
Abstract
Background
This study aims to assess the health literacy of medical patients admitted to hospitals and examine its correlation with patients’ emergency department visits, hospital readmissions, and durations of hospital stay.
Methods
This prospective cohort study recruited patients admitted to the general internal medicine units at the two urban tertiary care hospitals. Health literacy was measured using the full-length Test of Functional Health Literacy in Adults. Logistic regression analyses were performed to examine the correlation between health literacy and the desired outcomes. The primary outcome of interest of this study was to determine the correlation between health literacy and emergency department revisit within 90 days of discharge. The secondary outcomes of interest were to assess the correlation between health literacy and length of stay and hospital readmission within 90 days of discharge.
Results
We found that 50% had adequate health literacy, 32% had inadequate, and 18% of patients had marginal health literacy. Patients with inadequate health literacy were more likely to revisit the emergency department as compared to patients with adequate health literacy (odds ratio: 3.0; 95% Confidence Interval: 1.3–6.9, p = 0.01). In patients with inadequate health literacy, the mean predicted probability of emergency department revisits was 0.22 ± 0.11 if their education level was some high school or less and 0.57 ± 0.18 if they had completed college. No significant correlation was noted between health literacy and duration of hospital stay or readmission.
Conclusions
Only half of the patients admitted to the general internal medicine unit had adequate health literacy. Patients with low health literacy, but high education, had a higher probability of emergency department revisits.
Similar content being viewed by others


Background
Health literacy is the ability of an individual to effectively use their reading, writing, verbal, and numerical skills to contribute to their personal healthcare positively [1, 2]. An individual’s health literacy skills are crucial for health-related decisions. Health literacy is described as “personal knowledge and competencies which enable people to access, understand, appraise, and use information and services in ways which promote and maintain good health and wellbeing for themselves and those around them” [3]. It is essential that patients and their families are able to “... obtain, process, and understand [the] basic health information and services needed to make appropriate health decisions to manage their health.” More than 43 million people in the United States have inadequate health literacy, and nearly half of the adult Canadians have literacy skills below a high school level, affecting their ability to function [4,5,6,7,8].
The relationship between eudcation and health literacy is not well understood. Education has been suggested to be a key factor for adequate health literacy and thereby good health [9, 10]. Evidence shows that people with lower education have lower health literacy skills as compared to people with higher education. Nevertheless, health literacy and general literacy are not identical concepts. Inadequate health literacy is not uncommon among patients with a high level of education [10]. General literacy does not provide all the skills required to manage and communicate critical health information and concerns [11, 12]. Evidence supports an incongruity between the average reading ability of patients and their ability to interpret and comprehend health information, as when managing health and complex diseases, patients require more than the ability to read and manipulate numbers [13].
Inadequate health literacy is recognized as a stronger predictor of poor health than age, income, employment status, education level, or race [14]. It has been found that people with inadequate health literacy often have difficulty understanding prescription labels, participating in medical decisions, following medical recommendations, and attending their follow-up appointments [15, 16]. Individuals with inadequate or marginal health literacy often struggle with poor self-care behaviors, receive fewer preventive measures, and have increased all-cause mortality [17,18,19,20,21,22,23]. Williams et al. showed that a quarter of the patients visiting the emergency department had inadequate health literacy, and one-third did not understand how many pills should be taken in their prescription [15]. Inadequate health literacy affects the use of health services and impacts patient satisfaction and the physician–patient relationship [24]. Furthermore, inadequate health literacy is one of the key barriers in the delivery of effective healthcare and quality outcomes [25]. Low health literacy is considered a key source of economic inefficiency in the U.S. healthcare system [25, 26]. It is estimated that inadequate health literacy adds additional 106 to $238 billion cost to the health care system representing 7–17% of all personal healthcare expenditures [26].
