
Abstract
Background
Moderate and late preterm (MLPT) birth accounts for the vast majority of preterm births, which is a global public health problem. The association between MLPT and neurobehavioral developmental delays in children and the underlying biological mechanisms need to be further revealed. The “placenta-brain axis” (PBA) provides a new perspective for gene regulation and risk prediction of neurodevelopmental delays in MLPT children.
Methods
The authors performed multivariate logistic regression models between MLPT and children’s neurodevelopmental outcomes, using data from 129 MLPT infants and 3136 full-term controls from the Ma’anshan Birth Cohort (MABC). Furthermore, the authors identified the abnormally regulated PBA-related genes in MLPT placenta by bioinformatics analysis of RNA-seq data and RT-qPCR verification on independent samples. Finally, the authors established the prediction model of neurodevelopmental delay in children with MLPT using multiple machine learning models.
Results
The authors found an increased risk of neurodevelopmental delay in children with MLPT at 6 months, 18 months, and 48 months, especially in boys. Further verification showed that APOE and CST3 genes were significantly correlated with the developmental levels of gross-motor domain, fine-motor domain, and personal social domain in 6-month-old male MLPT children.
Conclusions
These findings suggested that there was a sex-specific association between MLPT and neurodevelopmental delays. Moreover, APOE and CST3 were identified as placental biomarkers. The results provided guidance for the etiology investigation, risk prediction, and early intervention of neurodevelopmental delays in children with MLPT.
Similar content being viewed by others


Background
The World Health Organization defines preterm birth as delivery before 37 weeks of gestation and is further classified according to the gestational age of delivery: extremely preterm birth (< 28 weeks), very preterm birth (28–31+6 weeks), and moderate and late preterm birth (MLPT) (32–36+6 weeks) [1]. Extremely preterm birth and very preterm birth have attracted much attention due to high mortality and morbidity [2,3,4,5]. However, in recent years, studies have found that children with MLPT are also at greater risk of neurobehavioral developmental delays compared with full term (FT) children [6]. MLPTs account for approximately 84% of preterm births globally, and the dramatic increase in preterm birth rates in recent decades is largely attributable to the growth in the number of MLPTs [7, 8]. Therefore, MLPT is a global public health problem, and its impact on human health, population quality, and national economy cannot be ignored.
Abnormal intrauterine environment is not suitable for fetal growth and development and may lead to the occurrence of MLPT. The placenta is not only a maternal–fetal barrier but also a maternal–fetal link bridge between endogenous development and postnatal growth and development [9,10,11,12], which plays a key role in maintaining a suitable intrauterine environment. Therefore, the placenta is an important organ for understanding the intrauterine regulatory mechanism of neurodevelopmental outcomes, and the concept of the “placenta-brain” axis was born [13], which has become a potential source of early identification of high-risk infant biomarkers. Recent studies have found that lots of abnormally regulated genes in the placenta affect fetal brain development; these genes are defined “placenta-brain axis (PBA) genes,” including genes in pathways related to neurotransmitter synthesis and secretion, immunity and inflammation, and cell surface receptor signaling [14, 15].
In this study, we first investigated the association between MLPT and neurodevelopmental delays in children based on the prospective birth cohort MABC. Secondly, we screened out the abnormally regulated PBA-related gene sets in MLPT children’s placentas and verified them in an independent cohort, providing a basis for placental regulation in MLPT children with an increased risk of neurodevelopmental delays. Finally, we further identified sex-specific RNAs associated with neurodevelopmental outcomes in the placentas of MLPT children through RT-qPCR and established a risk prediction model based on these RNA biomarkers using machine learning methods. This study provides guidance for the etiology investigation, risk prediction, and early intervention of neurodevelopmental delays in children with MLPT.
Methods
Study design and population
This study was based on Ma’anshan Birth Cohort (MABC), which is a longitudinal study of health during early life period in Ma’anshan, Anhui, China. The MABC was recruited from May 2013 to September 2014, with women from the Ma’anshan Maternal and Child Health Hospital. The inclusion criteria for pregnant women were as follows: (1) ≥ 18 years old and ≤ 14 gestational weeks; (2) willing to have antenatal checkups and childbirth in Ma’anshan Maternal and Child Health Hospital; (3) had no serious physical diseases or serious mental illness and could complete the questionnaires independently; (4) willing to participate in follow-ups during childhood. A total of 3474 pregnant women from MABC study were eligible. The study protocol has been approved by the Ethics Committee of Anhui Medical University (No. 20131195). All participants provided written informed consent. A detailed description of the cohort information and inclusion and exclusion criteria has been published elsewhere [16].
The China National Birth Cohort (CNBC) was used as an independent sample source to verify the differential expression of PBA-related genes. The CNBC study conducted in Ma’anshan, Anhui, China, is a prospective birth cohort study recruited from May 2017 to September 2018. The inclusion criteria for pregnant women were as follows: (1) Chinese residents of Ma’anshan city; (2) ≥ 18 years old and ≤ 14 gestational weeks; (3) conceived naturally; (4) willing to have antenatal checkups and childbirth in Ma’anshan Maternal and Child Health Hospital; (5) willing to participate in follow-ups during childhood. A total of 1508 women were recruited from the Ma’anshan Maternal and Child Health Hospital. Details of the inclusion exclusion criteria have been published previously [17].
Children’s neurodevelopment assessment and definition
Children’s neurodevelopmental behavior was assessed by the Ages and Stages Questionnaire of China (ASQ-C) at the age of 6 months, 18 months, and 48 months based on the responses filled in by the children’s parents or guardians. The ASQ-C was translated from the ASQ with necessary cross-cultural adaptations for China [18], which contains a series of 30 questions representing five domains or developmental areas: gross motor skill domain, fine motor skill domain, communication domain, personal-social skill domain, and problem solving domain. The sum of the scores from the 6 questions in each domain provides the final score [19]. The maximum score of each domain was 60, a score that was 1 SD (standard deviation) below the mean of each domain was used as the principal cutoff point in the present study, and children with scores in each domain below 1 SD relative to the mean were defined as having SDD (suspected developmental delay) [20].
Confounders and covariates
According to previously published studies [21] and our univariate analysis results, we obtained following confounders and covariates: maternal information about the age at children’s birth, pre-pregnancy body mass index (BMI), feeding patterns at 6 months, monthly income of family per capita, educational level, smoking status during pregnancy, pregnancy-related anxiety, and children’s information about sex.
