
Abstract
Background
Having a research-engaged health and medical workforce is associated with improvements in clinical outcomes for patients. As such, there has been significant government investment internationally to support health care organisations and services to increase staff engagement with research.
Objectives
This scoping review sought to provide an overview of the literature describing strategies employed to increase research engagement by health care providers and organisations, and to undertake a qualitative analysis to generate a list of research engagement strategies.
Methods
A scoping review using systematic search strategies was undertaken to locate peer-review publications and grey literature related to research engagement by health care providers and organisations. Research engagement was defined as a ‘deliberate set of intellectual and practical activities undertaken by health care staff and organisations to conduct research’. A database search of electronic records was performed with no limit on publication date. Publications were included regardless of study type (excluding systematic reviews) and categorised as either databased (presenting data or new analysis of existing data) and non-databased (no new data or analyses). Databased publications were further classified according to study type, study design and setting. A qualitative synthesis using a Framework Approach was undertaken with all studies that described a strategy to improve research engagement.
Results
A total of 152 publications were included in this study with 54% categorised as non-databased. Of the databased articles, the majority (72%) were descriptive studies describing prevalence of correlates of research engagement, 17 (25%) described intervention studies where only two were controlled studies. The following research engagement strategies were identified: i) dual skilled team/staff, ii) resources or physical infrastructure, iii) incentives, iv) leadership support of research, v) education/training, vi) networks, vii) forming partnerships or collaborations and viii) overall leadership structure of entity.
Conclusions
The literature on research engagement is primarily opinion-based and descriptive in nature. To provide the evidence needed to inform strategies, this needs to progress beyond descriptive to more rigorous well-designed intervention research.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Health services are under continuing pressure to improve the quality of care they provide and the outcomes of such care for patients. To address this, health services employ a wide range of strategies such as the implementation of new treatments, devices and models of care, the recruitment of skilled staff, professional development of existing staff, investment in quality improvement staff and initiatives, development of IT and other care delivery support systems, tools and resources, and establishment of care delivery and performance monitoring systems [1–5].
The conduct of research in health services, or research engagement by health service providers, has also been suggested to have additional benefits to the quality of patient care and outcomes through indirectly modifying the culture and practice of care delivery [6, 7]. Research engagement has been variably defined with one review describing clinician research engagement as a ‘deliberate set of intellectual and practical activities undertaken by health care staff and organisations to conduct research’ [8]. Systematic reviews have reported improvements in health outcomes and provision of care where clinicians and organisations are research-engaged [6, 7]. Further, several longitudinal studies have reported that provider and/or health care organisation participation in clinical trials can result in lower mortality rates and greater adherence to clinical guidelines [9]. This greater focus on ‘knowledge production/generation’ by health service end users, and engagement of such end users in identifying research priorities has been suggested to promote better quality health care and patient outcomes [10]. In response, a shift in health and medical research and health service delivery policies toward increasing the engagement of health care services in the conduct of research is occurring internationally [11–13].
One example of this is the National Institute for Health Research (NIHR) in England where 10 million pounds was invested to establish nine collaboration units (Collaborations for Leadership in Applied Health Research and Care (CLAHRCs)) in 2008 aimed at engaging NHS staff to participate in research to improve patient outcomes [11, 12]. A number of funding structures have been put in place to support the integrated Knowledge Translation (iKT) research model in Canadian hospitals to increase researcher’s collaboration with ‘knowledge users’ (i.e. health care providers/users) to increase the generation of evidence that is more readily able to be implemented into practice [14]. In Australia, over $10 million was invested in building Advanced Health Research and Translation Centres (AHRTC) and Centres for Innovation in Regional Health (CIRHs) to facilitate collaboration between researchers, health care and industry stakeholders to undertake applied research directly relevant to improve patient care [13].
Identifying the research question
Although healthcare professionals, policy makers and the public at large recognise that research engagement by health care organisations is worthwhile, little is known about the evidence base surrounding research engagement and the type of strategies that have been used to facilitate increased research engagement. Previous reviews examining this have examined research engagement together with how to increase clinicians’ application of research in practice (i.e. implementation science). A review by Boaz et al. examined potential mechanisms between clinician engagement with research and improved health service and patient outcomes [6]. The review found that supporting clinicians to undertake research was a distinct behaviour from increasing clinicians’ implementation and multifaceted strategies are required to support research engagement, findings consistent with other reviews describing research co-production. For example, a review by Gagliardi et al. provides a summary of how integrated knowledge translation approaches have been applied to target decision makers’ engagement with research and described a range of individual and structural barriers and enablers that need to be targeted to support research engagement by health care organisations [15]. The previous reviews examining clinician research engagement specifically however have focused on describing the impact of capacity building strategies that target individual factors only [16, 17]. Our review seeks to extend on this literature by providing an overview of the different strategies that can be used to promote research engagement by health care providers [16]. In areas such as this where terminology, types of strategies and outcomes are unclear, an examination of the volume and characteristics of available research is needed to provide an overview of the evidence available to inform practice and policy making, and to assist in identifying gaps and areas for future research investment to increase health provider/ organisation research engagement [18]. Scoping reviews are recommended to provide an opportunity to clarify key concepts; describe gaps in the research; and characterise the types and sources of evidence to inform practice, policymaking and future research [18].
Objectives
As such, to identify gaps in the area and opportunities for further research, this study aimed to: i) describe the percentage, type and study design of publications that examined research engagement by health care providers and organisations and ii)provide a list of the types of strategies used to promote research engagement by health care professionals and organisations reported in the literature.
Methods
Study design
A scoping review using systematic search processes was undertaken to locate peer-reviewed publications and grey literature related to ‘research engagement by health care providers and organisations’. The manuscript was reported consistent with the PRISMA-ScR [19]. No protocol was registered; however a copy can be provided from the corresponding author upon request. The definition of research engagement applied in this study was informed by a comprehensive commissioned review undertaken by Hanney et al. (2013) which distinguishes between ‘engagement with research’ and ‘engagement in research’ with the former including a less substantial involvement at an organisational level and relating more to receiving and transmitting research findings, more conventionally known as knowledge translation or implementation (evidence-based practice) in the literature [8].
Similar to the review by Hanney et al., this study focused on ‘engagement in research’, defined as a ‘deliberate set of intellectual and practical activities undertaken by health care staff and organisations to conduct research’ [8]. This definition requires health care providers, services and organisations to have a more involved role in the entire research process including in its design, commissioning, conduct and dissemination [8].
This review applied methods consistent with the Cochrane Handbook for conduct of scoping reviews, and was based on the updated framework outlined by Peters et al. [20, 21]. This involved; i) identifying the research question; ii) identifying relevant studies; iii) study selection; iv) charting the data; and v) collating, summarizing and reporting results.
Systematic search processes and broad eligibility criteria were developed by the research team apriori, however consistent with recommendations for the conduct of scoping reviews, the search was supplemented with additional articles based on advice/recommendations from policy makers and experts in the field known to the research team, as well as additional grey literature searches using search terms identified from the initial electronic search (see Additional file 1).
Identifying relevant studies
A database search of electronic records was performed in the following electronic databases with no limit on date, MEDLINE (1950-); EMBASE (1947 -)’ PsycINFO (1950-); Academic Search Ultimate; CINAHL on the 27th December 2019.