People with inadequate health literacy may utilize more resources through more frequent use of inpatient and emergency department visits and have higher care costs with poorer health outcomes. A systematic review examined health literacy in emergency departments and found that a substantial portion of emergency patients does not have adequate health literacy [27]. Howard et al. found an increase in emergency department use and higher costs for patients with inadequate health literacy (as compared to those with adequate literacy) after controlling for age, sex, race or ethnicity, income, education, health behaviors, and chronic conditions [28].
Despite the negative implications of low health literacy, physicians are typically unaware of their patients’ health literacy levels and its subsequent effects on their patients’ outcomes [29]. Health literacy is not routinely evaluated or recorded in patients’ medical records and administrative data. However, health literacy can be an important indicator in evaluating patients’ risks of poor outcomes after hospital discharge and improving patient-physician communication [30].
Most of the studies that have assessed outcomes of patients with inadequate health literacy were performed either in the emergency department or in outpatient settings. Therefore, current knowledge of the outcomes of inadequate health literacy in hospitalized patients with multiple comorbid conditions is limited. This study aims to assess the health literacy of patients admitted to a hospital general medical unit and examine its correlation with emergency room visits, readmissions, and duration of hospital stay.
Methods
Setting and study participants
This study was approved by the University of Saskatchewan Research Ethics Board (Bio#308). This prospective cohort study was conducted in the two urban tertiary care hospitals in Saskatoon, Canada. Based on the assumption that approximately 50% patients will have inadequate or marginal health literacy and about 10% pateints will loss to follow up we estimated a smple size of 150 patients with an alpha error of 0.05 with a 2-sided p value. This sample size was felt to have adequate power for subgroups analysis. Adult patients admitted to the hospitals’ general internal medicine units were enrolled in the study after written informed consent was obtained. Research assistants recruited patients over the period of June–September 2019. Patients who could read, write, speak English, and were 18 years and older were eligible for enrollment in this study. Patients with known diagnoses of dementia were excluded. Participating patients had their visual acuity checked using a pocket Snellen chart to ensure their ability to complete the assessment.
Data collection instrument
Health literacy was measured using the full-length Test of Functional Health Literacy in Adults (TOFHLA). The TOFHLA was developed and validated as a measure of functional health literacy used by healthcare providers and researchers [31]. This tool measures health literacy on the assumption that more than general literacy is necessary to understand and negotiate healthcare systems adequately. We used the full-length TOFHLA as it provides richer information about the levels of functioning. It is also recommended to use the full-length TOFHLA when health literacy is used as a dependent or independent variable in research [31]. A license was obtained to reproduce the TOFHLA for use in research from Peppercorn Book and Press Inc.
The TOFHLA assesses an individual’s numeracy and reading comprehension. In this context, numeracy is defined as a patient’s ability to understand and act on numerical directions given by healthcare providers or pharmacists, and reading compression is defined as a patient’s ability to read passages using actual materials from healthcare settings. The test takes 10–20 minutes to complete. The TOFHLA assigns scores into three groups of health literacy: adequate, marginal, and inadequate. An adequate score ranges from 75 to 100 and indicates that patients should be able to read, understand, and interpret most health care texts; a marginal score ranges from 60 to 74 and indicates that patients will have difficulty reading and interpreting health texts; an inadequate score ranges from 0 to 59 and indicates that patients will have difficulty reading, understanding, and interpreting most health materials.
The primary outcome of interest of this study was to determine the correlation between health literacy and emergency department revisit within 90 days of discharge. The secondary outcomes of interest were to assess the correlation between health literacy and length of stay and hospital readmission within 90 days of discharge. Hospital readmission was defined as any admission, for any cause, to either of the two study hospitals within 90 days after discharge from an index hospitalization. If a patient had a subsequent admission after their emergency department revisit, that emergency department revisit was not included in the analysis. We included measures of whether a patient had readmission (yes or no) and the total number of readmissions experienced within 90 days post-discharge. We categorized readmissions into no readmission and ≥ 1 readmission. Similarly, we categorized emergency department revisit within 90 days after discharge into no revisit and ≥ 1 revisit. Length of stay was kept as a continuous variable in days. All eligible patients close to their discharge from a medical unit were provided with the full-length TOFHLA. Patients were prospectively followed, and the length of their hospital stay was recorded. Data for hospital readmissions and emergency department revisits was obtained from the Discharge Abstract Database (DAD) and National Ambulatory Care Reporting System (NACRS).
