
Abstract
Background
Healthcare systems around the world are facing large challenges. There are increasing demands and costs while at the same time a diminishing health workforce. Without reform, healthcare systems are unsustainable. Relocating care, for example, from hospitals to sites closer to patients’ homes, is expected to make a key contribution to keeping healthcare sustainable. Given the significant impact of this initiative on citizens, we conducted a scoping review to provide insight into the factors that influence citizens’ attitudes towards relocating care.
Method
A scoping review was conducted. The search was performed in the following databases: Pubmed, Embase, Cinahl, and Scopus. Articles had to include relocating healthcare and citizens’ perspectives on this topic and the articles had to be about a European country with a strong primary care system. After applying the inclusion and exclusion criteria, 70 articles remained.
Results
Factors positively influencing citizens’ attitudes towards relocating care included: convenience, familiarity, accessibility, patients having more control over their disease, and privacy. Factors influencing negative attitudes included: concerns about the quality of care, familiarity, the lack of physical examination, contact with others, convenience, and privacy. Furthermore, in general, most citizens preferred to relocate care in the studies we found, especially from the hospital to care provided at home.
Conclusion
Several factors influencing the attitude of citizens towards relocating care were found. These factors are very important when determining citizens’ preferences for the location of their healthcare. The majority of studies in this review reported that citizens are in favour of relocating care. In general citizens’ perspectives on relocating care are very often missing in articles. It was significant that very few studies on relocation from the hospital to the general practitioner were identified.
Similar content being viewed by others

Introduction
Demand for healthcare is increasing across the world due to a number of developments including populations ageing, technical advances in medical care, and rising incomes [1,2,3]. With an increase in demand, costs will also rise, while at the same time a diminishing health workforce. [1,2,3,4,5]. Consequently, reforms within the healthcare system will be necessary in order to control increasing healthcare costs and staff shortages [1,2,3]. It is assumed that reforming healthcare systems with a view to making better use of resources will make a key contribution to keeping healthcare sustainable. Estimates suggest that one fifth of health spending could be channelled towards better use, thus improving healthcare efficiency [6]. Increased efficiency could be accomplished in several ways. These may include: reducing the number of patients who receive low-value or unnecessary care; providing the same care with fewer resources, for instance by providing care in more cost-effective settings rather than in hospitals; or by reducing administrative processes that add no value [6]. This article focuses on providing care with fewer resources by relocating it to more cost-effective settings. This, in the first instance, would mean from secondary care to primary care. The thought behind this is that general practitioners (GPs) can generally provide care at less expense than hospitals for certain procedures that do not need hospital staff or environment [6]. These may include minor interventions, such as the placement of an intra-uterine device (IUD), or follow-up care, such as yearly blood- and ultrasounds, for patients who have been treated for cancer[6,7,8,9]. Relocating care to control costs could also include relocating care from secondary to homecare, self-care or eHealth [10]. Delivering care digitally can prevent a patient from having to go to the hospital. For example, an app could be used to monitor a patient receiving oxygen at home. Care commonly provided by the GP could also be relocated, to self-care, eHealth or to other healthcare providers (HCPs), like a physiotherapist or dietitian. This could result in more time for the GP to take on other secondary or primary care tasks.
It is important for relocating care to succeed, to get insights into the perspectives and needs of healthcare providers and citizens. Although involving citizens is a very important aspect of policy-making processes, it is an often overlooked form of evidence according to the World Health Organization (WHO) [11]. Citizen engagement will strengthen societal trust, will lead to more effective public policies and will lead to an improved quality of care. Furthermore, citizen engagement is essential because healthcare systems are transitioning towards a patient-centered approach, where citizens' perspectives on quality are inherently meaningful and should be a primary focus within healthcare systems [12].Extensive research has already been undertaken regarding the perspective of healthcare providers [9, 13,14,15,16], the quality and outcomes of care [17,18,19,20] and the cost perspectives [10, 17, 18, 20, 21], but not regarding the citizens' perspective on relocating care. To our knowledge, a review about citizens’ perspectives on relocating care does not exist yet. We have, therefore, conducted a scoping review with the goal of describing the findings and range of research concerning citizens’ perspectives on relocating care in more detail. A strong primary care system is required to make relocating care possible [6]. We, therefore, searched for studies that were undertaken in countries in Europe with a strong primary care [22]. Table 1 describes the characteristics of countries with strong primary care. The research questions answered in this review are: (1) Which factors influence citizens’ attitudes towards relocating care? (2) What are citizens’ preferences towards the location of care?
Method
The aim of this review is to understand citizens’ attitudes and preferences towards relocating care. As this topic is quite broad and may be studied using many different study designs, and considering that we are not aware of any prior synthesis on this topic, a scoping review rather than a systematic review was conducted. This scoping review was carried out on the basis of the guideline by Arksey and O’Malley [23]. The review includes the following key phases: 1) identifying the research question; 2) identifying relevant studies; 3) study selection; 4) charting the data, and; 5) collating, summarising, and reporting the results.
The search strategy and selection of literature
An initial broad search of the literature was undertaken by the first author in order to identify relevant articles that could be used for designing a search strategy. During this search, 18 key articles were identified, which included citizens, preference, and relocating care, these three terms formed the basis of our search strategy. A qualified medical information specialist was consulted in order to design and execute a sensitive search strategy. The medical information specialist also advised on which databases were most likely to contain the type of studies we were seeking and thus constituted an initial search strategy. This was refined several times after consultation. The final version was first used on the Pubmed database and then converted for each of these subsequent databases, Embase, Cinahl, and Scopus. The final search strategy, shown in Appendix A, was able to find 16 out of the 18 key articles identified. In total, it identified 19.587 articles. Duplicate references were removed, leaving 11.080 unique references. The most recent search was executed on 5 July 2022.
