
Abstract
Background
Health care professionals (HCP) are known key elements of effective patient’s counselling and education. For patients taking warfarin, education about the dose, side effects, and toxicity is clearly identified as a cornerstone of achieving improved health and quality of life. The study objective was to evaluate the patients’ knowledge about warfarin and assess the impact of the health care professionals’ counselling in enhancing patients’ knowledge in achieving warfarin therapeutic outcomes.
Method
A six-month prospective multicentered study was conducted in three hospitals, enrolling 300 patients admitted to the cardiac care unit and internal medicine departments. Patients’ warfarin knowledge and INR levels were assessed before and after the clinical pharmacist counselling. The main therapeutic outcome was the impact of the clinical pharmacist-physician counselling on improving patient’s education and achieving therapeutic INR level.
Results
A higher mean knowledge about warfarin score was found after counselling as compared to before counselling (4.82 vs 13.2; p < 0.001). Likewise, the drug dose (1.05 vs 1.88), drug toxicity (0.41 vs 1.92), drug-drug and food-drug interactions (0.02 vs 1.89), therapeutic INR and general drug knowledge scores (2.66 vs 4.68) were significantly higher after as compared to before counselling (p < 0.001 for all variables). The percentages of patients who achieved therapeutic INR levels pre/post counselling was 37.2% and 74.4% respectively (p < 0.001).
Conclusion
Based on the study findings, HCP play a major role in enhancing patients’ knowledge about the factors that affect warfarin therapeutic outcomes. This study highlights the need to establish and develop strategies for appropriate warfarin utilization in Lebanon.
Similar content being viewed by others


Background
Vitamin K antagonists, namely warfarin, remain one of the main oral anticoagulant treatments used for the prevention and treatment of cardiac, thromboembolic and hypercoagulable diseases [1,2,3,4]. Because of its narrow therapeutic index, warfarin requires regular monitoring and dose corrections to retain its optimum anticoagulation effect [3]. Monitoring the International Normalized Ratio (INR) is mandatory to optimize patient outcomes and minimize the risk of thrombosis, without increasing the risk of bleeding complications [5,6,7]. In fact, previous studies revealed that warfarin adverse reactions were responsible for considerable hospital admissions [8, 9]. Indeed, warfarin is listed among the top ten drugs to cause the largest number of serious adverse events reported during the last two decades, according to the adverse events reporting system of the Food and Drug Administration [3]. Achievement of therapeutic outcomes in patients maintained on warfarin is hindered because it is associated with significant inter-patient variability related to age, gender, ethnicity, body weight and genetic variations, and a wide range of drug interactions [10, 11].
A useful strategy that can be used to decrease possible adverse drug reactions is to provide patients with adequate education in order to improve their knowledge. This would also allow patients control their INR more, and consequently decrease the frequency of checking it and the hospitalization rate [12,13,14].
Previously conducted studies reported that warfarin knowledge among patients is often inadequate [15,16,17], while others showed an improvement in anticoagulation control in patients provided with the appropriate information [18, 19]. Therefore, this study was conducted to evaluate the patients’ knowledge about warfarin and assess the impact of the health care professionals counselling in enhancing patient’s knowledge in achieving warfarin therapeutic outcomes.
Methods
Setting
A cross-sectional population-based prospective multicentered study was conducted between January and June 2016. Patients were recruited from three urban Lebanese university hospitals chosen randomly from the list of hospitals provided from the Lebanese Order of Pharmacists. The questionnaire was administered face-to-face by trained researchers, who had a training prior to the start of the data collection to ensure the quality of research. Participants who were on warfarin for any of its approved indications (venous thromboembolism (VTE), atrial fibrillation (A.Fib), valve disease/replacement, stroke or Systolic Left Ventricular Dysfunction (SLVD) were enrolled in this study. Excluded from the analysis were patients who could not answer the questionnaire adequately either due to a decreased mental alertness or decreased cognitive function (cognitive disorders, sedated patients, Alzheimer’s disease, etc.). Four physicians and two clinical pharmacists received thorough training before the beginning of the study to ensure homogeneity and standardization of the data collection. Each physician counselled each patient about the warfarin treatment during the clinic visit; another counselling session was done by the clinical pharmacist, who was responsible of counselling the patient about the side effects of warfarin and the importance of patient’s compliance as well. A two-page brochure entitled “Warfarin: Understanding Side Effects and the Importance of Compliance” was prepared and distributed by the clinical pharmacist at the end of the face-to-face session. To assess patient’s adherence to treatment, we used the Medication Possession Ratio (MPR), defined as the proportion (or percentage) of days’ supply obtained over either refill interval, where last refill is the end point, or fixed refill, where a specific time period is set [20].