The following covariates were examined: age groups (< 65 and ≥ 65 years old); sex (male or female); employment status (disabled or injured, retired, and other); household income, marital status; education (some high school or less, completed high school, some college, and complete college); and Charleston Comorbidity Index (CCI).
Statistical analysis
Data were analyzed using SPSS (Version 26.0, IBM, Armonk, NY, USA) and Stata 13 (Stata Corp, College Station, TX, USA). Descriptive data were presented for patient demographics, health literacy levels’ hospital readmissions, emergency department revisits, and length of stay, including medians with interquartile range values, frequencies, and proportions where applicable. Multivariate logistic regression was performed to examine whether health literacy affects a patient’s emergency department revisits and hospital readmissions, controlling for other possible confounders. Multiple linear regression modeling was conducted after log-transforming to examine the length of stay variable.
Bivariate analyses were conducted first, retaining variables significant at the 0.2 alpha level when modeled alone and with an alpha less than 0.05 in the final multivariate models. In the multivariate levels, interactions among independent variables and covariates were examined. If interaction effects were present, the mean predicted probabilities with their standard deviation were calculated. A two-sided p < 0.05 was considered to be significant.
Patient and public involvement
Patients were not involved.
Results
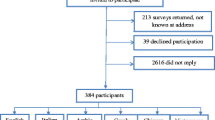
A total 174 (63%) of 278 eligible patients were consented to be interviewed (Fig. 1). Patient’s characteristics are described in Table 1. In multivariate analysis 7 (4%) patients were excluded due to missing data on length of stay, ER revisits and hospital readmissions. Overall, 46% were men and 54% were women (ratio men/women = 1:1.2). Out of the study population, only 50% of patients had adequate health literacy, 32 and 18% of patients had inadequate and marginal health literacy, respectively. Of the men, 30.4% had inadequate health literacy, 19.0% had marginal health literacy, and 50.6% had adequate health literacy; however, of the women, 33.0% had inadequate health literacy, 17.0% had marginal health literacy, and 50% had adequate health literacy.

Flow chart showing eligible patients
Older patients had a significantly higher rate of inadequate health literacy compared to younger patients. In patients over 65 years of age, 45.6% had inadequate health literacy, 22.8% had marginal health literacy, and 31.7% had adequate health literacy; however, in patients under 65 years of age, 20% had inadequate health literacy, 14.4% had marginal health literacy, and 65.6% had adequate health literacy (p < 0.05).
Only 24% of patients had full-time employment. Overall, 26.8% of patients who were full-time employed had inadequate or low health literacy as compared with 51.4% of patients who were disabled (< 0.5). Likewise, 64.9% of patients with no income or annual income below $20,000 had inadequate or low health literacy compared with 25% of patients with an annual income of $75,000 or greater (< 0.05). Of all patients, 37% received some high school or less education, 19% completed high school, 13% received some college education, and 31% completed college. In patients who received some high school or less education, 56.3% had inadequate health literacy, 18.8% had marginal health literacy, and 18.4% had adequate health literacy (p < 0.05). In patients who completed a college education, 13.0% had inadequate health literacy, 14.8% had marginal health literacy, and 72.2% had adequate health literacy (p < 0.05).
Overall, 23% of the patients revisited the emergency department, and 30% required readmission to the hospital at least once within 90 days after their discharge (Table 2). Characteristics of patients who revisited the emergency department are described in Table 3.
In univariate analysis, patients who had inadequate and marginal health literacy were more likely to revisit the emergency department as compared to patients with adequate health literacy; the odds ratio (OR) for inadequate health literacy was 3.0 (95% Confidence Interval [CI]: 1.3–6.89, p = 0.01), whereas the OR for emergency department revisit for marginal health literacy was 2.28 (95% CI: 0.82–6.32, p = 0.11) (Table 4).