The selection process was performed by all authors. First, inclusion and exclusion criteria were developed. There were several inclusion criteria for this scoping review. The topic of the articles had to be citizens’ perspectives on relocating care. Only articles related to European countries with strong primary care systems were included, as a strong primary care system is required to make relocating care possible [6]. These countries were: the Netherlands, the United Kingdom, Belgium, Spain, Portugal, Finland, Estonia, Lithuania, Denmark, and Slovenia [22]. Only articles written in English, Dutch, or German were included as these were languages sufficiently mastered by the authors. In addition, all study designs were included. An overview of inclusion and exclusion criteria are shown in Table 2. In order to calibrate the inclusion process, the researchers independently applied the inclusion and exclusion criteria to a selection of three hundred articles. The task was to include, or exclude, articles based on the title alone. The results were discussed by the researchers to see if there was a maximum margin of disagreement up to 10%. This percentage was agreed in advance by the researchers. During this process, the inclusion and exclusion criteria were further refined (See Table 2). As disagreement remained, a second round of calibration was performed on 50 articles, including both titles and abstracts. The disagreement rate was now only 4% and therefore all the remaining articles were distributed among the reviewers to be scored, based on the title and abstract. After screening on the title and abstract, 167 references remained and two key articles that were not found with the search were added. These articles were distributed among the researchers once more in order to read the full text. While reading the full texts, another three relevant articles were identified through the references. These were then added too. This resulted in a total of 172 full text articles. Results from included articles were charted in a spreadsheet, which was tested by the researchers before using it. When one of the reviewers had doubts about an article, it was read by a second reviewer and the outcomes were discussed until the two researchers came to an agreement.
Data extraction
A spreadsheet was created to categorise the information that contributed to answering the research questions.
The information extracted from the articles was structured according to the type of relocation, including: relocating from the hospital to the GP, to care at home, to self-care, or to eHealth, and relocating from the GP to self-care, to care at home, or to eHealth. The difference between self-care and care at home is that self-care does not involve a healthcare provider, unlike care at home. Both forms of relocating do not involve eHealth. When the article was about eHealth it was catalogued with the eHealth category. Articles that remained, of which there was only one, were placed within the category ‘other’.
The information extracted included factors that determined citizens’ attitudes towards relocating care. All of these factors were coded by highlighter and categorised. The categories were discussed within the research team. Subsequently, we made a top three of factors for each form of relocation that occurred most often.
Furthermore, we extracted information regarding preferences for healthcare location in the articles. Citizens could have a preference for either keeping care its current location, relocating care, or a combination of both, suggesting that citizens may prefer a hybrid approach where some aspects of healthcare are relocated, while others remain in their current location. Citizens could also express equal preferences for both locations. In addition, we compared the outcomes of the one-armed, the two-armed, and the hypothetical studies, to see if there were major differences, in the preferences for healthcare location, resulting from their methodological approaches. In the one-armed studies, care was relocated for all participants in the study [24]. In the two-armed studies there was one group of participants where care was relocated, but also one group who received care as usual. The outcomes of the two groups were then compared. Hypothetical studies, presented scenarios without actual choices. They asked citizens how they would feel if care were relocated. Two-armed studies are generally considered of higher quality than one-armed and hypothetical studies, due to the presence of both an experimental group and a control group, which increases their internal validity [25].
Results
Search flow
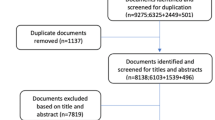
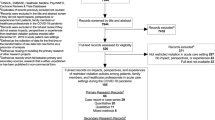
A total of 19,587 references were identified from the databases, of which 8,507 were duplicates, as shown in Fig. 1. At the end of the selection process, 70 full text articles were included. The characteristics of these studies are shown in Table 3.

Flowchart of the review process
The majority of studies of citizens’ perspectives on relocating care took place in the UK (N = 44), followed by the Netherlands (N = 13), and Denmark (N = 11). One study is from Spain and one from Estonia. Most studies are one-armed (N = 42), followed by two-armed (n = 19), and nine studies were hypothetical. While eight studies are from 2013, most studies were published quite recently in 2019 (N = 7), 2020 (N = 6), 2021 (N = 16), and 2022 (N = 9). Relocating care from the hospital to eHealth is the form of relocating that is most often examined within the studies identified (N = 28) [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53]. This is followed by relocating from the hospital to self-care (N = 15) [54,55,56,57,58,59,60,61,62,63,64,65,66,67] and care at home (N = 13) [30, 68,69,70,71,72,73,74,75,76,77,78,79,80]. Forms of relocating care that are not frequently studied include relocating from the hospital to the GP (N = 7) [16, 69, 81,82,83,84,85] and from the GP to self-care (N = 4) [86,87,88,89]. Five more forms of relocating are listed under the heading “other”. These include: relocating from the hospital to a community-based clinic [90]; from outpatient visits to a one-stop clinic [91]; nurse home visits that were replaced by eHealth [92]; hospital care relocated to a mobile chemotherapy unit [93]; and, care relocated from the GP to eHealth [94]. Most studies are about the relocation of care for oncology patients (N = 19), followed by citizens in general (N = 10), and cardiology patients (N = 8).
Which factors influence citizens’ attitudes towards relocating care?
Convenience
The most frequently cited factors influencing citizens’ attitudes towards relocating care are shown in Table 4. Convenience was most often reported, from the citizens’ perspective, as an advantage of relocating care. This was true for all forms of relocation [27,28,29,30, 32,33,34, 38, 41, 42, 45, 47, 49, 52,53,54, 58,59,60, 65,66,67, 69, 70, 73, 78, 82, 84,85,86, 88, 90, 93, 94]. Citizens think of relocating as convenient because in most cases it saves travel time [26, 29, 53]. It saves costs [26, 69]. It avoids stress due to factors such as transport problems, busy traffic, travelling while you are sick, or long sojourns in waiting rooms [26, 53, 73, 93]. When relocating to self-care it was very often mentioned that it is an advantage to have more flexibility [30, 86]. Citizens can do a self-test whenever and wherever they want, without having to consider opening hours, for example [59, 66, 67]. Convenience was also mentioned as a reason for not wanting to relocate care. This factor was especially mentioned when relocating from the hospital or GP to self-care [59, 60, 86]. With regard to home dialysis, some citizens said that they did not have the space at home to do this. It was, therefore, not convenient [60]. In addition, for citizens living close to the hospital, self-care was sometimes more expensive and did not save time [59, 86].
