
Abstract
Background
Fangcang shelter hospitals have played an important role in the battle against the COVID-19 epidemic in China. Patients’ verbal and physical attacks on medical workforce are prone to occur in such hospitals. This study explored the impacts of patient mistreatment on healthcare workers’ role behaviors (service performance and patient-oriented organizational citizenship behavior).
Methods
We examined the influence of patient mistreatment on service performance and patient-oriented organizational citizenship behavior, as well as the mediating effect of emotional exhaustion and the moderating effect of displaced aggression by patients, using hierarchical linear regression and conditional process analysis.
Results
Patient mistreatment was positively associated with emotional exhaustion among healthcare workers, while emotional exhaustion was negatively associated with service performance and patient-oriented organizational citizenship behavior. Mediation analysis revealed that emotional exhaustion mediated the association between patient mistreatment and both types of role behaviors. Moderated mediation analysis found that the mediation effect was weaker when the displaced aggression by patients was high.
Conclusions
The findings clarified the relationship among patient mistreatment, emotional exhaustion, service performance, and patient-oriented organizational citizenship behavior. Additional assistance should be provided to healthcare workers dealing with patient mistreatment. Displaced aggression by patients attenuates the positive effects of patient mistreatment on the emotional exhaustion of healthcare workers. Our findings reveal the mechanism and boundary conditions of patient mistreatment affecting healthcare workers' service performance and patient-oriented organizational citizenship behavior.
Similar content being viewed by others


Background
Workplace violence against healthcare workers has been on the rise since the COVID-19 pandemic [1]. Assaults against healthcare workers are increasing at an alarming rate globally, especially verbal attacks by patients [2, 3]. In 2022, omicron virus led to the pandemic outbreak of neo-coronavirus pneumonia in Shanghai, with mass infected patients arising nationwide in a short period of time. Fangcang shelter hospitals were quickly established and used to isolate and treat patients with mild to moderate COVID-19. Such hospitals were large-scale, temporary hospitals built by converting public venues such as stadiums and exhibition centers into healthcare facilities. Healthcare professionals in Fangcang shelter hospitals also suffer from patient mistreatment. Patients who enter the concentration isolation sites of these hospitals are more likely to suffer from mental health problems, such as anxiety, depression, anger, etc., because they are in a relatively narrow space [4]. This may cause patients to act aggressively toward the healthcare staff. Numerous studies have shown that workplace violence adversely affects the quality of patient care and reduces the organizational commitment, job performance, and job satisfaction of healthcare workers [5,6,7,8]. Patient mistreatment negatively affects the role behaviors of healthcare workers [9]. However, there are few studies on how and when this occurs. Therefore, the current research aims to clarify the relationship between patient mistreatment and healthcare workers' role behaviors. Specifically, we focus on two types of role behaviors: service performance and patient-oriented organizational citizenship behavior (OCB hereafter). Effective interventions are necessary to support healthcare workers during health emergencies and possible future outbreaks.
Previous studies have elaborated on the negative impact of customer mistreatment on employees, and it is important to explore the boundary conditions behind it. For example, accountability and supervisor support can weaken the impact of customer mistreatment on employees' negative emotions [10, 11]. At present, there is no perspective from the self-verification of healthcare workers to explore the boundary conditions that alleviate the negative effects of patient mistreatment. Based on the self-verification theory, healthcare professionals constantly accept and process external information to enhance their self-concept. This study proposes that displaced aggression by patients (DAP hereafter) may have a moderating effect between patient mistreatment and emotional exhaustion. Healthcare professionals with extensive work experience are able to detect changes in patient behaviors and emotions during this emergency epidemic, while standing in the patient's perspective to think about problems and empathize with the patient. The patients "indiscriminate" aggression may stimulate empathy among healthcare workers, reducing the depletion of their own self-efficacy and emotional resources, thereby influencing service performance and patient-oriented OCB.
Therefore, we aimed to study the impacts of patient mistreatment on the service performance and patient-oriented OCB of healthcare workers and explore the mechanisms and boundary conditions behind this relationship. This study attempted to answer the following questions: Is patient mistreatment related to service performance and patient-oriented OCB through emotional exhaustion? Can healthcare professionals perceive DAP as a protective resource to reduce emotional exhaustion?
Patient mistreatment and emotional exhaustion
Customer mistreatment refers to unfair and low-quality interpersonal treatment of service personnel by customers during the service process, including cruel hostility, insult, and other acts of intensity less than physical violence [12]. Walker et al. (2014) found that customer mistreatment as a source of stress can induce negative emotions in employees [13]. Customer mistreatment indirectly affects the organization’s negative reputation through employees’ OCB [14]. Specifically, in the healthcare service industry, customer mistreatment is referred as patient mistreatment. However, there are limited academic studies on the impact of patient mistreatment on healthcare workers, particularly in Fangcang shelter hospitals.
