline hemoglobin A1c levels with bleeding in patients with non-ST-segment elevation acute coronary syndrome underwent percutaneous coronary intervention: insights of a multicenter cohort study from China. J Geriatr Cardiol. 2022;19(7):487–97.
Szummer K, Wallentin L, Lindhagen L, Alfredsson J, Erlinge D, Held C, James S, Kellerth T, Lindahl B, Ravn-Fischer A, et al. Relations between implementation of new treatments and improved outcomes in patients with non-ST-elevation myocardial infarction during the last 20 years: experiences from SWEDEHEART registry 1995 to 2014. Eur Heart J. 2018;39(42):3766–76.
Godoy LC, Lawler PR, Farkouh ME, Hersen B, Nicolau JC, Rao V. Urgent Revascularization strategies in patients with diabetes mellitus and acute coronary syndrome. Can J Cardiol. 2019;35(8):993–1001.
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165.
Morrow DA, Cannon CP, Jesse RL, Newby LK, Ravkilde J, Storrow AB, Wu AH, Christenson RH, Apple FS, Francis G, et al. National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: clinical characteristics and utilization of biochemical markers in acute coronary syndromes. Clin Chem. 2007;53(4):552–74.
Heeschen C, Hamm CW, Mitrovic V, Lantelme NH, White HD. N-terminal pro-B-type natriuretic peptide levels for dynamic risk stratification of patients with acute coronary syndromes. Circulation. 2004;110(20):3206–12.
Jernberg T, Lindahl B, Siegbahn A, Andren B, Frostfeldt G, Lagerqvist B, Stridsberg M, Venge P, Wallentin L. N-terminal pro-brain natriuretic peptide in relation to inflammation, myocardial necrosis, and the effect of an invasive strategy in unstable coronary artery disease. J Am Coll Cardiol. 2003;42(11):1909–16.
Ndrepepa G, Braun S, Mehilli J, Niemöller K, Schömig A, Kastrati A. A prospective cohort study of prognostic power of N-terminal probrain natriuretic peptide in patients with non-ST segment elevation acute coronary syndromes. Clin Res Cardiolo. 2007;96(1):30–7.
Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–367.
Michou E, Fahrni G, Mueller C. Quantifying heart failure using natriuretic peptides may help the HEART team in decision-making. Eur Heart J. 2019;40(41):3406–8.
Redfors B, Chen S, Crowley A, Ben-Yehuda O, Gersh BJ, Lembo NJ, Brown WM 3rd, Banning AP, Taggart DP, Serruys PW, et al. B-type natriuretic peptide assessment in patients undergoing revascularization for left main coronary artery disease: analysis from the EXCEL Trial. Circulation. 2018;138(5):469–78.
Zhang C, Jiang L, Xu L, Tian J, Liu J, Zhao X, Feng X, Wang D, Zhang Y, Sun K, et al. Implications of N-terminal pro-B-type natriuretic peptide in patients with three-vessel disease. Eur Heart J. 2019;40(41):3397–405.
Ciardullo S, Rea F, Cannistraci R, Muraca E, Perra S, Zerbini F, Mortara A, Perseghin G. NT-ProBNP and mortality across the spectrum of glucose tolerance in the general US population. Cardiovasc Diabetol. 2022;21(1):236.
Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med. 2012;367(14):1287–96.
Killip T, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967;20(4):457–64.
Idzerda NMA, Persson F, Pena MJ, Brenner BM, Brunel P, Chaturvedi N, McMurray JJ, Parving HH, de Zeeuw D, Heerspink HJL. N-terminal pro-brain natriuretic peptide (NT-proBNP) predicts the cardio-renal response to aliskiren in patients with type 2 diabetes at high renal and cardiovascular risk. Diabetes Obes Metab. 2018;20(12):2899–904.
Tarnow L, Gall MA, Hansen BV, Hovind P, Parving HH. Plasma N-terminal pro-B-type natriuretic peptide and mortality in type 2 diabetes. Diabetologia. 2006;49(10):2256–62.
Classification and Diagnosis of Diabetes. Standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S15-s33.
Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, Fadl YY, Fortmann SP, Hong Y, Myers GL, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107(3):499–511.
Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, Kusek JW, Van Lente F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247–54.
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139(2):137–47.
Vaduganathan M, Claggett BL, Greene SJ, Aggarwal R, Bhatt AS, McMurray JJV, Fonarow GC, Solomon SD. Potential Implications of Expanded US Food and Drug Administration Labeling for Sacubitril/Valsartan in the US. JAMA cardiology. 2021;6(12):1415–23.
Hogenhuis J, Voors AA, Jaarsma T, Hillege HL, Boomsma F, van Veldhuisen DJ. Influence of age on natriuretic peptides in patients with chronic heart failure: a comparison between ANP/NT-ANP and BNP/NT-proBNP. Eur J Heart Fail. 2005;7(1):81–6.
Taki M, Ishiyama Y, Mizuno H, Komori T, Kono K, Hoshide S, Kario K. Sex Differences in the Prognostic Power of Brain Natriuretic Peptide and N-Terminal Pro-Brain Natriuretic Peptide for Cardiovascular Events - The Japan Morning Surge-Home Blood Pressure Study. Circ J. 2018;82(8):2096–102.