Information on monthly income of family per capita, educational level and smoking during pregnancy, feeding patterns at 6 months, and pregnancy-related anxiety were obtained from children’s mothers in the structured self-administered questionnaires. Information on maternal age at child’s birth and child sex were extracted from medical records. Maternal pre-pregnancy BMI [BMI = weight (kg)/height (m)2] was measured by doctors at the time of the first prenatal checkup.
Placenta samples collection
Placental tissue samples were collected by trained personnel immediately after delivery. The edge part of the placenta and the area near the umbilical cord were avoided during sample collection. The samples were taken at least 3 cm from the cord insertion and 3 cm from the placental edge. After washing with normal saline, extracted placental lobules without calcified or fascia were dissected and longitudinally cut into four equal-sized sections, each containing both maternal and fetal surfaces. They were then immersed in RNAlater and refrigerated for 4 °C overnight. The next morning, after pouring off the RNAlater fluid, the placental tissue was stored at − 80 °C until use.
RNA extraction and sequencing
We selected 30 MLPT placentas from the placenta samples collected from the MABC cohort as the case group for RNA sequencing, including 15 male MLPT placentas and 15 female MLPT placentas. In addition, strictly matching the age of pregnant women, pre-pregnancy BMI, and fetal sex, we selected 30 FT placentas as the control group for RNA sequencing. Total RNA was extracted from the placenta using TRIzol® Reagent according the manufacturer’s instructions (Magen). RNA samples were detected based on the A260/A280 absorbance ratio with a Nanodrop ND-2000 system (Thermo Scientific, USA), and the RIN of RNA was determined by an Agilent Bioanalyzer 4150 system (Agilent Technologies, CA, USA). Qualified samples were used for library construction. Paired-end libraries were prepared using a ABclonal mRNA-seq Lib Prep Kit (ABclonal, China) following the manufacturer’s instructions. The mRNA was purified from 1 μg total RNA using oligo (dT) magnetic beads followed by fragmentation carried out using divalent cations at elevated temperatures in ABclonal First Strand Synthesis Reaction Buffer. Subsequently, first-strand cDNAs were synthesized with random hexamer primers and reverse transcriptase (RNase H) using mRNA fragments as templates, followed by second-strand cDNA synthesis using DNA polymerase I, RNAseH, buffer, and dNTPs. The synthesized double stranded cDNA fragments were then adapter-ligated for preparation of the paired-end library. Adaptor ligated cDNA were used for PCR amplification. PCR products were purified (AMPure XP system) and library quality was assessed on an Agilent Bioanalyzer 4150 system. Finally, sequencing was performed with an Illumina Novaseq 6000 /MGISEQ-T7 instrument.
Bioinformatics analysis of RNA-seq data
The data generated from Illumina platform were used for bioinformatics analysis. Raw data of fastq format were firstly processed through fastp (https://github.com/OpenGene/fastp). In this step, remove the adapter sequence and filter out low quality (low quality, the number of lines with a string quality value less than or equal to 25 accounts for more than 60% of the entire reading), and N (N means that the base information cannot be determined) ratio is greater than 5% reads to obtain clean reads that can be used for subsequent analysis. Samples that failed quality control (QC) were removed from downstream analysis. Then, clean reads were separately aligned to reference genome with orientation mode using the HISAT2 software (http://daehwankimlab.github.io/hisat2/) to obtain mapped reads. FeatureCounts (http://subread.sourceforge.net/) was used to count the reads numbers mapped to each gene. And then FPKM of each gene was calculated based on the length of the gene and reads count mapped to this gene. We used edgeR package to identify differentially expressed genes (DEGs) between the placentas of MLPT children and FT children [22]. Based on some published literature [23,24,25], genes were considered statistically significant at |log2fold-change|> =|log2(1.5)| and FDR < 0.2. To evaluate the biological functions, the computational web servers g:Profiler (https://biit.cs.ut.ee/gprofiler/gost) was used to perform Kyoto Encyclopedia of Genes and Genomes (KEGG) and the gene ontology (GO) pathway analysis for DEGs of interest [26]. GO and KEGG pathway terms with the FDR of the Fisher’s exact test < 0.05 were considered statistically significant.
Curation of PBA-related genes
A comprehensive search was performed to identify studies from inception to 18 January 2022 that involved PBA genes. The applied search terms were broad, including synonyms and truncations of “placenta,” “neurodevelopment,” “predict,” “biomarker,” “brain,” “multi-omics,” and “disorders.” The selected literature must contain both the terms “placenta” and “brain” and the remaining terms help to filter. We carefully read the collected literature and excluded some of the irrelevant literature, to ensure that the literature cited can provide the PBA genes and PBA pathways. The PBA genes were collected from literature that suggested that abnormalities of these genes in the placenta could cause neurodevelopmental abnormalities in children. The PBA pathway genes were collected from PBA pathways, including neurotransmitter-related pathways such as serotonin, dopamine, and norepinephrine/adrenaline. These neurotransmitters were secreted by the placenta during pregnancy and had an important impact on fetal brain development [13, 27,28,29,30]. There were 40 PBA genes and 636 PBA pathway genes, of which 7 genes belong to both PBA genes and PBA pathway genes. Finally, we collected 669 PBA-related genes in total.
RT-qPCR validation
RNA extraction and RT-qPCR were performed according to the manufacturer’s instructions. Briefly, total RNA was extracted from placenta samples using Trizol (Invitrogen 15,596–026). The concentration and purity of RNA were measured by Denovix spectrophotometer (Thermo Scientifc, Wilmington, DE, USA). Then, RNA was reverse-transcribed using the Evo M-MLV RT-PCR Kit (AG11707). Real-time RT-PCR was implemented after reverse transcription. Expression levels were quantified using a LightCycler 96 Instrument’s realtime PCR system (Roche 05815916001) with a SYBR Green master mix (Yeasen 11201ES08). Primers are shown in Additional file 1: Table S1. Data were exported to Excel; relative gene expression was calculated by the comparative CT method (ΔΔCT) and normalized based on the level of human 18S mRNA. The differences between two groups were analyzed using a two-tailed Mann–Whitney test. Each value reflects the mean ± standard error of the mean (SEM) of at least three different biological replicates.