Sample size calculation
A sample of 203 patients was targeted to allow for adequate power for bivariable and multivariable analyses to be carried out according to the Epi info sample size calculations with a population size of 4 million in Lebanon, a 15.7% expected frequency of knowledge about warfarin treatment [21], a 5% confidence limits [22]. We decided to distribute 350 questionnaires to take refusals into account.
The questionnaire
The first part of the questionnaire aimed at collecting the patient’s demographic data (age, gender). The second part included a 17-item survey to measure patient’s knowledge about warfarin. This survey was designed by two clinical pharmacists based on existing documents that took into account education and counselling of warfarin therapy provided to patients during their hospital discharge (Additional file 1) [23,24,25]. An INR between 2 and 3 for all indications except for mitral valve replacement (INR range: 2.5-3.5) was considered as an adequate anticoagulation control [26]. The duration of warfarin therapy since the patient started the treatment was divided into 4 categories (2-3 months, 4-6 months, 7-12 months and more than a year) [2].
Furthermore, we assessed patients’ knowledge about warfarin and INR level recording (baseline) before the clinical pharmacist/physician counselling. As part of the effective anticoagulation management, frequent INR monitoring, dose alteration, and patient’s education are also necessary. Therefore, a health care professional (clinical pharmacist or physician) provided an oral counselling session for the patients to raise their level of awareness after the baseline assessment. Warfarin has a long half-life; following a single dose, the terminal elimination half-life is about 1 week, with a mean effective half-life of 40 h [27]. Individual verbal and written counselling was provided to each participant. Therefore, a second evaluation was scheduled 2 months after the counselling session to allow the drug to reach a steady-state concentration and determine whether patient’s knowledge had improved. Patients were divided into two different groups representing warfarin awareness and therapeutic INR status before and after the counselling session.
The survey included questions about drug information and dose, toxicity, drug-drug and drug-food interactions, and INR knowledge. For each question, every correct answer was given one mark then all scores were added. The final score in each section was calculated by adding the marks scored. The greater the score, the greater the level of knowledge.
Data entry and analysis
Data entry was performed by one inspector who was not involved in the data collection process. Descriptive statistics were calculated for all study variables. This includes the mean and standard deviation for continuous measures, counts, and percentages for categorical variables. Paired t-tests were used to look for the difference between the patients’ knowledge before and after the counselling. The statistical package SPSS version 23 was used for all statistical analysis. Statistical significance was set at p < 0.05.
Results
A total of 300 patients were screened. Consequently, 285 participants were enrolled in the study. All enrolled patients completed the warfarin awareness questionnaire before and after counseling whereas 259 completed the INR level assessment: 9 patients could not be contacted for the follow-up evaluation, 7 patients had their warfarin therapy discontinued by their doctors and 10 patients withdrew from the study. The randomization and follow-up of patients in this study are presented in Fig. 1. It is worth noting that all patients were adherent to their treatment throughout the study period and refilled their prescription without any delays.

Flow chart of patient’s randomization and follow up
Enrolled patients had a mean age of 61.18 ± 16.64 years; 53% were males. The majority of warfarin users had a past medical history of cardiovascular disease (62.5%) and hypertension (57.5%). Other patients’ characteristics are listed in Table 1.
The most frequently dispensed warfarin therapy indication was atrial fibrillation (47.7%), followed by VTE (31.6%), and valve disease/replacement (14.7%). In addition, 43.5% of the patients were taking warfarin for 2-3 months, 12.3% between 4 and 6 months 18.2% between 7 and 12 months and 26% for more than a year (Table 2).
Confirmatory factor analysis
We ran a confirmatory factor analysis on the whole sample (n = 300) to check the validity of the created questionnaire. The items converged over a solution of two factors that had an Eigen value over 1. High Cronbach’s alphas were also found for the full scale (0.856), showing good reliability.
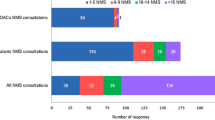
Evaluation of patients’ level of warfarin knowledge
Figure 2 shows the study findings relevant to the evaluation of the patient’s level of warfarin knowledge before and after the clinical pharmacist’s counselling. A higher mean knowledge about warfarin score was found after counselling as compared to before counselling (4.82 vs 13.2; p < 0.001). Likewise, the drug dose (1.05 vs 1.88), drug toxicity (0.41 vs 1.92), drug-drug and food-drug interactions (0.02 vs 1.89), therapeutic INR and general drug knowledge scores (2.66 vs 4.68) were significantly higher after as compared to before counselling (p < 0.001 for all variables).

Comparison of the standard error and mean warfarin knowledge questionnaire score before and after counseling
From the total enrolled patients, a significantly lower percentage of patients with therapeutic INR values was found before counselling (37.2%, mean INR 1.69 ± 0.716), compared to those after counselling (74.4%, mean INR 2.11 ± 0.517) (p < 0.001) (Tables 3, 4 and 5).