The final model for multivariate analysis was adjusted for education, age, sex, CCI, and marital status. In multivariate analysis, the test for interaction between health literacy and education status was positive. Therefore, mean predicted probabilities and standard deviations were calculated on the interaction between health literacy and education status.
In patients with inadequate health literacy, the mean predicted probability (±SD) of emergency department revisit was 0.22 ± 0.11 if they had received some high school or less education and 0.57 ± 0.18 if they had completed a college (Table 5). In other words, in patients with inadequate health literacy, two of ten with no college education and six of ten with a college education, revisited the emergency department within 90 days of their discharge. In patients with marginal health literacy, the mean predicted probability (±SD) of revisiting the emergency department was 0.25 ± 0.08 if they had completed some high school or less education and 0.15 ± 0.08 if they had completed a college. In patients with adequate health literacy, the mean predicted probability (±SD) of revisiting the emergency department was 0.24 ± 0.12 if they had received some high school and or less education and 0.10 ± 0.04 if they had completed college.
In the univariate analysis of all patients who had at least one hospital readmission, 40% had marginal health literacy, 22% had inadequate health literacy, and 38% had adequate health literacy; however, this was not statistically significant (p = 0.115).
The median duration of hospital stay was 9 days. Patients with inadequate health literacy had a median duration of hospital stay of 12.5 days, while patients with marginal and adequate health literacy had median durations of 13 days and 7.5 days (p > 0.05), respectively. Regarding the length of stay, in univariate regression analysis, the average duration was higher for patients with marginal and inadequate health literacy; however, this was not statistically significant.
Discussion
Our findings indicate a low rate of adequate health literacy in hospitalized patients in medical units. Only about 50% of hospitalized patients had adequate health literacy, suggesting that almost half of the hospitalized patients in medical units have difficulty reading, understanding, and interpreting healthcare information. Patients with inadequate health literacy were more likely to revisit the emergency department as compared to patients with adequate health literacy. Patients with low health literacy, but high education, had a higher probability of emergency department revisits. No significant correlation was noted between health literacy and duration of hospital stay or readmission.
To the best of our knowledge, there is a scarcity of research on health literacy, and its impact on patients’ emergency department revisits and hospital readmissions after their discharge from the medical units in hospitals. The reported prevalence of inadequate health literacy in hospital settings ranges from 29 to 76.7% in the literature [32,33,34]. This wide range can be due to the use of different health literacy tools in diverse patient populations. There was no difference in health literacy scores between men and women in this study which is consistent with the literature [35]. Our findings indicate that a higher number of patients older than 65 years of age had inadequate or marginal health literacy as compared to younger patients, which is also found in previous research [34, 36]. The lower level of health literacy in the older population could be due to the decline in comprehension, memory, and word recognition abilities that occur in older age. Although patients with a known diagnosis of dementia were excluded [37], some may have had undetected mild cognitive deficits, which influenced this study’s results. In addition, social determinants of health, including low or no income or disability, were correlated with a lower level of health literacy.
We found that patients with low health literacy scores had a higher probability of emergency department revisits when controlling for other factors, including age, sex, marital status, comorbidity, and education level. Notably, we observed that patients with low health literacy and low education levels had a significantly lower probability of revisiting the emergency department compared to patients with low health literacy and high education levels. It has been previously shown that low education was associated with a higher probability of emergency department visits after surgery [38]. The data data in patients who were admitted to general internal medicine is sparse. A retrospective secondary analysis of clinical trial dataset in medical patients examined the relationship between health literacy and hospital reutilization within 30 days of discharge [32]. The study showed that 49% patients had inadequate or marginal health literacy and that inadequate health literacy was an independent factor for 30-day hospital reutilization after discharge.
