
Abstract
Introduction
Organizational commitment refers to the extent to which employees identify with and are involved with a given organization. It is an important variable for healthcare organizations to consider since it acts as a predictor of job satisfaction, organizational efficiency and effectiveness, health professionals’ absenteeism, and turnover. However, there is a knowledge gap in the health sector about workplace factors that are associated with healthcare provider commitment to their organization. Thus, this study aimed to assess organizational commitment and associated factors among health professionals working in public hospitals in the southwestern Oromia region, Ethiopia.
Methods
A facility-based analytical cross-sectional study was conducted from March 30 to April 30, 2021. A multistage sampling technique was employed to select 545 health professionals from public health facilities. Data were collected using a structured self-administered questionnaire. simple and multiple linear regression analyses were employed to assess the association between organizational commitment and explanatory variables after checking the assumptions of factor analysis and linear regression. The statistical significance was declared at a p-value of < 0.05 and Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI).
Results
Health professionals’ organizational commitment percentage mean score was 48.8% (95% CI: 47.39, 50.24). A higher level of organizational commitment was associated to satisfaction with recognition, work climate, supervisor support, and workload. Besides, good practice of transformational and transactional leadership styles and employee empowerment are significantly associated with high organizational commitment.
Conclusion
The overall level of organizational commitment is a bit low. To improve the organizational commitment of health professionals, hospital managers, and healthcare policy-makers need to develop and institutionalize evidence-based satisfaction strategies, practice good leadership styles and empower healthcare providers on the job.
Similar content being viewed by others


Background
Organizational commitment refers to the relative strength of an individual’s identification and involvement with the overall employing organization and not with a department or specific workgroup [1]. Organizational commitment also means complying with the aims and objectives of the organization, organizational principles, rules and norms, and volunteering for their survival [2].
Meyer and Allen theorized three types of organizational commitment in 1984: affective, continuance, and normative commitment [3]. Affective commitment is related to an employee’s emotional connection, identification, and participation in the organization. Normative commitment is about employees’ feelings of responsibility to the organization, while continuance commitment is associated with perceived costs related to exiting the organization [3, 4].
According to studies on the issue, several factors such as; work climate, recognition, supervisor support, workload, leadership styles, and individual and job characteristics related variables were the most significant factors that determine employees’ commitment to their organizations [5, 6].
A high level of employee organizational commitment has several implications for healthcare organizations, including a strong desire to achieve organizational goals, a strong desire to stay in the organization, improved organizational performance, increased motivation, belongingness, and attachment to their organization, increased effectiveness and efficiency of their organization, improved job satisfaction, reduced turnover, burnout, and staff absenteeism [7,8,9]. On the contrary, having poor organizational commitment increases the occurrence of medical errors and poses a threat to patient safety [10].
Researchers found that employees committed to their organization provided a high quality of care [9], had better performance [11], ensured patient safety [12], and continuous routine operations [13]. However, various findings showed organizational commitment among healthcare professionals is low. In Saudi Arabia and Egypt, the magnitude of organizational commitment was reported to be 57.3% and 63.9%, respectively [14, 15]. Similarly, studies on the issue in different parts of Ethiopia showed results ranging from 64.81 to 88.06% [7, 16, 17].
Considerable studies focused on organizational commitment in the field of nursing [18,19,20,21,22,23]. However, organizational commitment gaps are affecting other healthcare professions as well and there is a shortage of knowledge in the health sector on workplace factors that are associated with employees’ commitment to their organization. Moreover, variables such as leadership styles and health professionals’ empowerment that might significantly influence employees’ organizational commitment have not yet been assessed in previous studies in Ethiopia. Therefore, this study set out to address workplace factors that influence the organizational commitment of healthcare professionals.
Thus, the study fills the knowledge gap in organizational commitment in the health sector and provides evidence for making decisions that are appropriate to the context. Besides, it helps managers and policymakers better understand the underlying issue and implement strategies that improve healthcare providers’ commitment to their organization.
Method and materials
Study design and setting
A facility-based analytical cross-sectional study design was employed to assess the organizational commitment of healthcare professionals working in the southwestern Oromia region public health facilities, in Ethiopia from March 30 to April 30, 2021. In this part of the region, there are seven administrative zones, of which, we have chosen three zones, namely Buno Bedele, Ilubabor, and Jimma zones randomly. Bedele, Metu, and Jimma are the administrative towns of the three zones, respectively. The towns are 480, 600, and 354 km away from Addis Ababa, respectively.
