
Abstract
Background
The International Classification of Diseases (ICD) has been grouping the allergic and hypersensitivity disorders involving the respiratory tract under topographic distribution, regardless of the underlying mechanisms, triggers or concepts currently in use for allergic and hypersensitivity conditions. In order to strengthen awareness and deliberate the creation of the new “Allergic or hypersensitivity disorders involving the respiratory tract” section of the ICD-11, we here propose make the building process public.
Methods
The new frame has been constructed to cover the gaps previously identified and was based on consensus academic reports and ICD-11 principles. Constant and bilateral discussion was kept with relevant groups representing specialties and resulted in proposals submission into the ICD-11 online platform.
Results
The “Allergic or hypersensitivity disorders involving the respiratory tract” section covers 64 entities distributed across five main categories. All the 79 proposals submitted resulted from an intensive collaboration of the Allergy working group, relevant Expert working groups and the WHO ICD governance.
Conclusion
The establishment of the ICD-11 “Allergic or hypersensitivity disorders involving the respiratory tract” section will allow the dissemination of the updated concepts to be used in clinical practice by many different specialties and health professionals.
Similar content being viewed by others

Background
Allergic and hypersensitivity disorders involving the respiratory tract
The World Health Organization (WHO) defines non-communicable chronic respiratory diseases (CRDs) as conditions of the airways and other structures of the lung, such as asthma, chronic obstructive pulmonary diseases (COPD), occupational lung diseases, cystic fibrosis and pulmonary hypertension. Changes in life-style and in exposure to environmental pollutants and allergens have increased both the prevalence and the severity of CRDs in different age groups, with increased impact on quality of life and healthcare costs, as has been shown particularly for asthma.
Over the last few decades, the world has been facing an asthma and allergy epidemic, becoming a serious public health problem and a prominent cause of disability and mortality worldwide. The WHO estimates that about 235 million people currently suffer from asthma [1]. Although most common in childhood, asthma can persist into adulthood and the prevalence can vary widely across the age groups [1].
Though asthma mortality rates are higher in lower and lower-middle income countries, it has been accepted as a major public health problem in all countries. Among the European Union (EU) member states, asthma accounted for an average of 53 hospital admissions per 100,000 inhabitants in 2009 [2]. The annual direct and indirect costs in European countries due to asthma are estimated at €22,2 billion and €16,4 billion respectively per year. Data on the value of disability-adjusted life-years lost due to asthma obtained from WHO Health Statistics 2011 and the Global Burden of Disease study indicate an estimated monetized total cost of €43.2 billion [3, 4].
Allergic and hypersensitivity disorders involving the respiratory tract comprise a range of different clinical presentations including asthma, rhinitis, and pneumonitis among others. They can manifest at any age and in differing degrees of severity, frequently giving rise to a significant impact on the quality of life of patients and their families. They are likely to be encountered at some stage by every health professional.
Many international initiatives have been launched to prevent and decrease the negative outcome of these conditions, which are considered a global health problem [5, 6]. However, international classification and coding systems such as the International Classification of Diseases (ICD) have grouped them under topographic distribution, regardless of the underlying mechanisms and triggers. This has led to the framework of both the 10th and draft 11th revisions of ICD (ICD-10 2010 version and ICD-11 beta draft as at May 2014 respectively) to be deficient in capturing the concepts currently in use for allergic and hypersensitivity conditions [7]. These findings highlight the need for the major respiratory societies to be involved in updating the representation of allergic and hypersensitivity disorders involving the respiratory tract in the ongoing ICD-11 revision.
Rationale for updating allergic and hypersensitivity disorders involving the respiratory tract in the ICD-11 framework
The allergy specialty scope
Allergy and clinical immunology, while perceived as a secondary discipline in some medical communities, has been increasingly recognized around the world as a key specialty in its own right [8, 9]. Unlike many other specialties, which focus mostly on specific organ systems, the allergy discipline is a cross-cutting specialty, which transcends such boundaries, in that allergists deal with conditions involving multiple systems, often managing them jointly with colleagues from “sister specialties” such as respiratory medicine, pediatrics, dermatology, ophthalmology, otorhinolaryngology and gastroenterology. However, the terms currently used on a daily basis by allergists are not all widely known by practitioners from the “sister specialties” and their absence from health classification and coding systems contributing to the misclassification and/or under-representation of these entities in official health statistics and, as a consequence, a tremendous negative impact at many different levels on the management of allergic disorders.
