
Abstract
Background
Bronchoalveolar lavage (BAL) is a key tool in respiratory medicine for sampling the distal airways. BAL bile acids are putative biomarkers of pulmonary microaspiration, which is associated with poor outcomes after lung transplantation. Compared to BAL, large airway bronchial wash (LABW) samples the tracheobronchial space where bile acids may be measurable at more clinically relevant levels. We assessed whether LABW bile acids, compared to BAL bile acids, are more strongly associated with poor clinical outcomes in lung transplant recipients.
Methods
Concurrently obtained BAL and LABW at 3 months post-transplant from a retrospective cohort of 61 lung transplant recipients were analyzed for taurocholic acid (TCA), glycocholic acid (GCA), and cholic acid by mass spectrometry and 10 inflammatory proteins by multiplex immunoassay. Associations between bile acids with inflammatory proteins and acute lung allograft dysfunction were assessed using Spearman correlation and logistic regression, respectively. Time to chronic lung allograft dysfunction and death were evaluated using multivariable Cox proportional hazards and Kaplan–Meier methods.
Results
Most bile acids and inflammatory proteins were higher in LABW than in BAL. LABW bile acids correlated with inflammatory proteins within and between sample type. LABW TCA and GCA were associated with acute lung allograft dysfunction (OR = 1.368; 95%CI = 1.036–1.806; P = 0.027, OR = 1.064; 95%CI = 1.009–1.122; P = 0.022, respectively). No bile acids were associated with chronic lung allograft dysfunction. Adjusted for risk factors, LABW TCA and GCA predicted death (HR = 1.513; 95%CI = 1.014–2.256; P = 0.042, HR = 1.597; 95%CI = 1.078–2.366; P = 0.020, respectively). Patients with LABW TCA in the highest tertile had worse survival compared to all others.
Conclusions
LABW bile acids are more strongly associated than BAL bile acids with inflammation, acute lung allograft dysfunction, and death in lung transplant recipients. Collection of LABW may be useful in the evaluation of microaspiration in lung transplantation and other respiratory diseases.
Similar content being viewed by others


Background
Bronchoalveolar lavage (BAL) is a well-established tool for minimally invasive sampling of the microenvironment in the lower airways. It is performed by wedging the tip of a flexible bronchoscope within a selected bronchopulmonary segment, instilling a volume of sterile isotonic saline sufficient to reach the alveolar space, followed by suctioning of the fluid [1, 2]. Analysis of BAL samples through biochemical, cytological, and microbiological techniques play a predominant role in the diagnosis of a wide variety of diseases in respiratory medicine. In contrast to BAL, a bronchoscopic fluid sample that has been utilized less commonly in the clinical setting is the bronchial wash, which has been defined as a non-wedged or lower volume bronchoscopic sampling where the instilled fluid does not reach the alveolar space [2]. Specifically, the large airway bronchial wash (LABW) is obtained with the bronchoscope tip in a mainstem or lobar airway. The diagnostic value of bronchial wash and BAL has been directly compared in only a few disease states, including pulmonary tuberculosis [3], lymphangitic carcinomatosis [4], and peripheral lung cancer [5]. All of these studies found that BAL had higher sensitivity.
LABW may be more advantageous than BAL as a diagnostic sample to detect pulmonary microaspiration driven by gastroesophageal reflux disease (GERD). In BAL, the presence of biochemical compounds originating from the stomach, such as pepsin and bile acids, have been shown as indicators of microaspiration in patients receiving mechanical ventilation [6], advanced lung disease patients [7,8,9], and lung transplant recipients [10, 11]. Given the relative proximity of the large airways and tracheobronchial space to the gastrointestinal tract, LABW may yield biomarkers of microaspiration at more clinically useful levels than BAL.