Given our findings, it is plausible that not only education but education and health literacy combined have an essential role in the probability of patients revisiting the emergency department and thus their health outcomes. To our knowledge, this study is the first to report that patients with low health literacy but high education have a higher probability of revisiting the emergency department than patients with low health literacy and low education. Further data is needed to identify the critical factors in this result. It is plausible that patients with low education and low health literacy are not fully aware of the harmful effects of underlying illness and are, therefore, less likely to seek early medical attention. Patients with low health literacy may not fully understand and follow the medical instructions provided to them at their hospital discharge, and the consequent inability to attend follow-up visits and delays in seeking medical attention could result in detrimental effects on their health outcomes.
This study has many implications and contributions to society and the medical field at large. Our findings underscore the importance of health literacy interventions. Health education can reduce a patient’s probability of revisiting the emergency department. It is vital to develop and evaluate interventions that run from during a patient’s stay in hospital to their discharge that aim to improve health knowledge. Similarly, it would be necessary to explore factors outside the hospital setting that decreases emergency department revisits for patients with low health literacy. These factors could include access to primary care physicians, support in the community, and knowledge of underlying medical illnesses [39].
Unlike earlier reports [40,41,42,43], this study did not find a significant association between low health literacy and duration of stay or hospital readmission. Patients with inadequate or marginal health literacy had an average length of stay almost twice that of patients with adequate health literacy; however, this was not statistically significant in univariate analysis.
The key strengths of our study are that patients were followed prospectively, and a validated tool was used to assess health literacy. Furthermore, we were able to adjust for essential variables in multivariate modeling. However, our study has some limitations; significant limitations are that non-English speaking patients were not included, and the sample size was relatively small. We were not able to capture if patients had readmission or revisits to the ER for the same or differrent medical conditions due to multiple medical conditons. In addition, instead of short TOFHLA we used full-lenght TOFHLA which takes about 20 minutes to complete. A comprehensive measurement of health litrecacy in the acute care setting may be challenging for some patients as refelcted by 37% refusal rate to particpate in our study. Lastly, our patient population was sampled from two tertiary care hospitals, and although both hospitals received referrals from remote communities, most of the patients were likely from urban areas; therefore, rural and remote populations were underrepresented in this sample, making the results not generalizable to the greater population.
Conclusions
Our results indicate that only half of the patients admitted to general internal medicine units have adequate health literacy. Patients with inadequate or marginal health literacy scores are more likely to revisit the emergency room within 90 days following their discharge from the hospital. It is prudent to address the needs of the population with marginal and inadequate health literacy as improved health literacy can have positive effects on healthcare systems and individuals’ health outcomes. Future studies are required to identify and address strategies for improving the health outcomes of people with inadequate health literacy.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due the confidentiality of the participants but are available from the corresponding author on reasonable request.
References
Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15(Suppl 2):9–19.
Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67:2072–8.
Nutbeam D, Muscat DM. Health promotion glossary 2021. Health Promot Int. 2021;36(6):1578–98.
United States Department of Education National Center for Education Statistics. Adult literacy in the United States; July 2019. https://nces.ed.gov/data points/2019179.asp [Accessed 2 Jan 2022].
Organization for Economic Cooperation and Development (OECD). OECD skills outlook 2013: first results from the survey of adult skills. Paris: OECD Publishing; 2013. https://doi.org/10.1787/9789264204256-en
Kutner M, Greenberg E, Jin Y, et al. The Health Literacy of America's Adults: Results from the 2003 National Assessment of Adult Literacy. Washington, DC: National Center for Education Statistics (U.S. Department of Education) Report No.: nces 2006, 483.
Selden CR, Zorn M, Ratzan SC, et al. Current bibliographies. In: Medicine: health literacy. Bethesda: National Library of Medicine; 2000. p. 479.
Martin LR, Williams SL, Haskard KB, Dimatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1:189–99.