Discussion
This is the first study that investigates the Lebanese patients’ knowledge concerning warfarin therapy on anticoagulation control (INR) within the Lebanese population. A higher percentage of our patients (74.4%) achieved good INR control after counselling compared to previous studies [2, 28].
Conflicting results have been reported in the literature regarding the relationship between warfarin knowledge and anticoagulation control. Our results are in agreement with previous findings [15, 29], but opposite to other findings [16]. In this study, patients completed the warfarin knowledge questionnaire on two scheduled follow-ups during the study, before and after the health care professional’s (HCP) counselling. Any question answered incorrectly was reinforced and the correct answers were documented. This was displayed by the mean score of the total warfarin knowledge which revealed a significant improvement after counselling, emphasizing the importance of the HCP implication in the process of disease prevention and treatment through adequate education and proper communication with patients. Our results support the findings of previous researches [30, 31] that showed that inadequate patient’s education and resultant misuse of warfarin correlate with increased difficulty in therapeutic outcome achievements. Other studies showed that patients’ knowledge and awareness about warfarin therapy significantly improved with effective education programs given by health care professionals, [32, 33].
Therefore, HCP, clinical pharmacists more importantly, can improve the patient’s quality of life and enhance his safety by reducing medication errors through the optimization of the appropriate dose, duration of the medication and encouraging routine monitoring.
Education can improve patients’ understanding of warfarin therapy and factors which affect INR control [1]. It is recommended that future studies examine such effect on the population. This suggests that following warfarin education and patient’s follow-up, a large number were able to manage, comply and monitor their warfarin medication, which in turn resulted in better therapeutic control. Previous studies have shown that adherence to warfarin therapy is significantly associated with improved anticoagulation (INR) control [15, 16]. In the present study, patients were educated about their warfarin therapy and taught about how to adjust doses according to their INR results and be compliant with their treatment. The findings showed that the percentage of patients achieving therapeutic INR values increased as the patient’s knowledge enhanced, in line with the findings of Collins et al. that showed that the positive effects of counselling and increasing patients’ warfarin knowledge were beneficial regardless of health literacy level [19]. Thus, HCP interventions significantly contributed to lower non-therapeutic INR scores.
Limitations
Our study has some limitations: the questionnaire used was not validated. Patients were recruited from limited areas of Lebanon; thus, our results couldn’t be generalized to the entire population. In addition, lost to follow-up some patients might cause a selection bias. Our study did not assess patient’s knowledge about warfarin side effects both before and after counselling. When two categories of health care professionals are involved in the counselling, we cannot ascertain whose counselling is really effective or better than the other. Surely, it also makes differences how long someone is on warfarin, as those who are recently beginning the warfarin treatment will have a much greater likelihood of being out of range in the first month. Our study has elucidated a preliminary plan for a good therapeutic INR control in patients on warfarin, however, future studies are needed to address in depth these issues and evaluate the impact of long term follow-up has on patient’s warfarin knowledge, management, therapeutic outcomes, and complications.
Conclusion
Warfarin therapy remains a potentially high risk and problematic challenge for both patients and health care professionals. The study results implied that educated patients about warfarin enhanced the knowledge about factors affecting therapeutic outcomes, and improved medication safety. Hence, HCPs have an important role in improving anticoagulation outcomes through a structured patient counselling and education.
Abbreviations
- A.Fib:
-
Atrial fibrillation
- HCP:
-
Health care professional
- INR:
-
International Normalized Ratio
- MPR:
-
Medication possession ratio
- SLVD:
-
Systolic left ventricular dysfunction
- SPSS:
-
Statistical package for the social sciences
- VTE:
-
Venous thromboembolism
References
Barcellona D, Contu P, Marongiu F. Patient education and oral anticoagulant therapy. Haematologica. 2002;87(10):1081–6.
Khudair IF, Hanssens YI. Evaluation of patients’ knowledge on warfarin in outpatient anticoagulation clinics in a teaching hospital in Qatar. Saudi Med J. 2010;31(6):672–7.
Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167(13):1414–9.
Yahaya A, et al. Factors associated with warfarin therapy knowledge and anticoagulation control among patients attending a warfarin clinic in Malaysia. J Clin Diagn Res. 2009;3(4):1663–70.
Hasan SS, et al. Factors affecting warfarin-related knowledge and INR control of patients attending physician- and pharmacist-managed anticoagulation clinics. J Pharm Pract. 2011;24(5):485–93.
Hirsh J, et al. Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008;133(6 Suppl):141S–59S.
Murray ET, et al. Patient self-management of oral anticoagulation and external quality assessment procedures. Br J Haematol. 2003;122(5):825–8.
Hirri HM, Green PJ. Audit of anticoagulant therapy and acute hospital admissions. Clin Lab Haematol. 2002;24(1):43–5.