Microaspiration biomarkers with diagnostic and prognostic value are highly sought after in clinical lung transplantation as GERD-driven microaspiration has been linked to acute rejection [12], acute decline in pulmonary function [13], and development of chronic lung allograft dysfunction (CLAD) [10], presumably through inflammation and fibrosis [14]. Although early anti-reflux surgery in lung transplant recipients may slow lung function deterioration, its related risks and complications necessitate improved patient selection [15]. Our group recently reported that a specific bile acid, taurocholic acid (TCA), in BAL at 3 months post-transplant was associated with concurrent objective evidence of GERD, inflammation, and acute lung allograft dysfunction (ALAD) [16]. Moreover, BAL TCA was reduced following anti-reflux surgery [16]. Urso et al. recently showed that elevated bile acids in LABW at 3 months post-transplant were independent predictors of CLAD, death, and bacterial infections [17]. Similarly, Nakajima et al. observed that bronchial wash from donor lungs declined for implantation in recipients due to aspiration or infection had higher bile acids compared to those from accepted donor lungs. [18]
A direct comparison of the diagnostic and prognostic value of LABW and BAL bile acids in the context of microaspiration in lung transplant recipients would be timely and helpful in guiding future biomarker research. Leveraging the existing cohort from our previous BAL bile acid study [16] and our institutional protocol of routinely collecting both LABW and BAL, we aimed to compare bile acid levels between sample types and their associations with relevant short- and long-term clinical outcomes. We hypothesized that LABW bile acid at 3 months post-transplant are more strongly associated with inflammation, ALAD, CLAD, and death compared to BAL bile acid.
Methods
Patient selection
This single-center, retrospective cohort study was approved by the University Health Network Research Ethics Board (REB# 15-9698). Informed written consent was obtained from all patients for publication of the study data. The study cohort was derived from a previously described cohort (Fig. 1) [16]. 285 adults who underwent lung transplantation at Toronto General Hospital between 2010 and 2015 with available post-transplant 24-h esophageal pH/impedance reflux study were assessed for eligibility. Patients were categorized as with GERD (≥ 48 total reflux episodes) or without GERD (< 48 total reflux episodes) [19]. Both acidic and non-acidic episodes were included in the total number of reflux episodes as 92% of patients were on proton pump inhibitors. Patients with GERD were excluded if reflux study was performed > 365 days post-transplant or no BAL samples were available. Patients without GERD were matched 2:1 to patients with GERD by transplant type, starting from patients with the lowest number of reflux episodes, and excluded if reflux study was performed > 365 days post-transplant, clinical symptoms were reported during the study, no BAL samples were available, or other reasons detailed in Fig. 1. 8 patients with GERD and 7 patients without GERD were excluded due to no matching LABW samples available, arriving at the final study size of 61 patients (17 with GERD and 44 without GERD). Reflux testing was performed at a median of 11 days from bronchoscopy and BAL/LABW sampling.

Study flow diagram. The study cohort was derived from a parent cohort of patients with or without GERD, which we previously described. We excluded 8 patients with GERD and 7 patients without GERD who did not have matching LABW samples available at 3 months after transplantation. We then combined the remaining 17 patients with GERD and 44 patients without GERD to form the study cohort of 61 patients
Sample collection, processing, and analysis
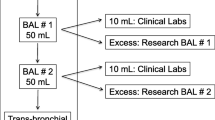
During bronchoscopy, LABW samples were collected by instilling and suctioning 20 mL of isotonic saline through a flexible bronchoscope in the mainstem bronchus. Suctioning proximal to the vocal cords was avoided. The bronchoscope was then wedged in a bronchopulmonary segment, and two BAL fractions were obtained by sequentially instilling and suctioning two 50 ml aliquots of isotonic saline. The second BAL fraction was used for this study, as it may preferentially sample the distal bronchoalveolar space [20]. The default locations of LABW and BAL were the right mainstem bronchus and right middle lobe, respectively, unless there were localizing clinical findings, such as consolidation on imaging or localized secretions on airway exam. Samples remained on ice until centrifugation for 20 min at 3184G at 4 °C; supernatants were then separated and stored at − 80 °C until analysis. Liquid chromatography with tandem mass spectrometry was used to measure levels of taurocholic acid (TCA), glycocholic acid (GCA), and cholic acid (CA). Ten inflammatory proteins (IL-1α, IL-1β, IL-6, IL-8, IL-12p70, CCL2, CCL5, defensins S100A8 and S100A12, and soluble RAGE) were measured using multiplex immunoassay (R&D Systems, USA). Club cell secretory protein (CCSP), a marker of epithelial secretory function and injury [21], was measured by ELISA (R&D Systems, USA). Analyte concentrations were not normalized since there is no universally accepted method and normalization can have unpredictable effects on results. [2]
Clinical protocols and definitions
Standard of care was described previously by the Toronto Lung Transplant Program [22]. Briefly, patients underwent routine surveillance bronchoscopy to obtain LABW, BAL, and transbronchial biopsies at 0.5, 1.5, 3, 6, 9, 12, 18, and 24 months post-transplant. For this study, 3-month LABW and BAL samples were analyzed in order to optimize the proximity to reflux testing, which typically occurred around 3 months post-transplant as per institutional protocol. Routine pulmonary function tests were performed weekly in the first 3 months, monthly from 3 months to 2 years post-transplant, and every 3 months thereafter. Additional bronchoscopies and pulmonary function tests were performed as clinically indicated.