As research engagement is not homogenously defined in the literature and consequently not always clearly indexed in electronic databases, the search strategy was developed based on extensive consultations and piloting of search terms with a university health systems librarian. The librarian, acting in line with Peer Review of Electronic Search Strategies (PRESS) 2015 Guidelines, assessed all aspects of the search terms, subject headings, search strings, limits and filters to ensure they were conceptually and functionally accurate in relation to the research question [22]. This strategy was adapted from that previously employed in a comprehensive review examining the association between research participation/engagement and health outcomes and refined to suit the purposes of this review [8]. The search strategy was kept intentionally broad, consisted of search terms for research engagement combined with search terms for health care providers/organisations. The reference list of all included studies were screened to identify further studies that could be relevant. Subsequently, a search of the grey literature using Google was undertaken using key terms identified from articles included from the electronic database search. Five separate searches were undertaken and included entering ‘research capacity building, collaborative activities/research, health research capacity strengthening and research engagement’ into the Google Scholar search engine and reviewing the first 100 hits in June 2019. Four policy makers and research experts provided additional articles that were relevant to the review aims.
Study selection
Inclusion and exclusion criteria
The main concepts of the review question which shaped the inclusion and exclusion criteria for the search can be found in Table 1.
Studies that examined research engagement were included regardless of study type. Articles not published in English were excluded from the study. Studies that examined appraising or applying the evidence solely without actual conduct of research, those that examined ‘how’ to move research into practice (i.e., implementation science) and dissemination of research findings exclusively, as well as those undertaken in non-health care settings/or with non-health care practitioners were excluded.
Screening
The search, screening and data charting processes were systematic and undertaken by two independent authors. Abstract and full text screening was undertaken independently by two authors (SY/KB/MF/AG/MK) using COVIDENCE [23]. Where there was disagreement, a third reviewer resolved any differences (LW). All studies regardless of study type were included as long as they explored research engagement (defined above).
Charting the data
Charting data from included publications was conducted according to the data classifications outlined below and consistent with previous studies [24–26].
A standardised data charting tool (see Additional file 2) was developed to chart the following additional information: author, year of publication, country where research was conducted (or first author affiliation if review), study design, study type, study setting and the detail of the intervention (verbatim from the text). A detailed instruction sheet with how to code each study was developed to ensure standardised data charting. All extraction were undertaken by two authors in Microsoft Excel, and all differences resolved via discussion (KB/SY/JW/CW).
Publication classification
All studies were categorised as either databased (i.e. data-driven, presenting data or new analysis of existing data relating to research engagement) or non-databased (i.e. not data-driven, no data or new analyses), as a means of differentiating between the different levels of evidence [27]. Databased publications were further classified according to study type, study design, translation levels and study setting.
Study type: Databased studies were further classified into quantitative or qualitative based on that reported by the authors. Where this was not explicitly described, we based this on the type of analysis used. Studies that used both quantitative and qualitative methods were classified as mixed methods. Databased studies were also categorised into measurement, descriptive or intervention research consistent with definitions from previous studies [24–28]. The following definitions were used:
-
1.
Measurement: Papers developed or examined the qualities of a measurement instrument such as reliability, validity, or acceptability. Data collection methods included the use of questionnaires, interviews, physiological assessments, risk screening and observations. Papers that focused on both measurement and descriptive issues were coded as measurement research.
-
2.
Descriptive: Papers exploring the frequency, patterns, correlates or predictors of research engagement strategies. These include epidemiological studies examining frequency or patterns of risk factors and correlates of research engagement.
-
3.
Intervention: Papers that tested the effectiveness of an intervention to increase research engagement and/or providers. Intervention publications will be defined by the research aims rather than the study design or type of intervention. Papers that focused on both descriptive and intervention issues will be classified as intervention research.
Non-databased articles were categorised as below consistent with previous studies [27]:
-
a
Discussion papers or commentaries: Editorials, comments, letters, news or interviews. These articles did not present original data or describe a specific research project or intervention.
-
b
Case reports: Articles in which the publication description indicated that it was a case report.
-
c
Program description: Descriptions of methods or processes undertaken for research engagement. This category included articles that described an intervention or health initiative being applied, or that had the potential to be applied, but in which no data-based evaluation was reported.
Study design: Those with an intervention focus were further classified according to the levels of evidence (including cross-sectional, case control, cohort studies, non-randomised controlled trial, quasi randomised controlled trial, and randomised controlled trial) [29].
Study setting: The study setting was recorded as either hospital(s) or a department within hospitals, community health settings, primary care, health care setting more broadly (not specific), and networks or collaborations at a national or international level or other.
Qualitative synthesis
To produce a list of strategies used to promote research engagement (i.e. research engagement strategies), we undertook a qualitative synthesis of data from databased intervention studies, and all non-databased studies, using a Framework Approach (FA) [30, 31]. This was undertaken on the narrative description of the research engagement strategies that were extracted verbatim from the relevant studies. The FA is a type of systematic, transparent qualitative content analysis composed of several inter-related stages that allow for a structured case- or theme-based analysis of data [30, 31]. FA is conducted by a team, where analysis is aided by collaborative development of highly structured outputs (charts/displays) providing an accessible visual reference that can be interpreted by people with little qualitative research experience [31]. Such qualitative methods of synthesising review findings have been recommended to generate broad findings/key themes and to highlight opportunities to advance the evidence-base [32, 33].
As part of this, the team (JW, KB, SY, CW) employed five stages of the analysis, including; 1) familiarisation with the data; 2) identification of recurrent and important themes; 3) coding; 4) grouping codes into an analytical framework; and 5) applying an analytical framework to data [31]. The entire process was facilitated by a skilled qualitative researcher (KB). The focus of the analysis was to produce descriptive accounts to answer predefined research questions (elements of research engagement strategies that are intended to, have been used to, or have been evaluated in the context of improving research engagement by health care providers and organisations). The analytical framework(s) emerging from the qualitative data analysis was intended to be pragmatic in nature, tailored to produce information that can be used to inform public health practice. Aligned with the project specifications and aims, we applied a positivist approach to qualitative synthesis, where we comprehensively searched for empirical findings and then accumulated and described these findings [32].
Results
Collating, summarising and reporting results of included studies
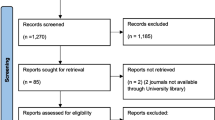
From the electronic search, 13,983 references were screened by two reviewers and 53 were identified through other sources. A total of 13,996 articles were screened after removal of duplications. A total of 271 articles were included in the full text screen and 152 were included in this study (see Fig. 1 for PRISMA diagram). This total included 107 from the database search, 40 searching from the grey literature included articles and and five based on expert recommendations, resulting in a total of 152 records for inclusion (see Fig. 1).

Flowchart outlining number of studies included at each review stage
A range of terminology was used to describe clinician and health care organisation research engagement including building research capacity, collaborative research, academic clinicians, building research infrastructure in health care, research participation, translational research, fostering clinician led research, exchanging knowledge, research networks, practice-research collaboration, integrated knowledge translation, research-based practice and research co-production.
Most studies were conducted in or had a first author located in the United States (n = 46), Australia (n = 41), the United Kingdom (including England, Ireland and Scotland, n = 36) and Canada (n = 17). The remaining were in New Zealand (n = 2), Norway (n = 1), Denmark (n = 1), the Netherlands (n = 1), Sweden (n = 1), Spain (n = 1), Switzerland (n = 1), France (n = 1), Ireland (n = 1), Japan (n = 1), and two in low to middle income countries.