Understanding of the underlying mechanisms
Medical science’s understanding of the immune system has advanced significantly over the last decade having positive implications for both research and clinical practice. This development has led to an increasing number of commercially available diagnostic tools as well as a number of new products for the management of allergic and hypersensitivity conditions. In general, there is now an accepted understanding of the mechanisms underlying the most important of them, enabling a comprehensive range of “stem” concepts to be incorporated into ICD-11. The “stem” concepts can then be further characterized by appending further detail (e.g. triggers, chronology and severity grading) to produce a sophisticated post-coordinated expression (e.g. Drug-induced anaphylaxis: grade III: due to benzylpenicillin).
From a public health perspective
Integration of a comprehensive allergic and hypersensitivity conditions classification into national and international health information systems is crucial to the identification of their health impact at both a national and a global level and to help identify service deficiencies and provide the motivation for change. Misconceptions about and under-representation of common allergic disorders in healthcare coding systems hinder clinical research and contribute to a lack of ascertainment and poor recognition of their importance for health care planning, resource allocation and reimbursement.
For these reasons, we have considered it timely to update the representation of allergic and hypersensitivity conditions within ICD [10].
Methods
Allergy perspective of the ICD-11 revision
The ICD is a system of classifying medical diagnoses, developed and periodically revised by the WHO, providing a common language both for health records and for epidemiological analyses of disease. The WHO started to work on ICD-11 in 2007. A Revision Steering Group (RSG) has overseen some 18 content-specific Topic Advisory Groups (TAGs), each charged with updating sections of the classification relevant to it, in collaboration where necessary with other TAGs [10]. As new proposals come forward they can be viewed and commented upon the online ICD-11 beta draft [11].
The structure of ICD-11 is more complex than that of its predecessors in that it is based on a ”Foundation” from which a suite of different classifications or “views” can be extracted, of which the principal is the core ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS), the direct replacement for ICD-10. The current plans envisage that ICD-11 MMS will be finalized in 2018. In addition to the ICD-11 MMS this there is scope for more detailed specialty classifications, which could include one for Allergic disorders. The polyhierarchical structure of the Foundation, in which an entity may have more than one hierarchical parent, permits a single condition to be represented in more than one location, as explained in more detail below.
In contrast to previous revisions, the current ICD-11 draft is housed online and can receive external proposals for consideration by the TAGs, RSG and WHO.
Realizing that the current ICD revision would offer a unique opportunity to reach a better classification, definition and standardization of allergic and hypersensitivity conditions, an international collaboration of Allergy Academies has convened an Allergy Working Group (AWG) which has worked tirelessly since 2013 on providing scientific evidence to support the need for change and on developing an improved and up-to-date classification of allergic disorders.
The actions so far have been supported and acknowledged by the WHO ICD Revision Project staff, with whom the AWG has been keeping bilateral continuous dialog, and have been documented by a series of peer-reviewed publications [7, 12–19]. The construction of the “Allergic and hypersensitivity conditions” section of the new ICD-11 chapter “Disorders of the immune system” has involved numerous steps and would not have been possible if the AWG had not undertaken constant discussions with the relevant TAGs [11].
Results
Classification of allergic or hypersensitivity disorders involving the respiratory tract
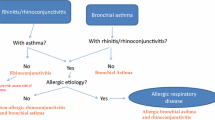
The section of ICD-11 entitled “Allergic and hypersensitivity disorders involving the respiratory tract” has been constructed with full agreement of the involved TAGs and Expert Working Groups (EWGs) (Fig. 1). The structure was based on the overall design of the section “Allergic and hypersensitivity diseases”, which was validated by crowd-sourcing and simplified according to guidance from members of the RSG. The discussion had the scientific and technical basis to ensure comparability and consistency. An intensive exchange of e-mails, tele- and video-conferences started in February 2014 and was the basis for what was submitted into the online ICD-11 beta draft proposal platform. All the actions of the AWG have been undertaken with RSG guidance.