According to the 2019 projected population report of Ethiopia, the three zones had a total population of 5,095,050. There are 15 public hospitals in these zones among these hospitals; one found in Jimma town is a specialized hospital, the other found in Metu town namely Karl hospital is a referral hospital and the rest of the public hospitals are primary hospitals. According to the information obtained from Oromia regional health bureau in 2020, there were 2,577 health professionals working in the public hospitals of the three zones.
All health professionals working in public hospitals in the southwestern Oromia region were the source population, whereas health professionals working in randomly selected public hospitals were the study population.
Health professionals who have been working for at least 6 months in the selected public hospitals were included in the study, whereas volunteers and part-time workers were excluded.
Sample size determination and sampling procedure
The sample size was determined by using a single population mean estimation formula (n = (Zα/2)2 * δ2/d2). A confidence level of 95% and a margin of error(d) of 1% were used. In a similar study at Jimma University specialized hospital, in Ethiopia, a standard deviation (σ) of 8.22 was used [17]. By considering design effect 2 and 10% non-response rate the final sample size was 572.
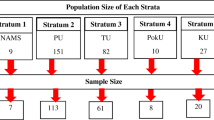
A multi-stage with a simple random sampling technique was used. Initially, out of the seven administrative zones in southwestern Oromia, three zones: Buno Bedele, Ilubabor and Jimma zones were selected by lottery method. Second, seven government hospitals were chosen from the three selected zones using a simple random sampling method. The calculated sample size was then proportionally allocated to each selected hospital according to the number of health professionals they had. Finally, study participants were selected using simple random sampling from the health professionals’ payroll forms (Fig. 1).

Schematic presentation of sampling procedure
Note: PH: Primary Hospital; GH: General Hospital and SH: Specialized Hospital
Variables and measurement
Organizational commitment
Is the degree of health professionals’ attachment, loyalty, and identification with their organization. Its overall level of organizational commitment was measured by 10 items with a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree) [24]. The mean score was converted to a percentage of the scale mean score (%SM). This value ranges from “0%” to “100%”, and was calculated using the formula: \(\text{\%} \text{S}\text{M}=\frac{\text{A}\text{c}\text{t}\text{u}\text{a}\text{l} \text{s}\text{c}\text{o}\text{r}\text{e} - \text{s}\text{c}\text{o}\text{r}\text{e} \text{m}\text{i}\text{n}\text{i}\text{m}\text{u}\text{m}}{\text{s}\text{c}\text{o}\text{r}\text{e} \text{m}\text{a}\text{x}\text{i}\text{m}\text{u}\text{m} ? \text{s}\text{c}\text{o}\text{r}\text{e} \text{m}\text{i}\text{n}\text{i}\text{m}\text{u}\text{m}}\text{*}100\) [25]. The composite scale of organizational commitment score was created from the three factors that emerged during the factor analysis of organizational commitment items. This score was used as a continuous dependent variable during linear regression.
Job satisfaction
Is the degree of positive or negative views workers has about their job or job experience. It was measured with four dimensions (perceived recognition (5 items), perceived working climate (10 items), perceived supervisor support (4 items), and perceived workload (3 items)) consisting of 22 items of five-point Likert scales [26].
Perceived recognition
The health professionals’ feeling toward the praise they get for doing a good job. It was measured with five items on a 5-point Likert scale [26].
Perceived working climate
The quality of both physical attributes and the degree to which the working environment provides meaningful work. It was measured by using ten items each scoring a 5-point Likert scale [26].
Perceived supervisor support
Is the supervisors’ responsibility both in preventing and solving employee problems. It was measured by using four items each scoring a 5-point Likert scale [26].
Perceived workload
It describes the participant’s work requirement, the amount of time and resources for this requirement. It is measured by using three items each scored 5-point Likert scale [26].
Perceived organizational support
It refers to the extent to which employees see that organizations recognize their contribution and care about their well-being. It was measured by four items which were measured in a 5-point Likert type; factor analysis was used to explore the factor structure of the scale [27].
Perceived leadership style
This is the perception of HPs regarding how their immediate leader treats them. It was measured with two dimensions consisting of seven items which were created on factor analysis, to be measured on a 5-point Likert scale [28].
Perceived transformational leadership style
The perception of health professionals about how their immediate leader influence and inspire them. It was measured by using five items each scoring a 5-point Likert scale [28].