Publication classifications
Of the 152 included records, 68 (44%) presented new, synthesised data (databased) and the remaining 84 (56%) were non-databased. Twenty-four studies were published before the year 2000, 46 were published between 2000 and 2009 and the remaining 82 were published after 2009 (2010–2019) (see Table 2).
-
i.
Study type
Of the databased articles (n = 68), 17 (25%) studies were mixed methods, 23 (34%) were qualitative and 28 (41%) were quantitative. The majority (n = 49, 72%) were categorised as descriptive studies, 17 were intervention studies (25%) and two were measurement studies (3%). Of the non-databased articles (n = 84), the majority (n = 46, 55%) were commentaries, one was a case study (1%) and the remainder were program descriptions (n = 37, 44%).
-
ii.
Study design
Of the 18 data based studies that were interventions, only two were controlled studies [74, 107] and one was a protocol of a controlled trial [142]. Nine studies were post-intervention, cross sectional assessments without control arms [34,35,36,37,38,39,40,41,42], five were prospective or retrospective cohorts, pre-post studies, or repeat cross sectional assessments [54,55,56,57,58].
-
iii.
Study setting and participants
Of the 68 databased articles, 29 studies were conducted either in hospital(s) or a department within a hospital, seven were in health care settings more broadly, four were in community health care settings, 16 explored networks (usually a collaboration of academic/health care partnerships and institutions), 11 were in primary care, and one in a university. There were a range of participants in these studies including Aboriginal Health Workers, nurses, midwives, physiotherapists, primary care practitioners, pharmacists, allied health practitioners, community health care workers and practitioners, clinicians and administrators within particular health systems or context (i.e. NHS, CLARHC), counsellors, ICU staff, multidisciplinary primary health care team and medical students.
Qualitative synthesis of strategies
Table 3 outlines the strategies identified in all studies that described an intervention (both databased and non-databased) and examples of suggested/actual application in practice. We identified and described eight categories of strategies: dual skilled team/staff, resources or physical infrastructures, incentive, leadership support of research, education/training, networks, forming partnerships or collaborations and overall leadership for entity.
Discussion
This scoping review sought to provide an overview of the existing research exploring strategies that have been suggested to improve provider and health care organisation’s engagement with research. This review found that over half of publications describing research engagement did not formally present any new data (non-databased and opinion pieces). Of the databased publications (those that formally presented new data), the majority were descriptive in nature largely providing evidence of the extent of the behaviour and association between strategies and research engagement. Our study found only two controlled trials evaluating the impact of research engagement strategies [74, 107]. Similarly, the review by Gagliardi et al. in 2015, also found only 13 studies, none were controlled studies, describing how iKT approaches have been operationalised and used to improve collaboration between researchers and decision makers in the research process [15]. Such findings are consistent with that of an emerging field, however, are of concern given significant resource investment by governments internationally to establish structures and implement strategies to build research leadership and capacity in health care organisations. For example, the NIH Roadmap allocated an initial $125 million in 2004, with planned increases to $2 billion in the later stages of implementation [186] where funds are distributed across developing new innovations, developing new models for research and increasing research translation.
Encouragingly, the percentage of databased and intervention studies appears to be increasing over time although the overall number is still small. Using a FA, we identified and described strategies that were suggested to be useful, or had been previously applied to increase clinician and health care organisations engagement with research, with the intent of providing a list of strategies that could be applied and evaluated in future studies. The research engagement strategies were described across eight categories targeting clinician, team, organisation and supra organisation factors [71]. Such strategies seek to target the broader determinant described by Gagliardi et al. and are consistent with that outlined in the research co-production literature [187], which suggests that interventions need to move beyond targeting just knowledge and skills of clinicians. Findings from this review also add to research capacity building frameworks for practitioners by describing the broader collaborative (e.g. networks), structural or workforce arrangements (e.g. clinician researchers) that could be put in place to support clinical research leadership [16]. Further intervention research is warranted targeting these eight distinct categories to better understand the impact of such strategies on increasing clinician research engagement. Additionally, a systematic review of the descriptive literature may also provide additional insights into the association of such strategies with engagement outcomes.
Our review highlights a mismatch between investment in research engagement strategies and the available evidence to support such strategies. While initiatives like the NIHR CLARHC provided significant opportunity and funding to embed a broad range of strategies to facilitate research co-production and clinician-led research, the impact these structures have on research engagement have yet to be examined [188]. Further, to our knowledge, there have been no controlled evaluations of multi-level formalised programs such as CLAHRC [188]. This may be due to the challenges with defining important outcomes of multi-level initiatives that account for the individualised approaches taken by different sites to contextualise the intervention. These non-controlled evaluations provide rich and important data to understand the factors [189] that facilitate implementation and the context in which these initiatives are delivered. However evidence from these non-controlled evaluations needs to be coupled with rigorous comparative evaluations to provide essential evidence for decision-making and to justify continued investments.
Strengths/limitation
This study used high quality, systematic processes to ensure that a broad range of studies examining research engagement were included. At least two screeners were included in each of the review processes. The use of structured qualitative processes to generate a list of strategies allowed for a broad examination of the types of strategies previously discussed or applied in research and practice, and enabled a collaborative analyses by researchers with varying degrees of qualitative research experience.
While a comprehensive search strategy consisting of a database search, search of the grey literature and consultations with experts in the field was used, it is possible that studies were missed due to inconsistent terminology and the rapidly progressing evidence-base. We excluded non-English studies and as such could have missed potentially relevant studies published in other languages. Nevertheless, this study to our knowledge provides a comprehensive overview of the characteristics of studies examining research engagement using high quality processes. This scoping review highlights that future empirical research is needed to identify the impact of such proposed strategies on health services, practice and patient outcomes.
Conclusions
This scoping review for the first time provides a list of research engagement strategies that have been proposed to be useful to increase clinicians and health care organisations collaboration in research activity. The majority of the evidence however has been descriptive in nature, providing limited empirical evidence to support the efficacy of research engagement strategies. There is a need for future research to progress beyond descriptive research to methodologically rigorous intervention research, to provide the evidence needed to inform decision making.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Pearson SD, Rawlins MD. Quality, innovation, and value for money: NICE and the British National Health Service. JAMA. 2005;294(20):2618–22.
Awad A, Trenfield SJ, Pollard TD, Ong JJ, Elbadawi M, McCoubrey LE, et al. Connected healthcare: Improving patient care using digital health technologies. Adv Drug Deliv Rev. 2021;178:113958.
Gould D, Berridge E-J, Kelly D. The National Health Service Knowledge and Skills Framework and its implications for continuing professional development in nursing. Nurse Educ Today. 2007;27(1):26–34.
Lyon AR, Lewis CC. Designing health information technologies for uptake: development and implementation of measurement feedback systems in mental health service delivery. Adm Policy Ment Health. 2016;43(3):344–9.
Wolfenden L, Williams CM, Kingsland M, Yoong SL, Nathan N, Sutherland R, et al. Improving the impact of public health service delivery and research: a decision tree to aid evidence-based public health practice and research. Aust N Z J Public Health. 2020;44(5):331–2.