The most recent forced expiratory volume in 1 second (FEV1) measurement preceding the time of sample collection was used to define concurrent lung function. ALAD was defined as a ≥ 10% decline in most recent measured FEV1 at the time of bronchoscopy compared to the maximum of two preceding FEV1 measurements, consistent with our previous study [16]. Baseline lung allograft dysfunction (BLAD) was defined as failure to achieve ≥ 80% predicted FEV1 [23]. CLAD was defined in accordance to the 2019 International Society for Heart and Lung Transplantation consensus report [24]. CLAD and death outcomes were censored on February 28, 2019. No patients were lost to follow-up.
Statistical approach
All statistical analyses were performed using R version 3.6.2. Wilcoxon signed-rank test was used to compare biomarker levels between LABW and BAL. Spearman correlation was used to compare biomarker levels in concurrent samples. Univariable logistic regression was used to assess the association between bile acid levels and ALAD or BLAD. Multivariable Cox proportional hazards models were used to determine the association of bile acid levels (as continuous variables) with time to CLAD or death. CLAD-free survival and overall survival were adjusted for major known risk factors [25]: recipient age, sex, primary disease, cytomegalovirus (CMV) mismatch, and acute rejection at time of bronchoscopy. Kaplan–Meier method was used to compare overall survival stratified by bile acid tertiles. Correction for multiple comparison was not applied due to multicollinearity of bile acids and proteins. Unadjusted P values are reported; a threshold of P < 0.05 was considered statistically significant.
Results
Study population
Sixty-one patients were included in the study (Fig. 1). Baseline patient characteristics are described in Table 1. There was no missing data. Seventeen (28%) patients had GERD as defined by ≥ 48 reflux episodes on 24-h esophageal pH-impedance reflux study. The median time from transplant to bronchoscopy, when LABW and BAL samples were concurrently obtained, was 3.02 months. The median follow-up time for CLAD-free survival was 4.67 years, for a total follow-up time of 260.59 person-years. The median follow-up time for overall survival was 5.04 years, for a total follow-up time of 288.66 person-years.
Biomarker levels in LABW versus BAL
The BAL biomarker levels were measured as part of our prior publication [16] and are included herein for purposes of comparison with LABW levels. Levels of TCA, GCA, IL-1α, IL-1β, IL-6, IL-8, IL-12p70, CCL2, CCL5, S100A8, and CCSP were higher in LABW compared to BAL (Fig. 2). RAGE levels were lower in LABW compared to BAL. CA and S100A12 levels were not statistically different between sample types.

Biomarker levels in LABW vs. BAL. Wilcoxon signed rank test was used to compare levels of biomarkers in paired LABW vs BAL samples. Statistically significant differences as defined by P < 0.05 are indicated by a star. TCA, GCA, IL-1α, IL-1β, IL-6, IL-8, IL-12p70, CCL2, CCL5, S100A8, and CCSP were higher in LABW compared to BAL. RAGE was lower in LABW compared to BAL. CA and S100A12 levels were not statistically different between LABW and BAL. Y-axes units are nM for bile acids and pg/ml for proteins
Biomarker correlations within and between samples
Within LABW, nearly all bile acid and protein levels had significant positive correlations with each other, with the exception of S100A12 which was negatively correlated (Fig. 3A). Between sample types, LABW TCA and GCA positively correlated with the majority of BAL proteins, specifically IL-1α, IL-1β, IL-6, IL-8, CCL2, and CCL5 (Fig. 3B). BAL TCA and GCA positively correlated with only CCL2 and CCL5 in LABW.

