
Abstract
Background
Urothelial carcinoma (UC) is the most common neoplasm of the canine lower urinary tract, affecting approximately 2% of dogs. Elderly female patients of certain breeds are predisposed, and clinical signs of UC can easily be confused with urinary tract infection or urolithiasis. Diagnosis and treatment are challenging given the lack of disease-specific markers and treatments. The S100A8/A9 complex and S100A12 protein are Ca2+-binding proteins expressed by cells of the innate immune system and have shown promise as urinary screening markers for UC. The neutrophil-to-lymphocyte ratio (NLR) can also aid in distinguishing certain neoplastic from inflammatory conditions. Our study aimed to evaluate the tissue expression of S100/calgranulins and the blood NLR in dogs with UC. Urinary bladder and/or urethral tissue samples from dogs with UC (n = 10), non-neoplastic inflammatory lesions (NNUTD; n = 6), and no histologic changes (n = 11) were evaluated using immunohistochemistry. Blood NLRs were analyzed in dogs with UC (n = 22) or NNUTD (n = 26).
Results
Tissue S100A12-positive cell counts were significantly higher in dogs with lower urinary tract disease than healthy controls (P = 0.0267 for UC, P = 0.0049 for NNUTD), with no significant difference between UC and NNUTD patients. Tissue S100A8/A9-positivity appeared to be higher with NNUTD than UC, but this difference did not reach statistical significance. The S100A8/A9+-to-S100A12+ ratio was significantly decreased in neoplastic and inflamed lower urinary tract tissue compared to histologically normal specimens (P = 0.0062 for UC, P = 0.0030 for NNUTD). NLRs were significantly higher in dogs with UC than in dogs with NNUTD, and a cut-off NLR of ≤ 2.83 distinguished UC from NNUTD with 41% sensitivity and 100% specificity. Higher NLRs were also associated with a poor overall survival time (P = 0.0417).
Conclusions
These results confirm that the S100/calgranulins play a role in the immune response to inflammatory and neoplastic lower urinary tract diseases in dogs, but the tissue expression of these proteins appears to differ from their concentrations reported in urine samples. Further investigations of the S100/calgranulin pathways in UC and their potential as diagnostic or prognostic tools and potential therapeutic targets are warranted. The NLR as a routinely available marker might be a useful surrogate to distinguish UC from inflammatory conditions.
Similar content being viewed by others

Background
Urothelial carcinoma (UC), previously referred to as urinary tract transitional cell carcinoma (TCC), is an epithelial neoplasm originating from the urothelium. It is the most common neoplasia affecting the lower urinary tract (i.e., bladder and urethra) in dogs and comprises approximately 2% of all malignancies in this species [1,2,3]. Affected dogs are typically elderly females of small- to medium-size breeds. Other known risk factors for UC development include obesity, certain breed predispositions (e.g., Scottish terrier), and chronic exposure to herbicides and pesticides [4,5,6]. In contrast, vegetable consumption appears to have a protective effect [7].
Clinical signs are usually nonspecific and include hematuria, stranguria, and pollakiuria [1, 3, 8,9,10]. These may result from the effects of the tumor or a complicating bacterial urinary tract infection (UTI), a frequent concurrent diagnosis in UC patients [11]. Clinical signs in UC patients often do not occur until the late stages of the disease and can be confused with a UTI, rendering UC diagnosis challenging in clinical practice. With metastatic disease, lameness or neurological deficiencies may be seen if bone metastasis occurs to the lumbar vertebrae, pelvis, or limbs [12,13,14]. In patients suspected of UC, diagnostic imaging (abdominal ultrasonography and/or computed tomography) aids in patient evaluation [15] as UC typically reveals a papillary growth pattern [1, 3]. A single location (typically the trigonal area of the urinary bladder) can be affected in some cases, but often UC is multifocal due to the “field effect” of urine [16]. A minimal database is recommended in all dogs, but urine should not be obtained by cystocentesis due to the risk of needle tract implantation (“seeding effect”) [17]. Several treatment options have been reported with varying outcomes [18,19,20,21,22,23,24,25]. The best overall survival times are achieved by combining surgical and medical treatment options comprised of cyclooxygenase (COX)-2 inhibitors and chemotherapy [8, 19, 26,27,28]. Many chemotherapeutics have been studied [22, 29, 30], but UC treatment remains challenging as there is no gold standard treatment protocol, and further research is needed to identify more effective therapeutic targets [1, 3, 9, 21, 31].
Different diagnostic modalities for UC diagnosis vary in specificity and sensitivity. In only 30% of affected dogs, tumor cells can be detected on urine sediment analysis. Also, it can be very challenging to distinguish neoplastic from highly reactive urothelial cells [12, 13]. The urine veterinary bladder tumor antigen (V-BTA) test is highly sensitive, easily performed, and non-invasive, but has a low specificity to distinguish UC from UTI, particularly in dogs with glucosuria, hematuria, pyuria, or proteinuria [32]. Although a recently developed diagnostic test for the BRAF mutation has a higher diagnostic accuracy [33,34,35,36], histopathologic examination of tissue biopsy samples remains the gold standard diagnostic. Sampling such biopsies usually requires cystoscopic examination [37]. Thus, screening tests for dogs at risk would be highly favorable to spare dogs that are not-affected from general anesthesia. While novel diagnostic tools would be favorable, prognostic markers and effective treatment options are also lacking. Few studies have evaluated pathway-specific therapeutic targets (beyond COX-inhibition), including the tyrosine kinase inhibitors lapatinib [38] and toceranib [39]. Further evaluating cell signaling pathways in UC appears to be a promising approach to exploring new ways to modulate molecular signals therapeutically.
S100A8/A9 (calprotectin or calgranulin A/B complex) and S100A12 (calgranulin C) belong to the family of Ca2+-binding S100 proteins of the innate immune system [40]. These alarmins play an important role in several neoplastic and inflammatory diseases in humans and dogs and are valuable diagnostic and potentially prognostic biomarkers in human medicine [40,41,42,43,44,45,46,47,48]. However, their role in UC pathogenesis and their diagnostic use in veterinary medicine is currently limited. A recent study suggested measuring the S100/calgranulins in urine samples to be a promising biomarker for distinguishing inflammatory from neoplastic urinary tract conditions [49, 50]. Higher concentrations of the S100/calgranulins were detected in dogs with inflammatory or neoplastic urinary tract diseases than in healthy dogs, and the S100A8/A9-to-S100A12 ratio was significantly lower in dogs with inflammatory conditions compared to those with neoplastic disease or health [49]. However, the source of S100/calgranulin expression in these conditions remains unknown, and to the authors’ knowledge, S100A8/A9 and S100A12 have not been evaluated in urinary bladder and urethral tissue samples from dogs. Thus, this study aimed to compare the expression of the S100/calgranulins in biopsy samples of neoplastic and inflammatory lesions in urinary bladder and urethral tissue using immunohistochemistry (IHC). We hypothesized that the individual expression and ratio of the S100/calgranulins in lower urinary tract tissue samples mirror the urinary concentrations previously reported for dogs with these conditions. A secondary aim was to evaluate whether S100/calgranulin expression in neoplastic tissue is limited to innate immune cells (granulocytes) or if neoplastic cells also express these proteins.