Boaz A, Hanney S, Jones T, Soper B. Does the engagement of clinicians and organisations in research improve healthcare performance: a three-stage review. BMJ Open. 2015;5(12):e009415.
Bombard Y, Baker GR, Orlando E, Fancott C, Bhatia P, Casalino S, et al. Engaging patients to improve quality of care: a systematic review. Implement Sci. 2018;13(1):1–22.
Hanney S, Boaz A, Soper B, Jones T. Engagement in research: an innovative three-stage review of the benefits for health-care performance. Health Serv Delivery Res. 2013;1(8).
Clarke M, Loudon K. Effects on patients of their healthcare practitioner’s or institution’s participation in clinical trials: a systematic review. Trials. 2011;12(1):1–10.
Greenhalgh T, Jackson C, Shaw S, Janamian T. Achieving research impact through co-creation in community-based health services: literature review and case study. Milbank Q. 2016;94(2):392–429.
Collaborations for Leadership in Applied Health Research and Care. [Available from: http://www.nihr.ac.uk/files/pdfs/CLAHRC%20-%20Call%20for%20Proposals%20for%20Pilots.pdf.
NIHR Collaborations for Leadership in Applied Health Research and Care (CLAHRCs). [Available from: http://www.nihr.ac.uk/infrastructure/Pages/infrastructure_clahrcs.aspx.
Rapid Applied Research Translation initiative. [Available from: https://www.health.gov.au/initiatives-and-programs/rapid-applied-research-translation-initiative.
Guide to Knowledge Translation Planning at CIHR: Integrated and end-of-Grant Approaches. [Available from: https://cihr-irsc.gc.ca/e/45321.html.
Gagliardi AR, Berta W, Kothari A, Boyko J, Urquhart R. Integrated knowledge translation (IKT) in health care: a scoping review. Implement Sci. 2016;11(1):38.
Matus J, Walker A, Mickan S. Research capacity building frameworks for allied health professionals – a systematic review. BMC Health Serv Res. 2018;18(1):716.
Schneider M, van de Water T, Araya R, Bonini BB, Pilowsky DJ, Pratt C, et al. Monitoring and evaluating capacity building activities in low and middle income countries: challenges and opportunities. Glob Ment Health Camb. 2016;3:e29.
Wickremasinghe D, Kuruvilla S, Mays N, Avan BI. Taking knowledge users’ knowledge needs into account in health: an evidence synthesis framework. Health Policy Plan. 2015;31(4):527–37.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping Reviews (2020 version). 2020. In: JBI Manual for Evidence Synthesis. JBI. Available from: https://synthesismanual.jbi.global.
Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. 2020;18(10):2119–26.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–6.
Covidence systematic review software. Veritas Health Innovation. Melbourne, Australia. Available from www.covidence.org.
Metse AP, Wiggers JH, Wye PM, Wolfenden L, Prochaska JJ, Stockings EA, et al. Smoking and mental illness: a bibliometric analysis of research output over time. Nicotine Tob Res. 2016:ntw249.
Milat AJ, Bauman AE, Redman S, Curac N. Public health research outputs from efficacy to dissemination: a bibliometric analysis. BMC Public Health. 2011;11(1):934.
Wolfenden L, Milat AJ, Lecathelinais C, Sanson-Fisher RW, Carey ML, Bryant J, et al. What is generated and what is used: a description of public health research output and citation. Eur J Public Health. 2016;26(3):523–5.
Sanson-Fisher RW, Campbell EM, Htun AT, Bailey LJ, Millar CJ. We are what we do: research outputs of public health. Am J Prev Med. 2008;35(4):380–5.
Yoong SL, Jackson J, Barnes C, Pearson N, Swindle T, O’Reilly S, et al. Changing landscape of nutrition and dietetics research? A bibliographic analysis of top-tier published research in 1998 and 2018. Public Health Nutr. 2021;24(6):1318–27.
How to use the evidence: assessment and application of scientific evidence. [Available from: https://www.nhmrc.gov.au/sites/default/files/documents/reports/clinical%20guidelines/how-to-use-evidence-cp69.pdf.
Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117.
Ward DJ, Furber C, Tierney S, Swallow V. Using framework analysis in nursing research: a worked example. J Adv Nurs. 2013;69(11):2423–31.
Green J, Thorogood N. Qualitative Methods for Health Research, 4th Ed. Green J, Thorogood N, editors: Sage; 2018.
Marston C, King E. Factors that shape young people’s sexual behaviour: a systematic review. Lancet. 2006;368(9547):1581–6.
Abbott S, Gunnell C. Developing R&D capacity in primary care nursing: report of a research project. Primary Health Care Res Dev. 2005;6(2):95–100.
Akerjordet K, Lode K, Severinsson E. Clinical nurses' attitudes towards research, management and organisational resources in a university hospital: part 1. J Nurs Manag. 2012;20(6):814–23. https://doi.org/10.1111/j.1365-2834.2012.01477.x.
Albert NM, editor. Building and sustaining a hospital-based nursing research program. 1st ed. New York, USA: Springer Publishing Company; 2015.
Albert NM, Siedlecki SL. Developing and implementing a nursing research team in a clinical setting. J Nurs Adm. 2008;38(2):90–6. https://doi.org/10.1097/01.NNA.0000310714.30721.ca.
Alcock D. Research in clinical settings. Child Health Care. 1989;18(3):170–3. https://doi.org/10.1207/s15326888chc1803_8.
Armstrong AY, Decherney A, Leppert P, Rebar R, Maddox YT. Keeping clinicians in clinical research: the Clinical Research/Reproductive Scientist Training Program. Fertil Steril. 2009;91(3):664–6. https://doi.org/10.1016/j.fertnstert.2008.10.029. Epub 2009 Jan 14.
Aronson JK. How to attract, retain and nurture young academic clinicians. J R Soc Med. 2011;104(1):6–14.
Axon R, Leykum L, Wald H, Meltzer D. Results of a survey of academic hospitalist researchers. J Hosp Med. 2012;7:S80–S1.
Babl F, Borland M, Ngo P, Acworth J, Krieser D, Pandit S, Pitt WR, Cotterell E, Jamison S. Paediatric Research in Emergency Departments International Collaborative (PREDICT): first steps towards the development of an Australian and New Zealand research network. Emerg Med Australas. 2006;18(2):143–7. https://doi.org/10.1111/j.1742-6723.2006.00823.x.
Bacigalupo R, Cooke J, & Hawley M. Research activity, interest and skills in a health and social care setting, a snapshot of a primary care trust in northern England: Implications for collaboration and capacity. Primary Health Care Res Dev. 2006;7(1):68–77. https://doi.org/10.1191/1463423606pc265oa.
Bailey J, Veitch C, Crossland L, Preston R. Developing research capacity building for Aboriginal & Torres Strait Islander health workers in health service settings. Rural Remote Health. 2006;6(4):556. Epub 2006 Dec 21.
Bakken S, Lantigua RA, Busacca LV, Bigger JT. Barriers, enablers, and incentives for research participation: a report from the Ambulatory Care Research Network (ACRN). J Am Board Fam Med. 2009;22(4):436–45. https://doi.org/10.3122/jabfm.2009.04.090017.
Balakas K, Bryant T, Jamerson P. Collaborative research partnerships in support of nursing excellence. Nurs Clin North Am. 2011;46(1):123–8. https://doi.org/10.1016/j.cnur.2010.10.006.
