
Abstract
Background
Chronic Obstructive Pulmonary Disease (COPD) may be associated with accelerated aging. Telomere shortening is a biomarker of aging. Cross-sectional studies describe shorter telomeres in COPD compared with matched controls. No studies have described telomere length trajectory and its relationship with COPD progression. We investigated telomere shortening over time and its relationship to clinical and lung function parameters in a COPD cohort and smoker controls without COPD.
Methods
At baseline leukocyte telomere length was measured by qPCR in 121 smokers with COPD and 121 without COPD matched by age (T/S0). The measurements were repeated in 70 of those patients with COPD and 73 non-COPD smokers after 3 years of follow up (T/S3).
Results
At initial measurement, telomeres were shorter in COPD patients when compared to smoker controls (T/S = 0.68 ± 0.25 vs. 0.88 ± 0.52, p = 0.003) independent from age and sex. During the follow-up period, we observed an accelerated telomere shortening in individuals with COPD in contrast to smoker controls (T/S0 = 0.66 ± 0.21 vs. T/S3 = 0.46 ± 0.16, p < 0.001, for the patients with COPD and T/S0 = 0.83 ± 0.56 vs. T/S3 = 0.74 ± 0.52, p = 0.023 for controls; GLIM, p = 0.001). This shortening was inversely related to the baseline telomere length (r = −0.49, p < 0.001). No significant relationship was found between the rate of change in telomere length and change in lung function in the patients with COPD (p > 0.05).
Conclusions
Compared with smokers, patients with COPD have accelerated telomere shortening and this rate of attrition depends on baseline telomere length. Furthermore, the telomere length and its rate of shortening did not relate to clinical and lung function parameters changes over 3 years of follow-up.
Similar content being viewed by others


Background
Chronic obstructive pulmonary disease (COPD), a major cause of morbidity and mortality throughout the world, is thought to result from the interaction of environmental agents such as tobacco smoking or exposure to biomass fuel and inherited genetic factors [1]. COPD is a multidimensional disease that frequently coexists with other age-related co-morbidities such as osteoporosis, cardiovascular disease, lung cancer, depression and diabetes [2, 3].
It has been suggested that COPD is a disease of accelerated aging [4, 5] and telomere length has been proposed as a biomarker of aging [6, 7]. Telomeres consist of stretches of repetitive hexanucleotides (5´-TTAGGG-3´) that protect the end of chromosomes from being recognized as double-strand breaks and avoid truncation. Because the DNA cannot be duplicated at the end of the chromosome, each duplication results in its shortening. Thus, telomeres get progressively shorter as cells divide, an event that is known as the end-replication process. Other mechanisms may also account for the accelerated loss of telomeres, such as the DNA damage induced by oxidative stress [8].
There is no uniform acceptance of the interaction between telomere length and COPD. However, some studies have shown that patients with COPD exhibit shorter telomeres in circulating leukocytes compared to age matched smokers without COPD [9, 10]. Some authors have proposed that telomere shortening might be accelerated in patients with COPD and serve as a biomarker of disease progression [11], a theory that has some clinical support because the telomere length in peripheral leukocytes of patients with COPD has been related to important health outcomes such as all-cause and cancer mortality [12].
The unanswered question fueling the debate about the meaning of telomere shortening in patients with COPD is that all of the studies performed have been cross-sectional in design, not informing whether there are changes in length over time and whether there is any relationship between those changes and outcomes. That this is possible in COPD is highlighted by a recent study that analyzed leukocyte telomere trajectory in a cohort of individuals with coronary artery disease and found that this is powerfully influenced by baseline telomere length in a pattern suggestive of negative feedback regulation [13].
The aim of the present study was to investigate if telomere shortening occurs over time in patients with COPD and if this shortening is related to clinical and lung function parameters.