S100/calgranulin proteins are predominantly produced and released by granulocytes (but also monocytes and macrophages) in the intestinal mucosa. This local innate immune response might extend systemically and be reflected by systemic leukocyte differences, which have not been evaluated in canine UC. The neutrophil-to-lymphocyte ratio (NLR) is an inexpensive marker derived from the minimum database. Given the interest in new inexpensive and simple predictive tools, the blood NLR has been shown to have diagnostic and/or prognostic potential in human patients with inflammatory and neoplastic diseases, including UC [51,52,53,54]. Consequently, great interest in the NLR as a biomarker arose in veterinary medicine, where the NLR shows promise as an indicator of outcome in several inflammatory [55,56,57,58] and neoplastic [59, 60] conditions. These include chronic inflammatory enteropathy [56], pneumonia [57], acute diarrhea in puppies [58], soft tissue sarcoma [59], and multi-centric lymphoma [60]. Because the NLR has not been studied in canine UC, the third aim of the study was to evaluate the NLR in dogs with UC and their potential to differentiate affected dogs from those with NNUTD.
Results
Study population
Dogs with UC – Breeds included Airedale terrier, Bernese Mountain dog, Bordeaux mastiff, Border collie, Cocker spaniel, Eurasian dog, Jack Russell terrier, Soft Coated Wheaton terrier, West Highland White terrier (each n = 1), Labrador retriever (n = 3), and mixed breed dogs (n = 11) (Suppl. Table 1). The UC group comprised predominantly female patients (82%), of which 6 dogs (33%) were spayed. UC was confirmed by histopathological examination in all urinary tract tissue biopsies. A urine culture was performed in 12 of the 22 dogs, 3 (25%) of which were positive for bacterial growth (Escherichia coli: n = 2; Staphylococcus intermedius: n = 1). Treatment at the time of tissue biopsy included non-steroidal anti-inflammatory drugs (NSAID; carprofen: n = 1; firocoxib: n = 1; meloxicam: n = 11; robenacoxib: n = 1).
Sufficient tissue biopsy material for IHC analyses was available from 9 dogs diagnosed with UC (Table 1). The most common tumor location was the urinary bladder (n = 6), followed by the urethra (n = 4). All tissue biopsies from patients that survived to discharge from the hospital (n = 8) were obtained via urethrocystoscopy guidance. One tissue biopsy was taken during necropsy, and pulmonary metastasis was confirmed post-mortem in this patient. Three dogs were suspected or confirmed to have metastases or another neoplastic process in the spleen (n = 2), liver (n = 1), uterus (n = 1), mammary gland (n = 1), and/or lung (n = 1) based on diagnostic imaging. None of these sites were sampled.
Follow-up information was available from 18 dogs. At the end of the study, 3 dogs were still alive with stable disease for up to 575 days under mitoxantrone chemotherapy (n = 1; 192 days) or NSAID treatment (n = 2; 179 and 575 days). All remaining dogs (n = 15) were euthanized either immediately after diagnosis (n = 3) or within 2–330 days (median: 16 days) of diagnosis, while one dog was diagnosed with UC on necropsy. All but 3 dogs received NSAID treatment, one dog received a combination of meloxicam and metronomic chlorambucil chemotherapy and lived another 180 days, and one dog that received chemotherapy with mitoxantrone was euthanized 25 days after diagnosis. The dog with a 330 day-survival was treated with NSAID and alfuzosin.
Dogs with non-neoplastic urinary tract inflammation – Breeds included Yorkshire terrier (n = 4), Labrador retriever, Schnauzer (each n = 2), Beagle, Bernese Mountain dog, Berger de Brie, Chihuahua, Dachshund, Dalmatian, Doberman, English bulldog, German Shepherd dog, Newfoundland, Pug, Rottweiler, Shih tzu (each n = 1), and mixed breed dogs (n = 5) (Suppl. Table 1). Diseases included urolithiasis (n = 22) and/or histologically confirmed cystitis/urethritis (n = 7). Urine culture was performed in 18/26 dogs and was positive for bacterial growth in 8/18 (44%) dogs, and a negative culture was seen in the remaining 10 dogs. Bacterial isolates were S. intermedius (n = 5), Proteus mirabilis (n = 1), E. coli (n = 1), Streptococcus canis (n = 1), and Enterobacter cloacae (n = 1); one dog had a polymicrobial urinary tract infection. Most dogs in this group were male (n = 20; 77%), five of which (25%) were neutered. The remaining dogs (n = 6; 23%) were females.
Follow-up information was available from 17 dogs. Ten dogs were still alive at the conclusion of the study, one dog with recurrent urolithiasis-associated micturition disorder resolved by catheterization. Nine dogs were lost to follow-up. The remaining 7 dogs were euthanized (n = 6; within 2–1,247 days after diagnosis, median: 106 days) or had died (n = 1; after 4 days); one dog surviving 90 days was euthanized for reasons unrelated to the urinary tract disease.
Sufficient tissue material for IHC staining and analysis was available from 5 dogs (Table 1). Diagnoses in these dogs were marked suppurative cystitis (n = 4) and/or urethritis (n = 1), and cystitis was associated with struvite or urate urolithiasis in 1 dog each. All 5 dogs received antimicrobials and analgesics after tissue biopsy sampling. Surgical biopsies were obtained from 4 dogs (57%) during diagnostic laparotomy with cystotomy, and tissue biopsy samples were endoscopically obtained in the remaining 3 cases (43%).
Control dogs – Breeds included American Staffordshire terrier, Collie, Dachshund, Labrador retriever, Maltese (each n = 1), and mixed breed (n = 2). Most of these dogs (86%) had died or were euthanized for reasons unrelated to the urinary tract, and 1 dog (14%) was diagnosed with a detrusor sphincter dyssynergia and normal urinary bladder histology (but was not included in IHC analysis). All dogs (n = 7) were male, with 29% neutered (n = 2). Age-related conditions not reported to affect the urinary tract (e.g., degenerative joint disease) were not considered exclusion criteria.
Dogs with UC were significantly older (median: 11.2 years, range: 6.8–14.3 years) than dogs with non-neoplastic urinary tract inflammation (median: 6.6 years, range: 0.3–14.5 years; P = 0.0001) (Table 1). Body weight was not significantly different among the 3 groups of dogs (P = 0.5074).
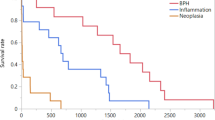
In the survival analysis (Fig. 1), 15 dogs in the UC group and 7 dogs in the NNUTD group reached the endpoint (death). Survival times were lower in the UC group (median: 6 days, 95% confidence interval [CI]: 0–28 days) than in the dogs with NNUTD (median: 60 days, 95%CI: 1–1,146 days), but statistical significance was not reached in the log-rank test (P = 0.1067).

Kaplan–Meier survival plot for dogs with malignant versus benign lower urinary tract diseases. Median survival time in the urothelial carcinoma (UC) group was lower (6 days) than in dogs with non-neoplastic (inflammatory) urinary tract diseases (NNUTD; median: 60 days), but the difference was not statistically significant (P = 0.1067)
Tissue S100/calgranulin expression
For IHC analysis, a total of 10 tissue samples from 9 dogs diagnosed with UC were of adequate quality, 6 tissue samples from 5 dogs with NNUTD, and 11 samples from 6 control dogs (Table 2).
Cells staining positive for S100A8/A9 and S100A12 were predominantly infiltrating immune cells, resembling mostly neutrophils and macrophages based on their morphology, whereas negligible S100/calgranulin-staining was detected in UC cells. Numbers of S100A8/A9+ cells per mm2 were numerically smaller in dogs with UC (median: 22) compared to non-neoplastic urinary tract diseases (median: 312) but similar to the control group (median: 21) (Fig. 2). However, the difference between dogs with UC and dogs with non-neoplastic urinary tract diseases did not reach statistical significance (P = 0.3741). In contrast, the numbers of S100A12+ cells were significantly higher in dogs with UC (median: 15) and the NNUTD group (median: 75) compared to the control group (median: 0; P = 0.0267 and P = 0.0049) (Table 2, Fig. 2). However, there was no significant difference in S100A12+ cell counts between the UC and the NNUTD group of dogs (P = 0.1372). The Cal-ratio was significantly lower in UC dogs (median: 2.0) and dogs with NNUTD (median: 1.3) compared to control dogs (median: 12.6; P = 0.0062 and P = 0.0030, respectively), with no significant difference between the two disease groups (P = 0.2884) (Table 2, Fig. 2).