Barnsteiner JH, Reeder VC, Palma WH, Preston AM, Walton MK. Promoting evidence-based practice and translational research. Nurs Adm Q. 2010;34(3):217–25. https://doi.org/10.1111/cts.1215010.1097/NAQ.0b013e3181e702f4.
Beeson T, Jester M, Proser M, Shin P. Engaging Community Health Centers (CHCs) in research partnerships: the role of prior research experience on perceived needs and challenges. Clin Transl Sci. 2014;7(2):115–20. https://doi.org/10.1111/cts.12150.
Berger J, Polivka B. Advancing Nursing Research in Hospitals Through Collaboration, Empowerment, and Mentoring. J Nurs Adm. 2015;45(12):600–5. https://doi.org/10.1097/NNA.0000000000000272.
Black AT, Bungay V, Mackay M, Balneaves LG, Garossino C. Understanding Mentorship in a Research Training Program for Point-of-Care Clinicians. J Nurs Adm. 2016;46(9):444–8. https://doi.org/10.1093/hsw/17.3.22310.1097/NNA.0000000000000373.
Blevins D, Farmer MS, Edlund C, Sullivan G, Kirchner JE. Collaborative research between clinicians and researchers: a multiple case study of implementation. Implement Sci. 2010;5:76.
Bogo M, Wells L, Abbey S, Bergman A, Chandler V, Embleton L, Guirgis S, Huot A, McNeill T, Prentice L, et al. Advancing social work practice in the health field: a collaborative research partnership. Health Soc Work. 1992;17(3):223–35. https://doi.org/10.1093/hsw/17.3.223.
Boydell K, Shaul RZ, D'Agincourt-Canning L, Da Silva M, Simpson C, Czoli CD, Rashkovan N, Kim CC, Levin AV, Schneider R. Paediatric physician-researchers: coping with tensions in dual accountability. Narrat Inq Bioeth. 2012;2(3):213–21. https://doi.org/10.1353/nib.2012.0060.
Bragg EJ, Meganathan K, Shay K, Gilman SC, Zeiss RA, Hettler DL. The impact of VA’s geriatric research, education and clinical centers on academic affiliates. Gerontol Geriatr Educ. 2011;32(1):5–21.
Brauer SG, Haines TP, Bew PG. Fostering clinician-led research. Aust J Physiother. 2007;53(3):143–4. https://doi.org/10.1016/s0004-9514(07)70020-x.
Brewer BB, Brewer MA, Schultz AA. A collaborative approach to building the capacity for research and evidence-based practice in community hospitals. Nurs Clin North Am. 2009;44(1):11–25, ix. https://doi.org/10.1016/j.cnur.2008.10.003.
Brown T. Collaborative research between clinicians and academics: Necessary conditions, advantages and potential difficulties. Aust Occup Ther J. 1994;41:19–26. https://doi.org/10.1111/j.1440-1630.1994.tb01807.x.
Bryar RM. Practitioner research: An approach to developing research capacity in primary care. NT Research. 2003;8(2):101–14. https://doi.org/10.1177/136140960300800204.
Bullock A, Morris ZS, Atwell C. Collaboration between health services managers and researchers: making a difference? J Health Serv Res Policy. 2012;17(2):2–10.
Bullock A, Morris ZS, Atwell C. Exchanging knowledge through healthcare manager placements in research teams. Serv Ind J. 2013;33(13–14):1363–80.
Callard F, Rose D, Wykes T. Close to the bench as well as at the bedside: involving service users in all phases of translational research. Health Expect. 2012;15(4):389–400. https://doi.org/10.1111/j.1369-7625.2011.00681.x. Epub 2011 May 25.
Castonguay LG, Locke BD & Hayes JA. The Center for Collegiate Mental Health: An Example of a Practice-Research Network in University Counseling Centers. J College Student Psychother. 2011;25:2:105–19. https://doi.org/10.1080/87568225.2011.556929.
Castonguay LG, Pincus AL, McAleavey AA. Practice research network in a psychology training clinic: building an infrastructure to foster early attachment to the scientific-practitioner model. Psychother Res. 2015;25(1):52–66. https://doi.org/10.1080/10503307.2013.856045. Epub 2013 Nov 27.
Chan R, Gardner G, Webster J & Geary A. Building research capacity in the nursing workforce: The design and evaluation of the nurse researcher role. Aust J Adv Nurs. 2010;27(4):62–9.
Chapman R, Combs S. Collaboration in the Emergency Department: an innovative approach. Accid Emerg Nurs. 2005;13(1):63–9. https://doi.org/10.1016/j.aaen.2004.10.012.
Chassie MB, Rosser D, Heaton SF, Norton MJ, Herman J. Collaboration to enhance research productivity: the Adjunct Nurse Researcher program. Nursingconnections. 1990 Winter;3(4):59-67.
Chester P, Kennedy E, Hynd S, Matthews DR. Clinical research networks in diabetes: the evolving role of the research nurse. Eur Diab Nursing. 2007;4(1):10–3. https://doi.org/10.1002/edn.69.
Cleary M, Hunt GE, Walter G, Jackson D. Fostering real-world clinical mental health research. J Clin Nurs. 2010;19(23-24):3453–8. https://doi.org/10.1111/j.1365-2702.2010.03487.x. Epub 2010 Oct 20.
Cluver J, Book S, Brady K, Back S, Thornley N. Engaging medical students in research: reaching out to the next generation of physician-scientists. Acad Psychiatry. 2014;38(3):345–9.
Cole DC, Boyd A, Aslanyan G, Bates I. Indicators for tracking programmes to strengthen health research capacity in lower-and middle-income countries: a qualitative synthesis. Health Res Policy Syst. 2014;12(1):1–13.
Cooke J. A framework to evaluate research capacity building in health care. BMC Fam Pract. 2005;6(1):1–11.
Cooke J, Sarre G. Building Health Research Capacity Through a Collaborative Network: The CLAHRC SY Experience. 3rd Annual Global Healthcare Conference (GHC 2014): GSTF; 2014. p. 17–9. https://doi.org/10.5176/2251-3833_GHC14.15.
Cooke J, Ariss S, Smith C, Read J. On-going collaborative priority-setting for research activity: a method of capacity building to reduce the research-practice translational gap. Health Res Policy Syst. 2015;13(1):25.
Corchon S, Portillo MC, Watson R, Saracíbar M. Nursing research capacity building in a Spanish hospital: an intervention study. J Clin Nurs. 2011;20(17–18):2479–89.
Currey J, Considine J, Khaw D. Clinical nurse research consultant: a clinical and academic role to advance practice and the discipline of nursing. J Adv Nurs. 2011;67(10):2275–83. https://doi.org/10.1111/j.1365-2648.2011.05687.x.
Currie G, Lockett A, El Enany N. From what we know to what we do: lessons learned from the translational CLAHRC initiative in England. J Health Serv Res Policy. 2013;18(3 Suppl):27–39. https://doi.org/10.1177/1355819613500484.
Dawson P. Realizing the imperative of clinical nursing research: the experiences of a collaborative research program in long-term care. Can J Nurs Res. 1998;30(2):125–34.
Denis JL, Lehoux P, Hivon M, Champagne F. Creating a new articulation between research and practice through policy? The views and experiences of researchers and practitioners. J Health Serv Res Policy. 2003;8 Suppl 2:44–50. https://doi.org/10.1258/135581903322405162.