Perceived transactional leadership style
The perception of health professionals about how their immediate leader responds or reacts to problems/situations. It was measured by using two items each scoring a 5-point Likert scale [28].
Employee empowerment
It describes the feeling of health professionals having proportionate power in their organization. It was measured by using five items each scored on a 5-point Likert scale [29].
Data collection tools and procedures
Data were collected using self-administered structured questionnaires adapted from different literature and have 6 parts. Part one sociodemographic and economic data with 12 items, part two job satisfaction data comprised 22 items, and part three perceived organizational support questionnaire with 8 items [9]. Part four OC was measured with 24 items which were adapted from questionnaires developed and validated by Meyer and Allen [24], and part five perceived leadership style measure with 9 items adapted from the Multifactor Leadership Questionnaire (MLQ) [28]. Except for the sociodemographic and economic data, all parts will be measured on a 5-point Likert scale ranging from strongly disagree = 1, to strongly agree = 5.
Three public health officers and two BSc nurses for data collection and three public health officer lecturers for supervision were employed. Each data collector collected data from health professionals working in their zone. Supervisors and principal investigators were responsible for routine supervision.
Data quality control
To ensure consistency, the questionnaires were initially prepared in English and translated into the local language (Afan Oromo and Amharic) and finally back into English. One day of training was given to data collectors and supervisors before the data collection. To ensure the study’s internal validity, the tool was pre-tested with 5% of the sample outside the study area and modification was made before actual data collection. The overall internal consistency of the tools was checked using Cronbach’s alpha reliability test, and the score for the items of each component was greater than 0.79. Moreover, each item was qualitatively evaluated by all authors for readability, meaning, clarity and feasibility related to study participants. To test the discriminatory validity of the item scales that measure each dimension of the constructs of the variable, a principal component analysis was employed. Items with a loading coefficient of less than 0.30 were excluded from further analysis. Because of their weak discriminatory ability with the items of the other constructs, some items were excluded from the subsequent analysis. In the end, a single scale is created by averaging items that fulfill the discriminant validity for each of the variables.
Data management and analysis
The data were cleaned and checked for consistency, coded, and entered into Epi Info version 7 software, and exported to Stata version 14 statistical software for analysis. Recoding, computing, ranking, and counting were performed before data analysis. All assumptions of factor analysis were checked. The normality of the data was evaluated by performing the Shapiro-Wilk test, and the result indicates evidence of both the normality of the data and the absence of outliers (W = 0.94, P-value = 0.32). The linearity of the data was assessed by generating a scatter plot and all of the points in the plot fall along a straight line. The Variance Inflation Factors (VIF) were used to test for multicollinearity, and all the values were below 10. Homoscedasticity was assessed by generating a plot of standard residual against standard predicted values of the dependent variable in regression models through which the random patterned distribution and independence of error terms were assessed.
Simple linear regression analysis was done to identify candidate variables for multiple linear regression analysis and a p-value of ≤ 0.20 was used to select these variables. Factors predicting organizational commitment were differentiated by using multiple linear regression analysis at a significance level of p-value < 0.05 and a 95% CI.
Results
Sociodemographic characteristics of respondents
A total of 545 health professionals participated in this study, with a response rate of 95.30%. More than half of the respondents (57.61%) were males. Nearly two out of the three respondents were married (62.57%) and about 43.67% were nurses in their profession. The median age of the participants was 30 years, Inter Quartile Range (IQR = 7). The median net monthly salary of Health professionals was 6,500 Birr (IQR = 2,900) (Table 1).
Job satisfaction
Among job satisfaction dimensions, the highest percentage mean score, 53.2%, was observed in the category of working climate, and the lowest score, 44.6%, was in the supervisor support component. (Table 2).
Leadership style, organizational support, and employee empowerment
Regarding leadership styles, 46.65% and 46.9% percentage mean score was observed for transformational and transactional leadership styles, respectively. The percentage mean score of organizational support and employee empowerment was 48.75% and 52.85%, respectively (Table 3).
Level of organizational commitment
In this study, among organizational commitment domains, the affective commitment dimension had the highest mean score (3.10 ± 0.93). The overall mean score for organizational Commitment was 2.95 ± 0.65 (%SM = 48.80% with 95% CI: 47.39, 50.24,) with 53.68% of health professionals scoring higher than the composite percentage sum mean score. (Table 4).