Heatmaps showing correlations between biomarker levels within LABW and between sample types. Spearman correlation was used to assess correlations between two biomarker levels within LABW (A) and between LABW and BAL (B). The colour and size of circles indicate respectively the direction (blue = positive; red = negative) and strength (larger = stronger; smaller = weaker) of correlation. Statistically significant correlations as defined by P < 0.05 are indicated by a star
Association of biomarker levels with clinical outcomes
Six (10%) patients had ALAD. LABW TCA and GCA were positively associated with ALAD in univariable logistic regression (OR = 1.368; 95%CI = 1.036–1.806; P = 0.027 and OR = 1.064; 95% CI = 1.009–1.122; P = 0.022, respectively). When GERD status was added to the model as a predictor, it was not significantly associated with ALAD, and the strength of associations between bile acids and ALAD remained unchanged (Additional file 1: Table S1). Bile acids in BAL were not significantly associated with ALAD (Fig. 4A).

Forest plots showing association of bile acids with ALAD, CLAD, and death. Univariable logistic regression was used to assess associations of bile acid levels (as continuous variables) with ALAD (A). Multivariable Cox proportional hazards models, adjusted for recipient age, sex, primary disease, CMV mismatch, and concurrent acute rejection, were used to assess association of bile acid levels (as continuous variables) with time to CLAD (B) and time to death (C). Horizontal lines indicate 95% confidence intervals. Squares indicate point estimates. Statistically significant associations as defined by P < 0.05 are indicated by a star
No bile acids in LABW were associated with BLAD at up to 13 months (Additional file 1: Table S2). LABW TCA and GCA had weak but significant positive correlations with the number of proximal and total reflux episodes (Additional file 1: Fig. S1).
Sixteen (26%) patients developed CLAD, at a median follow-up time of 1.97 years. No bile acids in either LABW or BAL were significantly predictive of CLAD in multivariable Cox proportional hazards models adjusted for recipient age, sex, primary disease, CMV mismatch, and concurrent acute rejection (Fig. 4B).
Fifteen (25%) patients died, at a median follow-up time of 3.65 years. In multivariable Cox proportional hazards models, LABW TCA and GCA were independent predictors of death (HR = 1.513; 95% CI = 1.014–2.256; P = 0.042 and HR = 1.597; 95% CI = 1.078–2.366; P = 0.020, respectively). No bile acid in BAL significantly predicted death (Fig. 4C).
By Kaplan–Meier method, patients with LABW TCA in the top tertile (≥ 0.5 nM) had significantly worse overall survival compared to others (62% vs. 85% at 5 years; log-rank P = 0.018; Fig. 5A). Patients with LABW GCA in the top tertile (≥ 2.9 nM) had worse overall survival compared to others, which was not meeting the pre-specified level of significance (log-rank P = 0.07; Fig. 5B).

Kaplan–Meier curves for overall survival in patients stratified by TCA or GCA level. Kaplan–Meier survival curves with 95% confidence interval and number at risk table between patients in the highest tertile for TCA (A) or GCA (B) compared to all others. P value for log-rank test are shown
Discussion
Our study reveals that bile acids, specifically TCA and GCA, are present at higher concentrations in LABW compared to BAL. This is consistent with the long-held theory that bile acid presence in the lungs is the result of microaspirated gastrointestinal contents [16]. Bile acid-containing refluxate initially enters the large airways and tracheobronchial tree, which are preferentially sampled by LABW. As refluxate travels more distally to small airways and alveolar space, it mixes with airway secretions and becomes progressively diluted, leading to the lower bile acid concentrations measured in BAL. We speculate this model is applicable in health and disease states, although impaired mucociliary clearance in lung transplant recipients may have exaggerated the effect in our study population [26].