Machine learning method for building prediction models
Three machine learning methods including logistic regression (LR), random forest (RF), and decision tree (DT) were used to evaluate the classification performance of the selected features. We used the leave-one-out cross-validation (LOOCV) for model selection. The prediction performance of each model was evaluated by the area under the receiver operating characteristic curve (AUROC). All analyses were performed with python version 3.10.
Statistical analysis
Descriptive statistics for maternal demographic and obstetric characteristics were described by MLPT using the mean ± standard deviation (SD) or percentage (n %). The differences between two groups were analyzed using Student’s t-test. Multiple comparisons were performed using ANOVA.
The association between MLPT and neurodevelopmental delay at 6, 18, and 48 months was analyzed separately by children’s sex by using the odds ratio (OR) and 95% confidence interval (CI) in multivariable logistic regression model. The repeated measurement analysis of the association between MLPT and different ASQ domains was calculated by using generalized estimating equations (GEE) analysis. The Mann–Whitney test was used to compare the two groups such as placental mRNA expression and neurodevelopmental delay.
Statistical analyses, including Student’s t-test, ANOVA, logistic regression, Mann–Whitney test, and receiver operator characteristic (ROC), were performed by the R software (ver. 4.1.2; R Foundation for Statistical Computing, Vienna, Austria) and SPSS (version 22.0, Chicago, IL, USA) software. The significance threshold was set at a p-value < 0.05.
Results
Demographics
This study was based on Ma’anshan Birth Cohort (MABC). One hundred twenty-nine MLPT infants and 3136 full term (FT) controls were recruited. The average gestational age at delivery was 35.2 weeks (standard deviation [SD], 1.11) for the MLPT group and 39.2 weeks (SD, 1.08) for the FT group. Compared with the FT group, the infants in the MLPT group were more likely to have lower birth weights; the mothers in the MLPT group have greater age at delivery, higher prenatal BMI, higher smoking rates, and higher rates of pregnancy-related complications, such as diabetes mellitus in pregnancy and hypertensive disorder complication pregnancy (Table 1 and Fig. 1).

Flowchart of participants through the children’s ASQ-C follow-up
Associations between MLPT and neurodevelopmental delay
We applied ASQ-C to assess children’s neurodevelopmental behavior at the age of 6, 18, and 48 months, which filled in by the children’s parents or guardians. Then, we evaluated the associations between MLPT and neurodevelopmental outcomes based on ASQ-C data. The age of pregnant women, body mass index (BMI) before pregnancy, educational level of pregnant women, duration of breastfeeding, child sex, per capita monthly income of the family, pregnancy-related anxiety, and smoking status of pregnant women were taken as confounding factors; the development of MLPT children in the gross motor domain at 6 months was significantly delayed (OR = 2.17, 95% CI = 1.15–4.08, P-value = 0.017); the development of MLPT children in communication domain was significantly delayed at 18 months (OR = 2.07, 95% CI = 1.12–3.84, P-value = 0.021); the development of MLPT children in gross motor domain (OR = 1.84, 95%CI = 1.08–3.13, P-value = 0.025) and personal-social domain (OR = 1.92, 95% CI = 1.10–3.36, P-value = 0.023) was significantly delayed at 48 months (Fig. 2a). Stratified by sex, boys with MLPT showed significantly delayed development in the gross motor domain (OR = 2.73, 95% CI = 1.23–6.07, P-value = 0.014), fine motor domain (OR = 2.73, 95% CI = 1.43–5.22, P-value = 0.002), and personal-social domain (OR = 1.94, 95% CI = 1.01–3.74, P-value = 0.048) at 6 months, the communication domain at 18 months (OR = 2.07, 95% CI = 1.01–4.23, P-value = 0.046), and the gross motor domain at 48 months (OR = 2.09, 95% CI = 1.05–4.16, P-value = 0.036) (Fig. 2b). As for girls with MLPT, the development of gross motor domain was significantly delayed at 18 months (OR = 3.35, 95% CI = 1.22–9.17, P-value = 0.019), and the development of personal-social domain was significantly delayed at 48 months (OR = 2.69, 95% CI = 1.05–6.92, P-value = 0.040) (Fig. 2c). Moreover, repeated measurement analysis and multiple testing correction does enhance the reliability of the results, so we calculated the association between MLPT and different domains of ASQ at 6, 18, and 48 months by using generalized estimating equations (GEE) analysis (Additional file 1: Table S2) and reported false discovery rates of different domains and different ages of ASQ respectively calculated by using Bonferroni-Holm method (Additional file 1: Table S3). After adjustment for confounders same as above, we found that the development of MLPT children in the gross motor domain (OR = 0.58, 95% CI = 0.39–0.85, P-value = 0.006) and personal-social domain was significantly delayed (OR = 0.61, 95% CI = 0.42–0.90, P-value = 0.013). Stratified by sex, boys with MLPT showed significantly delayed development in the gross motor domain (OR = 0.56, 95% CI = 0.33–0.95, P-value = 0.033), fine motor domain (OR = 0.56, 95% CI = 0.35–0.90, P-value = 0.018), and personal-social domain (OR = 0.60, 95% CI = 0.39–0.93, P-value = 0.021). No significant result was found between MLPT and neurodevelopmental delay in girls. These results provide more convincing evidence of an increased risk of neurodevelopmental delay in MLPT children, especially in boys.

Associations between MLPT exposure and neurodevelopmental delays. a All. b Male. c Female. The model adjusted for characteristics of mothers (maternal age, maternal pre-pregnancy BMI, maternal educational level, monthly income of family per capita, passive smoking status, breastfeeding duration, pregnancy-related anxiety) and children (sex). *p < 0.05, **p < 0.01, multivariate logistic regression analysis. MLPT, moderate and late preterm; BMI, body mass index; ASQ, Ages and Stages Questionnaire; CI, confidence interval; OR, odds ratio
Transcriptome-wide analysis of placentas from MLPT and full-term birth
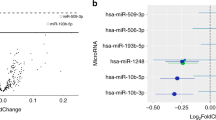
To examine whether alterations in the placental transcriptome are associated with an increased risk of neurodevelopmental delay in children with MLPT, we profiled RNA-seq to identify dysregulated genes in the placentas of MLPT infants (Additional file 1: Table S4). Considering sex specificity, we divided the data into three groups for analysis, namely “all,” “male,” and “female” groups. In total, 67 upregulated genes and 16 downregulated genes were identified between MLPT and FT in the all group (Fig. 3a, b). Seven hundred nine upregulated genes and 65 downregulated genes were identified between MLPT and FT in the male group; 86 upregulated genes and 398 downregulated genes were identified between MLPT and FT in the female group (Additional file 1: Table S5). There were only a few common DEGs among the all, male, and female groups (Fig. 3c, d), which reflects that the relevance of placental gene expression to MLPT is sex-specific and provides potential clues for the sex specificity in incidence and risks of neurodevelopmental delays of MLPT children.