Factors associated with organizational commitment
In this study, a simple linear regression analysis was performed for all independent variables to see their independent effect on the level of organizational commitment. Accordingly, eight variables were identified as having less than 0.2 significance level in the bivariable simple linear regression and entered into the final multivariable linear regression model. The final model explained 77% (Adjusted R Square = 0.77) of the variability in the organizational commitment of healthcare professionals.
Job satisfaction-related factors: (work climate, recognition, supervisor support, and workload) was found to have a positive significant association with organizational commitment. Among these dimensions, work climate was the strongest predictor of organizational commitment. For a unit increase in work climate, the organizational commitment score increases by 0.32 units (95% CI: 0.18, 0.46).
Besides, there was a positive significant association between leadership styles and organizational commitment. In this regard, the organizational commitment score increases by 0.42 units for a unit increase in the transformational leadership style (95% CI: 0.28, 0.55). Similarly, for a unit increase in transactional leadership style, the organizational commitment score increases by 0.54 units (95% CI: 0.45, 0.62).
Employee empowerment was also found to have a positive significant association with organizational commitment. For a unit increase in employee empowerment, the organizational commitment score increases by 0.08 units (95% CI: 0.05, 0.11) (Table 5).
Discussion
In this study, the magnitude of organizational commitment in the southwestern Oromia public health facilities was 48.8%. Health professionals’ job satisfaction, leadership style, and employee empowerment are factors associated with organizational commitment.
Organizational commitment in the current study was lower compared to related studies conducted in Saudi Arabia [14], in Ethiopia Gurage zone [9], Bench-sheko zone [7], and Jimma university specialized hospital [17], where the percentage mean score of organizational commitment were 57.3%, 64.81%, 74.6%, and 88.06%, respectively. These differences could be due to socioeconomic, political, and cultural variations, particularly in the Saudi Arabia study, and participants’ regard to nurses alone at Jimma University specialized hospital. Besides, unlike the studies conducted at Gurage and Benchsheko Zone, which addressed health professionals working in health centers, our study was done in a hospital setting, where health professionals would face a large volume of patient flow and a high workload. Furthermore, during the COVID-19 pandemic, the medical environment is quite intensive. The combination of pressure, high vulnerability to COVID-19, spikes in workload, and a stressful workplace has produced a difficult organizational climate that may reduce health professionals’ commitment to their organization.
Our study suggested that satisfaction with work climate and recognition were significantly associated with organizational commitment. This implies that improving job satisfaction, specifically enhancing the working environment and recognition, is an important variable in promoting employees’ organizational commitment. This finding is in line with the result of other similar studies conducted in Ethiopia and Riyad [7, 9, 30]. This association can be explained by the fact that organizations with a conducive work environment will give healthcare professionals a sense of security and comfort, and this impression may intern lead employees to be committed to their organization, support its goals, and maintain membership [31]. Recognition of health professionals’ role and contribution to the organization may also have an impact on their perception of self-worth within the organization, and hence on their commitment to the organization.
In this study, satisfaction with supervisor support and workload were significantly associated with organizational commitment. This finding is in agreement with the study conducted in Nederland [32]. This can be explained by the fact that the supervisors may be regarded by their employees as representatives of the organization, and they may respond to the organization by expressing their attitudes or perception toward their supervisor.
Our finding also shows that leadership styles were found to have a significant positive association with the level of organizational commitment. This finding is congruent with the result of other similar studies conducted in Ethiopia and Saudi Arabia [7, 9, 14]. This can be explained by the characteristics of the transformational leadership style, which include idealized influence, inspirational motivation, intellectual stimulation, and individualized consideration, in which the leader gives followers a vision and a sense of mission and earns their respect and confidence from followers while also providing support, encouragement, and developmental opportunities.
When leaders exhibit transformational leadership behavior, employees express a highly personal connection with their leaders and go beyond self-interest because they are highly motivated and inspired to achieve what is expected of them which makes them committed [33].
In our study, employee empowerment was found to have a significant association with organizational commitment. This finding was in agreement with a study conducted in Egypt [34]. This may be the fact that employees who feel empowered at work are more likely to have a sense of autonomy or control over their work, believe they are competent in their skills and that they can make a difference. They are also strong, self-assured individuals, who are committed to a meaningful goal and show initiative to attain it.
Limitations of the study
The use of a self-reporting questionnaire might lead to reporting bias, which may occur when respondents erroneously interpret questions. We also admit that COVID-19 social distancing measures may have affected responses. Furthermore, a qualitative method was not used to triangulate the data.