Collaboration between specialties for the construction of the “Allergic or hypersensitivity disorders involving the respiratory tract” (TAG = Topic Advisory Group)
The ICD-11 beta draft supports a proposal system in which four main types of proposal are possible: i) content enhancement proposal, ii) addition of new child entity to an existing entity iii) deletion of an existing entity and iv) complex hierarchical changes (Fig. 2). Each submitted proposal has to be supported by a rationale and peer-reviewed references, and must follow an established “content model”. The ICD-11 content model incorporates: title, definition, synonyms, narrower terms, exclusions, body system, body site, signs and symptoms, causal agents and causal mechanisms [10]. The ICD-11 beta draft platform [11] can be considered a WHO web-observatory in which the members of the RSG and TAGs can monitor proposal submissions and comments and can recommend implementation or rejection of proposals.

Purposes of the four main proposal type available in the ICD-11 beta draft platform
The AWG carried out discussions with the relevant TAGs and EWGs with whom it shared common interests; we started the submission process as soon as we reached a consensus was reached. Most of the proposals for the construction of this section were submitted between February and April 2014 but improvements have continued to be made based on comments received. During this process, the AWG submitted a total of 79 proposals, most of which (87.3%) have been implemented (Fig. 3). We did not identify any entities which required to be deleted.

Proposals submitted into the ICD-11 beta draft platform (November 2015 version) for the construction of the “Allergic and hypersensitivity disorders involving the respiratory tract”
Currently, the respiratory tract allergy and hypersensitivity classification contains 64 entities distributed across 5 main categories: i) Allergic and non-allergic rhinitis, ii) Hypersensitivity pneumonitis, iii) Aspergillus-induced allergic or hypersensitivity conditions, iv) Chronic rhinosinusitis and v) Asthma. Two further entities have been added more recently: “Drug-induced bronchospasm” and “Bronchospasm provoked by allergy to food substance” (Fig. 4).

The current “Allergic and hypersensitivity disorders involving the respiratory tract” section of the ICD-11 beta draft platform (November 2015 version)
As explained above the ICD-11 Foundation is a polyhierarchical construct. Both entities Samter syndrome and Allergic Aspergillus rhinosinusitis are represented in two categories, meaning that Samter syndrome is displayed in the ICD-11 Foundation as a child both of Chronic rhinosinusitis and of Other specified asthma; and Allergic Aspergillus rhinosinusitis is displayed similarly as a child both of Aspergillus-induced allergic or hypersensitivity conditions and of Chronic rhinosinusitis. Although allergic ocular conditions, such as allergic conjunctivitis usually coexist with respiratory allergies, we did not include these disorders under the “Allergic or hypersensitivity disorders involving the respiratory tract” section since they are classified under a specific section named “Allergic or hypersensitivity disorders involving the eye”.
The ICD-11 MMS permits only one hierarchical parent for a given entity but does display entities that are located primarily elsewhere to be shown as cross-references in gray. As a consequence many of the entities to be found in the “Allergic or hypersensitivity disorders involving the respiratory tract “ section of the ICD-11 MMS are shown as cross-references from the “Diseases of the respiratory system” chapter.
Discussion
Lessons of the building process
The construction of a classification of respiratory allergies was a labor-intensive and complicated process. The classification forms only a part of the new section on Allergic and hypersensitivity conditions which WHO has accepted for inclusion in the new Disorders of the immune system chapter in ICD-11, thus for the first time enabling these disorders to be properly represented in ICD.