DeVon HA, Patmon FL, Rosenfeld AG, Fennessy MM, Francis D. Implementing clinical research in the high acuity setting of the emergency department. J Emerg Nursing. 2013;39(1):6-12.
Dickinson H, Ledger J. Accelerating Research Translation in Healthcare: The Australian Approach. In: Denis J-L, Waring J, Dickinson H, editors. Organizational Behaviour in Health Care: Springer International Publishing; 2018. p. 201-16.
Downie J, Orb A, Wynaden D, McGowan S, Zeeman Z, Ogilvie S. A practice-research model for collaborative partnership. Collegian. 2001;8(4):27–32.
Dupin CM, Borglin G, Debout C, Rothan-Tondeur M. An ethnographic study of nurses' experience with nursing research and its integration in practice. J Adv Nurs. 2014;70(9):2128–39. https://doi.org/10.1111/jan.12371.
Ekeroma AJ, Kenealy T, Shulruf B, Nosa V, Hill A. Building Capacity for Research and Audit: Outcomes of a Training Workshop for Pacific Physicians and Nurses. J Educ Train Stud. 2015;3(4):179–92.
Ekeroma AJ, Shulruf B, McCowan L, Hill AG, Kenealy T. Development and use of a research productivity assessment tool for clinicians in low-resource settings in the Pacific Islands: a Delphi study. Health Res Policy Syst. 2016;14:9. https://doi.org/10.1186/s12961-016-0077-4.
Embi PJ, Payne PR. Evidence generating medicine: redefining the research-practice relationship to complete the evidence cycle. Med Care. 2013;51(8 Suppl 3):S87–91. https://doi.org/10.1097/MLR.0b013e31829b1d66.
Engler MB, Austin JK, Grady P. The National Institute of Nursing Research Graduate Partnerships Program (NINR-GPP): an opportunity for PhD students. Nurs Outlook. 2014;62(6):469–74. https://doi.org/10.1016/j.outlook.2014.08.009.
Farmer E, Weston K. A conceptual model for capacity building in Australian primary health care research. Aust Fam Physician. 2002;31(12):1139–42.
Fetherstonhaugh D, Nay R, Heather M. Clinical school partnerships: the way forward in nursing education, research and clinical practice. Aust Health Rev. 2008;32(1):121–6. https://doi.org/10.1071/ah080121.
Finch E, Cornwell P, Ward EC, McPhail SM. Factors influencing research engagement: research interest, confidence and experience in an Australian speech-language pathology workforce. BMC Health Serv Res. 2013;13:144.
Fitzgerald M, Milberger P, Tomlinson PS, Peden-Mcalpine C, Meiers SJ, Sherman S. Clinical nurse specialist participation on a collaborative research project: barriers and benefits. Clinical Nurse Specialist: J Adv Nurs Pract. 2003;17(1):44–9.
Friesen EL, Comino EJ, Reath J, Derrett A, Johnson M, Davies GP, et al. Building research capacity in south-west Sydney through a Primary and Community Health Research Unit. Aust J Prim Health. 2014;20(1):4–8.
Gagliardi AR, Perrier L, Webster F, Leslie K, Bell M, Levinson W, et al. Exploring mentorship as a strategy to build capacity for knowledge translation research and practice: protocol for a qualitative study. Implementation Science. 2009;4(1):55.
Gagliardi AR, Dobrow MJ. Identifying the conditions needed for integrated knowledge translation (IKT) in health care organizations: qualitative interviews with researchers and research users. 2016.
Giles G, Malin M, Harvey P. The Centre of Clinical Research Excellence In Aboriginal and Torres Strait Islander Health: An Operational Rationale and Some Reflections on Progress so far. Aust J Prim Health. 2006;12(2):97–104.
Gillibrand W, Burton C, Watkins G. Clinical networks for nursing research. Int Nurs Rev. 2002;49(3):188–93.
Govoni AL, Pierce LL. Collaborative research among clinical nurse specialists and staff nurses. J Continuing Educ Nurs. 1997;28(4):181–7.
Happell B. The Centre for Psychiatric Nursing Research and Practice: an innovative approach to enhancing clinical nursing research in the psychiatric/mental health field. Issues Ment Health Nurs. 2004;25(1):47–60.
Happell B. Clinical-academic partnerships research: converting the rhetoric into reality. Int J Psychiatr Nurs Res. 2005;11(1):1218–26.
Harrison R. Barriers and opportunities to developing research capacity in primary care trusts: The views of staff attached to a primary care trust. Prim Health Care Res Dev. 2005;6(3):185–9.
Hauck YL, Lewis L, Bayes S, Keyes L. Research capacity building in midwifery: Case study of an Australian Graduate Midwifery Research Intern Programme. 2015. p. 259–63.
Heinemann A. Metrics of Rehabilitation Research Capacity. Am J Phys Med Rehabil. 2005;84(12):1009–19.
Heintzman J, Gold R, Krist A, Crosson J, Likumahuwa S, DeVoe JE. Practice-based research networks (PBRNs) are promising laboratories for conducting dissemination and implementation research. J Am Board Fam Med. 2014;27(6):759–62.
Henderson A, Winch S, Holzhauser K. Leadership: the critical success factor in the rise or fall of useful research activity. J Nurs Manag. 2009;17(8):942–46.
Hinchcliff R, Greenfield D, Braithwaite J. Is it worth engaging in multi-stakeholder health services research collaborations? Reflections on key benefits, challenges and enabling mechanisms. Int J Qual Health Care. 2014;26(2):124–8.
Hiscock H, Ledgerwood K, Danchin M, Ekinci E, Johnson E, Wilson A. Clinical research potential in Victorian hospitals: the Victorian clinician researcher needs analysis survey. Internal Med J. 2014;44(5):477-82.
Hoeijmakers M, Harting J, Jansen M. Academic Collaborative Centre Limburg: A platform for knowledge transfer and exchange in public health policy, research and practice? Health Policy. 2013;111(2):175–83.
Holden L, Pager S, Golenko X, Ware RS, Weare R. Evaluating a team-based approach to research capacity building using a matched-pairs study design. BMC Fam Pract. 2012;13(1):1–10.
Holden L, Pager S, Golenko X, Ware R. Validation of the research capacity and culture (RCC) tool: measuring RCC at individual, team and organisation levels. Aust J Prim Health. 2012;18(1):62-7.
Holge-Hazelton B, Kjerholt M, Berthelsen C, Thomsen T. Integrating nurse researchers in clinical practice-A challenging, but necessary task for nurse leaders. J Nurs Manag. 2016;24(4):465-74.
Hopps L. The development of research in nursing in the United Kingdom. J Clin Nurs. 1994;3(4):199-204.
Hulcombe J, Sturgess J, Souvlis T, Fitzgerald C. An approach to building research capacity for health practitioners in a public health environment: an organisational perspective. Aust Health Rev. 2014;38(3):252-58.
Hurst K. Building a research conscious workforce. J Health Organ Manag. 2003;17(5):373-84.
Ishiguro A, Sasaki H, Yahagi N, Kato H, Kure S, Mori R. Needs assessment for collaborative network in pediatric clinical research and education. Pediatr Int. 2017;59(1):74-9.