Methods
Subjects
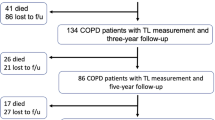
A total of 422 subjects were screened for this study at the Hospital Universitario La Candelaria, Tenerife and the Clinica Universitaria de Navarra, Pamplona, Spain. From these, the control group of 165 smokers without COPD had a smoking history of > 15 pack-years and normal lung function (FEV1 > 80%; FEV1/FVC ≥ 0.70). There were 257 smokers with COPD followed annually as part of the BODE study [14]. Inclusion criteria: age > 40 years, smoking history >15 pack-years and post-bronchodilator FEV1/FVC ratio < 0.70 measured 20 min after administration of 400 mg of albuterol. Pulmonary function test, spirometry lung volumes and exercise capacity were measured according to ATS-ERS guidelines [15–17] using the European Community for Steel and Coal as reference values [18]. Dyspnea was evaluated by mMRC scale [19]. The BODE Index was calculated as previously described [14]. Co-morbidity was quantified using the Charlson index [20]. Patients were clinically stable (no exacerbation for at least 6 weeks) at the time of evaluation. Repeated determinations of the complete blood count revealed similar values at all visits. Exclusion criteria: uncontrolled co-morbidities such as malignancy at baseline, asthma or other pulmonary conditions than COPD. From the screened group, 121 patients with COPD were matched with 121 smokers without COPD and were included in the present study for baseline comparison (Fig. 1). From these subjects, 70 patients with COPD age-matched with 73 control smokers returned for all follow-up evaluations over 3-years and were analyzed in the longitudinal study. The individuals included in the final analysis did not have any relevant clinical difference with the ones that did not complete the 3-year study (see Additional files 1 and 2). The study was approved by the institutional review board at both hospitals. All participants provided written informed consent.

Consort diagram illustrating the selection and assessment of patients and control smokers included in the study
Telomere length measurement
Venous blood was obtained at baseline and at the third-year post enrollment. DNA was extracted from leukocytes using the QIAamp DNA Mini Kit (GE Healthcare). Telomere length was measured using a qPCR based protocol previously published [21, 22]. Briefly, DNA samples were quantified using the Nanodrop lite spectrophotometer (Thermo Scientific, Wilmington, DE, USA). Telomere length measurement was performed in triplicate using 20 ng of DNA. Intra-plate coefficients of variance (CV) were calculated between the replicates and samples with CV > 5% were excluded from further analysis. As a reference DNA sample with shorter telomeres we used the DNA from MCF-7 cells. For longer telomeres, we assayed a DNA from a young control individual. These calibrator samples were assayed in triplicate on each PCR plate to control for variation between plates. Inter-assay variability was controlled by measuring two control DNA samples per run as a normalizing factor. Inter-plate CV for the calibrator sample was calculated to be <9%. Standard curves were derived from serially diluted reference DNA. Albumin, being a single copy gene, was used as a reference gene. The primer sequences and cycling conditions for the measurement of telomere length were the same used by others [22]. qPCR reactions were performed in 20 μL reactions for each individual: 10 μL SYBRGreen PCR Master Mix (BioRad), 0.9 μM of Telg and Telc and 0.6 μM of Albu and Albd. All the reactions were performed on triplicates of the telomere and reference gene assays on the iQ Cycler Real-Time PCR Instrument (BioRad).
Telomere length was calculated as a ratio of telomere to albumin as previously described [22]. The T/S ratio for an experimental DNA sample is T, the number of nanograms of the Standard DNA that matches the experimental sample for copy number of the telomere template, divided by S, the number of nanograms of the standard DNA that matches the experimental sample for copy number of the albumin single copy gene. The telomere length standardized to the reference single copy gene (T/S) was calculated using the “∆∆Cp with efficiency correction” calculation method [23].
Statistical analysis
For the cross-sectional analysis, patients with COPD were categorized in three groups by telomere length ratio (T/S) tertiles at baseline: shorter, medium or longer telomeres.
For the longitudinal analysis, telomere length changes were calculated as the difference between baseline (T/S0) and the third year (T/S3) of the telomere length measure. Individuals analyzed for follow-up were categorized as follows: subjects showing a steeper rate of telomere shortening in contrast to subjects with a lower telomere shortening rate, maintenance or lengthen of their telomeres (defined by the median telomere length change).
A t-Student, ANOVA, Chi2 and Paired Sample T test were used to test differences in means and proportions of baseline and follow-up characteristics between groups. The association between baseline telomere length (T/S) or telomere length change with clinical and/or pulmonary function variables was explored using Pearson’s correlation coefficients. A multiple logistic regression was performed to test the association of telomere length with COPD susceptibility adjusting for age, sex and pack years. By using a general linear modelling for repeated measures (GLIM) we tested the telomere dynamics difference between patients with COPD and smokers without COPD, or within these groups between current and former smokers. We also conducted a longitudinal analysis to evaluate the progression of the disease of clinical and pulmonary function variables using change in telomere length as comparative factor (GLIM). SPSS 20.0 IBM Co software was used for all statistical analyses and two-tailed p-values < 0.05 were considered significant.