Familiarity
Familiarity was another factor which was reported as important to citizens regarding their attitude towards relocating care [29,30,31,32,33, 58, 61, 67,68,69,70, 73, 74, 77, 83,84,85,86, 90, 94]. Some citizens feel more familiar with their GP than with a hospital specialist and would, therefore, want to relocate care [83, 84]. Other citizens experience a sense of familiarity due to the environment in which care is provided. When receiving care at home, citizens feel more familiar, because they are in their own environment with their own support system [29, 30, 50, 58, 70, 77]. In addition, when receiving care at home, the HCP enters the personal space of the patient. This, according to some of the patients, provided a better and more personal connection with the HCP. As shown in Table 4, familiarity is also named as a reason not to want to relocate. While some citizens said that they had a better relationship with their GP, others said they were more familiar with the specialist so they would rather go there [85]. Some citizens thought that personal contact was reduced when using eHealth. They felt that it was more distant [31, 33, 36, 47, 51]. In addition, during telephone consultations, citizens did not feel a sense of familiarity if they had never seen the HCP before and therefore could not picture the face belonging to the voice. [29]. With regard to self-care, some citizens did not feel a sense of familiarity because this care is usually performed alone, while they preferred to have the support of a HCP [60, 63].
Accessibility
The third most frequently mentioned factor that influenced citizens’ perceptions of relocating care was “accessibility”. Citizens were more willing to relocate care when waiting times became shorter and so the accessibility became better [28,29,30, 45, 49, 54, 58, 82,83,84, 88, 90, 91, 93]. For example when relocating from the hospital to the GP [82,83,84]. Regarding self-tests, citizens mentioned that they had very rapid access. They can pick up the test and then apply it directly, without having to make an appointment with a HCP, who is often not immediately available [30, 54, 55, 58]. In addition, with a self-test you often get the results without delay [55, 59]. With regard to eHealth, citizens said that access to the HCP improved because they could contact them easily when they had questions [28, 49].
Patients have more control
Another advantage of relocating care, mentioned by citizens, is being more in control, especially when relocating care from the hospital to eHealth, self-care, or to care at home [30, 54, 58, 60, 70, 73]. The sense of increased control can stem from two primary factors. Firstly, patients become more actively engaged in their healthcare, leading to a better understanding of their diagnoses and consequently, greater control over their condition [38, 49, 53, 59, 86]. Secondly, citizens felt more involved in the process of decision making regarding their healthcare, affording them the ability to influence what happens and when [49, 50, 59, 74]. This gives them the feeling of having more control over their lives.
Privacy
The last factor named as an advantage, but also as a disadvantage of relocating care, is ‘privacy’. Citizens who saw it as an advantage mentioned that there is more privacy at home using eHealth or self-care than there is in a hospital [53,54,55, 58, 60, 66, 69, 70, 74]. With regard to self-care there are a lot of articles about using self-tests to check for sexually transmitted infections or about administering drugs oneself at home in order to induce an abortion. Citizens indicated that having such tests carried out at a clinic may cause a lot of embarrassment [54]. You may run into acquaintances for example [67]. Self-care, on the other hand, is more anonymous and thus offers more privacy [55]. However, privacy is also named as an disadvantage by citizens. Regarding eHealth, some citizens are concerned about whether the privacy of their data can be guaranteed [33]. In addition, some citizens said that it was hard to find a private space in their house during the covid-19 crisis [30]. Furthermore, when care is being given at home, some citizens do not like the fact that other family members may witness them being treated [69] or that caregivers are having to enter their home, thus violating their privacy [70].
Quality of care
The most frequently mentioned factor for having a negative attitude towards relocating care is that citizens have concerns about the quality of care when care is being relocated, due to less expertise of the HCP or insufficient quality of the instrument or self-test, which will be involved in the new location [28, 32,33,34, 36, 47, 51, 54, 55, 59, 60, 63, 65, 67, 69, 70, 73, 77, 82, 85,86,87, 90, 94]. Regarding relocating care to eHealth or self-care a lack of trust in eHealth technology [33, 34, 36, 47], or a particular self-care device, [54, 55, 59, 60, 63, 65, 67] was reported very often. Citizens fear technical problems or that important factors might be overlooked. Neither do some citizens feel that they have the right skills for using the new eHealth technology [36] or performing self-care in the right way [54, 60, 65, 67]. Regarding care at home, citizens were concerned with the absence of constant surveillance and a diminished contact with the doctor. Moreover, citizens felt that the hospital is better equipped [77]. With regard to relocating from the hospital to the GP, some citizens thought that the specialist had more expertise which was a reason for them not wanting to relocate [82, 85].
No physical examination
Another factor for not wanting to relocate care is where it results in an absence of physical examination. This reason was named many times when relocating care from the hospital to eHealth [27, 29, 31, 34, 47, 51, 52] and relocating from the GP to self-care [86, 89]. With regard to eHealth, some citizens say that they found it difficult because they are not able to demonstrate physical symptoms and they find it hard to describe problems without seeing the HCP [31, 33].
Contact with others
The last factor, frequently mentioned as a disadvantage of relocating care, is less contact with their peers. This aspect was most mentioned regarding relocating from the hospital to care at home [69, 70, 73]. Some citizens enjoyed going to the hospital because of the social interaction with other citizens. They were afraid of social isolation [60].
What are citizens’ preferences regarding the location of care?
A total of 49 articles investigated citizens’ preferences regarding the location of healthcare. Their location preferences for each form of relocating care will be discussed below and are shown in Table 5.