Jackson C, Butterworth T. Every-one's business, no-one's responsibility: Reporting clinical academic research activity by nurses in the United Kingdom. J Res Nurs. 2007;12(3):2013-223.
Jackson C, Greenhalgh T. Co-creation: a new approach to optimising research impact? MJA. 2015;7:283-4.
Jamerson PA, Fish AF, Frandsen G. Nursing Student Research Assistant Program: A strategy to enhance nursing research capacity building in a Magnet status pediatric hospital. Appl Nurs Res. 2011;24(2):110-3.
Jamerson PA, Vermeersch P. The Role of the Nurse Research Facilitator in Building Research Capacity in the Clinical Setting. J Nurs Adm. 2012;42(1):21-7.
Janssen J, Hale L, Mirfin-Veitch B, Harland T. Building the research capacity of clinical physical therapists using a participatory action research approach. Phys Ther. 2013;93(7):923–34.
Jennings G, Walsh M. Integrated health research centres for Australia. MJA. 2013;5:320-21.
Johnson C, Lizama C, Harrison M, Bayly E, Bowyer J. Cancer health professionals need funding, time, research knowledge and skills to be involved in health services research. J Cancer Educ. 2014;29(2):389-94.
Jordan M, Rowley E, Morriss R, Manning N. An analysis of the Research Team-Service User relationship from the service user perspective: A consideration of 'The Three Rs' (Roles, Relations, and Responsibilities) for healthcare research organisations. Health Expect. 2015;18(6):2693-703.
Joubert L, Hocking A. Academic Practitioner Partnerships: A Model for Collaborative Practice Research in Social Work. Australian Social Work. 2015;68(3):352-63.
Jowett S, Macleod J, Wilson S, Hobbs F. Research in primary care: extent of involvement and perceived determinants among practitioners from one English region. Br J Gen Pract. 2000;50:387-89.
Keefe M, Pepper G, Stoner M. Toward research-based nursing practice: the Denver Collaborative Research Network. Appl Nurs Res. 1988;1(3):109-15.
Keenan S, Martin C, Kossuth M, Jennifer D., Eberhard J, Sibbald WJ. The Critical Care Research Network: a partnership in community-based research and research transfer. J Eval Clin Pract. 2000;6(1):15-22.
Koerner K, Castonguay L. Practice-oriented research: What it takes to do collaborative research in private practice. Psychother Res. 2014;25(1):67-83.
Kuehnle K, Winkler DT, Meier-Abt P. Swiss national MD-PhD program: An outcome analysis Swiss Medical Weekly. 2009;189(37-38):540-46.
Lach P, Reifler C. On doing research in a clinical setting. J Am Coll Health Assoc. 1980;29(3):154-5.
Ledley F, J. L, H. F. Factors Influencing the Interests, Career Paths, and Research Activities of Recent Graduates From an Academic, Pediatric Residency Program. Pediatrics. 1993;92(3):436
LeGris J, Weir R, Browne G, Gafni A, Stewart L, Easton S. Developing a model of collaborative research: the complexities and challenges of implementation. Int J Nurs Stud. 2000;37(1):65-79.
Lester HE, Carter YH, Dassu D, Hobbs FD. Survey of research activity, training needs, departmental support, and career intentions of junior academic general practitioners. Br J Gen Pract. 1998;48(431):1322-6.
Long JC, Cunningham FC, Carswell P, Braithwaite J. Patterns of collaboration in complex networks: the example of a translational research network. BMC Health Serv Res. 2014;14:225.
Loomis ME, Krone KP. Collaborative research development. J Nurs Adm. 1980;10:32-5.
MacPhee M. Developing a practice-academic partnership logic model. Nursing Outlook. 2009;57(3):143–47.
Mainous A, Hueston W. Characteristics of community-based primary care physicians participating in research. J Fam Pract. 1995;40(1):51–6.
Mays GP, Hogg RA, Castellanos-Cruz DM, Hoover AG, Fowler LC. Public health research implementation and translation: evidence from practice-based research networks. Am J Prev Med. 2013;45(6):752–62.
McAleavey AA, Lockard AJ, Castonguay LG, Hayes JA, Locke BD. Building a practice research network: obstacles faced and lessons learned at the Center for Collegiate Mental Health. Psychother Res. 2015;25(1):134–51.
McIntyre E, Brun L, Cameron H. Researcher development program of the primary health care research, evaluation and development strategy. Aust J Prim Health. 2011;17(1):114–21.
McKee G, Codd M, Dempsey O, Gallagher P, Comiskey C. Describing the implementation of an innovative intervention and evaluating its effectiveness in increasing research capacity of advanced clinical nurses: using the consolidated framework for implementation research. BMC Nurs. 2017;16(1):1–13.
McWilliam CL, Desai K, Greig B. Bridging town and gown: building research partnerships between community-based professional providers and academia. J Prof Nurs. 1997;13(5):307–15.
Miller J, Bryant MacLean L, Coward P, Broemeling AM. Developing strategies to enhance health services research capacity in a predominantly rural Canadian health authority. Rural Remote Health. 2009;9(4):1266.
Misso ML, Ilic D, Haines TP, Hutchinson AM, East CE, Teede HJ. Development, implementation and evaluation of a clinical research engagement and leadership capacity building program in a large Australian health care service. BMC Med Educ. 2016;16(1):1–9.
Mitchell K, Baillie L, Phillips N. Increasing nurse and midwife engagement in research activity. Nurs Stand. 2015;29(23):37–42.
Moore A. Research, the collaborative approach: Clinicians and academics. Physiother. 1997;83(5):229–34.
Morris K, Smyth G. A survey of research capacity and partnerships among mental health occupational therapists in the UK. Ment Health Rev J. 2017;22(2):136–47.
Mortenius H, Baigi A, Palm L, Fridlund B, Bjorkelund C, Hedberg B. Impact of the organisational culture on primary care staff members' intention to engage in research and development. J Health Organ Manage. 2015;29(2):234–51.
Murphy M, Staffileno B, Carlson E. Collaboration among DNP- and PhD-prepared nurses: Opportunity to drive positive change. J Prof Nurs. 2015;31(5):388–94.
Naik AD, Lawrence B, Kiefer L, Ramos K, Utech A, Masozera N, et al. Building a primary care/research partnership: lessons learned from a telehealth intervention for diabetes and depression. Fam Pract. 2015;32(2):216–23.
Nelson P, Holland D, Derscheid D, Tucker S. Clinical nurse specialist influence in the conduct of research in a clinical agency. Clinical Nurse Specialist: J Advanced Nurs Pract. 2007;21(2):95–100.
Nichols R, Meyer J, Batehup L, Waterman H. Promoting action research in healthcare settings. Nurs Stand. 1997;11(40):36–8.
Norton C. Supporting MCRN research through improving clinical trial delivery by hospital pharmacies. Arch Dis Child. 2011;96(4):e1.
Norman EM. Research Collaboration Between Staff Nurses and a University Professor. Orthop Nurs. 1987;6(5):16–9.
Nutting P. Practice-Based Research Networks: Building the Infrastructure of Primary Care Research. J Fam Pract. 1996;42(2):199–203.
Pager S, Holden L, Golenko X. Motivators, enablers, and barriers to building allied health research capacity. J multidisciplinary Healthc. 2012;5:53–9.