Results
Baseline findings
The clinical characteristics and lung function data of the 121 COPD patients and 121 controls at baseline, are summarized in Table 1. The range of airflow obstruction distributed by GOLD stages in COPD was as follows: 1 (19.8%), 2 (43%), 3 (28.9%) and 4 (8.3%). As expected, patients with COPD had worse lung function and a higher BODE index than controls. However, the two groups were similar in age, sex, BMI and Charlson co-morbidity score. Although the total pack years smoking was higher in COPD patients, there were more current smokers in the control group. Telomere length measured by the T/S ratio inversely correlated with age in COPD (r = −0.21; p = 0.02) and in smoker controls (r = −0.19; p = 0.02). Given this relationship, all subsequent analyses were adjusted by age.
COPD patients had significant shorter telomeres than smokers without COPD (T/S = 0.68 ± 0.25 vs. 0.88 ± 0.52, p < 0.0001) even after adjusting for age, sex and pack-years (95% CI: 0.11–0.64, p = 0.003), (Table 1 and Fig. 2). There were no significant differences between males (0.68 ± 0.28) and females (0.66 ± 0.20) within the COPD group or in the smokers (0.82 ± 0.53 vs. 0.96 ± 0.49 for males and females, respectively).

Average telomere length and SE relative telomere length (T/S) in COPD patients (n = 121) vs. age-matched smokers without COPD (n = 121)
There was no relationship between telomere length and the clinical and lung function parameters (Table 2) or between patients with less and more severe COPD (GOLD 1–2 vs. GOLD 3–4 or BODE ≤2 vs. BODE > 2) (p > 0.05). In addition, no significant associations were found between comorbidities such as cardiovascular events, diabetes, hypertension or cancer and relative telomere length in patients with COPD.
Telomere length dynamics
This difference in telomere length remained significant after 3 years between the 70 patients with COPD age matched with 73 smoker controls that presented the follow-up (T/S3 = 0.46 ± 0.16 vs. 0.74 ± 0.52, p < 0.001); even after adjusting for age, sex and smoking habit in a logistic regression analysis (95% CI: 0.12–0.90), p = 0.03).
The telomere length ratio in the control group of smokers without COPD, decreased significantly (T/S0 = 0.83 ± 0.56 vs. T/S3 = 0.74 ± 0.52, p = 0.002) after the follow-up period. The same occurred in the group of patients with COPD (T/S0 = 0.66 ± 0.21 vs. T/S3 = 0.46 ± 0.16, p < 0.001). However, when we compared the telomere trajectory between these groups over the follow-up period, we observed an accelerated telomere shortening in individuals with COPD in contrast to the control group (GLIM, general lineal model for repetitive measures, p = 0.001) (Fig. 3).

Telomere length (relative T/S ratio) dynamics in COPD patients (n = 70) vs. age-matched smokers without COPD (n = 73) after 3 years’ follow-up (p = 0.001, using GLIM - general lineal model for repetitive measures; T/S differences between groups p(T/Sxgroups)=0.002)
Relation of telomere length change and clinical variables
We found a strong relationship between baseline telomere length and change in telomere length (r = −0.49, p < 0.001; adjusted by age) (Fig. 4).

Correlation between baseline telomere length and the rate of change in telomere shortening in COPD patients after 3 years’ follow-up (r = −0.49, p = 0.001, adjusted by age)
Compared with COPD patients that did not change, lengthened or had a low rate of telomere shortening, those patients with a more rapid shortening of their telomeres had similar lung function characteristics (Table 3).
By using correlation matrices, we were not able to find any significant relationship between the rate of change in telomere length and change in lung function in the patients with COPD (see Additional file 3). This lack of association was seen whether we compared current vs. former smokers, number of comorbidities or mortality (Chi2, p > 0.05).
Discussion
This longitudinal study shows that COPD patients experience an accelerated telomere shortening process compared with smokers without COPD and this telomere attrition occurs in close relation to baseline telomere length. The study also confirms that patients with COPD have shorter telomeres than smokers who do not have COPD. However, there were no associations between telomere length and clinical and lung function parameters at baseline or between changes in telomere length and change in those parameters overtime. To our knowledge, this is the first study reporting the course of telomere length change in a well-characterized cohort of patients with COPD and smoker controls.