Jansen T, Rademakers J, Waverijn G, Verheij R, Osborne R, Heijmans M. The role of health literacy in explaining the association between educational attainment and the use of out-of-hours primary care services in chronically ill people: a survey study. BMC Health Serv Res. 2018;18(1):394.
van der Heide I, Wang J, Droomers M, Spreeuwenberg P, Rademakers J, Uiters E. The relationship between health, education, and health literacy: results from the Dutch adult literacy and life skills survey. J Health Commun. 2013;18;(Suppl 1):172–184.
Nielsen-Bohlman L, Panzer AM, Kindig DA. Health literacy: a prescription to end confusion. Washington, DC: National Academies Press; 2004.
Rudd RE, Anderson JE, Oppenheimer S, et al. Health literacy: an update of medical and public health literature. In: Review of adult learning and literacy, Policy and Practice, Vol. 7: Connecting Research. Comings JP, Garner B, Smith CA, editors. Mahwah: Lawrence Erlbaum Associates; 2007. p. 175–204.
Wolf MS, Wilson EAH, Rapp DN, et al. Literacy and learning in healthcare. Pediatrics. 2009;124:275–81.
American Medical Association. Health literacy: Report of the Council on Scientific Affairs. Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association. JAMA. 1999;281:552–7.
Williams MV, Parker RM, Baker DW, Parikh NS, Pitkin K, Coates WC, et al. Inadequate functional health literacy among patients at two public hospitals. JAMA. 1995;274:1677–82.
Comings J, Reder S, Sum A. Building a level playing field: the need to expand and improve the national and state adult education and literacy systems. Cambridge: National Center for the Study of Adult Learning and Literacy; 2001.
Baker DW, Parker RM, Williams MV, Clark WS, Nurss J. The relationship of patient reading ability to self-reported health and use of health services. Am J Public Health. 1997;87:1027–30.
Baker DW, Parker RM, Williams MV, Clark WS. Health literacy and the risk of hospital admission. J Gen Intern Med. 1998;13:791–8.
Eckman MH, Wise R, Leonard AC, Dixon E, Burrows C, Khan F, et al. Impact of health literacy on outcomes and effectiveness of an educational intervention in patients with chronic diseases. Patient Educ Couns. 2012;87:143–51.
Dewalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes: a systematic review of the literature. J Gen Intern Med. 2004;19:1228–39.
Wang C, Lang J, Xuan L, Li X, Zhang L. The effect of health literacy and self-management efficacy on the health-related quality of life of hypertensive patients in a western rural area of China: a cross-sectional study. Int J Equity Health. 2017;16:58.
Moser DK, Robinson S, Biddle MJ, Pelter MM, Nesbitt TS, Southard J, et al. Health literacy predicts morbidity and mortality in rural patients with heart failure. J Card Fail. 2015;21:612–8.
Mancuso CA, Rincon M. Impact of health literacy on longitudinal asthma outcomes. J Gen Intern Med. 2006;21:813–7.
Kripalani S, Jacobson TA, Mugalla IC, Cawthon CR, Niesner KJ, Vaccarino V. Health literacy and the quality of physician-patient communication during hospitalization. J Hosp Med. 2010;5:269–75.
Rasu RS, Bawa WA, Suminski R, Snella K, Warady B. Health literacy impact on National Healthcare Utilization and expenditure. Int J Health Policy Manag. 2015;4(11):747–55.
Low Health Literacy: Implications for National Health Policy. https://publichealth.gwu.edu/departments/healthpolicy/CHPR/downloads/LowHealthLiteracyReport10_4_07.pdf [Accessed 16 Aug 2022].
Herndon JB, Chaney M, Carden D. Health literacy and emergency department outcomes: a systematic review. Ann Emerg Med. 2011;57:334–45.
Howard DH, Gazmararian J, Parker RM. The impact of low health literacy on the medical costs of Medicare managed care enrollees. Am J Med. 2005;118:371–7.
Kelly PA, Haidet P. Physician overestimation of patient literacy: a potential source of health care disparities. Patient Educ Couns. 2007;66:119–22.