Paget SP, Lilischkis KJ, Morrow AM, Caldwell PHY. Embedding research in clinical practice: differences in attitudes to research participation among clinicians in a tertiary teaching hospital. 2014. p. 86–9.
Paget S, Caldwell P, Murphy J, Lilischkis K, Morrow A. Moving beyond 'not enough time': factors influencing paediatric clinicians' participation in research. Intern Med J. 2017;47(3):299–306.
Perron M, Nadeau S, Dubé F. Involvement of paramedical clinicians in research: A must for improving clinical practices. Ann Phys Rehabil Med. 2016;59:e49.
Pikethly M, Sullivan F. Four years of TayRen, a primary care research and development network. Prim Health Care Res Dev. 2003;4(4):279–83.
Pomeroy V, Tallis R, Stitt E. Dismantling some barriers to evidenced-based rehabilitation with ‘hands-on’clinical research secondments: initial development. Physiotherapy. 2003;89(5):266–75.
Queensland Health. Impact of a Research Capacity Building Initiative: Qualitative Evaluation of HP Research Positions. Prepared by Dr Rachel Wenke and Prof. Sharon Mickan. State of Queensland (Queensland Health); 2016.
Rait G, Rogers S, Wallace P. Primary care research networks: perspectives, research interests and training needs of members. Prim Health Care Res Dev. 2002;3(1):4–10.
Reay H, Sears J. A collaborative model for training clinical research staff. Nurs Manag. 2013;20(3):22–7.
Redman-MacLaren ML, MacLaren DJ, Solomon J, Muse A, Asugeni R, Harrington H, et al. Research workshop to research work: initial steps in establishing health research systems on Malaita, Solomon Islands. Health Res Policy Syst. 2010;8(1):1–7.
Reijneveld S. The practising public health researcher. Eur J Public Health. 2009;19(2):130.
Rickels K, Hesbacher P, Fisher E, Norstad N. The Private Practice Research Group (PPRG): A Working Model from Psychopharmacology for Clinical Research in Family Practice. J Clin Pharmacol. 1977:541–54.
Ried K, Fuller J. Building a culture of research dissemination in primary health care: the South Australian experience of supporting the novice researcher. Aust Health Rev. 2005(1):6.
Rosenberg L. The physician-scientist: An essential — and fragile — link in the medical research chain. J Clin Invest. 1999;103(12):1621–26.
Sahs J, Nicasio A, Storey J, Guarnaccia P, Lewis-Fernandez R. Developing research collaborations in an academic clinical setting: Challenges and lessons learned. Community Ment Health J. 2016;53(6):647–60.
Schwartz MA. Are Academic Pharmacists Meeting the Clinical Scientist Role? Drug Intell Clin Pharm. 1987;21(2):114–7.
Short A, Jackson W, Nugus P. Expanding clinical research capacity through a community of practice (CoPER). Nurse Educ Pract. 2010;10:52–6.
Short A, Holdgate A, Ahern N, Morris J. Enhancing research interest and collaboration in the interdisciplinary context of emergency care. J Interprof Care. 2009;23(2):156–68.
Skinner E, Williams C, Haines T. Embedding research culture and productivity in hospital physiotherapy departments: challenges and opportunities. Aust Health Rev. 2015;39:312–14.
Smolowitz J, Murray M. Nursing research activities in New York state are alive and well: a survey of selected acute care facilities and schools of nursing. J N Y State Nurses Assoc. 1997;28(3):20–3.
Soper B, Hinrichs S, Drabble S, Yaqub O, Marjanovic S, Hanney S, et al. Delivering the aims of the Collaborations for Leadership in Applied Health Research and Care: understanding their strategies and contributions. 2015.
Stiller K, Haensel N. An initiative to build research capacity within a physiotherapy department: hits and misses over a 20-year period. Internet J Allied Health Sci Pract. 2016;14(4):Article 1.
Stockton R, Morran K. Reflections on practitioner-researcher collaborative inquiry. Int J Group Psychother. 2010;60(2):295–305.
Tanner J, Hale C. Research-active nurses' perceptions of the barriers to undertaking research in practice. NT Res. 2002;7(5):363–75.
Teal R, Bergmire D, Johnston M, Weiner B. Implementing community-based provider participation in research: an empirical study. Implementation Sci. 2012;7:41.
The Academy of Medical Sciences. Strengthening Clinical Research: A report from the Academy of Medical Sciences. 2003.
Tierney A, Taylor J. Research in practice: an 'experiment' in researcher-practitioner collaboration. J Adv Nurs. 1991;16(5):506–10.
Walshe K, Davies H. Health research, development and innovation in England from 1988 to 2013: from research production to knowledge mobilization. J Health Serv Res Policy. 2013;18(3):1–12.
Willson D, Dean J, Meert K, Newth C, Anand K, Berger J, et al. Collaborative pediatric critical care research network: looking back and moving forward. Pediatr Crit Care Med. 2010;11(1):1–6.
Wolfenden L, Yoong S, Williams C, Grimshaw J, Durrheim D, Gillham K, et al. Embedding researchers in health service organizations improves research translation and health service performance: the Australian Hunter New England Population Health example. J Clin Epidemiol. 2017;85:3–11.
Woolf SH. The Meaning of Translational Research and Why It Matters. JAMA. 2008;299(2):211–3.
Yawn B. What Does It Mean to Build Research Capacity? Fam Med. 2002;34(9):678–84.
Check E. NIH “roadmap” charts course to tackle big research issues. Nature. 2003;425:438.
Smith H, Budworth L, Grindey C, Hague I, Hamer N, Kislov R, et al. Co-production practice and future research priorities in United Kingdom-funded applied health research: a scoping review. Health Res Policy Syst. 2022;20(1):36.
Kislov R, Wilson PM, Knowles S, Boaden R. Learning from the emergence of NIHR Collaborations for Leadership in Applied Health Research and Care (CLAHRCs): a systematic review of evaluations. Implement Sci. 2018;13(1):111.
Harvey G, Fitzgerald L, Fielden S, McBride A, Waterman H, Bamford D, et al. The NIHR collaboration for leadership in applied health research and care (CLAHRC) for Greater Manchester: combining empirical, theoretical and experiential evidence to design and evaluate a large-scale implementation strategy. Implement Sci. 2011;6(1):96.
Acknowledgements
The authors wish to thank Librarian Debbie Booth for conducting the literature search and Courtney Barnes and Melanie Lum for assistance with screening.
Funding
SLY is a postdoctoral research fellow funded by an Australian Research Council Discovery Early Career Researcher Award (DE170100382). LW is a Hunter New England Clinical Research Fellow and is supported by a National Health and Medical Research Leadership fellowship.
Author information
Authors and Affiliations
Contributions
SY and JW conceptualised the review. SY, KB, MF, AG and MK conducted the abstract and full text screening. LW resolved any differences during screening. Data extraction was conducted by KB, SY, JW and CW. Drafting of the manuscript was conducted by SY, JW and KR with all authors contributing to and reviewing the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Electronic search strategy applied for the search.
Additional file 2.
Data extraction form.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yoong, S.L., Bolsewicz, K., Reilly, K. et al. Describing the evidence-base for research engagement by health care providers and health care organisations: a scoping review. BMC Health Serv Res 23, 75 (2023). https://doi.org/10.1186/s12913-022-08887-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-08887-2