Analysis of differentially expressed genes (DEGs) in placenta samples from MABC study. a Volcano plot for all genes in the MLPT infants’ placentas vs FT infants’ placentas. b Heatmap of DEGs in placenta samples of MLPT infants and FT infants. c, d Upset plot of upregulated genes and downregulated genes of both all, male, and female. c Upregulated; d downregulated. e, f GO functional annotation clustering analysis of DEGs. g, h KEGG pathway analysis
We further investigated functional coherence by calculating enrichment in curated pathways from Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG). As for GO categories, although the number and types of up regulated genes varied widely between the all, male, and female groups, they were all enriched for biological pathways related to immune response and antigen binding. Among them, the placenta of male MLPT infants has the largest number of upregulated genes and the highest enrichment in biological pathways such as leukocyte-mediated immunity and lymphocyte-mediated immunity, while the upregulated genes in the placenta of female MLPT infants were also enriched in pathways related to B cell-mediated immunity and immunoglobulin-mediated immune response (Fig. 3e). For all MLPT infants, the upregulated genes were enriched in biological pathways related to humoral immune response. The downregulated genes in the placenta of male MLPT infants were associated with pathways about multicellular organismal process and secondary metabolic process. In addition, the downregulated genes in the placenta of female MLPT infants were also enriched in pathways related to transmembrane signaling receptor activity, immune response, and cytokine production (Fig. 3f).
As for KEGG pathways, the upregulated genes in the placenta of male MLPT infants were enriched for NF-kappa B signaling pathway, NOD-like receptor signaling pathway, and B cell receptor signaling pathway. In the placenta of female MLPT infants, the downregulated genes were associated with pathways of neutrophil extracellular trap formation, chemokine signaling pathway, etc. (Fig. 3g, h).
Dysregulated PBA-related genes were identified as potential biomarkers
To investigate whether DEGs in MLPT placenta are associated with the increased risk of neurodevelopmental delay in MLPT fetuses, we collected PBA-related gene sets from the literature and related pathways (Additional file 1: Table S6-S7). These PBA-related genes are involved in neurodevelopment pathways, such as synaptic signaling and neuron projection (Additional file 2: Figure S1). Then, we firstly overlapped DEGs with PBA-related genes, and there were 4, 30, and 17 differentially expressed PBA-related genes in the all, male, and female groups, respectively (Fig. 4a). Secondly, to eliminate noise from genes with very low expression levels, we filtered out genes with median FPKM < 1 in both the MLPT and FT groups, leaving 2, 16, and 7 PBA-related genes in the all, male, and female groups, respectively (Fig. 4b). Furthermore, for PBA pathway genes, we retained the genes whose coefficient of variation (CV) were less than 1 in both MLPT and FT group. Finally, there were 14 PBA-related genes (including 12 PBA pathway genes and 2 PBA genes) for subsequent experimental verification (Additional file 1: Table S8), among which 2, 9, and 4 were in the all, male, and female groups, respectively (Fig. 4c–e). Regardless of sex specificity, CST3 and CA2 were upregulated in the all group (Fig. 4c). Considering sex specificity, CXCL8, CA2, PRKCD, TREM2, KCNQ1, GNG5, GNB2, CST3, and APOE were upregulated in the male group (Fig. 4d); KCNG1 was upregulated, and PTGS2, CXCR2, and LIN7A were downregulated in the female group (Fig. 4e). In short, we selected 14 placenta-brain axis-related genes which were also DEGs for further experimental validation considering fold change, FDR and CV (Additional file 1: Table S9).

Association between DEGs and PBA-related genes from manual collection and validation of the PBA-related genes in placenta samples from CNBC study. a Venn plot of DEGs in MABC study with the PBA-related gene set. The significance of overlap was calculated by hypergeometric test. b Heatmap of log2FC for selected PBA-related genes. c–e Boxplot of FPKM for 14 PBA-related genes. c All; d male; e female. f In all placenta samples, CST3 mRNA expression are not significantly associated with MLPT. g In male placenta samples, GNB2, APOE, and CST3 mRNA expression are significantly increased in MLPTs. h In female placenta samples, CXCR2 and PTGS2 mRNA expression are significantly increased in MLPTs. *p < 0.05, **p < 0.01, Mann–Whitney-Wilcoxon test. Error bars indicate SEM
Independent validation of the selected biomarkers
We further validated the selected 14 PBA-related genes using RT-qPCR in an independent cohort (CNBC, see “ Methods” section). Regardless of sex specificity, CST3 was upregulated in the MLPT placentas, which was consistent with the trend in RNA-seq (Fig. 4f). Considering sex specificity, the expression pattern of four RNAs in male placentas and four RNAs in female placentas validated in CNBC from RT-qPCR were all consistent with those in MABC from RNA-seq. Additionally, three (GNB2, APOE, CST3) RNAs in male and two (CXCR2, PTGS2) RNAs in female and showed statistical significance (Fig. 4g–h). Other PBA-related RNAs’ expression patterns for experimental validation in CNBC cohort were contrary to the expression trend in RNA-seq (Additional file 2: Figure S2).
Prediction models for neurodevelopmental delay in MLPT children
Next, we performed RT-qPCR to evaluate the performance of the identified signatures for predicting neurodevelopmental delay of male (three RNAs) and female (two RNAs) in MLPT cohort. We found that APOE and CST3 were significantly upregulated in the placentas of MLPT children with developmental delay in gross motor skills domain, fine motor skills domain, and personal-social skills domain at 6 months, which suggested that APOE and CST3 are reliable biomarkers for neurodevelopment prediction of MLPT children (Fig. 5a–c and Additional file 2: Figure S3).