Vergaro G, Gentile F, Meems LMG, Aimo A, Januzzi JL Jr, Richards AM, Lam CSP, Latini R, Staszewsky L, Anand IS, et al. NT-proBNP for risk prediction in heart failure: identification of optimal cutoffs across body mass index categories. JACC Heart failure. 2021;9(9):653–63.
Wijkman MO, Claggett BL, Malachias MVB, Vaduganathan M, Ballantyne CM, Kitzman DW, Mosley T, Matsushita K, Solomon SD, Pfeffer MA. Importance of NT-proBNP and conventional risk factors for prediction of death in older adults with and without diabetes mellitus- A report from the Atherosclerosis Risk in Communities (ARIC) study. Diabetes Res Clin Pract. 2022;194: 110164.
Prausmüller S, Resl M, Arfsten H, Spinka G, Wurm R, Neuhold S, Bartko PE, Goliasch G, Strunk G, Pavo N, et al. Performance of the recommended ESC/EASD cardiovascular risk stratification model in comparison to SCORE and NT-proBNP as a single biomarker for risk prediction in type 2 diabetes mellitus. Cardiovasc Diabetol. 2021;20(1):34.
Birukov A, Eichelmann F, Kuxhaus O, Polemiti E, Fritsche A, Wirth J, Boeing H, Weikert C, Schulze MB. Opposing Associations of NT-proBNP With Risks of Diabetes and Diabetes-Related Complications. Diabetes Care. 2020;43(12):2930–7.
He WF, Jiang L, Chen YY, Liu YH, Chen PY, Duan CY, Zeng LH, Fan HL, Wei XB, Guo W, et al. The association of baseline N-terminal pro-B-type natriuretic peptide with short and long-term prognosis following percutaneous coronary intervention in non-ST segment elevation acute coronary syndrome with multivessel coronary artery disease: a retrospective cohort study. BMC Cardiovasc Disord. 2021;21(1):202.
Lindholm D, James SK, Bertilsson M, Becker RC, Cannon CP, Giannitsis E, Harrington RA, Himmelmann A, Kontny F, Siegbahn A, et al. Biomarkers and coronary lesions predict outcomes after revascularization in non-ST-elevation acute coronary syndrome. Clin Chem. 2017;63(2):573–84.
Riezebos RK, Ronner E, de Boer BA, Slaats EH, Tijssen JG, Laarman GJ. Dynamics in N-terminal pro-brain natriuretic peptide concentration in patients with non-ST-elevation acute coronary syndrome. Am Heart J. 2005;150(6):1255–9.
Troughton RW, Richards AM. B-type natriuretic peptides and echocardiographic measures of cardiac structure and function. JACC Cardiovasc Imaging. 2009;2(2):216–25.
Pop-Busui R, Januzzi JL, Bruemmer D, Butalia S, Green JB, Horton WB, Knight C, Levi M, Rasouli N, Richardson CR. Heart failure: an underappreciated complication of diabetes a consensus report of the American Diabetes Association. Diabetes Care. 2022;45(7):1670–90.
Bayes-Genis A. Diabetes and NT-proBNP: Partners in crime. Diabetes Res Clin Pract. 2022;194: 110165.
Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34(1):29–34.
Thrainsdottir IS, Aspelund T, Thorgeirsson G, Gudnason V, Hardarson T, Malmberg K, Sigurdsson G, Rydén L. The association between glucose abnormalities and heart failure in the population-based Reykjavik study. Diabetes Care. 2005;28(3):612–6.
Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, Deanfield J, Smeeth L, Timmis A, Hemingway H. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet Diabetes Endocrinol. 2015;3(2):105–13.
Bugger H, Abel ED. Molecular mechanisms of diabetic cardiomyopathy. Diabetologia. 2014;57(4):660–71.
Acknowledgements
The authors thank Guoliang Zhao (Beijing Friendship Hospital, Capital Medical University) for technical support.
Funding
This work was supported by the National Key R&D Program of China (2021ZD0111000), the National Natural Science Foundation of China (82070357), and Beijing Key Clinical Subject Program.
Author information
Authors and Affiliations
Contributions
MW performed the study, did statistical analysis, and wrote the manuscript. WS participated in the study data collection. HC contributed discussion and edited the manuscript. HL provided funding support, designed the study, and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study data collections were approved by the Institutional Review Board of Beijing Friendship Hospital, Capital Medical University, and written informed consent was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Kaplan-Meier curves for MACCEs, all-cause mortality, cardiovascular mortality, non-fatal MI, non-fatal stroke, and revascularization according to NT-proBNP categories. Table S1. P-value of the interaction of glycemic and NT-proBNP categories in the prediction of incident MACCEs and all-cause mortality. Table S2. Adjusted HRs of incident MACCE across the spectrum of diabetes status and NT-proBNP categories for different subgroups. Table S3. Adjusted HR of cardiovascular outcomes across the spectrum of glycemic control and NT-proBNP categories.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, M., Su, W., Chen, H. et al. The joint association of diabetes status and NT-ProBNP with adverse cardiac outcomes in patients with non-ST-segment elevation acute coronary syndrome: a prospective cohort study. Cardiovasc Diabetol 22, 46 (2023). https://doi.org/10.1186/s12933-023-01771-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01771-1