Telomere length and change over time
In our study, at baseline, telomere length was shorter with older age, both in the COPD patients and the smokers without COPD. However, COPD patients presented shorter telomeres than the control group independent of age and sex. Other studies evaluating the relation between telomere length and COPD have shown discordant results. Morla et al. [24] failed to find a difference in telomere length between COPD patients and smokers, whereas some other studies have reported shorter telomeres in subjects with COPD compared to smokers and healthy individuals [8, 10]. These discordant results may have been due to differences in sample size in the studies or by technical bias or defects in study design, some of which lacked of appropriate controls. We found no relationship between telomere length and clinical or lung function parameters in our COPD cohort in the cross-sectional analysis. This is in agreement with the results of Savale et al. [9] who described a borderline correlation between PaO2 and PaCO2 and telomere length but strangely not to lung function parameters. However, Rode et al. [25] in a study of more than 45.000 individuals in a Danish population reported a modest correlation between telomere length and the lung function expressed by the FEV1. More recently, Rutten et al. studying several markers of aging in patients with COPD, found telomere length to be the only one associated with lung function [26]. All these studies were cross-sectional in design and in consequence not adequate to evaluate the possible relationship between telomere length and COPD progression. In addition, the only lung function parameter evaluated was FEV1 and patients with comorbidities were excluded.
The current report is the first one to document that COPD patients have an accelerated rate of telomere shortening in contrast to smoker controls, and this difference was more marked in those individuals with longer baseline telomeres. In our study, 85% of the COPD patients showed telomere length shortening after 3 years of follow-up, a proportion that is similar to that observed in general population studies [27–29], however, the rate of decline is significantly lower in those normal individuals. It is important to compare our findings with that of other populations including different pathologies. Fazarneh et al. [13] analyzed leukocyte telomere trajectory over 5 years in a cohort of individuals with coronary artery disease and found, as we have, that telomere shortening rate is powerfully influenced by baseline telomere length. Our results support a pattern suggestive of negative feedback regulation in the telomere shortening dynamics, as has been proposed by others [29]. It may be that once a critical telomere length has been reached, activation of certain mechanisms in the cells occur to prevent telomere shortening over years accounting for less attrition per replication or maintenance of viable telomere lengths in subjects with shorter telomeres.
The exact reason why telomeres shorten faster in patients with COPD was beyond the scope of this study. However, oxidative stress and inflammation are the most important factors thought to be responsible for the loss of telomeric DNA [8], which in turn may favor the development of structural tissue damage [30]. Studies on mouse models of accelerated aging and lung dysfunction, suggested that this process might enhance susceptibility to COPD [5].
Telomere length and clinical variables
Previous cross-sectional studies have concentrated primarily on the relationship between telomere length and the FEV1. We expanded on those studies relating not only FEV1, but also lung hyperinflation (IC/TLC), diffusion capacity (KCO) and gas exchange to telomere length. Disappointingly, we were unable to document any association between telomere length in COPD patients with any clinical or functional expression of the disease or presence of any comorbidities at baseline. This is in general agreement with most of the published studies that have reported poor associations, if any, between the actual telomere length and the FEV1. Of interest, the studies that have described an association between telomere shortening and lower FEV1 have included larger sample size, thus facilitating a statistical significance to those findings. This is important when attempting to relate statistical associations to practical the clinical application of those findings.
Because the value of a biomarker resides primarily in its capacity to reflect association to prognosis or to change in disease progression, we followed patients and controls over 3 years. We observed no correlation between the rate of shortening of telomeres and the change in lung function, or for that matter with any other clinical variable, rendering those findings difficult to interpret of to apply clinically. Perhaps, a longer period of observation or a larger sample may be necessary to evaluate these clinical and physiological variables or other patient related outcomes such as exacerbations, cardiovascular events and all-cause mortality. On the other hand, these findings suggest that the rate of telomere shortening may not be a viable surrogate marker of disease progression of major clinical utility.