Validation of the three main PBA-related genes in male placenta samples from MABC study and ROC curves of three prediction models for neurodevelopment in MLPT children from MABC study. a–c For male neurodevelopment delay at 6 months, APOE and CST3 mRNA expression are significantly increased in MLPTs. a Gross-motor domain; b fine-motor domain; c personal-social domain. d–f ROC curves of prediction model using random forest. d Gross-motor domain; e fine-motor domain; f personal-social domain. Base model: birth weight + gestational age at delivery + maternal age + monthly income family capita + pre-pregnancy BMI, mixed model: APOE + CST3 + base model. g–i ROC curves of prediction model using logistic regression. g Gross-motor domain; h fine-motor domain; i personal-social domain. Base model: birth weight + gestational age at delivery + maternal age + monthly income family capita + pre-pregnancy BMI, mixed model: APOE + CST3 + base model. j–l ROC curves of prediction model using decision tree. j Gross-motor domain; k fine-motor domain; l personal-social domain. Base model: birth weight + gestational age at delivery + maternal age + monthly income family capita + pre-pregnancy BMI, mixed model: APOE + CST3 + base model
Next, we used three classifiers to access the predictive capacity of APOE and CST3 expression level determined by RT-qPCR. We found that the random forest (RF) model that take both APOE and CST3 as input achieved a higher AUC in predicting the gross motor skills domain (AUC = 0.861), fine motor skills domain (AUC = 0.822), and personal-social skills domain (AUC = 0.833) than model take APOE or CST3 alone, which also outperformed the logistic regression (LR) and decision tree (DT) models based on the same data as a whole (Fig. 5d–l). Adding potentially relevant clinical factors (birth weight, gestational age at delivery, maternal age, monthly income of family per capita and pre-pregnancy BMI) could not further boost model performance. It proved that APOE and CST3 expression levels alone are good predictors (Additional file 1: Table S9).
Discussion
The intensity and duration of the effect of MLPT on children’s neurobehavioral development remain to be determined. A longitudinal cohort study in Australia found that MLPT children had significantly higher risks of cognitive delay, language delay, motor delay, and social-emotional ability problems at the correction age of 2 years compared with children born at term [31]. A study from China revealed that MLPT children had a high overall developmental delay rate, especially in the fine motor domain (OR: 2.43, 95% CI: 1.04–5.56) [32]. However, an Italian study using the Bayley-II Scale to evaluate the neural development of infants and young children found that the strength of association between MLPT and neural development did not reach a statistically significant level at the corrected age of 12 and 18 months [21]. Overall, our prospective cohort study indicated that there existed a strong statistically significant association between MLPT and neurodevelopmental delays from 6 months old to 48 months old, which provided obvious evidence for an increased risk of neurodevelopmental delay in children with MLPT.
Furthermore, our data informed that PBA-related genes might be the potential gene targets of MLPT’s impact on fetal neurodevelopment. The placenta acts as an endocrine organ and secretes neuroactive signaling molecules that regulate the function of other endocrine glands to effect infants’ neurodevelopment [33,34,35,36]. In our study, we systematically collected the PBA-related gene sets from published articles and related databases, which provided a useful resource for subsequent studies.
Our results suggested that male MLPT infants were associated with more neurodevelopmental delays than females. Similarly, recent studies indicated that there were sex-specific in neurodevelopmental outcomes in preterm infants [37,38,39]. Male neurodevelopment appeared to be much more sensitive than female to poor postnatal growth, but the specific mechanism still needed to be explored [40, 41]. The above results indicated that both neurodevelopmental outcomes and PBA-related genes are sex-specific in MLPT infants.
It is well known that APOE is an important gene in the occurrence and progression of neurodegenerative diseases [42, 43]. In recent years, the role of APOE in children’s neurodevelopment has also attracted much attention [44,45,46]. APOE was an important molecule due to not only its lipid transport and cholesterol metabolic functions but also involved in several biological processes, such as response to oxidative stress, cGMP biosynthetic processes, and glutamate receptor clustering [47], which are associated with controlling brain microenvironment homeostasis and partially modulating synaptic plasticity. What is more, lipopolysaccharides (LPS) induced inflammation and decreased the mRNA expression level of APOE in both rat and human placentas [48]. In addition to this anti-inflammatory function, placental APOE also promotes the transfer of cholesterol from maternal to fetal circulation. APOE has been shown to be anti-inflammatory, neuroprotective, and essential for neurodevelopment [49, 50]. APOE might work as an important factor for neurodevelopmental disabilities [51]. CST3 gene encodes an inhibitor of cysteine proteinases, which is widely found in biological fluids and especially in the cerebrospinal fluid that surrounds and protects the brain and spinal cord [52]. The gene’s function is related to the formation of amyloid plaques; thus, it has already been shown to be involved in some brain disorders [53, 54]. Previous studies are showing that CST3 is strongly expressed in the brain and decidual tissue of the placenta [55,56,57]. It had been demonstrated that an overexpression of the CST3 gene in the placenta and higher levels of cystatin C existed in the dopamine-depleted rat striatum [58]. There was a link between these early insults and neurodevelopmental disorders in which there is dopamine dysregulation [27]. Thus, the placental abnormal expression of CST3 might cause abnormal neurodevelopment in children by dysregulation affecting dopamine. Recently, based on the result of a whole genome methylation analyze of schizophrenia patients [59], CST3 was considered to be important for neurodevelopment [60]. Besides, some studies suggest that injection of CST3 into the hippocampus and dentate gyrus or in vitro application of CST3 played a role in the mediation of neuronal death, and increased expression of CST3 in glial cells was accompanied by neuronal death [61, 62]. These studies also provide support for our finding that CST3 can be used as a biomarker for neurodevelopment. However, APOE and CST3 are PBA pathway genes that we screened based on the PBA pathway. These existing studies are not enough to prove that the abnormal regulation of APOE, and CST3 in the placenta will affect the neural development of the fetus. Our study provides clues for this, but further experiments are still needed to reveal the potential mechanism.
Our study has several advantages. First, we elucidate the strength and duration of the effect of MLPT on children’s neurobehavioral development based on a large birth cohort, with prospective cohort studies to reduce recall bias and repeated measures at different months of age to increase confidence. Poor ASQ performance in children at early age has been shown to be sensitive to the diagnosis of ASD, a more severe neurodevelopmental disorder [63]. Therefore, our conclusion has certain guiding significance for the early detection of ASD in children with MLPT. Secondly, we systematically sorted out the PBA-related genes and provided resources for related research. For the first time, we focused on MLPT, rather than the placental transcriptome of all preterm or very preterm children, and revealed that placental gene regulation in MLPT children is aberrant and sex-specific. In the end, the results of this study will serve as evidence for the increased risk of abnormal neurobehavioral development in MLPT children, provide targets for molecular mechanism research, offer biomarkers and intelligent models for risk prediction, and shed light on early management and intervention of MLPT children.