S100/calgranulin-positive cell counts in tissue biopsies of dogs with lower urinary tract diseases. A S100A8/A9+ cell counts per mm2 were numerically (but not statistically) higher in dogs with non-neoplastic (inflammatory) urinary tract diseases (NNUTD; median: 312, range: 0–890) than in dogs with urothelial carcinoma (UC; median: 22, range: 0–98; P = 0.2382) and healthy controls (control; median: 21, range: 2–39; P = 0.2478). B S100A12+ cell counts per mm2 were significantly higher in dogs with UC (median: 15, range: 0–69) and dogs with NNUTD (median: 75, range: 0–540) than in healthy controls (median: 0, range: 0–7; P = 0.0267 and P = 0.0049, respectively), but no significant difference between UC and NNUTD (P = 0.1372). C The S100A8/A9+-to-S100A12.+ ratio (Cal-ratio) was significantly lower in dogs with UC (median: 2.0, range: 1.3–4.3) and dogs with NNUTD (median: 1.3, range: 0.8–6.7) than in healthy controls (median: 12.6, range: 1.8–13.2; P = 0.0062 and P = 0.0030, respectively), but did not significantly differ between UC and NNUTD (P = 0.2884)
Numbers of S100A8/A9+ and S100A12+ cells were highly correlated in tissues of UC dogs (ρ = 0.96, P < 0.0001) and in dogs with non-neoplastic disease (ρ = 0.94, P = 0.0048).
Association of S100/calgranulin expression with disease characteristics
Prior NSAID treatment or the presence of metastasis at the time of diagnosis were not found to affect the number of S100A8/A9+ or S100A12+ cells or the Cal-ratio (all P > 0.05). Survival time and the site evaluated (urinary bladder vs. urethra) or primarily affected were also not associated with the expression of S100/calgranulins or their ratio (all P > 0.05), albeit a trend was detected for the Cal-ratio to inversely correlate with survival time in dogs with non-neoplastic disease (ρ = -0.95, P = 0.0513).
Evaluating both disease groups of dogs (UC and non-neoplastic disease) combined, bacterial culture-positive dogs (n = 5) had higher numbers of S100A8/A9+ cells (median: 331/mm2) and S100A12+ cells (median: 50/mm2), but lower Cal-ratios (median: 1.6) than those dogs with no bacterial growth on culture (n = 5; medians: 11/mm2, 0/mm2, and 2.9), but the differences did not reach statistical significance (all P > 0.05).
Blood neutrophil-to-lymphocyte ratio (NLR)
Dogs with non-neoplastic urinary tract disease had significantly higher neutrophil counts than those with UC (P < 0.0001), but no difference in lymphocyte counts between both groups (P = 0.7564), yielding higher NLRs in dogs with NNUTD than with UC (P = 0.0017) (Table 3). NLR was available for only one dog in the control group, excluding this group from NLR analysis.
The area under the ROC curve for NLR to separate dogs with UC from those with other non-neoplastic (inflammatory and/or infectious) urinary tract diseases was 0.73. Using a cut-off NLR of ≤ 2.83 yielded 41% sensitivity (95%CI: 23–61%) and a specificity of 100% (95%CI: 87–100%) to detect UC patients.
Higher NLRs showed a trend to be associated with lower numbers of tissue S100A12+ cells in dogs with NNUTD (ρ = -0.80; P = 0.0590).
Association of NLR with disease characteristics
The NLR showed a moderate inverse correlation with the survival time in UC patients (ρ = -0.55; P = 0.0417), but did not distinguish between patients with UC and evidence or suspicion of metastasis at the time of diagnosis (median: 3.6) and dogs without such lesions (median: 3.3; P = 0.8734).
Dogs with bacterial growth on urine culture had significantly higher NLRs (median: 10.0; n = 10) than culture-negative dogs (median: 4.6; n = 19; P = 0.0389).
Discussion
This study evaluated the local tissue expression of S100A8/A9 and S100A12 in neoplastic and inflammatory lower urinary tract disease in dogs compared to healthy controls. The results suggest that cells expressing these S100/calgranulin proteins – either resident or infiltrating cells – are involved in the local immune response associated with inflammatory and neoplastic disease processes in the lower urinary tract (referred to as inflammatory tumor microenvironment). This agrees with S100A12- and RAGE (receptor for advanced glycation end products)-mRNA being overexpressed in human UC [61]. Further studies should also evaluate whether the S100/calgranulin pathways (including their innate immune receptors) might determine the prognosis and/or even present potential novel therapeutic targets.
The present study followed a previous investigation by our group [49] and further evaluated the source and cellular distribution of S100/calgranulin secretion into the urine. In our previous study, urinary concentrations of S100A8/A9 and S100A12 were both significantly increased in dogs with TCC, prostatic adenocarcinoma (PCA), or UTI compared to healthy control dogs. Furthermore, the urinary Cal-ratio was significantly lower in dogs with UTI than in the other two groups of dogs, suggesting its potential as a screening test [49]. Surprisingly, the present study found no difference in S100A8/A9 positivity between dogs with UC and healthy controls, but the number of S100A8/A9+ cells was markedly (albeit not significantly) increased in tissues with inflammatory lesions when compared to neoplastic tissues. A possible explanation for these discrepant findings is that the sheer number of cells staining positive for S100A8/A9 and/or S100A12 does not inevitably reflect the amount of S100/calgranulin expression and release. Addressing this issue would require the quantification of S100/calgranulin staining using an automated scanning tool with a positive pixel-based algorithm [62]. Also, urinary S100/calgranulin concentrations were not measured for comparison in this present study due to the retrospective inclusion of most dogs. In people, urinary calprotectin (S100A8/A9) is increased in high-grade UC (the human counterpart of the invariably present muscle-invasive form of canine UC) compared to low-grade UC or absence of UC, provided the exclusion of renal failure and pyuria [63] because calprotectin loses specificity as a tumor marker even with sterile leukocyturia (pyuria) [65]. These findings are consistent with our numerically higher tissue S100/calgranulin-positive cell counts in dogs with (concurrent) UTI compared to dogs with no evidence of a UTI based on a quantitative urine culture.
In contrast to a previous study by our group, in which all dogs with TCC/PCA were treatment-naïve at the time of urine sampling, some dogs in the present study had received a COX-2 selective NSAIDs prior to tissue diagnosis. Thus, an effect of this treatment cannot be excluded, although prior NSAID administration was not significantly associated with different S100/calgranulin-positive cell counts. Myeloid-derived suppressor cells are attracted by inflammatory cytokines (e.g., IL-1β, IL-6, PGE2, and tumor growth factors), increasing their production of S100/calgranulins [65, 66]. This response is further enhanced by positive autocrine feedback mechanisms involving S100/calgranulin binding to the innate immune receptors Toll-like receptor (TLR) 4 and RAGE, resulting in increased leukocyte chemotaxis via nuclear factor (NF)-κB and MAPK signaling pathways [61, 65,66,67]. NF-κB increases COX-2 expression, catalyzing prostaglandin E2 (PGE2) synthesis [68, 69], with which COX-inhibitors aim to interfere. As a result of stopping this overt and/or perpetual process, S100/calgranulin (particularly S100A8/A9) production and release might decrease. COX-2 overexpression has been confirmed in UC cells [71, 73], and COX-2 inhibitors play an important neoadjuvant role in the treatment of UC in dogs [1, 3, 9] due to their analgesic, anti-inflammatory, and anti-tumor effects [26]. Thus, the effects of COX-inhibition on S100/calgranulin expression in canine lower urinary tract inflammatory and neoplastic diseases need to be clarified in further research.