Conclusion
The level of organizational commitment of health professionals working in southwestern Oromia region public hospitals was found to be low. Dissatisfaction with recognition, supervisor support, work climate, and high workload had a negative effect on organizational commitment. Additionally, practicing good transformational and transactional leadership styles was found to be a significant predictor of organizational commitment. Furthermore, employee empowerment showed a significant positive effect on organizational commitment.
Therefore, to increase the commitment of health professionals to their organization, hospital managers and healthcare policymakers should consider the factors pointed out in this study.
Data Availability
Data will be available from the corresponding author on reasonable request.
Abbreviations
- HCOs:
-
Healthcare Organizations
- HRH:
-
Human Resource for Health
- HSTP:
-
Health Sector Transformation Plan
- HWs:
-
Health Workers
- HWF:
-
Health Work Force
- IRB:
-
Institutional Review Board
- JS:
-
Job Satisfaction
- LMIC:
-
Low and Middle-Income Countries
- OC:
-
Organizational Commitment
- OST:
-
Organizational Support Theory
- SET:
-
Social Exchange Theory
- SDG:
-
Sustainable Development Goals
- SSA:
-
Sub-Saharan Africa
- SW:
-
Southwest
- UHC:
-
Universal Health Coverage and WHO:World Health Organization
References
Mowday RT. Reflections on the study and relevance of organizational commitment. Hum Resource Manage Rev. 1998;8(4):387–401.
Dominic E, Salim M. A study on the role of organizational commitment and perception towards organizational justice and fairness in triggering organizational citizenship behavior among b school faculty members in Kerala. Rajagiri Manage J. 2018;12(1):23–42.
Meyer JP, Allen NJ. Testing the” side-bet theory” of organizational commitment: some methodological considerations. J Appl Psychol. 1984;69(3):372.
Meyer JP, Allen NJ. A three-component conceptualization of organizational commitment. Hum resource Manage Rev. 1991;1(1):61–89.
Mowday RT, Steers RM, Porter LW. The measurement of organizational commitment. J Vocat Behav. 1979;14(2):224–47.
Demir C, Sahin B, Teke K, Ucar M, Kursun O. Organizational commitment of military physicians. Mil Med. 2009;174(9):929–35.
Alemayehu D, Ololo S, Siraneh Y. Organizational commitment and Associated factors among Health Professionals Working in Public Health Facilities of Benchsheko Zone Southwest Ethiopia. In.: Research Square; 2021.
Almeida H, Kim YI, Geun HG, Choi S, Lee YS. The impact of organizational commitment and nursing Organizational Culture on Job satisfaction in korean American Registered Nurses. West J Nurs Res. 2017;28(6):590–7.
Nima GH, Kerie MW, Nebeb GT. Organizational commitment of health professionals and associated factors in government health facilities of Gurage zone, South Ethiopia. Clin Med Res. 2016;5(5):82–90.
Chen SY, Wu WC, Chang CS, Lin CT, Kung JY, Weng HC, Lin YT, Lee SI. Organizational justice, trust, and identification and their effects on organizational commitment in hospital nursing staff. BMC Health Serv Res. 2015;15:363.
Health FDRoEMo: Health sector transformation plan. (2015/16–2019/20). In.: Federal Ministry of Health Addis Ababa, Ethiopia; 2015.
Chen S-Y, Wu W-C, Chang C-S, Lin C-T, Kung J-Y, Weng H-C, Lin Y-T, Lee S-I. Organizational justice, trust, and identification and their effects on organizational commitment in hospital nursing staff. BMC Health Serv Res. 2015;15(1):1–17.
Ramaprasad BS, KP NP, Lakshminarayanan S, Pai YP. Human resource management practices and organizational commitment: research methods, issues and future directions (2001–2016). Industrial and Commercial Training 2017.
Al-Haroon HI, Al-Qahtani MF. Assessment of Organizational Commitment Among Nurses in a Major Public Hospital in Saudi Arabia. 2020, 13:519–526.
Ahmed RM, Abdelwahab EA, Elguindy H. Staff nurses’ intention to leave nursing profession and their organizational commitment in selected hospitals at Beni-Sueif city. Egypt Nurs J. 2017;14(1):17.
Hailemicae G, Woldie M, Tsega G. Health Professionals Organizational Commitment and Associated Factors in Government Health Facilities of Gurage Zone, South Ethiopia. 2014.
Walle F, Woldemichae K, Demeke T. Organizational commitment and its predictors among nurses working in Jimma University Specialized Teaching Hospital, Southwest Ethiopia. 2016.