However, our study also has some limitations. First, the sex-specific association between high placental APOE and CST3 expression and increased risk of neurobehavioral developmental delays in MLPT children requires further in vivo and in vitro experiments to reveal the mechanism. In addition, although the PBA-related genes were collected from the literature after rigorous screening, they were not come from the meta-analysis which may weaken the reliability of evidence. Further understanding of PBA-related genes would require a formal systematic review which contains a more global analysis. In the differential expression analysis, we used a significance threshold of FDR < 0.2 for this analysis based on some published literature to avoid missing the potential differences. However, the DEGs identified need further verification to avoid false positives. Due to technical limitations, it is difficult to accurately distinguish maternal and fetal surfaces in our placenta samples. Moreover, because placental tissue is composed of multiple cell types, including stromal cells, mesenchymal cells, and trophoblast cells, biomarker detection may be somewhat heterogeneous [64,65,66]. What is more, although it is reasonable to assume that the gene expression of APOE and CST3 in placenta will influence the neurodevelopment of infants, the expression trends of APOE and CST3 in the fetal brains may be different from the trends in the placentas, which still needs more studies to explore the regulations of APOE and CST3 by using fetal brain samples. Therefore, the prediction model composed of APOE and CST3 needs to be validated in larger independent cohort.
Conclusions
This study supports a sex-specific association between MLPT and neurodevelopmental delay in children and demonstrated that the placental-brain axis genes could be used as placental biomarkers to predict the risk of neurodevelopmental delay in boys with MLPT.
Availability of data and materials
The RNA sequencing datasets generated and analyzed in the current study have been submitted to the NCBI Sequencing Read Archive (SRA) with accession number SRP410951.
Abbreviations
- ASQ-C:
-
Ages and Stages Questionnaire of China
- AUC:
-
Area under curve
- BMI:
-
Body mass index
- BP:
-
Biological process
- CC:
-
Cellular component
- CNBC:
-
China National Birth Cohort
- DEGs:
-
Differentially expressed genes
- DT:
-
Decision tree
- GEE:
-
Generalized estimating equations
- GO:
-
Gene ontology
- LR:
-
Logistic regression
- MABC:
-
Ma’anshan Birth Cohort
- MF:
-
Molecular function
- MLPT:
-
Moderate and late preterm
- OR:
-
Odds ratio
- PBA:
-
Placenta-brain axis
- RF:
-
Random forest
- ROC:
-
Receiver operator characteristic
- RT-qPCR:
-
Real-time quantitative PCR
References
Chawanpaiboon S, Vogel JP, Moller AB, Lumbiganon P, Petzold M, Hogan D, et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health. 2019;7(1):e37–46.
Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–35.
Cao G, Liu J, Liu M. Global, regional, and national incidence and mortality of neonatal preterm birth, 1990–2019. JAMA Pediatr. 2022;176(8):787–96.
Deng K, Liang J, Mu Y, Liu Z, Wang Y, Li M, et al. Preterm births in China between 2012 and 2018: an observational study of more than 9 million women. Lancet Glob Health. 2021;9(9):e1226–41.
Bolk J, Farooqi A, Hafström M, Åden U, Serenius F. Developmental coordination disorder and its association with developmental comorbidities at 6.5 years in apparently healthy children born extremely preterm. JAMA Pediatr. 2018;172(8):765–74.
Natarajan G, Shankaran S. Short- and long-term outcomes of moderate and late preterm infants. Am J Perinatol. 2016;33(3):305–17.
Martin JA, Hamilton BE, Osterman MJK, Driscoll AK, Drake P. Births: final data for 2016. Natl Vital Stat Rep. 2018;67(1):1–55.
Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–72.
Gillman MW. Developmental origins of health and disease. N Engl J Med. 2005;353(17):1848–50.
O’Donnell KJ, Meaney MJ. Fetal origins of mental health: the developmental origins of health and disease hypothesis. Am J Psychiatry. 2017;174(4):319–28.
Nomura Y, Rompala G, Pritchett L, Aushev V, Chen J, Hurd YL. Natural disaster stress during pregnancy is linked to reprogramming of the placenta transcriptome in relation to anxiety and stress hormones in young offspring. Mol Psychiatry. 2021;26(11):6520–30.
Ramirez-Celis A, Croen LA, Yoshida CK, Alexeeff SE, Schauer J, Yolken RH, et al. Maternal autoantibody profiles as biomarkers for ASD and ASD with co-occurring intellectual disability. Mol Psychiatry. 2022;27:3760–7.
Rosenfeld CS. The placenta-brain-axis. J Neurosci Res. 2021;99(1):271–83.
Shallie PD, Naicker T. The placenta as a window to the brain: a review on the role of placental markers in prenatal programming of neurodevelopment. Int J Dev Neurosci. 2019;73:41–9.
Behura SK, Dhakal P, Kelleher AM, Balboula A, Patterson A, Spencer TE. The brain-placental axis: therapeutic and pharmacological relevancy to pregnancy. Pharmacol Res. 2019;149:104468.
Ge X, Tao F, Huang K, Mao L, Huang S, Niu Y, et al. Maternal snoring may predict adverse pregnancy outcomes: a cohort study in China. PLoS One. 2016;11(2):e0148732.
Lu MJ, Huang K, Yan SQ, Zhu BB, Shao SS, Zhu P, et al. Association of antenatal anxiety with preterm birth and low birth weight: evidence from a birth cohort study. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(7):1072–5.
Yue A, Jiang Q, Wang B, Abbey C, Medina A, Shi Y, et al. Concurrent validity of the Ages and Stages Questionnaire and the Bayley Scales of Infant Development III in China. PLoS One. 2019;14(9):e0221675.
Squires J, Bricker DD, Twombly E. Ages & stages questionnaires, social-emotional (ASQ:SE-2TM)) : a parent-completed child monitoring system for social-emotional behaviors. 2nd ed. Baltimore, Maryland: Brookes Publishing; 2015.