In view of the fact that “Allergy” as a specialty crosses boundaries between disciplines, many allergic and hypersensitivity conditions are also relevant to other specialties. Intensive cooperation between the representatives of different specialties enabled consensus to be reached for the construction of the “Allergic or hypersensitivity disorders involving the respiratory tract” section. As an example the proposal that “Bronchospasm provoked by allergy to food substances” should be placed within “Allergic or hypersensitivity disorders involving the respiratory tract” was put forward by the Dermatology TAG and then agreed by the Respiratory EWG of the Internal Medicine TAG, the AWG and the Pediatric TAG.
More than a mere discussion of classification, these interactions helped us to develop a common vision for handling concepts, terminology and ontology. Throughout this systematic process and after a fruitful discussion we were able to capture the “external” real understanding of how allergy and hypersensitivity conditions are perceived by others. This provided us with a global view of the key issues to be managed in order to strengthen the allergy specialty.
Conclusion
The establishment of the ICD-11 “Allergic or hypersensitivity disorders involving the respiratory tract” section, as well as the other sessions of the “Allergic and hypersensitivity conditions” chapter will allow the dissemination of the updated concepts to be used in clinical practice by many different specialties and health professionals.
Abbreviations
- AWG:
-
Allergy working group
- CRDs:
-
Chronic respiratory diseases
- COPD:
-
Chronic obstructive pulmonary diseases
- EU:
-
European Union
- EWGs:
-
Expert working groups
- ICD:
-
International classification of diseases
- ICD-11 MMS:
-
ICD-11 for mortality and morbidity statistics
- RSG:
-
Revision steering group
- TAGs:
-
Topic advisory groups
- WHO:
-
World Health Organization
References
World Health Organization website (cited, available: http://www.who.int/en/), Accessed Nov 2015.
Gibson GJ, Loddenkemper R, Sibille Y, Lundback B. The European Respiratory White Book. European Respiratory Society. Available: http://www.erswhitebook.org/chapters/the-economic-burden-of-lung-disease/the-cost-of-respiratory-disease/.
WHO Department of Health Statistics and Informatics of the Innovation, Information, Evidence and Research Cluster. WHO Health Statistics 2011. Available: http://www.who.int/gho/publications/world_health_statistics/EN_WHS2011_Full.pdf.
WHO Department of Health Statistics and Informatics of the Innovation, Information, Evidence and Research Cluster. Burden of Diseases: DALYs. Available: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_part4.pdf.
Bousquet J, Addis A, Adcock I, Agache A, Agusti A, Alonso A, et al. Integrated care pathways for airway diseases (AIRWAYS-ICPs). Eur Respir J. 2014;44(2):304–23.
Bousquet J, Dahl R, Khaltaev N. Global alliance against chronic respiratory diseases. Allergy. 2007;62:216–23.
Tanno LK, Calderon MA, Goldberg BJ, Akdis CA, Papadopoulos NG, Demoly P. Categorization of allergic disorders in the new world health organization international classification of diseases. Clin Transl Allergy. 2014;4:42.
De Monchy JG, Demoly P, Akdis CA, Cardona V, Papadopoulos NG, Schmid-Grendelmeier P, Gayraud J. Allergology in Europe, the blueprint. Allergy. 2013;68:1211–8.
Del Giacco S, Rosenwasser LJ, Crisi CD, Frew AJ, Kaliner MA, Lee BW, et al. What is an allergist? reconciled document incorporating member society comments. World Allergy Organ J. 2008;1(1):19–20.
World Health Organization ICD revision website (cited, available: http://www.who.int/classifications/icd/en/). Accessed Nov 2015.
World Health Organization ICD-11 Beta Draft website. (cited, available: http://apps.who.int/classifications/icd11/browse/l-m/en#/). Accessed Nov 2015.
Tanno LK, Ganem F, Demoly P, Toscano CM, Bierrenbach AL. Undernotification of anaphylaxis deaths in Brazil due to difficult coding under the ICD-10. Allergy. 2012;67:783–9.
Demoly P, Tanno LK, Akdis CA, Lau S, Calderon MA, Santos AF, Sanchez-Borges M, Rosenwasser LJ, Pawankar R, Papadopoulos NG. Global classification and coding of hypersensitivity diseases – An EAACI – WAO survey, strategic paper and review. Allergy. 2014;69:559–70.