Within the articles about relocating from the hospital to eHealth, 23 articles out of 28 provided the preferences of respondents towards the location of care. In ten articles there was a preference for eHealth [28, 32,33,34, 42, 44,45,46, 50, 53] and in six articles a preference for the hospital [26, 31, 36, 39, 43, 48]. In four articles, citizens expressed a wish for a combination of eHealth and face to face contact [37, 47, 49, 52]. In the remaining articles (N = 3), the preference was equal for the hospital and for eHealth [35, 41, 51].
Eight out of 15 articles about relocating from the hospital to self-care investigated citizens preferences for the location of care. In five articles citizens showed a preference for self-care [56, 57, 61, 64, 66] and in three articles for the hospital [55, 60, 65].
With regard to articles about relocating from the hospital to care at home, ten out of 13 articles investigated a preference for healthcare location. In eight articles, the participants had a preference for care at home [68, 69, 72, 74, 75, 78,79,80]. In two articles, preferences for care at home and the hospital were equal [71, 76]. There were no articles with a preference for the hospital.
Regarding relocating from the hospital to the GP, there were five out of seven articles investigating citizens preferences regarding healthcare location. In two articles, participants preferred the hospital over the GP [81, 85]. In one they preferred the GP [84], and in the other, preferences were equal [16]. In the fifth study citizens could choose between three locations: the hospital, the GP, or care at Home. Here they preferred care at home followed by care at the general practice [69].
Two out of four articles about relocating from the GP to self-care investigated a preference for a healthcare location. In one article, citizens preferred self-care [86], and in the other, they preferred the GP [89].
Within the category “other”, there were two articles which investigated a preference for a healthcare location. In the article about relocating from the hospital to one-and-a-half line care, citizens preferred one-and-a-half line care [91]. The last article was about nurse home visits that were relocated to eHealth. Here, citizens preferred eHealth over the nurse visits [93].
Most articles adopted a one-armed approach. Since two-armed articles are often of higher quality, we compared the results of the one-armed, and the two-armed, articles. In total there were 19 two-armed articles of which 14 investigated a preference for healthcare location. In nine out of 14 articles citizens preferred relocating healthcare and in two articles they did not. In the other articles, preferences were equal. Of the 35 one-armed articles which investigated healthcare preferences in 18 articles, citizens gave a preference for relocating healthcare. Thus, in both cases, there is a preference for relocating care in just over half of the articles. We see here a different outcome than with the hypothetical studies (N = 10). Here there was no preference for relocating care in five out of seven articles.
Discussion
This scoping review was conducted in order to provide insight into the factors that influence citizens attitudes towards relocating care. Seventy articles were included and most which were found were about relocating care from the hospital to eHealth. Most of these articles about eHealth were published in 2020 or later (N = 20). Only eight articles were published in 2019 or earlier. This is likely due to covid-19, which started in 2020 in Europe and required healthcare providers in many places to offer care online.
The first research question concerned which factors influence citizens attitudes towards relocating care. The most frequent reported factor for a positive attitude towards relocating care is “convenience”, according to citizens, followed by “familiarity”. Other factors that were in the top three of reasons for a positive attitude towards relocating care were “accessibility”, “patients have more control”, and “privacy”. The positive drivers for relocating care are almost the same for all forms of relocating. The two most mentioned factors for a negative attitude towards relocating care are, first of all, citizens having concerns about the quality of care and, secondly, citizens feel less familiar when care is being relocated. Other reasons to have a negative attitude towards relocating are “the lack of physical examination”, “contact with others”, “convenience”, and “privacy”.
The second research question concerned citizens’ preferences for healthcare location. In general, as far as the conditions and treatments mentioned in the articles are concerned, most citizens favoured relocating healthcare. Especially with regard to care at home, there were no articles found where citizens had a preference for the hospital instead of care at home. In addition, eHealth and self-care are also carried out from home. Citizens thus prefer receiving care at home.
Not all articles investigated preferences for the location of healthcare, and of those which did, most were one-armed. However, there were no major differences found when comparing the outcomes of the one-armed and two-armed studies. This contrasted with the hypothetical studies, where citizens did not prefer relocating care in the majority of cases. This may be due to the fact that citizens are familiar with the current situation and do not know, or find it difficult to imagine, what a new situation will look like. Citizens may not want to relocate because familiarity is an important aspect of healthcare, as described earlier.
The articles found included a wide variety of conditions and phases of treatment. We would have preferred to distinguish between different conditions and treatment phases, as these aspects may determine the preference for healthcare location. For example, it might be the case that citizens would like to relocate follow-up cancer care to care at home, while keeping the treatment itself in the hospital. However, the large variation in conditions and phases of treatment resulted in a small N per condition or phase of treatment and this hampered further in-depth analysis.
Relocating care often involves not only the location changing, but also other aspects. For instance, the care provider may change too, for example a telephone consultation with a nurse instead of a face to face appointment with the specialist in the hospital [32, 53]. And in some cases, the purpose of treatment changed, for example, a telephone consultation that was meant for providing information and supporting patients, while a face to face consultation was more focused on looking for signs of recurrent disease [29]. All of these factors together determine the preference for healthcare location. So it is not only the location on which citizens base their preference. It is, therefore, important to take all aspects into account, not only the geography when investigating the preferences for healthcare location.
Strengths and limitations
A strength of this scoping review is that it has a broad search strategy developed together with a medical information specialist. This resulted in over 11.000 references that were all assessed. However, the search strategy may not have been broad enough, as some articles were missed, including two of the 18 key articles. This was known beforehand and so we investigated why the two key articles were not found. One key article was not found because we did not use the word “experience” [16] while the other focused on the terms “breast cancer”, “follow-up care”, and “healthcare models” [81], which we did not use in our search strategy. The words used in these two articles were not words we saw repeated in other relevant articles. Adding any of the key words yielded about 5,800 additional results in Pubmed alone. Therefore, we chose to add the key articles manually and left these words out of the search string. All statements made in this article are based on the conditions and forms of care that recurred in the studies we found. There may be other forms of care that could be relocated that have not been discussed in this article.
Another limitation of this study is that the articles are not double reviewed because of the large number of references found. However, to calibrate the inclusion process, the researchers applied the inclusion and exclusion criteria to a selection of 350 articles. Also, it was decided to start with reviewing abstracts, instead of titles, which is the normal procedure [23].