Squires J. ASQ-3 user’s guide. Baltimore: Paul H. Brookes Pub.; 2009.
Romeo DM, Di Stefano A, Conversano M, Ricci D, Mazzone D, Romeo MG, et al. Neurodevelopmental outcome at 12 and 18 months in late preterm infants. Eur J Paediatr Neurol. 2010;14(6):503–7.
Robinson MD, McCarthy DJ, Smyth GK. edgeR: a Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics. 2010;26(1):139–40.
Krebs CE, Ori APS, Vreeker A, Wu T, Cantor RM, Boks MPM, et al. Whole blood transcriptome analysis in bipolar disorder reveals strong lithium effect. Psychol Med. 2020;50(15):2575–86.
Mendez EF, Wei H, Hu R, Stertz L, Fries GR, Wu X, et al. Angiogenic gene networks are dysregulated in opioid use disorder: evidence from multi-omics and imaging of postmortem human brain. Mol Psychiatry. 2021;26(12):7803–12.
Ohguro H, Ida Y, Hikage F, Umetsu A, Ichioka H, Watanabe M, et al. STAT3 is the master regulator for the forming of 3D spheroids of 3T3-L1 preadipocytes. Cells. 2022;11(2):300.
Raudvere U, Kolberg L, Kuzmin I, Arak T, Adler P, Peterson H, et al. g:Profiler: a web server for functional enrichment analysis and conversions of gene lists (2019 update). Nucleic Acids Res. 2019;47(W1):W191–w198.
Baier CJ, Katunar MR, Adrover E, Pallares ME, Antonelli MC. Gestational restraint stress and the developing dopaminergic system: an overview. Neurotox Res. 2012;22(1):16–32.
Bonnin A, Goeden N, Chen K, Wilson ML, King J, Shih JC, et al. A transient placental source of serotonin for the fetal forebrain. Nature. 2011;472(7343):347–50.
Bonnin A, Levitt P. Fetal, maternal, and placental sources of serotonin and new implications for developmental programming of the brain. Neuroscience. 2011;197:1–7.
Muller CL, Anacker AM, Rogers TD, Goeden N, Keller EH, Forsberg CG, et al. Impact of maternal serotonin transporter genotype on placental serotonin, fetal forebrain serotonin, and neurodevelopment. Neuropsychopharmacology. 2017;42(2):427–36.
Cheong JL, Doyle LW, Burnett AC, Lee KJ, Walsh JM, Potter CR, et al. Association between moderate and late preterm birth and neurodevelopment and social-emotional development at age 2 years. JAMA Pediatr. 2017;171(4):e164805.
Zhou H, Qu X, Yang Y, Kc A, Liu X, Yang C, et al. Relationship between moderate to late preterm, diet types and developmental delay in less-developed rural China. Nutr Neurosci. 2022;25(1):70–9.
Vacher CM, Lacaille H, O’Reilly JJ, Salzbank J, Bakalar D, Sebaoui S, et al. Placental endocrine function shapes cerebellar development and social behavior. Nat Neurosci. 2021;24(10):1392–401.
Rosenfeld CS. Sex-specific placental responses in fetal development. Endocrinology. 2015;156(10):3422–34.
Hanswijk SI, Spoelder M, Shan L, Verheij MMM, Muilwijk OG, Li W, et al. Gestational factors throughout fetal neurodevelopment: the serotonin link. Int J Mol Sci. 2020;21(16):5850.
Areal LB, Blakely RD. Neurobehavioral changes arising from early life dopamine signaling perturbations. Neurochem Int. 2020;137:104747.
Benavides A, Bell EF, Georgieff MK, Josephson CD, Stowell SR, Feldman HA, et al. Sex-specific cytokine responses and neurocognitive outcome after blood transfusions in preterm infants. Pediatr Res. 2022;91(4):947–54.
Tottman AC, Bloomfield FH, Cormack BE, Harding JE, Taylor J, Alsweiler JM. Sex-specific relationships between early nutrition and neurodevelopment in preterm infants. Pediatr Res. 2020;87(5):872–8.
Zozaya C, Avila-Alvarez A, Arruza L, García-Muñoz Rodrigo F, Fernandez-Perez C, Castro A, et al. The effect of morbidity and sex on postnatal growth of very preterm infants: a multicenter cohort study. Neonatology. 2019;115(4):348–54.
Frondas-Chauty A, Simon L, Branger B, Gascoin G, Flamant C, Ancel PY, et al. Early growth and neurodevelopmental outcome in very preterm infants: impact of gender. Arch Dis Child Fetal Neonatal Ed. 2014;99(5):F366–372.
El Rafei R, Jarreau PH, Norman M, Maier RF, Barros H, Van Reempts P, et al. Association between postnatal growth and neurodevelopmental impairment by sex at 2 years of corrected age in a multi-national cohort of very preterm children. Clin Nutr. 2021;40(8):4948–55.
Fernández-Calle R, Konings SC, Frontiñán-Rubio J, García-Revilla J, Camprubí-Ferrer L, Svensson M, et al. APOE in the bullseye of neurodegenerative diseases: impact of the APOE genotype in Alzheimer’s disease pathology and brain diseases. Mol Neurodegener. 2022;17(1):62.
Martens YA, Zhao N, Liu CC, Kanekiyo T, Yang AJ, Goate AM, et al. ApoE Cascade Hypothesis in the pathogenesis of Alzheimer’s disease and related dementias. Neuron. 2022;110(8):1304–17.
Lien E, Andersen GL, Bao Y, Gordish-Dressman H, Skranes JS, Vik T, et al. Apolipoprotein E polymorphisms and severity of cerebral palsy: a cross-sectional study in 255 children in Norway. Dev Med Child Neurol. 2013;55(4):372–7.
Schmithorst VJ, Panigrahy A, Gaynor JW, Watson CG, Lee V, Bellinger DC, et al. Organizational topology of brain and its relationship to ADHD in adolescents with d-transposition of the great arteries. Brain Behav. 2016;6(8):e00504.
Wright RO, Hu H, Silverman EK, Tsaih SW, Schwartz J, Bellinger D, et al. Apolipoprotein E genotype predicts 24-month bayley scales infant development score. Pediatr Res. 2003;54(6):819–25.