In addition to bile acids, the vast majority of proteins are higher in LABW than in BAL. It is likely that variable dilution may play a role in our observed differences between LABW and BAL biomarker levels, since LABW involves instillation of 20 mL of isotonic saline as opposed to 50 mL for each BAL. However, the notable exception of RAGE being lower in LABW suggests that non-trivial reasons contribute, such as heterogeneous cell composition along the airways. Prior studies have shown RAGE is constitutively expressed by type 1 pneumocytes in the alveoli [27], which may account for its higher level in BAL. In contrast, CCSP is abundantly expressed within the conducting airway epithelium [28], explaining its higher level in LABW. In a study from another center where LABW was obtained prior to BAL (similar to our protocol), LABW recovered more epithelial cells and neutrophils, while BAL recovered more lymphocytes and alveolar macrophages [29]. Building upon these previous observations, our study further supports the idea that LABW and BAL can provide complementary information, as highlighted in the consensus guidelines for standardization of LABW collection and processing in lung transplantation. [2]
Similar to what we [16] and others [10] have reported in BAL, positive correlations exist between a majority of bile acids and inflammatory proteins in LABW. Our study examines this bile acid-inflammation link between sample types. We find that bile acids in LABW, specifically TCA and GCA, show strong positive correlations with many of the inflammatory proteins in BAL, specifically four proinflammatory cytokines and two chemokines. Conversely, TCA and GCA in BAL only correlate with two chemokines in LABW. The four BAL proinflammatory cytokines that correlate with LABW TCA and GCA (i.e. IL-1α, IL-1β, IL-6, IL-8) have all been implicated as key mediators of pulmonary inflammation and fibrosis. [30, 31]
LABW TCA and GCA are also the only bile acids in either sample type associated with a concurrent acute decline in lung function or ALAD. In our previous study on the larger BAL-only cohort of 76 patients, TCA and GCA were shown to be associated with ALAD [16]. After the exclusion of 15 patients who did not have matching LABW samples, BAL TCA and GCA do not demonstrate statistical significance in this present study, although both P values closely approach the statistical significance threshold. It is unclear whether lung inflammation and ALAD in our cohort were specifically due to microaspiration or other complications after lung transplantation such as acute rejection or infection. Nonetheless, LABW TCA and GCA appear to be more useful than their BAL counterparts in aiding the diagnosis of biologically and clinically relevant microaspiration in our cohort.
Consistent with the ALAD analysis, LABW TCA and GCA are the only bile acids in either sample type which are predictive of death after adjusting for major known risk factors. When stratifying our cohort by their bile acid levels (third tertile vs. first and second), TCA is better than GCA at identifying patients at higher risk of long-term mortality. These results are similar to those in our previous study, which found multiple strong signals with TCA, including associations with GERD, ALAD, and anti-reflux surgery. This was less so the case for GCA and not at all for CA. Overall, TCA and GCA seem more predictive than CA in our study. One of the important differences between these bile acid subspecies is that TCA and GCA are conjugated, whereas CA is unconjugated. Our findings confirm a recent study by Urso et al., which observed that conjugated bile acids in BW are associated with CLAD, mortality, and bacterial infections, in addition to changes in airway lipidome and cytokines [17]. As postulated by Urso et al., conjugated bile acids may be more deleterious to pulmonary epithelium compared to their unconjugated counterparts due to increased solubility. Our study thus provides additional evidence for the use of LABW over BAL in future mechanistic and translational research on bile acids.
Although our study focused on lung transplant recipients and microaspiration, it raises the question whether LABW sampling may be useful in general respiratory medicine. In contrast to previous studies that have compared the diagnostic yields of BAL and bronchial wash [3,4,5], ours is the first to identify a condition where LABW may offer superior clinical utility. Other possible conditions include tracheobronchial tuberculosis [32] or relapsing polychondritis [33], where the large airways and tracheobronchial space are preferentially affected. Moreover, there are certain clinical situations, such as in mechanically ventilated patients with acute respiratory distress syndrome, where significant hemodynamic instability, oxygen desaturation or even cardiac arrest have been reported after full volume BAL [34]. LABW may be considered a safer alternative to obtain an adequate sample for diagnostic purposes in these cases. We believe that future studies directly comparing between LABW and BAL in these broader clinical contexts would be helpful.