Rothman RL, DeWalt DA, Malone R, Bryant B, Shintani A, Crigler B, et al. Influence of patient literacy on the effectiveness of a primary care-based diabetes disease management program. JAMA. 2004;292:1711–6.
Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health literacy in adults: a new instrument for measuring patients' literacy skills. J Gen Intern Med. 1995;10:537–41.
Mitchell SE, Sadikova E, Jack BW, Paasche-Orlow MK. Health literacy and 30-day postdischarge hospital utilization. J Health Commun. 2012;17(Suppl 3):325–38.
Boyle J, Speroff T, Worley K, et al. Low health literacy is associated with increased transitional care needs in hospitalized patients. J Hosp Med. 2017;12:918–24.
Strijbos RM, Hinnen JW, van den Haak RFF, Verhoeven BAN, Koning OHJ. Inadequate health literacy in patients with arterial vascular disease. Eur J Vasc Endovasc Surg. 2018;56:239–45.
Dani KA, Stobo DB, Capell HA, Madhok R. Audit of literacy of medical patients in North Glasgow. Scott Med J. 2007;52:21–4.
Jessup RL, Osborne RH, Beauchamp A, Bourne A, Buchbinder R. Health literacy of recently hospitalised patients: a cross-sectional survey using the health literacy questionnaire (HLQ). BMC Health Serv Res. 2017;17:52.
Baker DW, Gazmararian JA, Sudano J, Patterson M. The association between age and health literacy among elderly persons. J Gerontol B Psychol Sci Soc Sci. 2000;55:S368–74.
Mahoney ST, Tawfik-Sexton D, Strassle PD, Farrell TM, Duke MC. Effects of education and health literacy on postoperative hospital visits in bariatric surgery. J Laparoendosc Adv Surg Tech A. 2018;28:1100–4.
Schumacher JR, Hall AG, Davis TC, Arnold CL, Bennett RD, Wolf MS, et al. Potentially preventable use of emergency services: the role of low health literacy. Med Care. 2013;51:654–8.
Jaffee EG, Arora VM, Matthiesen MI, Meltzer DO, Press VG. Health literacy and hospital length of stay: an inpatient cohort study. J Hosp Med. 2017;12:969–73.
Bailey SC, Fang G, Annis IE, O’Conor R, Paasche-Orlow MK, Wolf MS. Health literacy and 30-day hospital readmission after acute myocardial infarction. BMJ Open. 2015;5:e006975.
Cox SR, Liebl MG, McComb MN, Chau JQ, Wilson AA, Achi M, et al. Association between health literacy and 30-day healthcare use after hospital discharge in the heart failure population. Res Social Adm Pharm. 2017;13:754–8.
Rymer JA, Kaltenbach LA, Anstrom KJ, Fonarow GC, Erskine N, Peterson ED, et al. Hospital evaluation of health literacy and associated outcomes in patients after acute myocardial infarction. Am Heart J. 2018;198:97–107.
Acknowledgements
None.
Funding
This work was supported by a grant from the Royal University Hospital Foundation research grant (Grant # 99583) and the Department of Medicine, University of Saskatchewan research grant (Grant # N/A).
Author information
Authors and Affiliations
Contributions
RS provided the concept and design of the project, drafted the article, revised it for necessary content, and provided final approval for submitting the manuscript. PP, MS, LC, RF contributed to necessary revisions of the article. MS, LC, RF, and HW were involved in the concept. MS and RF were involved in the data collection. LC and PP were involved in the analysis. LC also contributed to the statistical analysis section of the manuscript. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the University of Saskatchewan Biomedical Research Ethics Board (Bio-Reb # 308). All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all subjects and/or their legal guardian(s).
Consent for publication
Not applicable.
Competing interests
None Declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shahid, R., Shoker, M., Chu, L.M. et al. Impact of low health literacy on patients’ health outcomes: a multicenter cohort study. BMC Health Serv Res 22, 1148 (2022). https://doi.org/10.1186/s12913-022-08527-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-08527-9