A limitation of a scoping review is that it analyses studies that use a range of data collection and techniques. This makes it more difficult to synthesise the results of the studies [23]. A strong point of this review is that we made a comparison between one-armed and two-armed articles and that approximately the same results emerged in the articles.
Research implications
A knowledge gap we identified is that citizens’ perspectives on relocating care received relatively little attention within the current literature. In particular, we found limited literature focusing on citizens’ perspectives regarding the relocation of care from the hospital to the GP. This gap is significant, because this is one of the forms of relocating that governments think of first in order to limit healthcare costs [6,7,8]. There are several studies about this subject but they do not involve the citizens’ perspective. Despite the importance of including citizens' perspectives in policy-making processes, it often remains underrepresented in the literature [11]. The World Health Organization (WHO) emphasizes that citizen engagement can enhance societal trust and lead to more effective public policies.
Another knowledge gap we identified is that insufficient research has been done on different treatment phases and conditions in healthcare with regard to citizens’ perspectives and relocating care. To fill this gap, future research should delve deeper into the relationship between the factors leading to particular attitudes towards relocating care, and preferences for location of care and different conditions and treatment phases, including diagnosis, treatment phase and aftercare.
Our study has also revealed practical implications that can inform healthcare policy and decision-making. Firstly, the factors we have identified can serve as conditions that governments can use to improve acceptance among citizens regarding healthcare location. They can be used as conditions that have to be met, and that can be used to direct citizens to a particular location. Secondly, it's evident from our findings that citizens generally prefer receiving care from home. This preference presents an opportunity for governments to invest in home-based healthcare services, potentially leading to higher citizen satisfaction and more cost-effective healthcare delivery.
Conclusion
Positive factors influencing the attitude of citizens towards relocating care are almost the same for all forms of this development—with convenience as the most important. The most often reported factor for having a negative attitude towards relocating care are concerns about the quality of care. The factors found are very important when determining a citizens’ preference for a particular healthcare location. The majority of studies in this review reported that citizens are in favour of relocating care, especially to care at home. Several knowledge gaps were identified. Strikingly, very few studies on relocation from the hospital to the GP were identified.
Availability of data and materials
Not applicable. The studies we used are accessible to everyone. All studies used are included in the references.
Abbreviations
- GP:
-
General practitioner
- HCP:
-
Healthcare provider
- IUD:
-
Intra-uterine device
References
Organisation for Economic Co-operation and Development. OECD work on health. Paris: OECD; 2021. p. 1–44.
Rechel B, Doyle Y, Grundy E, McKee M. How can health systems respond to population ageing? Technical report. Copenhagen: World Health Organization; 2009. Report No.: 10.
Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11.
Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global health workforce labor market projections for 2030. Hum Resour Health. 2017;15(1):11.
Boniol M, Kunjumen T, Nair TS, Siyam A, Campbell J, Diallo K. The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage? BMJ Glob Health. 2022;7(6):e009316.
Organisation for Economic Co-operation and Development. Tackling wasteful spending on Health. Paris: OECD; 2017.
Taskforce De Juiste Zorg Op de Juiste Plek. De Juiste zorg op de juiste plek rapport: Wie durft? Den Haag: Ministerie van Volksgezondheid, Welzijn en Sport; 2018.
Sibbald B, McDonald R, Roland M. Shifting care from hospitals to the community: a review of the evidence on quality and efficiency. J Health Serv Res Policy. 2007;12(2):110–7.
Liemburg GB, Korevaar JC, van Zomeren WT, Berendsen AJ, Brandenbarg D. Follow-up of curatively treated cancer in primary care: a qualitative study of the views of Dutch GPs. Br J Gen Pract. 2022;72(721):e592–600.
Gupta Strategists. No place like home. An analysis of the growing movement away from hospitals towards providing medical care to patients in their own homes. Amsterdam: Gutpa Strategists; 2016.
World Health Organization. Implementing citizen engagement within evidence-informed policy-making: an overview of purpose and methods. Geneva: World Health Organization; 2022.
Sofaer S, Firminger K. Patient perceptions of the quality of health services. Annu Rev Public Health. 2005;26:513–59.
Van Hoof SJM, Kroese MEAL, Spreeuwenberg MD, Elissen AMJ, Meerlo RJ, Hanraets MMH, et al. Substitution of hospital care with primary care: defining the conditions of primary Care Plus. Int J Integr Care. 2016;16(1):12.
Firet L, de Bree C, Verhoeks CM, Teunissen DA, Lagro-Janssen AL. Mixed feelings: general practitioners’ attitudes towards eHealth for stress urinary incontinence-a qualitative study. BMC Fam Pract. 2019;20:1–8.
Noels EC, Wakkee M, van den Bos RR, Bindels PJE, Nijsten T, Lugtenberg M. Substitution of low-risk skin cancer hospital care towards primary care: a qualitative study on views of general practitioners and dermatologists. Plos One. 2019;14(3): e0213595.
Van Hoof SJ, Spreeuwenberg MD, Kroese ME, Steevens J, Meerlo RJ, Hanraets MM, et al. Substitution of outpatient care with primary care: a feasibility study on the experiences among general practitioners, medical specialists and patients. BMC Fam Pract. 2016;17(1):1–9.
Crawford DC, Li CS, Sprague S, Bhandari M. Clinical and cost implications of inpatient versus outpatient orthopedic surgeries: a systematic review of the published literature. Orthop Rev (Pavia). 2015;7(4):6177.
Calkins TE, Mosher ZA, Throckmorton TW, Brolin TJ. Safety and cost effectiveness of outpatient total shoulder Arthroplasty: a systematic review. J Am Acad Orthop Surg. 2022;30(2):e233–41.