Our study’s strengths include the routine use of LABW and consistent bronchoscopy protocols at our lung transplant center. Given widely differing practices between institutions, with most centers rarely performing LABW, a multicenter study would be difficult. Another strength is our multimodal approach to analyzing samples, the completeness of follow-up, and the availability of clinical data which allowed us to evaluate relationships between biomarkers and relevant biological and clinical outcomes.
This work has several limitations which warrant discussion. Given its retrospective design, there are many potential unmeasured or unknown confounding variables which may have impacted the associations observed in our study. The study cohort was derived from a highly selected retrospective cohort of lung transplant recipients with and without GERD, approximately matched one to two. This limits the generalizability of our findings, as our study cohort may not be representative of the general lung transplant recipient population or patients with other respiratory diseases. Our sample size was limited, making it likely underpowered for multivariable survival analysis. Despite the low events and sample size in some analyses, we detected a consistent signal between LABW and BAL for TCA and GCA. However, our results should be interpreted with caution and require validation in larger studies before clinical translation.
Conclusions
In this single-center retrospective cohort study, most bile acids and inflammatory proteins are present at higher levels in LABW compared to BAL at 3 months after lung transplantation. Compared to their counterparts in BAL, LABW TCA and GCA are more strongly associated with key inflammatory mediators and ALAD, and more predictive of death with adjustment of known risk factors. The clinical utility of LABW TCA and GCA as microaspiration biomarkers in lung transplant recipients require validation in a larger cohort. The potential of LABW as a sampling tool in research and clinical settings beyond lung transplantation should be further explored.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALAD:
-
Acute lung allograft dysfunction
- BA:
-
Bile acid
- BAL:
-
Bronchoalveolar lavage
- BLAD:
-
Baseline lung allograft dysfunction
- CA:
-
Cholic acid
- CCL2:
-
C–C motif chemokine ligand 2
- CCL5:
-
C–C motif chemokine ligand 5
- CCSP:
-
Club cell secretory protein
- CLAD:
-
Chronic lung allograft dysfunction
- ELISA:
-
Enzyme-linked immunosorbent assay
- FEV1:
-
Forced expiratory volume in one second
- GCA:
-
Glycocholic acid
- GERD:
-
Gastroesophageal reflux disease
- IL-12p70:
-
Interleukin 12p70
- IL-1α:
-
Interleukin 1 alpha
- IL-1β:
-
Interleukin 1 beta
- IL-6:
-
Interleukin 6
- IL-8:
-
Interleukin 8
- LABW:
-
Large airway bronchial wash
- RAGE:
-
Receptor for advanced glycation endproducts
- S100A12:
-
S100 calcium-binding protein A12
- S100A8:
-
S100 calcium-binding protein A8
- TCA:
-
Taurocholic acid
References
Costabel U, Danel C, Haslam P, et al. Technical recommendations and guidelines for bronchoalveolar lavage (BAL). Report of the European Society of Pneumology Task Group. Eur Respir J. 1989;2(6):561–85.
Martinu T, Koutsokera A, Benden C, et al. International Society for Heart and Lung Transplantation consensus statement for the standardization of bronchoalveolar lavage in lung transplantation. J Heart Lung Transplant. 2020;39:1171–90.
Kim YW, Kwon BS, Lim SY, et al. Diagnostic value of bronchoalveolar lavage and bronchial washing in sputum-scarce or smear-negative cases with suspected pulmonary tuberculosis: a randomized study. Clin Microbiol Infect. 2020;26(7):911–6.
Levy H, Horak DA, Lewis MI. The value of bronchial washings and bronchoalveolar lavage in the diagnosis of lymphangitic carcinomatosis. Chest. 1988;94(5):1028–30.
De Gracia J, Bravo C, Miravitlles M, et al. Diagnostic value of bronchoalveolar lavage in peripheral lung cancer. Am Rev Respir Dis. 1993;147(3):649–52.