This study has several limitations. Telomere length was measured on circulating leukocytes and therefore our findings may not reflect the process occurring in the whole lung. Interestingly, telomere length in blood correlates well with telomere length in lung tissue of COPD [31] and rates of telomere shortening are similar in different tissues [32]. We used qPCR relative telomere length measures rather than absolute ones which may result in a loss of precision, however qPCR results were reported to be strongly correlated those obtained with southern blot technique [22]. Leukocyte telomere length is also considered a marker of oxidative stress and inflammation, and both contribute to COPD development. Telomere length is determined by environmental as well as genetic factors. There is a large inter-individual variability in telomere length in humans of the same age that makes difficult any cross-sectional comparisons. Our control smokers presented a shorter tobacco exposure history than the cohort of patients with COPD. However, analysis between current vs. former smokers in both cohorts did not show significantly differences. Another limitation is that the sample size or duration of observation (3 years) may not have been large or long enough to find significant associations between telomere shortening and lung function parameters. In this context, we cannot discard that our findings may be affected by regression towards the mean. Further studies with a larger follow-up period with many time points of measurements are needed to validate these findings. However, for implementation of precision medicine, biomarkers need to have clinical applicability in small numbers, if not in individuals. Lastly, we did not investigate other markers of aging; however, other authors who have done so, and have found telomere length to be the most relevant of all [26].
Conclusions
In summary, in this longitudinal observational study we found that compared with smoker controls, an accelerated telomere shortening occurs in patients with COPD, even if they had shorter telomeres at baseline. Interestingly, the speed of shortening relates inversely to baseline telomere length. However, the telomere length and its rate of shortening did not relate to clinical and lung function parameters and their change over time, making telomere length change an unlikely useful biomarker of COPD progression.
Abbreviations
- 6MWD:
-
6-min walk distance
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
- FEV1 :
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- GLIM:
-
General linear modelling for repeated measures test
- GOLD:
-
Global initiative for chronic obstructive lung disease
- IC/TLC:
-
Inspiratory to total lung capacity ratio
- KCO :
-
Diffusion capacity of carbon monoxide
- N.S.:
-
Non-significant
- PaO2 :
-
Partial oxygen tension
- pPCR:
-
Quantitative real time polymerase chain reaction
- SD:
-
Standard deviation
- T/S:
-
Relative telomere length ratio
- T/S0 :
-
Relative telomere length ratio at baseline
- T/S3 :
-
Relative telomere length ratio at the third year of follow-up
References
Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–65.
Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Resp J. 2009;33:1165–85.
Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:155–61.
Ito K, Barnes PJ. COPD as a disease of accelerated lung aging. Chest. 2009;135:173–80.
Maciewicz RA, Warburton D, Rennard SI. Can increased understanding of the role of lung development and aging drive new advances in chronic obstructive pulmonary disease? Proc Am Thorac Soc. 2009;6:614–7.
Mather KA, Jorm AF, Parslow RA, et al. Is telomere length a biomarker of aging? A review. J Gerontol A Biol Sci Med Sci. 2011;66(2):202–13.
Armanios M. Telomeres and age-related disease: how telomere biology informs clinical paradigms. J Clin Invest. 2013;123:996–1002.
Houben JM, Moonen HJ, van Schooten FJ, et al. Telomere length assessment: biomarker of chronic oxidative stress? Free Radic Biol Med. 2008;44:235–46.
Savale L, Chaouat A, Bastuji-Garin S, et al. Shortened telomeres in circulating leukocytes of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2009;179:566–71.
Mui TS, Man JM, McElhaney JE, et al. Telomere length and chronic obstructive pulmonary disease: evidence of accelerated aging. J Am Geriatr Soc. 2009;57:2372–4.
Houben JM, Mercken EM, Ketelslegers HB, et al. Telomere shortening in chronic obstructive pulmonary disease. Respir Med. 2009;103:230–6.
Lee J, Sandford AJ, Connett JE, et al. The relationship between telomere length and mortality in chronic obstructive pulmonary disease (COPD). PLoS One. 2012;7, e35567.
Farzaneh-Far R, Lin J, Epel E, et al. Telomere length trajectory and its determinants in persons with coronary artery disease: longitudinal findings from the heart and soul study. PLoS One. 2010;5, e8612.
Celli BR, Cote C, Marin JM, Casanova C, et al. The body mass index, airflow obstruction, dyspnea, exercise performance (BODE) index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:1005–12.
American Thoracic Society Statement. Lung function testing: selection of reference values and interpretative strategies. Am Rev Respir Dis. 1991;144:1202–18.
Macintyre N, Crapo RO, Viegi G, et al. Standardization of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005;26:720–35.