Hashikawa-Hobara N, Hashikawa N, Yutani C, Zamami Y, Jin X, Takatori S, et al. The Akt-nitric oxide-cGMP pathway contributes to nerve growth factor-mediated neurite outgrowth in apolipoprotein E knockout mice. J Pharmacol Exp Ther. 2011;338(2):694–700.
Dowling O, Chatterjee PK, Gupta M, Tam Tam HB, Xue X, Lewis D, et al. Magnesium sulfate reduces bacterial LPS-induced inflammation at the maternal-fetal interface. Placenta. 2012;33(5):392–8.
Palinski W. Maternal-fetal cholesterol transport in the placenta: good, bad, and target for modulation. Circ Res. 2009;104(5):569–71.
Kitagawa K, Matsumoto M, Kuwabara K, Takasawa K, Tanaka S, Sasaki T, et al. Protective effect of apolipoprotein E against ischemic neuronal injury is mediated through antioxidant action. J Neurosci Res. 2002;68(2):226–32.
Yan W, Yue H, Ji X, Li G, Sang N. Prenatal NO(2) exposure and neurodevelopmental disorders in offspring mice: transcriptomics reveals sex-dependent changes in cerebral gene expression. Environ Int. 2020;138:105659.
Mi W, Jung SS, Yu H, Schmidt SD, Nixon RA, Mathews PM, et al. Complexes of amyloid-beta and cystatin C in the human central nervous system. J Alzheimers Dis. 2009;18(2):273–80.
Wang B, Xie YC, Yang Z, Peng D, Wang J, Zhou S, et al. Lack of an association between Alzheimer’s disease and the cystatin C (CST3) gene G73A polymorphism in Mainland Chinese. Dement Geriatr Cogn Disord. 2008;25(5):461–4.
Hoghooghi V, Palmer AL, Frederick A, Jiang Y, Merkens JE, Balakrishnan A, et al. Cystatin C plays a sex-dependent detrimental role in experimental autoimmune encephalomyelitis. Cell Rep. 2020;33(1):108236.
Cole T, Dickson PW, Esnard F, Averill S, Risbridger GP, Gauthier F, et al. The cDNA structure and expression analysis of the genes for the cysteine proteinase inhibitor cystatin C and for beta 2-microglobulin in rat brain. Eur J Biochem. 1989;186(1–2):35–42.
Bernstein HG, Järvinen M, Pöllänen R, Schirpe H, Knöfel B, Rinne R. Cystatin C containing neurons in human postmortem hypothalamus. Neurosci Lett. 1988;88(2):131–4.
Song G, Spencer TE, Bazer FW. Progesterone and interferon-tau regulate cystatin C in the endometrium. Endocrinology. 2006;147(7):3478–83.
Xu L, Sheng J, Tang Z, Wu X, Yu Y, Guo H, et al. Cystatin C prevents degeneration of rat nigral dopaminergic neurons: in vitro and in vivo studies. Neurobiol Dis. 2005;18(1):152–65.
Rukova B, Staneva R, Hadjidekova S, Stamenov G, Milanova V, Toncheva D. Whole genome methylation analyses of schizophrenia patients before and after treatment. Biotechnol Biotechnol Equip. 2014;28(3):518–24.
Schmidt MJ, Mirnics K. Neurodevelopment, GABA system dysfunction, and schizophrenia. Neuropsychopharmacology. 2015;40(1):190–206.
Nagai A, Terashima M, Sheikh AM, Notsu Y, Shimode K, Yamaguchi S, et al. Involvement of cystatin C in pathophysiology of CNS diseases. Front Biosci. 2008;13:3470–9.
Olsson T, Nygren J, Håkansson K, Lundblad C, Grubb A, Smith ML, et al. Gene deletion of cystatin C aggravates brain damage following focal ischemia but mitigates the neuronal injury after global ischemia in the mouse. Neuroscience. 2004;128(1):65–71.
Hardy S, Haisley L, Manning C, Fein D. Can screening with the ages and stages questionnaire detect autism? J Dev Behav Pediatr. 2015;36(7):536–43.
Burton GJ, Jauniaux E. What is the placenta? Am J Obstet Gynecol. 2015;213(4 Suppl):S6.e1, S6-8.
Burton GJ, Jauniaux E. Pathophysiology of placental-derived fetal growth restriction. Am J Obstet Gynecol. 2018;218(2s):S745–s761.
Hemberger M, Hanna CW, Dean W. Mechanisms of early placental development in mouse and humans. Nat Rev Genet. 2020;21(1):27–43.
Acknowledgements
We thank all participants of the Ma’anshan birth cohort and those who contributed to the cohort follow-up efforts.
Funding
This work was supported by the National Natural Science Foundation of China (82103870), Key Project of Translational Medicine Research Institute of Anhui Province (2022zhyx-B06), Natural Science Foundation of Anhui Province (2108085QH360), and Regional Innovation and Development Joint Fund of the National Natural Science Foundation of China (U22A20361).
Author information
Authors and Affiliations
Contributions
YZ1, FT, and QW designed the project; YZ1, YZ2, and YJ analyzed the data; YZ2 and HJ carried out the experiment; CR, JL, and XW helped with the experiments; YZ1 and YZ2 wrote the manuscript; YZ1, YZ2, FT, and QW reviewed and edited the manuscript; KH, JT, HG, and FT contributed to the collection of the clinical samples and clinical data. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Anhui Medical University (No. 20131195). The samples collected during the study come from the relevant studies where written informed consent was received.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Primers for the RT-qPCR. Table S2. Results of generalized estimating equations models between MLPT and ASQ. Table S3. Results of multiple testing correction of logistic regression between MLPT and ASQ. Table S4. RNA-seq data statistical summary. Table S5. List of differential expression genes. Table S6. PBA genes. Table S7. PBA pathway genes. Table S8. PBA related genes for experimental validation in CNBC cohort. Table S9. Neurodevelopmental delays prediction and model development.
Additional file 2:
Figure S1. GO functional annotation clustering analysis of PBA related genes from manual collection. Figure S2. Validation of the main PBA related genes in placenta samples from CNBC study. Figure S3. Validation of the main PBA related genes in MLPT placenta samples from MABC study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhu, Y., Zhang, Y., Jin, Y. et al. Identification and prediction model of placenta-brain axis genes associated with neurodevelopmental delay in moderate and late preterm children. BMC Med 21, 326 (2023). https://doi.org/10.1186/s12916-023-03023-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-023-03023-1