Qin C, Dekker RG, Blough JT, Kadakia AR. Safety and outcomes of inpatient compared with outpatient surgical procedures for ankle fractures. J Bone Joint Surg Am. 2016;98(20):1699–705.
van Hoof SJM, Quanjel TCC, Kroese M, Spreeuwenberg MD, Ruwaard D. Substitution of outpatient hospital care with specialist care in the primary care setting: a systematic review on quality of care, health and costs. Plos One. 2019;14(8):e0219957.
Cryer L, Shannon SB, Van Amsterdam M, Leff B. Costs for “hospital at home” patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff (Millwood). 2012;31(6):1237–43.
Kringos D, Boerma W, Bourgueil Y, Cartier T, Dedeu T, Hasvold T, et al. The strength of primary care in Europe: an international comparative study. Br J Gen Pract. 2013;63(616):e742–50.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Evans SR. Clinical trial structures. J Exp Stroke Transl Med. 2010;3(1):8–18.
Malay S, Chung KC. The choice of controls for providing validity and evidence in clinical research. Plast Reconstr Surg. 2012;130(4):959–65.
Abdelmotagly Y, Noureldin M, Paramore L, Kummar R, Nedas T, Hindley R, et al. The impact of remote urology outpatient clinics during the COVID-19 pandemic. J Endoluminal Endourol. 2021;4(3):e17–25.
Barsom EZ, Jansen M, Tanis PJ, van de Ven AWH, van Blussé M, Buskens CJ, et al. Video consultation during follow up care: effect on quality of care and patient- and provider attitude in patients with colorectal cancer. Surg Endosc. 2021;35(3):1278–87.
Bager P, Hentze R, Nairn C. Outpatients with inflammatory bowel disease (IBD) strongly prefer annual telephone calls from an IBD nurse instead of outpatient visits. Gastroenterol Nurs. 2013;36(2):92–6.
Beaver K, Williamson S, Chalmers K. Telephone follow-up after treatment for breast cancer: views and experiences of patients and specialist breast care nurses. J Clin Nurs. 2010;19(19–20):2916–24.
Boydell N, Reynolds-Wright JJ, Cameron ST, Harden J. Women’s experiences of a telemedicine abortion service (up to 12 weeks) implemented during the coronavirus (COVID‐19) pandemic: a qualitative evaluation. BJOG: Int J Obstet Gynecol. 2021;128(11):1752–61.
Brewer A, Coleman V. Adaptation of a stoma care pathway and use of telephone clinics during the pandemic: patient experience survey. Br J Nurs. 2022;31(1):8–14.
Casey R, Powell L, Braithwaite M, Booth C, Sizer B, Corr J. Nurse-led phone call follow-up clinics are effective for patients with prostate cancer. J Patient Exp. 2017;4(3):114–20.
Damery S, Jones J, O’Connell Francischetto E, Jolly K, Lilford R, Ferguson J. Remote consultations versus standard face-to-face appointments for liver transplant patients in routine hospital care: feasibility randomized controlled trial of myVideoClinic. J Med Internet Res. 2021;23(9):e19232.
Duncan H, Russell RK. Role for structured telephone clinics in paediatric gastroenterology: reflections, lessons and patient feedback. BMJ Open Gastroenterol. 2019;6(1):e000245.
Hansen JB, Sørensen JF, Glassou EN, Homilius M, Hansen TB. Reducing patient–staff contact in fast-track total hip arthroplasty has no effect on patient-reported outcomes, but decreases satisfaction amongst patients with self-perceived complications: analysis of 211 patients. Acta Orthop. 2022;93:264.
Heeno E, Biesenbach I, Englund C, Lund M, Toft A, Lund L. Patient perspective on telemedicine replacing physical consultations in urology during the COVID-19 lockdown in Denmark. Scandinavian J Urol. 2021;55(3):177–83.
Jones MT, Arif R, Rai A. Patient experiences with telemedicine in a national health service rheumatology outpatient department during coronavirus disease-19. J Patient Exp. 2021;8:23743735211034972.
Khan Z, Kershaw V, Madhuvrata P, Radley S, Connor M. Patient experience of telephone consultations in gynaecology: a service evaluation. BJOG: Int J Obstet Gynecol. 2021;128(12):1958–65.
Kimman ML, Dellaert BG, Boersma LJ, Lambin P, Dirksen CD. Follow-up after treatment for breast cancer: one strategy fits all? An investigation of patient preferences using a discrete choice experiment. Acta Oncol. 2010;49(3):328–37.
Kjeldsted E, Lindblad KV, Bødtcher H, Sørensen DM, Rosted E, Christensen HG, et al. A population-based survey of patients’ experiences with teleconsultations in cancer care in Denmark during the COVID-19 pandemic. Acta Oncol. 2021;60(10):1352–60.
Knudsen LR, de Thurah A, Lomborg K. Experiences with telehealth followup in patients with rheumatoid arthritis: a qualitative interview study. Arthritis Care Res. 2018;70(9):1366–72.
Lee J, Hynes C, Humphries G, Thumbikat P. Pilot study to explore the use of video consultation for outpatient follow up of spinal cord injury (SCI) patients. Clin Rehabil. 2017;31(12):1690.
Lim K, Neal-Smith G, Mitchell C, Xerri J, Chuanromanee P. Perceptions of the use of artificial intelligence in the diagnosis of skin cancer: an outpatient survey. Clin Exp Dermatol. 2022;47(3):542–6.
Lo WB, Herbert K, Rodrigues D. Clinical effectiveness of and family experience with telephone consultation in a regional pediatric neurosurgery center in the United Kingdom. J Neurosurg Pediatr. 2021;28(4):483–9.
Patel S, Douglas-Moore J. A reflection on an adapted approach from face‐to‐face to telephone consultations in our Urology Outpatient Department during the COVID‐19 pandemic–a pathway for change to future practice? BJU Int. 2020;126(3):339–41.
Rovira A, Brar S, Munroe-Gray T, Ofo E, Rodriguez C, Kim D. Telephone consultation for two-week-wait ENT and head and neck cancer referrals: initial evaluation including patient satisfaction. J Laryngology Otology. 2022;136(7):615–21.