Statement ATS. Guidelines for the six-minute walk test. Am J Resp Crit Care Med. 2002;166:111–7.
Quanjer PH. Standardized lung function testing. Report of the working party for the European community for steel and coal. Bull Eur Physiopathol Respir. 1983;5:22e7.
Mahler D, Wells C. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93:580e6.
Charlson M, Szatrowski T, Peterson J, et al. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245e51.
Cawthon RM. Telomere measurement by quantitative PCR. Nucleic Acids Res. 2002;30, e47.
Cawthon RM. Telomere length measurement by a novel monochrome multiplex quantitative PCR method. Nucleic Acids Res. 2009;37, e21.
Pfaffl MW. A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 2001;29, e45.
Morlá M, Busquets X, Pons J, et al. Telomere shortening in smokers with and without COPD. Eur Respir J. 2006;27:525–8.
Rode L, Bojesen SE, Weischer M, et al. Short telomere length, lung function and chronic obstructive pulmonary disease in 46,396 individuals. Thorax. 2013;68:429–35.
Rutten EP, Gopal P, Wouters EF, Franssen FM, Hageman GJ, Vanfleteren LE, Spruit MA, Reynaert NL. Various mechanistic pathways representing the aging process are altered in COPD. Chest. 2016;149:53–61.
Gardner JP, Li S, Srinivasan S, et al. Rise in insulin resistance is associated with escalated telomere attrition. Circulation. 2005;111:2171–7.
Masi S, D'Aiuto F, Martin-Ruiz C, et al. Rate of telomere shortening and cardiovascular damage: a longitudinal study in the 1946 British Birth Cohort. Eur Heart J. 2014;35:3296–303.
Epel ES, Merkin SS, Cawthon R, et al. The rate of leukocyte telomere shortening predicts mortality from cardiovascular disease in elderly men. Aging (Albany NY). 2008;1:81–8.
Lee MS, Yaar M, Eller MS, et al. Telomeric DNA induces p53-dependent reactive oxygen species and protects against oxidative damage. J Dermatol Sci. 2009;56:154–62.
Saferali A, Lee J, Sin DD, et al. Longer telomere length in COPD patients with α1-antitrypsin deficiency independent of lung function. PLoS One. 2014;9, e95600.
Daniali L, Benetos A, Susser E, Kark JD, Labat C, Kimura M, Desai K, Granick M, Aviv A. Telomeres shorten at equivalent rates in somatic tissues of adults. Nat Commun. 2013;4:1597.
Acknowledgments
We will like to thank Angela Montejo-de-Garcini, Hilaria González Acosta and Delia Mayato for their excellent technical assistance. We are also thankful to Antonio Gonzalez Biorganic Institute (Tenerife, Spain) for their kindly donation of the MCF-7 cells line.
Funding
The study was supported by the Instituto de Salud Carlos III (PI 12/00355); European Regional Development Funds, ERDF, and Spanish Respiratory Society, SEPAR (PI 13/007).
Availability of data and materials
Any requests for data and material should be directed to the corresponding author.
Authors´ contributions
E.C.L. and C.C. participated in conception and design; analysis and interpretation and drafting the manuscript for important intellectual content. S.C.R., A.E.J. and A.A.J. participated in analysis and interpretation. B.C. participated in the interpretation of the results and helped draft the manuscript for important intellectual content. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval was obtained from Hospital Universitario La Candelaria, Tenerife and the Clinica Universitaria de Navarra, Pamplona, Spain. Written informed consent was obtained from all participants.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional information
The original version of this article was revised to correct author names.
An erratum to this article is available at http://dx.doi.org/10.1186/s12931-017-0589-7.
Additional files
Additional file 1:
Baseline characteristics of COPD patients with and without three-year follow-up included in the study. (DOCX 14 kb)
Additional file 2:
Baseline characteristics of smokers without COPD with and without three-year follow-up included in the study. (DOCX 75 kb)
Additional file 3:
Correlations between the rate of change in telomere length and the change in pulmonary function variables in patients with COPD after three years of follow-up. (DOCX 68 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Córdoba-Lanús, E., Cazorla-Rivero, S., Espinoza-Jiménez, A. et al. Telomere shortening and accelerated aging in COPD: findings from the BODE cohort. Respir Res 18, 59 (2017). https://doi.org/10.1186/s12931-017-0547-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-017-0547-4