Lee CH, et al. Venous thromboembolism: diagnosis and management of pulmonary embolism. Med J Aust. 2005;182(11):569–74.
Ho WK, Hankey GJ, Eikelboom JW. The incidence of venous thromboembolism: a prospective, community-based study in Perth, Western Australia. Med J Aust. 2008;189(3):144–7.
Kearon C, et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med. 2003;349(7):631–9.
Roche-Nagle G, et al. Evaluation of patient knowledge regarding oral anticoagulants. Ir Med J. 2002;96(7):211–3.
Tang EO, et al. Relationship between patients’ warfarin knowledge and anticoagulation control. Ann Pharmacother. 2003;37(1):34–9.
Briggs AL, et al. The development and performance validation of a tool to assess patient anticoagulation knowledge. Res Social Adm Pharm. 2005;1(1):40–59.
Connolly SJ, et al. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation. 2008;118(20):2029–37.
Morgan CL, et al. Warfarin treatment in patients with atrial fibrillation: observing outcomes associated with varying levels of INR control. Thromb Res. 2009;124(1):37–41.
van Walraven C, et al. Burden of potentially avoidable anticoagulant-associated hemorrhagic and thromboembolic events in the elderly. Chest. 2007;131(5):1508–15.
Wofford JL, Wells MD, Singh S. Best strategies for patient education about anticoagulation with warfarin: a systematic review. BMC Health Serv Res. 2008;8:40.
Collins S, Barber A, Sahm LJ. Pharmacist’s counselling improves patient knowledge regarding warfarin, irrespective of health literacy level. Pharmacy. 2014;2(1):114–23.
Andrade SE, et al. Methods for evaluation of medication adherence and persistence using automated databases. Pharmacoepidemiol Drug Saf. 2006;15(8):565–74.
Van Damme S, et al. Patient knowledge of and adherence to oral anticoagulation therapy after mechanical heart-valve replacement for congenital or acquired valve defects. Heart Lung. 2011;40(2):139–46.
Centers for disease control and prevention. Epi info 7 available on http://wwwn.cdc.gov/epiinfo/7/index.htm.
Leger S, et al. Therapeutic education of patients receiving anticoagulants for thromboembolic venous disease: description of the Educ'AVK program. J Mal Vasc. 2004;29(3):145–51.
Mazor KM, et al. Patient education about anticoagulant medication: is narrative evidence or statistical evidence more effective? Patient Educ Couns. 2007;69(1-3):145–57.
Zeolla MM, et al. Development and validation of an instrument to determine patient knowledge: the oral anticoagulation knowledge test. Ann Pharmacother. 2006;40(4):633–8.
Rosendaal FR, et al. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost. 1993;69(3):236–9.
Walfisch A, Koren G. The “warfarin window” in pregnancy: the importance of half-life. J Obstet Gynaecol Can. 2010;32(10):988–9.
Kagansky N, et al. Safety of anticoagulation therapy in well-informed older patients. Arch Intern Med. 2004;164(18):2044–50.
Jackson SL, et al. Point-of-care monitoring of anticoagulant therapy by rural community pharmacists: description of successful outcomes. Aust J Rural Health. 2004;12(5):197–200.
Brigden ML, et al. Audit of the frequency and clinical response to excessive oral anticoagulation in an out-patient population. Am J Hematol. 1998;59(1):22–7.
Arnsten JH, Gelfand JM, Singer DE. Determinants of compliance with anticoagulation: a case-control study. Am J Med. 1997;103(1):11–7.
Lodwick AD, Sajbel TA. Patient and physician satisfaction with a pharmacist-managed anticoagulation clinic: implications for managed care organizations. Manag Care. 2000;9(2):47–50.
Wilson SJ, et al. Comparing the quality of oral anticoagulant management by anticoagulation clinics and by family physicians: a randomized controlled trial. CMAJ. 2003;169(4):293–8.
Acknowledgments
The authors wish to thank Mr. Mohammad Iskandarani for his contribution in data entry and analysis.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
DM designed the study; NC drafted the manuscript; DM, BM and SH contributed to the discussion, reviewed the final manuscript and gave their consent. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The ethics approval was obtained from the Institutional Review Board of the School of Pharmacy at the Lebanese International University. The study objective was explained to the patient prior to the interview, and a written consent was obtained if the patient verbally agreed to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Patient’s knowledge evaluation questionnaire. Questionnaire we used during the data collection. (DOCX 28 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Choumane, N.S., Malaeb, D.N., Malaeb, B. et al. A multicenter, prospective study evaluating the impact of the clinical pharmacist-physician counselling on warfarin therapy management in Lebanon. BMC Health Serv Res 18, 80 (2018). https://doi.org/10.1186/s12913-018-2874-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-018-2874-7