Tanno LK, Calderon MA, Goldberg BJ, Gayraud J, Bircher AJ, Casale T, Li J, Sanchez-Borges M, Rosenwasser LJ, Pawankar R, Papadopoulos NG, Demoly P. Constructing a classification of hypersensitivity/allergic diseases for ICD-11 by crowdsourcing the allergist community. Allergy. 2015;70:609–15.
Tanno LK, Calderon MA, Papadopoulos NG, Demoly P. Mapping hypersensitivity/allergic diseases in the International Classification of Diseases (ICD)-11: cross-linking terms and unmet needs. Clin Transl Allergy. 2015;5:20.
Tanno LK, Calderon MA, Demoly P. Making allergic and hypersensitivity conditions visible in the International Classification of Diseases-11. Asia Pac Allergy. 2015;5:1–1.
Tanno LK, Calderon MA, Demoly P, on behalf the Joint Allergy Academies. New allergic and hypersensitivity conditions section in the international classification of diseases-11. Allergy Asthma Immunol Res. 2016;8(4):383–8. doi:10.4168/aair.2016.8.4.383.
Tanno LK, Calderon MA, Papadopoulos NG, Sanchez-Borges M, Rosenwasser LJ, Bousquet J, et al. Revisiting desensitization and allergen immunotherapy concepts for the international classification of diseases (icd)-11. J Allergy Clin Immunol Pract. 2016;4(4):643–9. doi:10.1016/j.jaip.2015.12.022.
Tanno LK, Calderon MA, Li J, Casale T, Demoly P. Updating allergy/hypersensitivity diagnostic procedures in the WHO ICD-11 revision. J Allergy Clin Immunol Pract. 2016;4(4):650–7. doi:10.1016/j.jaip.2016.01.015.
Acknowledgement
We are extremely grateful to all the representatives of the ICD-11 revision with whom we have been carrying on fruitful discussions, helping us to tune the here presented classification: Robert Jakob, Linda Best, Robert J G Chalmers, Jeffrey Linzer, Linda Edwards, Ségolène Ayme, Bertrand Bellet, Rodney Franklin, Matthew Helbert, August Colenbrander, Satoshi Kashii, Paulo E. C. Dantas, Christine Graham, Ashley Behrens, Julie Rust, Megan Cumerlato, Tsutomu Suzuki, Mitsuko Kondo, Hajime Takizawa, Nobuoki Kohno, Soichiro Miura, Nan Tajima and Toshio Ogawa.
Joint Allergy Academies: American Academy Of Allergy Asthma And Immunology (AAAAI), European Academy of Allergy and Clinical Immunology (EAACI), World Allergy Organization (WAO), American College of Allergy Asthma and Immunology (ACAAI), Asia Pacific Association of Allergy, Asthma and Clinical Immunology (APAAACI), Latin American Society of Allergy, Asthma and Immunology (SLAAI)
Funding
Pascal Demoly and Luciana Kase Tanno received an unrestricted AstraZeneca ERS-16-11927 grant through CHRUM administration.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available in the World Health Organization. ICD-11 Beta Draft website (URL: http://apps.who.int/classifications/icd11/browse/f/en).
Author’s contributions
LKT and PD contributed to the construction of the document (designed the study, analyzed and interpreted the data, and wrote the manuscript). MAC contributed in tuning the document and with the revision of the manuscript.
Competing interests
The authors declare that they do not have any conflict of interests related to the contents of this article.
Consent for publication
No consent for publication has been required since this study does not involve patients. This study is based on an online opened platform.
Ethics approval and consent to participate
No consent form or ethical statement has been required since this study does not involve patients or animals. This study is based on an online opened platform.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tanno, L.K., Calderon, M., Linzer, J.F. et al. Collaboration between specialties for respiratory allergies in the International Classification of Diseases (ICD)-11. Respir Res 18, 34 (2017). https://doi.org/10.1186/s12931-017-0513-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-017-0513-1