Another possible explanation for the discrepancy between tissue S100/calgranulin expression in this study and urinary S100/calgranulin levels in the previous investigation [49] might be differences in the disease state (i.e., presence of distant and/or local metastasis) affecting S100/calgranulin expression levels. The strong trend for an inverse correlation of tissue Cal-ratios with survival time might suggest increased S100A8/A9 expression in dogs with more advanced disease. However, our study included only one dog with confirmed pulmonary metastasis, which, interestingly, was not associated with S100A8/A9+ or S100A12+ cells (data not shown). Another 3 dogs were suspected of having metastatic disease. If confirmed, the metastatic rate in our study would agree with the literature, stating that about 40% of UC patients have metastatic disease at the time of diagnosis [1, 9, 12]. Interestingly, one dog was suspected of having distant UC metastasis to the uterus, mammary gland, and lungs. UC might cause pulmonary and uterine metastases, but mammary glands are not a typical site for UC to metastasize to [12] and most dogs in the UC group were intact elderly females with a risk of developing (concurrent) primary mammary neoplasia [73, 74]. Also, to what extent other factors such as the dog’s reproductive status (most dogs were intact, whereas mostly spayed/neutered dogs were included in the previous study) might affect S100/calgranulin expression is unknown, particularly with UC being far more likely in female dogs similar to the muscle-invasive type of the disease in people. The sex distribution also differed among the groups of dogs in our study, with a female predominance in the UC group, and an effect on the results of the study cannot be excluded. To the authors’ knowledge, the possibility of sex and reproductive status affecting urinary tract S100/calgranulin expression or urine concentrations of the S100/calgranulins has not been reported. A recent study evaluating the association of clinical characteristics and lifestyle factors with S100/calgranulin concentrations in feces from healthy dogs showed a link with the reproductive status in only female dogs but no correlation with sex or reproductive status in male dogs [75]. Thus, further evaluation of a possible association between S100/calgranulin expression and canine UC biology is warranted.
Another finding was the diagnosis of UC mostly in large breed dogs (median body weight of 24 kg), which differs from other reports where UC patients had a median body weight of about 15 kg [9] and overrepresented breeds included Scottish (and other small) Terriers, Shelties, and Beagles [1, 9]. Different breed lines could explain this difference, but geographical differences linked to increased risk factors (e.g., exposure to herbicides/pesticides [4,5,6]) or local breed popularities might be an alternative explanation. Obesity is another risk factor for UC development [4], but reliable body condition scores were unavailable.
An unexpected finding in our study was the lack of a significant difference in survival times between dogs with UC and complete follow-up (n = 15; median: 6 days) than dogs with inflammatory disease (median: 60 days; n = 7), but only 3 dogs with UC compared to 10 dogs with NNUTD were still alive at the end of the study. Two dogs with inflammatory lower urinary tract disease were severely affected with complications and did not survive to discharge from the hospital; the third dog was euthanized due to suspicion of hemangiosarcoma. Still, survival times in dogs with UC were shorter than reported in the recent literature, likely reflecting a more conservative treatment approach elected by most owners. Most UC dogs euthanized shortly after being presented to the hospital (n = 5) were unable to void urine, and more invasive procedures (e.g., urethral stents, UC laser ablation) [31, 76] were declined.
This study also evaluated the diagnostic potential of the NLR in canine lower urinary tract diseases and found NLRs to be significantly higher in dogs with NNUTD, which is consistent with higher neutrophil counts and NLRs in clinically more severely affected dogs with chronic gastrointestinal inflammation [56]. Our results could be due to higher cortisol levels (e.g., systemic disease, stress) or infection causing neutrophilia (reduced endothelial adherence causing prolonged circulation times) and lymphocyte migration into affected tissues. However, the NLR increase was solely based on higher neutrophil counts, with lymphocyte counts more consistent between both disease groups. Some dogs with non-neoplastic inflammatory urinary tract disease were clinically severely affected with evidence of complications (e.g., bladder rupture causing uroabdomen and systemic inflammatory response syndrome) compared to dogs with UC. In line with this, NLR was identified as a prognostic factor in various chronic and acute inflammatory conditions in people [77, 78]. Neutrophils are involved in the response to bacterial infections, and urine cultures were positive for bacterial growth in 44% of dogs with NNUTD compared to only 25% in the UC group. However, a possible effect of prior antimicrobial treatment in some dogs cannot be completely excluded. Moderate to high sensitivity and specificity of the NLR to distinguish UC from non-neoplastic urinary tract conditions warrants further evaluation of the diagnostic value of the NLR.
We acknowledge that the retrospective inclusion of most dogs presents a limitation of this study, particularly concerning the availability of complete medical records data. However, most owners and/or primary care veterinarians were contacted for further patient and follow-up information. The study included a moderate-sized population of dogs, and an effect of treatment(s) prior to sample collection on the results in some dogs cannot be excluded. Tissue biopsies were sampled using either urethrocystoscopy or laparotomy, but relevant effects of the sampling method on the results of IHC are not to be expected given that the mucosa or mucosal side of the tissue biopsies were evaluated and significant autolysis was not present in any of the tissue samples evaluated. Lastly, different pathologists were involved in the routine histologic evaluation of the tissues, potentially introducing inter-observer variation. However, a single pathologist not involved in the initial assessments (CG) examined all tissue specimens after IHC staining, arriving at the same interpretations and diagnoses.
Conclusions
This study confirms that the S100/calgranulins play a role in the immune response to inflammatory and neoplastic lower urinary tract diseases in dogs. However, the S100/calgranulin expression in lower urinary tract tissues detected in this study differs from our previous measurements of the same proteins in canine urine specimens. While the impact of pre-treatment (e.g., NSAIDs) and other patient factors (e.g., metastatic disease, sex, and reproductive status) on tissue S100/calprotectin expression and urinary secretion in affected dogs remains unknown, the latter might also not necessarily depend solely on the number of S100/calgranulin-expressing cells. Significant differences in S100A12+ cell counts and the Cal-ratio among dogs with UC or non-neoplastic inflammatory conditions and healthy controls warrant further exploration of the S100/calgranulin pathways in these diseases. NLRs were significantly higher with non-neoplastic urinary tract disease, and this routinely available marker might be a useful surrogate to distinguish UC from inflammatory conditions.
Methods
Ethics approval
All methods were carried out in accordance with relevant guidelines and regulations. The protocol for collection of tissue samples from dogs with urinary tract disease and healthy control dogs was independently reviewed and approved by the Regional Veterinary Council of the Free State of Saxony, Leipzig/Chemnitz, SN, Germany (TVA# 23/18), and written informed consent was obtained from all owners of dogs that were enrolled into the study.