Metheny NA, Chang YH, Ye JS, et al. Pepsin as a marker for pulmonary aspiration. Am J Crit Care. 2002;11(2):150–4.
Lee JS, Song JW, Wolters PJ, et al. Bronchoalveolar lavage pepsin in acute exacerbation of idiopathic pulmonary fibrosis. Eur Respir J. 2012;39(2):352–8.
Starosta V, Kitz R, Hartl D, Marcos V, Reinhardt D, Griese M. Bronchoalveolar pepsin, bile acids, oxidation, and inflammation in children with gastroesophageal reflux disease. Chest. 2007;132(5):1557–64.
Brodlie M, Aseeri A, Lordan JL, et al. Bile acid aspiration in people with cystic fibrosis before and after lung transplantation. Eur Respir J. 2015;46(6):1820–3.
D’Ovidio F, Mura M, Tsang M, et al. Bile acid aspiration and the development of bronchiolitis obliterans after lung transplantation. J Thorac Cardiovasc Surg. 2005;129(5):1144–52.
D’Ovidio F, Mura M, Ridsdale R, et al. The effect of reflux and bile acid aspiration on the lung allograft and its surfactant and innate immunity molecules SP-A and SP-D. Am J Transplant. 2006;6(8):1930–8.
Shah N, Force SD, Mitchell PO, et al. Gastroesophageal reflux disease is associated with an increased rate of acute rejection in lung transplant allografts. Transplant Proc. 2010;42(7):2702–6.
Palmer SM, Miralles AP, Howell DN, Brazer SR, Tapson VF, Davis RD. Gastroesophageal reflux as a reversible cause of allograft dysfunction after lung transplantation. Chest. 2000;118(4):1214–7.
Stovold R, Forrest IA, Corris PA, et al. Pepsin, a biomarker of gastric aspiration in lung allografts: a putative association with rejection. Am J Respir Crit Care Med. 2007;175(12):1298–303.
Roy SB, Elnahas S, Serrone R, et al. Early fundoplication is associated with slower decline in lung function after lung transplantation in patients with gastroesophageal reflux disease. J Thorac Cardiovasc Surg. 2018;155(6):2762–71.
Zhang CYK, Ahmed M, Huszti E, et al. Bronchoalveolar bile acid and inflammatory markers to identify high-risk lung transplant recipients with reflux and microaspiration. J Heart Lung Transplant. 2020;39:934–44.
Urso A, Leiva-Juárez MM, Briganti DF, et al. Aspiration of conjugated bile acids predicts adverse lung transplant outcomes and correlates with airway lipid and cytokine dysregulation. J Heart Lung Transplant. 2021;40(9):998–1008.
Nakajima D, Cypel M, Martinu T, Liu M, Keshavjee S. Donor bronchial wash bile acid and suitability of donor lungs for transplantation. J Heart Lung Transplant. 2017;37:304–6.
Cho YK. How to Interpret Esophageal Impedance pH Monitoring. J Neurogastroenterol Motil. 2010;16(3):327–30.
Levy L, Juvet SC, Boonstra K, et al. Sequential broncho-alveolar lavages reflect distinct pulmonary compartments: clinical and research implications in lung transplantation. Respir Res. 2018;19(1):102.
Kelly FL, Kennedy VE, Jain R, et al. Epithelial Clara cell injury occurs in bronchiolitis obliterans syndrome after human lung transplantation. Am J Transplant. 2012;12(11):3076–84.
Levy L, Huszti E, Renaud-Picard B, et al. Risk assessment of chronic lung allograft dysfunction phenotypes: Validation and proposed refinement of the 2019 International Society for Heart and Lung Transplantation classification system. J Heart Lung Transplant. 2020;39:761–70.
Liu J, Jackson K, Weinkauf J, et al. Baseline lung allograft dysfunction is associated with impaired survival after double-lung transplantation. J Heart Lung Transplant. 2018;37(7):895–902.