Singh N, Datta M. Single-centre telephone survey on patients’ perspectives regarding remote paediatric outpatient consultations in a district general hospital. BMJ Paediatrics Open. 2020;4(1):e000885.
Stavrou M, Lioutas E, Lioutas J, Davenport RJ. Experiences of remote consulting for patients and neurologists during the COVID-19 pandemic in Scotland. BMJ Neurol Open. 2021;3(2):e000173.
Trace S, Collinson A, Searle A, Lithander F. Using videoconsultations to deliver dietary advice to children with chronic kidney disease: a qualitative study of parent and child perspectives. J Hum Nutr Dietetics. 2020;33(6):881–9.
Tyler JM, Pratt AC, Wooster J, Vasilakis C, Wood RM. The impact of increased outpatient telehealth during COVID-19: retrospective analysis of patient survey and routine activity data from a major healthcare system in England. Int J Health Plann Manag. 2021;36(4):1338–45.
Van Erkel FM, Pet MJ, Bossink EH, Van de Graaf CF, Hodes MT, Van Ogtrop SN, et al. Experiences of patients and health care professionals on the quality of telephone follow-up care during the COVID-19 pandemic: a large qualitative study in a multidisciplinary academic setting. BMJ Open. 2022;12(3):e058361.
Watters C, Miller B, Kelly M, Burnay V, Karagama Y, Chevretton E. Virtual voice clinics in the COVID-19 era: have they been helpful? Eur Arch Otorhinolaryngol. 2021;278:4113–8.
Williamson S, Chalmers K, Beaver K. Patient experiences of nurse-led telephone follow-up following treatment for colorectal cancer. Eur J Oncol Nurs. 2015;19(3):237–43.
Aicken CR, Fuller SS, Sutcliffe LJ, Estcourt CS, Gkatzidou V, Oakeshott P, et al. Young people’s perceptions of smartphone-enabled self-testing and online care for sexually transmitted infections: qualitative interview study. BMC Public Health. 2016;16(1):1–11.
Baraitser P, Brown KC, Gleisner Z, Pearce V, Kumar U, Brady M. ‘Do it yourself’sexual health care: the user experience. Sex Health. 2011;8(1):23–9.
Boons CC, Timmers L, Janssen JJ, Swart EL, Hugtenburg JG, Hendrikse NH. Feasibility of and patients’ perspective on nilotinib dried blood spot self-sampling. Eur J Clin Pharmacol. 2019;75:825–9.
Bundgaard JS, Raaschou-Pedersen DT, Todsen T, Ringgaard A, Torp-Pedersen C, Von Buchwald C, et al. Danish citizens’ preferences for at-home oropharyngeal/nasal SARS-CoV-2 specimen collection. Int J Infect Dis. 2021;109:195–8.
Cameron S, Glasier A, Dewart H, Johnstone A. Women’s experiences of the final stage of early medical abortion at home: results of a pilot survey. BMJ Sex Reprod Health. 2010;36(4):213–6.
Grogan A, Coughlan M, Prizeman G, O’Connell N, O’Mahony N, Quinn K, et al. The patients’ perspective of international normalized ratio self-testing, remote communication of test results and confidence to move to self-management. J Clin Nurs. 2017;26(23–24):4379–89.
Haroon S, Griva K, Davenport A. Factors affecting uptake of home hemodialysis among self-care dialysis unit patients. Hemodial Int. 2020;24(4):460–9.
Hope J. A patient perspective on the barriers to home dialysis. J Ren care. 2013;39(S1):3–8.
Hoyos J, Maté T, Guerras J-M, Donat M, Agustí C, Kuske M, et al. Preference towards HIV Self-Testing above other testing options in a sample of men who have sex with men from five European countries. Int J Environ Res Public Health. 2021;18(9):4804.
Den Oudendammer WM, Broerse JE. Towards a decision aid for self-tests: users’ experiences in the Netherlands. Health Expect. 2019;22(5):983–92.
Tompson AC, Ward AM, McManus RJ, Perera R, Thompson MJ, Heneghan CJ, et al. Acceptability and psychological impact of out-of-office monitoring to diagnose hypertension: an evaluation of survey data from primary care patients. Br J Gen Pract. 2019;69(683):e389–97.
Tonna A, Anthony G, Tonna I, Paudyal V, Forbes-McKay K, Laing R, et al. Home self-administration of intravenous antibiotics as part of an outpatient parenteral antibiotic therapy service: a qualitative study of the perspectives of patients who do not self-administer. BMJ Open. 2019;9(1):e027475.
Veerus P, Hallik R, Jänes J, Jõers K, Paapsi K, Laidra K, et al. Human papillomavirus self-sampling for long-term non-attenders in cervical cancer screening: a randomised feasibility study in Estonia. J Med Screen. 2022;29(1):53–60.
Witzel T, Bourne A, Burns F, Rodger A, McCabe L, Gabriel M, et al. HIV self-testing intervention experiences and kit usability: results from a qualitative study among men who have sex with men in the SELPHI (Self‐Testing Public Health Intervention) randomized controlled trial in England and Wales. HIV Med. 2020;21(3):189–97.
Bendien S, van Leeuwen M, Lau H, Ten Brinke A, Visser L, de Koning E, et al. Home-based intravenous treatment with reslizumab for severe asthma in the Netherlands–An evaluation. Respir Med. 2022;194:106776.
Corrie P, Moody A, Armstrong G, Nolasco S, Lao-Sirieix S, Bavister L, et al. Is community treatment best? A randomised trial comparing delivery of cancer treatment in the hospital, home and GP surgery. Br J Cancer. 2013;109(6):1549–55.
Dismore LL, Echevarria C, Van Wersch A, Gibson J, Bourke S. What are the positive drivers and potential barriers to implementation of hospital at home selected by low-risk DECAF score in the UK: a qualitative study embedded within a randomised controlled trial. BMJ Open. 2019;9(4):e026609.