Sampling population
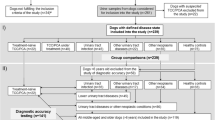
Patients (n = 55) for this case–control study were recruited at the Department for Small Animals, Leipzig University, College of Veterinary Medicine: dogs with UC (n = 22), NNUTD (n = 26), and healthy control dogs (n = 7). Inclusion criteria were the histologic documentation leading to a diagnosis of either urothelial carcinoma (UC group) or a primary or secondary inflammatory condition (e.g., cystitis, urolithiasis) where an underlying lower urinary tract neoplasm was not suspected and histologically excluded (NNUTD group). In addition, enough tissue biopsy material had to be available to perform IHC analysis and/or a complete blood cell count performed for NLR analysis. Prior treatment was not an exclusion criterion except for the administration of traditional chemotherapy or glucocorticoids (for NLR analysis).
A total of 14 dogs were prospectively enrolled, and archived tissue biopsy specimens and/or patient data were retrospectively included from 41 animals (Table 1). Of the 15 lower urinary tract disease patients included in the IHC study, 3 dogs were treatment-naïve whereas 12 dogs (86%) had received prior non-steroidal anti-inflammatory drugs (NSAID, n = 10; 71%), glucocorticoids (n = 1; 7%), and/or antimicrobials (n = 11; 73%) at the time of biopsy collection. Complete patient information was extracted from the electronic medical records (for retrospectively enrolled cases) and/or a study questionnaire completed by the owner and/or the attending veterinarian at patient enrolment (for prospectively enrolled cases). Dogs were followed up by contacting the referring veterinarian, owners, or both, using a standardized questionnaire. To be considered for inclusion in the control group of dogs, histopathology of urinary tract tissues had to be unremarkable.
Tissue sample analyses
Tissue biopsies of the urinary bladder (n = 17) and/or urethra (n = 11) from dogs with UC (n = 9), other non-neoplastic urinary tract diseases (NNUTD; n = 5), and healthy controls (n = 6) were used for the study (Table 1).
After sampling during routine diagnostic procedures under general anesthesia (protocols optimized for the individual patient) or necropsy, the specimens were fixed in formaldehyde solution (4%), paraffin-embedded, cut into 3-µm slices, and placed on microscopy slides. Routine histopathology of urinary tract tissues was performed on hematoxylin/eosin-stained slides by one of 6 board-certified and/or nationally certified veterinary anatomic pathologists. After obtaining a histologic diagnosis, 3-µm tissue re-cuts were prepared for IHC. The specimens (3 slides of tissue samples from each dog and tissue) were deparaffinized in xylene and rehydrated in an ethanol series. After washing the slides in phosphate-buffered saline (PBS) including Tween 20 (0.025% v/v) (PBST), heat-induced antigen retrieval was performed in 0.01 M citrate buffer (pH 6.0) at 95 °C for 45 min, followed by cooling at room temperature (approximately 20 °C) for 20 min. Slides were washed twice in PBST, and the specimens were incubated for 25 min with 4% bovine serum albumin (BSA) in PBS to prevent non-specific binding. Samples were then incubated overnight at 4 °C with the primary antibody by covering one specimen each with rabbit polyclonal anti-canine S100A8/A9 (final concentration: 0.2 µg/mL) [79] or anti-canine S100A12 (final concentration: 0.25 µg/mL) [80]. A third slide was used as a negative control using normal rabbit serum (final protein concentration: 0.2 µg/mL). Slides were washed twice in PBST and then incubated with the goat anti-rabbit alkaline phosphatase-labeled secondary antibodyFootnote 1 (concentration: 1.0 µg/mL) for 60 min at room temperature. After two PBST washes, the slides were incubated with Fast RedFootnote 2 for approximately 30 min. When optimal color had developed, the slides were first washed in PBST, followed by ddH2O. Mayer’s hematoxylin was used to counterstain the nuclei, with the reaction stopped after 90 s with running tap water. The slides were mounted with Fluoromount-G.Footnote 3 After a cursory assessment by light microscopy, the slides were digitized using the Pannoramic Scan IIFootnote 4 with a 20 × objective lens. The digital images were then examined by a board-certified veterinary pathologist (CG) in a blinded fashion and using the CaseViewer digital microscopy application.Footnote 5
After grossly re-evaluating the histopathologic diagnosis, distribution of positive staining, and the absence of staining in the corresponding negative control (Fig. 3), 5–7 regions of 1 mm2 were randomly selected based on optimal tissue integrity for evaluation using CaseViewer. In these regions, all S100A8/A9-positive (S100A8/A9+) and S100A12-positive (S100A12+) cells were identified and counted if yielding a cytoplasmic or membranous signal. For data analysis, the average numbers of S100A8/A9+ cells and S100A12+ cells were calculated for all regions evaluated from the same dog, and the S100A8/A9-to-S100A12 ratio (Cal-ratio) was determined as [average number of S100A8/A9+ cells] / [average number of S100A12+ cells].

S100/calgranulin immunohistochemistry (IHC) of urinary bladder tissue biopsies in dogs with lower urinary tract disease. Upper panel: moderate numbers of infiltrating cells staining positive (Fast-red) for S100A8/A9 (A) or S100A12 (B) in a 10½-year old female mixed breed dog diagnosed with urothelial carcinoma. Lower panel: large numbers and nest-like accumulations of infiltrating cells staining positive for S100A8/A9 (C, insert at the bottom right: negative staining control) or S100A12 (D) in a 4-months old male Newfoundland dog with marked transmural suppurative cystitis. Gray scale bars at the top right corners: 100 µm
Blood leukocyte analysis
Complete blood cell count analyses were performed using an automated blood cell analyzer. Neutrophil counts and lymphocyte counts were measured in × 109 cells/L (reference intervals: 3.0–11.6 × 109/L and 1.0–5.1 × 109/L), and the neutrophil-to-lymphocyte ratio (NLR) was calculated as [(neutrophil count)/(lymphocyte count)] [56].
Data analyses
A commercially available statistical software packageFootnote 6 was used for all statistical analyses. Data were tested for the assumption of normality using a Shapiro–Wilk test. Summary statistics are reported as medians and ranges (continuous data) or counts and percentages (categorical data). All parameters were tested among the 3 different groups of dogs using non-parametric multiple- (Kruskal–Wallis test: S100A8/A9+ cell counts, S100A12+ cell counts, and Cal-ratio) or two-group (Mann–Whitney U test: neutrophil and lymphocyte counts, NLR) comparisons. In addition, patient characteristics (age, sex, and body weight) were compared among the groups of dogs. Possible associations between numerical patient characteristics (survival time, S100/calgranulin-positive cell counts, NLR) were determined by calculating a Spearman correlation coefficient ρ. The Kaplan–Meier survival statistics was used to estimate the median (and 95% CI) time to death, and the log-rank test served to compare the survival times between dogs with UC and NNUTD. Statistical significance was set at P < 0.05, with P < 0.1 interpreted as a possible trend.
A receiver operating characteristic (ROC) curve was constructed to determine the sensitivity and specificity of the NLR to distinguish dogs with UC from dogs with other (inflammatory or infectious) urinary tract diseases, where the Youden index served to determine the best cut-off value.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Notes
Goat anti-rabbit alkaline phosphatase-labeled immunoglobulin, Dianova, Hamburg, Germany.
SigmaFast™ Fast Red TR/Naphthol AS, Merck, Darmstadt, Germany.
Fluoromount-G™ Mounting Medium, Thermo Fisher, Dreieich, Germany.
Pannoramic Scan II, 3D-Histech Ltd., Budapest, Hungary.
CaseViewer digital microscopy application, Slides.3D-Histech Ltd., Budapest, Hungary.
JMP v13.0, SAS Institute Inc., Cary, NC, USA.