Vandenberghe C, Bentein K, Panaccio A. Affective commitment to Organizations and Supervisors and turnover: a Role Theory Perspective. J Manag. 2014;43(7):2090–117.
Karami A, Farokhzadian J, Foroughameri G. Nurses’ professional competency and organizational commitment: is it important for human resource management? PLoS ONE. 2017;12(11):e0187863–3.
Yang FH, Chang CC. Emotional labour, job satisfaction and organizational commitment amongst clinical nurses: a questionnaire survey. Int J Nurs Stud. 2008;45(6):879–87.
Santos A, Chambel MJ, Castanheira F. Relational job characteristics and nurses’ affective organizational commitment: the mediating role of work engagement. J Adv Nurs. 2016;72(2):294–305.
Sasaki S, Fukada M, Okuda R, Fujihara Y. Impact of Organization and Career Commitment on clinical nursing competency. Yonago acta medica. 2019;62(2):221–31.
Vanaki Z, Vagharseyyedin SA. Organizational commitment, work environment conditions, and life satisfaction among iranian nurses. J Multidisciplinary Healthc. 2009;11(4):404–9.
Jaros S. Meyer and Allen model of organizational commitment: measurement issues. Icfai J Organizational Behav. 2007;6(4):7–25.
Baraki N, Siraneh Y, Ololo S, Tsega G, Yitbarek K, Adamu A, Erchafo B, Hailu M, Woldie M. Level and factors Associated with Professional Commitment of Health Professionals Providing Institutional Delivery Services in Public Health Facilities, Southwest Ethiopia. J Community Health. 2018;28(4):495–504.
Minnesota Satisfaction Questionnaire. (MSQ) Short form. https://sites.uni.edu/butlera/courses/org/msq.htm.
Pejtersen JH, Kristensen TS, Borg V, Bjorner JB. The second version of the Copenhagen Psychosocial Questionnaire. Scand J Public Health. 2010;38(3suppl):8–24.
Cristina M, Ticlau T. Transformational leadership in the public sector. A pilot study using MLQ to evaluate leadership style in Cluj county local authorities. Revista de cercetare si interventie sociala. 2012;36:74.
Menon ST. Employee empowerment: Definition, measurement and construct validation. 1995.
Habibi H, Al-Aameri AS. Job satisfaction and organizational commitment for nurses. J evidence-based Integr Med. 2000;21(6):531–5.
Pitaloka E, Paramita Sofia I, THE AFFECT OF WORK ENVIRONMENT, JOB SATISFACTION, ORGANIZATION COMMITMENT ON OCB OF INTERNAL AUDITORS. Int J Bus Econ Law. 2014;5:10–8.
Schagen Nv.: The effect of workload and job insecurity on affective organizational commitment: The moderating role of supervisory support; July 2014. file://C:/Users/Endalikachew/Downloads/Schagen__Nienke_van_6168280_MSc_EPBK%20(2).pdf.
Asiri SA, Rohrer WW, Al-Surimi K, Da’ar OO, Ahmed A. The association of leadership styles and empowerment with nurses’ organizational commitment in an acute health care setting: a cross-sectional study. BMC Nurs. 2016;15:38.
AbdElrahman M. Relationship between Empowerment and Organizational Commitment among Staff Nurses. 2018.
Acknowledgements
The authors would like to thank the Oromia region health bureau, respected hospitals, health professionals working in southern Oromia public hospitals, supervisors, and data collectors for their unreserved contribution to this study.
Funding
The authors did not received funding for this work.
Author information
Authors and Affiliations
Contributions
BF, ED and NW conceived the study, developed the tool and were involved in the data analysis. NW, ED, and AD drafted, edited, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from the Ethical Review Committee of the University of Gondar College of Medicine and Health Sciences, Institute of Public Health (Ref. No: IPH/1461/2013). Then, a permission letter was obtained from the respective public hospitals before the actual data collection. Written informed consent was obtained from each study participant. The autonomy and confidentiality of participants were maintained by using code numbers instead of personal identifiers. Finally, the study was performed in accordance with the Helsinki Declaration.
Consent for publication
Not applicable.
Competing interests
The authors declared no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fantahun, B., Dellie, E., Worku, N. et al. Organizational commitment and associated factors among health professionals working in public hospitals of southwestern Oromia, Ethiopia. BMC Health Serv Res 23, 180 (2023). https://doi.org/10.1186/s12913-023-09167-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-09167-3