Goossens LM, Utens CM, Smeenk FW, Donkers B, van Schayck OC, Rutten-van Mölken MP. Should I stay or should I go home? A latent class analysis of a discrete choice experiment on hospital-at-home. Value Health. 2014;17(5):588–96.
Hansson H, Kjaergaard H, Johansen C, Hallström I, Christensen J, Madsen M, et al. Hospital-based home care for children with cancer: feasibility and psychosocial impact on children and their families. Pediatr Blood Cancer. 2013;60(5):865–72.
Hansson H, Kjaergaard H, Schmiegelow K, Hallström I. Hospital-based home care for children with cancer: a qualitative exploration of family members’ experiences in Denmark. Eur J Cancer Care. 2012;21(1):59–66.
Jepsen LØ, Høybye MT, Hansen DG, Marcher CW, Friis LS. Outpatient management of intensively treated acute leukemia patients—the patients’ perspective. Support Care Cancer. 2016;24:2111–8.
Lohr PA, Wade J, Riley L, Fitzgibbon A, Furedi A. Women’s opinions on the home management of early medical abortion in the UK. BMJ Sex Reprod Health. 2010;36(1):21–5.
Rosted E, Aabom B, Hølge-Hazelton B, Raunkiær M. Comparing two models of outpatient specialised palliative care. BMC Palliat Care. 2021;20(1):1–13.
Schiff R, Oyston M, Quinn M, Walters S, McEnhill P, Collins M. Hospital at home: another piece of the armoury against COVID-19. Future Healthc J. 2022;9(1):90–5.
Uitdehaag MJ, Van Putten PG, Van Eijck CH, Verschuur EM, Van der Gaast A, Pek CJ, et al. Nurse-led follow-up at home vs. conventional medical outpatient clinic follow-up in patients with incurable upper gastrointestinal cancer: a randomized study. J Pain Symptom Manag. 2014;47(3):518–30.
Utens CM, Goossens LM, Van Schayck OC, Rutten-van Mölken MP, Van Litsenburg W, Janssen A, et al. Patient preference and satisfaction in hospital-at-home and usual hospital care for COPD exacerbations: results of a randomised controlled trial. Int J Nurs Stud. 2013;50(11):1537–49.
Van Ramshorst J, Duffels M, De Boer S, Bos-Schaap A, Drexhage O, Walburg S, et al. Connected care for endocarditis and heart failure patients: a hospital-at-home programme. Neth Heart J. 2022;30(6):319–27.
Baena-Cañada JM, Ramirez-Daffos P, Cortes-Carmona C, Rosado-Varela P, Nieto-Vera J, Benitez-Rodriguez E. Follow-up of long-term survivors of breast cancer in primary care versus specialist attention. Fam Pract. 2013;30(5):525–32.
Van Bodegom-Vos L, De Jong JD, Spreeuwenberg P, Curfs EC, Groenewegen PP. Are patients’ preferences for shifting services from medical specialists to general practitioners related to the type of medical intervention? Qual Prim Care. 2013;21(2):81–95.
Pollard L, Rogers S, Shribman J, Sprigings D, Sinfield P. A study of role expansion: a new GP role in cardiology care. BMC Health Serv Res. 2014;14(1):1–10.
Milosevic S, Joseph-Williams N, Pell B, Cain E, Hackett R, Murdoch F, et al. Managing lower urinary tract symptoms in primary care: qualitative study of GPs’ and patients’ experiences. Br J Gen Pract. 2021;71(710):e685–92.
Wildeboer JA, Van de Ven ART, De Boer D. Substitution of care for chronic heart failure from the hospital to the general practice: patients’ perspectives. BMC Fam Pract. 2018;19(1):8.
Cottrell E, McMillan K, Chambers R. A cross-sectional survey and service evaluation of simple telehealth in primary care: what do patients think? BMJ Open. 2012;2(6):e001392.
Scott A, Jones C. An exploration of the attitudes and perceptions of the UK public towards self-care for minor ailments. Br J Nurs. 2020;29(1):44–9.
McAteer A, Yi D, Watson V, Norwood P, Ryan M, Hannaford PC, et al. Exploring preferences for symptom management in primary care: a discrete choice experiment using a questionnaire survey. Br J Gen Pract. 2015;65(636):e478–88.
Fletcher B, Hinton L, McManus R, Rivero-Arias O. Patient preferences for management of high blood pressure in the UK: a discrete choice experiment. Br J Gen Pract. 2019;69(686):e629–37.
Heath G, Greenfield S, Redwood S. The meaning of ‘place’in families’ lived experiences of paediatric outpatient care in different settings: a descriptive phenomenological study. Health Place. 2015;31:46–53.
King KE. Patient satisfaction in a one-stop Haematuria clinic and urology outpatients: a comparison of clinics. Int J Urol Nurs. 2016;10(3):127–36.
Fitzsimmons DA, Thompson J, Bentley CL, Mountain GA. Comparison of patient perceptions of Telehealth-supported and specialist nursing interventions for early stage COPD: a qualitative study. BMC Health Serv Res. 2016;16:1–12.
Mitchell T. Patients’ experiences of receiving chemotherapy in outpatient clinic and/or onboard a unique nurse-led mobile chemotherapy unit: a qualitative study. Eur J Cancer Care. 2013;22(4):430–9.
Cook EJ, Randhawa G, Large S, Guppy A, Chater AM, Ali N. Barriers and facilitators to using NHS Direct: a qualitative study ofusers’ andnon-users’. BMC Health Serv Res. 2014;14(1):1–12.
Acknowledgements
We would like to thank Linda Schoonmade, medical information specialist, for her contribution to this research in helping develop the search strategy.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
The selection process of articles was performed by all authors. L.D. wrote the main manuscript text. All authors reviewed and edited the manuscript. L.T., J.J., B.K. and J.K. supervised.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix A.
Search string Pubmed.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Damen, L.J., Van Tuyl, L.H.D., Korevaar, J.C. et al. Citizens’ perspectives on relocating care: a scoping review. BMC Health Serv Res 24, 202 (2024). https://doi.org/10.1186/s12913-024-10671-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-024-10671-3