Abbreviations
- AUROC:
-
Area under the ROC curve
- BSA:
-
Bovine serum albumin
- Cal-ratio:
-
S100A8/A9-to-S100A12 ratio
- COX-2:
-
Cyclooxygenase-2
- NLR:
-
Neutrophil-to-lymphocyte ratio
- NNUTD:
-
Non-neoplastic urinary tract disease
- PBS:
-
Phosphate-buffered saline
- PBST:
-
PBS with Tween
- PCA:
-
Prostatic adenocarcinoma
- ROC:
-
Receiver operating characteristic curve
- S100A8/A9:
-
S100A8/A9 (calprotectin) protein complex
- S100A12:
-
S100A12 protein
- TCC:
-
Transitional cell carcinoma
- UTI:
-
Urinary tract infection
- UC:
-
Urothelial carcinoma
- IHC:
-
Immunohistochemistry
- NSAID:
-
Non-steroidal anti-inflammatory drug
References
Mutsaers AJ, Widmer WR, Knapp DW. Canine transitional cell carcinoma. J Vet Intern Med. 2003;17(2):136–44.
Knapp DW, Ramos-Vara JA, Moore GE, Dhawan D, Bonney PL, Young KE. Urinary bladder cancer in dogs, a naturally occurring model for cancer biology and drug development. ILAR J. 2014;55(1):100–18.
Fulkerson CM, Knapp DW. Management of transitional cell carcinoma of the urinary bladder in dogs: a review. Vet J. 2015;205(2):217–25.
Glickman LT, Schofer FS, McKee LJ, Reif JS, Goldschmidt MH. Epidemiologic study of insecticide exposures, obesity, and risk of bladder cancer in household dogs. J Toxicol Environ Health. 1989;28(4):407–14.
Raghavan M, Knapp DW, Dawson MH, Bonney PL, Glickman LT. Topical flea and tick pesticides and the risk of transitional cell carcinoma of the urinary bladder in Scottish Terriers. J Am Vet Med Assoc. 2004;225(3):389–94.
Glickman LT, Raghavan M, Knapp DW, Bonney PL, Dawson MH. Herbicide exposure and the risk of transitional cell carcinoma of the urinary bladder in Scottish Terriers. J Am Vet Med Assoc. 2004;224(8):1290–7.
Raghavan M, Knapp DW, Bonney PL, Dawson MH, Glickman LT. Evaluation of the effect of dietary vegetable consumption on reducing risk of transitional cell carcinoma of the urinary bladder in Scottish Terriers. J Am Vet Med Assoc. 2005;227(1):94–100.
Chun R, Knapp DW, Widmer WR, DeNicola DB, Glickman NW, Kuczek T, et al. Phase II clinical trial of carboplatin in canine transitional cell carcinoma of the urinary bladder. J Vet Intern Med. 1997;11(5):279–83.
Knapp DW, Glickman NW, DeNicola DB, Bonney PL, Lin TL, Glickman LT. Naturally-occurring canine transitional cell carcinoma of the urinary bladder A relevant model of human invasive bladder cancer. Urol Oncol. 2000;5(2):47–59.
Vail DM, Page RL, Withrow SJ. Withrow & MacEwen’s small animal clinical oncology. 5th ed. St. Louis, Mo: Elsevier/Saunders; 2013. Available from: http://search.ebscohost.com/login.aspx?direct=true&scope=site&db=nlebk&db=nlabk&AN=604176.
Budreckis DM, Byrne BA, Pollard RE, Rebhun RB, Rodriguez CO, Skorupski KA. Bacterial urinary tract infections associated with transitional cell carcinoma in dogs. J Vet Intern Med. 2015;29(3):828–33.
Norris AM, Laing EJ, Valli VE, Withrow SJ, Macy DW, Ogilvie GK, et al. Canine bladder and urethral tumors: a retrospective study of 115 cases (1980–1985). J Vet Intern Med. 1992;6(3):145–53.
Valli VE, Norris A, Jacobs RM, Laing E, Withrow S, Macy D, et al. Pathology of canine bladder and urethral cancer and correlation with tumour progression and survival. J Comp Pathol. 1995;113(2):113–30.
Malek S, Murphy KA, Nykamp SG, Allavena R. Metastatic transitional cell carcinoma in proximal humerus of a dog. Can Vet J. 2011;52(9):1013–7.
Macrì F, Di Pietro S, Mangano C, Pugliese M, Mazzullo G, Iannelli NM, et al. Quantitative evaluation of canine urinary bladder transitional cell carcinoma using contrast-enhanced ultrasonography. BMC Vet Res. 2018;14(1):84.
Slaughter DP, Southwick HW, Smejkal W. “Field cancerization” in oral stratified squamous epithelium. Clin Implications Multicentric Orig Cancer. 1953;6(5):963–8.
Nyland TG, Wallack ST, Wisner ER. Needle-tract implantation following us-guided fine-needle aspiration biopsy of transitional cell carcinoma of the bladder, urethra, and prostate. Vet Radiol Ultrasound. 2002;43(1):50–3.
Henry CJ, McCaw DL, Turnquist SE, Tyler JW, Bravo L, Sheafor S, et al. Clinical evaluation of mitoxantrone and piroxicam in a canine model of human invasive urinary bladder carcinoma. Clin Cancer Res. 2003;9(2):906–11.
Greene SN, Lucroy MD, Greenberg CB, Bonney PL, Knapp DW. Evaluation of cisplatin administered with piroxicam in dogs with transitional cell carcinoma of the urinary bladder. J Am Vet Med Assoc. 2007;231(7):1056–60.
Abbo AH, Jones DR, Masters AR, Stewart JC, Fourez L, Knapp DW. Phase I clinical trial and pharmacokinetics of intravesical mitomycin C in dogs with localized transitional cell carcinoma of the urinary bladder. J Vet Intern Med. 2010;24(5):1124–30.
McMillan SK, Boria P, Moore GE, Widmer WR, Bonney PL, Knapp DW. Antitumor effects of deracoxib treatment in 26 dogs with transitional cell carcinoma of the urinary bladder. J Am Vet Med Assoc. 2011;239(8):1084–9.
Schrempp DR, Childress MO, Stewart JC, Leach TN, Tan KM, Abbo AH, et al. Metronomic administration of chlorambucil for treatment of dogs with urinary bladder transitional cell carcinoma. J Am Vet Med Assoc. 2013;242(11):1534–8.
Szigetvari NM, Dhawan D, Ramos-Vara JA, Leamon CP, Klein PJ, Ruple AA, et al. Phase I/II clinical trial of the targeted chemotherapeutic drug, folate-tubulysin, in dogs with naturally-occurring invasive urothelial carcinoma. Oncotarget. 2018;9(97):37042–53.
Nagaya T, Okuyama S, Ogata F, Maruoka Y, Knapp DW, Karagiannis SN, et al. Near infrared photoimmunotherapy targeting bladder cancer with a canine anti-epidermal growth factor receptor (EGFR) antibody. Oncotarget. 2018;9(27):19026–38.
Henry CJ, Flesner BK, Bechtel SA, Bryan JN, Tate DJ, Selting KA, et al. Clinical evaluation of tavocept to decrease diuresis time and volume in dogs with bladder cancer receiving cisplatin. J Vet Intern Med. 2018;32(1):370–6.
Knapp DW, Richardson RC, Chan TC, Bottoms GD, Widmer WR, DeNicola DB, et al. Piroxicam therapy in 34 dogs with transitional cell carcinoma of the urinary bladder. J Vet Intern Med. 1994;8(4):273–8.
Boria PA, Glickman NW, Schmidt BR, Widmer WR, Mutsaers AJ, Adams LG, et al. Carboplatin and piroxicam therapy in 31 dogs with transitional cell carcinoma of the urinary bladder. Vet Comp Oncol. 2005;3(2):73–80.