Verleden GM, Glanville AR, Lease ED, et al. Chronic lung allograft dysfunction: definition, diagnostic criteria, and approaches to treatment—a consensus report from the Pulmonary Council of the ISHLT. J Heart Lung Transplant. 2019;38(5):493–503.
Yusen RD, Christie JD, Edwards LB, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirtieth Adult Lung and Heart-Lung Transplant Report–2013; focus theme: age. J Heart Lung Transplant. 2013;32(10):965–78.
Herve P, Silbert D, Cerrina J, Simonneau G, Dartevelle P. Impairment of bronchial mucociliary clearance in long-term survivors of heart/lung and double-lung transplantation. The Paris-Sud Lung Transplant Group. Chest. 1993;103(1):59–63.
Shirasawa M, Fujiwara N, Hirabayashi S, et al. Receptor for advanced glycation end-products is a marker of type I lung alveolar cells. Genes Cells. 2004;9(2):165–74.
Reynolds SD, Reynolds PR, Pryhuber GS, Finder JD, Stripp BR. Secretoglobins SCGB3A1 and SCGB3A2 define secretory cell subsets in mouse and human airways. Am J Respir Crit Care Med. 2002;166(11):1498–509.
Lam S, Leriche JC, Kijek K, Phillips D. Effect of bronchial lavage volume on cellular and protein recovery. Chest. 1985;88(6):856–9.
She YX, Yu QY, Tang XX. Role of interleukins in the pathogenesis of pulmonary fibrosis. Cell Death Discov. 2021;7(1):1–10.
Borthwick LA. The IL-1 cytokine family and its role in inflammation and fibrosis in the lung. Semin Immunopathol. 2016;38(4):517–34.
Pathak V, Shepherd RW, Shojaee S. Tracheobronchial tuberculosis. J Thorac Dis. 2016;8(12):3818–25.
Ernst A, Rafeq S, Boiselle P, et al. Relapsing polychondritis and airway involvement. Chest. 2009;135(4):1024–30.
Medford AR, Millar AB. Safety of broncho-alveolar lavage in ventilated patients with acute respiratory distress syndrome. J Bronchol Interv Pulmonol. 2007;14(3):215.
Acknowledgements
The authors would like to thank Dr. Frank D’Ovidio from Columbia University for valuable advice regarding LABW and BAL bile acid measurements in lung transplant recipients. They are grateful to the Toronto Lung Transplant Program Biobank team for helping with sample collection and retrieval. The authors also acknowledge members of the Clinical Trials in Organ Transplantation-20 (CTOT-20) who helped design the original cohort from which this study was derived, specifically Drs. Jamie L. Todd, Laurie D. Snyder, and Scott M. Palmer from Duke University Medical Center and S. Samuel Weigt from UCLA Medical Center.
Funding
This study was funded by The National Institutes of Health/National Institute of Allergy and Infectious Diseases, Clinical Trials in Organ Transplantation (CTOT-20) Ancillary Study Fund (TM), Toronto General & Western Hospital Foundation Grant (TM and SK), and University of Toronto Comprehensive Research Experience for Medical Students Program (CYKZ).
Author information
Authors and Affiliations
Contributions
MA, ATS, SA, JCY, LGS, SK, and TM contributed to study conception and design. CYKZ, MA, LL, SEH, KMB, SM, RG, OMC, and TM contributed to data acquisition. CYKZ, EH, and TM analyzed, synthesized, and interpreted the data. TM supervised the study. CYKZ wrote the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the University Health Network Research Ethics Board (REB# 15-9698). Consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Adjustment for GERD status in LABW bile acid and ALAD logistic regression. Table S2. Association of BLAD with LABW bile acids in univariable logistic regression. Figure S1. A: Spearman correlation of LABW TCA levels with reflux episodes. B: Spearman correlation of LABW GCA levels with reflux episodes. C: Spearman correlation of LABW CA levels with reflux episodes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, C.Y.K., Ahmed, M., Huszti, E. et al. Utility of bile acids in large airway bronchial wash versus bronchoalveolar lavage as biomarkers of microaspiration in lung transplant recipients: a retrospective cohort study. Respir Res 23, 219 (2022). https://doi.org/10.1186/s12931-022-02131-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-022-02131-5