Mutsaers AJ, Mohammed SI, DeNicola DB, Snyder PW, Glickman NW, Bennett PF, et al. Pretreatment tumor prostaglandin E2 concentration and cyclooxygenase-2 expression are not associated with the response of canine naturally occurring invasive urinary bladder cancer to cyclooxygenase inhibitor therapy. Prostaglandins Leukot Essent Fatty Acids. 2005;72(3):181–6.
Arnold EJ, Childress MO, Fourez LM, Tan KM, Stewart JC, Bonney PL, et al. Clinical trial of vinblastine in dogs with transitional cell carcinoma of the urinary bladder. J Vet Intern Med. 2011;25(6):1385–90.
Knapp DW, Henry CJ, Widmer WR, Tan KM, Moore GE, Ramos-Vara JA, et al. Randomized trial of cisplatin versus firocoxib versus cisplatin/firocoxib in dogs with transitional cell carcinoma of the urinary bladder. J Vet Intern Med. 2013;27(1):126–33.
McMillan SK, Knapp DW, Ramos-Vara JA, Bonney PL, Adams LG. Outcome of urethral stent placement for management of urethral obstruction secondary to transitional cell carcinoma in dogs: 19 cases (2007–2010). J Am Vet Med Assoc. 2012;241(12):1627–32.
Henry CJ, Tyler JW, McEntee MC, Stokol T, Rogers KS, Chun R, et al. Evaluation of a bladder tumor antigen test as a screening test for transitional cell carcinoma of the lower urinary tract in dogs. Am J Vet Res. 2003;64(8):1017–20.
Mochizuki H, Shapiro SG, Breen M. Detection of BRAF mutation in urine DNA as a molecular diagnostic for canine urothelial and prostatic carcinoma. PLoS ONE. 2015;10(12): e0144170.
Mochizuki H, Kennedy K, Shapiro SG, Breen M. BRAF mutations in canine cancers. PLoS ONE. 2015;10(6): e0129534.
Aupperle-Lellbach H, Grassinger J, Hohloch C, Kehl A, Pantke P. Diagnostic value of the BARF variant V595E in urine samples, smears and biopsies from canine transitional cell carcinoma [Article in German]. Tierarztl Prax Ausg K Kleintiere Heimtiere. 2018;46(5):289–95.
Grassinger JM, Merz S, Aupperle-Lellbach H, Erhard H, Klopfleisch R. Correlation of BRAF variant V595E, breed, histological grade and cyclooxygenase-2 expression in canine transitional cell carcinomas. Vet Sci. 2019;6(1):31.
Childress MO, Adams LG, Ramos-Vara JA, Freeman LJ, He S, Constable PD, et al. Results of biopsy via transurethral cystoscopy and cystotomy for diagnosis of transitional cell carcinoma of the urinary bladder and urethra in dogs: 92 cases (2003–2008). J Am Vet Med Assoc. 2011;239(3):350–6.
Sakai K, Maeda S, Saeki K, Nakagawa T, Murakami M, Endo Y, et al. Anti-tumour effect of lapatinib in canine transitional cell carcinoma cell lines. Vet Comp Oncol. 2018;16(4):642–9.
Gustafson TL, Biller B. Use of toceranib phosphate in the treatment of canine bladder tumors: 37 cases. J Am Anim Hosp Assoc. 2019;55(5):243–8.
Ehrchen JM, Sunderkötter C, Foell D, Vogl T, Roth J. The endogenous Toll-like receptor 4 agonist S100A8/S100A9 (calprotectin) as innate amplifier of infection, autoimmunity, and cancer. J Leukoc Biol. 2009;86(3):557–66.
Hermani A, Hess J, de Servi B, Medunjanin S, Grobholz R, Trojan L, et al. Calcium-binding proteins S100A8 and S100A9 as novel diagnostic markers in human prostate cancer. Clin Cancer Res. 2005;11(14):5146–52.
Lorenz E, Muhlebach MS, Tessier PA, Alexis NE, Duncan Hite R, Seeds MC, et al. Different expression ratio of S100A8/A9 and S100A12 in acute and chronic lung diseases. Respir Med. 2008;102(4):567–73.
Yan WX, Armishaw C, Goyette J, Yang Z, Cai H, Alewood P, et al. Mast cell and monocyte recruitment by S100A12 and its hinge domain. J Biol Chem. 2008;283(19):13035–43.
Kim SK, Kim EJ, Leem SH, Ha YS, Kim YJ, Kim WJ. Identification of S100A8-correlated genes for prediction of disease progression in non-muscle invasive bladder cancer. BMC Cancer. 2010;10:21.
Kim WT, Kim J, Yan C, Jeong P, Choi SY, Lee OJ, et al. S100A9 and EGFR gene signatures predict disease progression in muscle invasive bladder cancer patients after chemotherapy. Ann Oncol. 2014;25(5):974–9.
Zhang L, Jiang H, Xu G, Wen H, Gu B, Liu J, et al. Proteins S100A8 and S100A9 are potential biomarkers for renal cell carcinoma in the early stages: results from a proteomic study integrated with bioinformatics analysis. Mol Med Rep. 2015;11(6):4093–100.
Cai H, Ye BG, Ao JY, Zhu XD, Zhang YY, Chai ZT, et al. High expression of S100A12 on intratumoral stroma cells indicates poor prognosis following surgical resection of hepatocellular carcinoma. Oncol Lett. 2018;16(4):5398–404.
Nicklas AP, Kramer MW, Serth J, Hennenlotter J, Hupe MC, Reimer DU, et al. Calgranulin A (S100A8) immunostaining: a future candidate for risk assessment in patients with non-muscle-invasive bladder cancer (NMIBC). Adv Ther. 2018;35(11):2054–68.
Heilmann RM, Wright ZM, Lanerie DJ, Suchodolski JS, Steiner JM. Measurement of urinary canine S100A8/A9 and S100A12 concentrations as candidate biomarkers of lower urinary tract neoplasia in dogs. J Vet Diagn Invest. 2014;26(1):104–12.
Heilmann RM, McNiel EA, Grützner N, Lanerie DJ, Suchodolski JS, Steiner JM. Diagnostic performance of the urinary canine calgranulins in dogs with lower urinary or urogenital tract carcinoma. BMC Vet Res. 2017;13(1):112.
Li DX, Wang XM, Tang Y, Yang YB, Feng DC, Li A, et al. Prognostic value of preoperative neutrophil-to-lymphocyte ratio in histological variants of non-muscle-invasive bladder cancer. Investig Clin Urol. 2021;62(6):641–9.
Mjaess G, Chebel R, Karam A, Moussa I, Pretot D, Abi Tayeh G, et al. Prognostic role of neutrophil-to-lymphocyte ratio (NLR) in urological tumors: an umbrella review of evidence from systematic reviews and meta-analyses. Acta Oncol. 2021;60(6):704–13.
Wang Y, Wang K, Ni J, Zhang H, Yin L, Zhang Y, et al. Combination of C-reactive protein and neutrophil-to-lymphocyte ratio as a novel prognostic index in patients with bladder cancer after radical cystectomy. Front Oncol. 2021;11: 762470.
Kool R, Marcq G, Shinde-Jadhav S, Mansure JJ, Saleh R, Rajan R, et al. Role of serum lymphocyte-derived biomarkers in nonmetastatic muscle-invasive bladder cancer patients treated with trimodal therapy. Eur Urol Open Sci. 2022;36:26–33.
Pierini A, Gori E, Lippi I, Ceccherini G, Lubas G, Marchetti V. Neutrophil-to-lymphocyte ratio, nucleated red blood cells and erythrocyte abnormalities in canine systemic inflammatory response syndrome. Res Vet Sci. 2019;126:150–4.
Becher A, Suchodolski JS, Steiner JM, Heilmann RM. Blood neutrophil-to-lymphocyte ratio (NLR) as a diagnostic marker in dogs with chronic enteropathy. J Vet Diagn Invest. 2021;33(3):516–27.
Conway EA, Pizarro Del Valle C, Waugh EM, French A, Ridyard AE. Retrospective investigation of the neutrophil-to-lymphocyte ratio in dogs with pneumonia: 49 cases (2011–2016). J Vet Emerg Crit Care (San Antonio). 2021;31(4):490–7.
Dinler AC. Neutrophil to lymphocyte ratio as a prognostic biomarker in puppies with acute diarrhea. J Vet Emerg Crit Care (San Antonio). 2022;32(1):83–9.
Macfarlane L, Morris J, Pratschke K, Mellor D, Scase T, Macfarlane M, McLauchlan G. Diagnostic value of neutrophil-lymphocyte and albumin-globulin ratios in canine soft tissue sarcoma. J Small Anim Pract. 2016;57(3):135–41.
Mutz M, Boudreaux B, Kearney M, Stroda K, Gaunt S, Shiomitsu K. Prognostic value of baseline absolute lymphocyte concentration and neutrophil/lymphocyte ratio in dogs with newly diagnosed multi-centric lymphoma. Vet Comp Oncol. 2015;13(4):337–47.
Khorramdelazad H, Bagheri V, Hassanshahi G, Karami H, Moogooei M, Zeinali M, et al. S100A12 and RAGE expression in human bladder transitional cell carcinoma: a role for the ligand/RAGE axis in tumor progression? Asian Pac J Cancer Prev. 2015;16(7):2725–9.
Center SA, McDonough SP, Bogdanovic L. Digital image analysis of rhodanine-stained liver biopsy specimens for calculation of hepatic copper concentrations in dogs. Am J Vet Res. 2013;74(12):1474–80.
Ebbing J, Mathia S, Seibert FS, Pagonas N, Bauer F, Erber B, et al. Urinary calprotectin: a new diagnostic marker in urothelial carcinoma of the bladder. World J Urol. 2014;32(6):1485–92.
Bausch K, Roth E, Heinz S, Horst D, Mathia S, Vlajnic T, et al. Urinary calprotectin loses specificity as tumour marker due to sterile leukocyturia associated with bladder cancer. PLoS One. 2019;14(3):e0213549.
Gottsch JD, Li Q, Ashraf F, O’Brien TP, Stark WJ, Liu SH. Cytokine-induced calgranulin C expression in keratocytes. Clin Immunol. 1999;91(1):34–40.
Lim MY, Thomas PS. Biomarkers in exhaled breath condensate and serum of chronic obstructive pulmonary disease and non-small-cell lung cancer. Int J Chronic Dis. 2013;2013: 578613.
Hofmann MA, Drury S, Fu C, Qu W, Taguchi A, Lu Y, et al. RAGE mediates a novel proinflammatory axis. Cell. 1999;97(7):889–901.
Srikrishna G, Nayak J, Weigle B, Temme A, Foell D, Hazelwood L, et al. Carboxylated N-glycans on RAGE promote S100A12 binding and signaling. J Cell Biochem. 2010;110(3):645–59.
Rivest S, Lacroix S, Vallières L, Nadeau S, Zhang J, Laflamme N. How the blood talks to the brain parenchyma and the paraventricular nucleus of the hypothalamus during systemic inflammatory and infectious stimuli. Proc Soc Exp Biol Med. 2000;223(1):22–38.
Simmons DL, Botting RM, Hla T. Cyclooxygenase isozymes: the biology of prostaglandin synthesis and inhibition. Pharmacol Rev. 2004;56(3):387–437.
Khan KN, Knapp DW, DeNicola DB, Harris RK. Expression of cyclooxygenase-2 in transitional cell carcinoma of the urinary bladder in dogs. Am J Vet Res. 2000;61(5):478–81.
Lee J-Y, Tanabe S, Shimohira H, Kobayashi Y, Oomachi T, Azuma S, et al. Expression of cyclooxygenase-2, P-glycoprotein and multi-drug resistance-associated protein in canine transitional cell carcinoma. Res Vet Sci. 2007;83(2):210–6.
Schneider R, Dorn CR, Taylor DO. Factors influencing canine mammary cancer development and postsurgical survival. J Natl Cancer Inst. 1969;43(6):1249–61.
Sorenmo K. Canine mammary gland tumors. Vet Clin North Am Small Anim Pract. 2003;33(3):573–96.
Heilmann RM, Guard MM, Toresson L, Unterer S, Grellet A, Grützner N. Association of clinical characteristics and lifestyle factors with fecal S100/calgranulin concentrations in healthy dogs. Vet Med Sci. 2021;7(4):1131–43.
Weisse C, Berent A, Todd K, Clifford C, Solomon J. Evaluation of palliative stenting for management of malignant urethral obstructions in dogs. J Am Vet Med Assoc. 2006;229(2):226–34.
Zahorec R. Ratio of neutrophil to lymphocyte counts—rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5–14.
İn E, Kuluöztürk M, Öner Ö, Deveci F. The importance of neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease. Turk Thorac J. 2016;17(2):41–6.
Heilmann RM, Suchodolski JS, Steiner JM. Purification and partial characterization of canine calprotectin. Biochimie. 2008;90(9):1306–15.
Heilmann RM, Cranford SM, Ambrus A, Grützner N, Schellenberg S, Ruaux CG, et al. Validation of an enzyme-linked immunosorbent assay (ELISA) for the measurement of canine S100A12. Vet Clin Pathol. 2016;45(1):135–47.
Acknowledgements
Part of the data has been presented as an oral abstract at the 32nd Annual Congress of the European College of Veterinary Internal Medicine-Companion Animals (ECVIM-CA), Gothenburg, Sweden (1–3 Sept 2022).
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was not supported by a grant or otherwise.
Author information
Authors and Affiliations
Contributions
JW, CG, SR, GUO, and RMH designed the study and enrolled patients in the study. JW, CG, WvB, DB, AS, SR, GUO, and RMH analyzed and interpreted the patient data. JW, CG, MP, GA, JMS, JS, and RMH analyzed the specimens and IHC data from dogs enrolled in the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations, and are reported in accordance with the ARRIVE guidelines. The protocol for collection of tissue samples from dogs with urinary tract disease and healthy dogs (animal use protocol) was independently reviewed and approved by the Regional Veterinary Council of the Free State of Saxony, Leipzig/Chemnitz, SN, Germany (TVA# 23/18), and written informed consent was obtained from the owners of all dogs that were prospectively enrolled into the study. For surplus specimens and medical records data of dogs that were retrospectively included in the study, written informed owner consent to the use of surplus samples and patient data had been obtained on the small animal clinic’s patient admission form at the time of the diagnostic investigation.
Consent for publication
Not applicable.
Competing interests
No conflicts of interest have been declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary Table 1. Overview of the patient demographic, treatment, outcome, and study participation information for the dogs in-cluded in the study (n=55).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Weinekötter, J., Gurtner, C., Protschka, M. et al. Tissue S100/calgranulin expression and blood neutrophil-to-lymphocyte ratio (NLR) in dogs with lower urinary tract urothelial carcinoma. BMC Vet Res 18, 412 (2022). https://doi.org/10.1186/s12917-022-03513-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12917-022-03513-z