According to conservation of resource theory, stress results from circumstances involving threatened or actual loss of valued resources, and individuals are motivated to defend, conserve, and acquire the resources they value [15]. Being judged or criticized by others (such as leaders, customers or patients) would lead to a loss of resources that are valuable in meeting job demands. Especially for healthcare workers, serving patients is itself a process of consuming physical and psychological resources [16,17,18]. Healthcare workers are suffering anxiety due to the heavy workloads in Chinese Fangcang shelter hospitals, which has depleted a great deal of the healthcare professionals' resources to perform their duties [19]. The occurrence of patient mistreatment is not only unable to replenish the original emotional resources of healthcare providers but also requires them to consume additional emotional resources to cope with it [20, 21]. If healthcare professionals’ existing resource reserves are repeatedly depleted without being replenished, it may provoke harmful emotional and psychological reactions, such as emotional exhaustion. In addition, patients' rude and aggressive behavior would impose a greater demand on healthcare professionals who need to spend more resources to regulate their emotions just in order to sustain a normal doctor-patient relationship [22,23,24]. For example, the established organizational rules or regulations require healthcare workers to suppress their overt expressions of negative emotions. As a result, healthcare professionals would have to exercise more energy to regulate their emotions, which would lead to an overuse of valuable resources, resulting in emotional exhaustion [25]. Based on the above analyses, the following hypothesis is proposed:
-
H1: Patient mistreatment is positively associated with emotional exhaustion of healthcare workers.
The mediating role of emotional exhaustion
In a service environment characterized by uncertainty and interdependence, employees need to go beyond the narrow scope of work to serve customers [26]. The distinction between in-role and extra-role behavior is reflected in the discretionary and formalization of employee service behaviors [27]. In-role behavior refers to the organization’s members’ activities within the provisions that must be performed to receive the corresponding remuneration [28]. Essentially, it belongs to the employees’ daily work tasks, usually for service performance [29]. The extra-role behavior is the spontaneous initiative of employees, which transcends the role and organizational remuneration system [30], such as autonomous work effort and OCB.
Resources are a set of important factors that can help individuals achieve their goals or meet their psychological needs [31]. Faced with customer mistreatment, employees must consume additional resources to engage in effective self-motivation to maintain good performance [32]. Studies have shown that emotional exhaustion during COVID-19 has a significant negative effect on unhealthy diets of healthcare workers [33]. In the case of emotional exhaustion, healthcare professionals will be more inclined to reduce the input of other resources, such as reducing work input or engagement, to compensate for the resource loss [34]. Due to the loss of resources, workers may spend time and attention calming themselves down, which reduces their involvement and attention at work and leads to a decline in service performance [35]. Healthcare professionals who have lost resources due to the increasing job stress from patient mistreatment, will be more protective of existing resources to prevent further loss. Thus, they may reduce their commitment and responsibility to patients by reducing patient-oriented OCB [36]. In general, patient mistreatment leads to a loss of emotional resources, which may further lower the initiative and motivation of healthcare professionals to provide services, thereby reducing their interests and willingness to serve patients [37]. Accordingly, we propose the following hypotheses:
-
H2a: Emotional exhaustion is negatively related to service performance.
-
H2b: Emotional exhaustion is negatively related to patient-oriented OCB.
-
Combining H1 and H2, this study proposes the following hypotheses regarding the mediating effects of emotional exhaustion:
-
H3a: Emotional exhaustion mediates the association between patient mistreatment and service performance.
-
H3b: Emotional exhaustion mediates the association between patient mistreatment and patient-oriented OCB.
The moderating role of displaced aggression by patients
Dodge et al. (1987) considered reactive aggression as an individual's defensive response to anger when confronted with frustration [38]. DAP is a particular type of reactive aggression. To eliminate anger, the attacked person will try to retaliate against the attacker [39]. However, they are often unable or unwilling to attack the attacker (e.g., their supervisor), then they often turn to attacking other innocent parties [40]. For example, workers show negative emotional and behavioral reactions toward their families after feeling dissatisfied with their leader [41], and studies have also shown that work-family conflicts can lower employees’ emotions and even engage in aggressive behavior toward those around them [42].
Based on the analysis above, we attempted to incorporate displaced aggression as a boundary condition to explore ways to mitigate the negative effects of patient mistreatment. According to self-verification theory, individuals in the process of self-concept formation will continuously receive, integrate, interpret, and modify external information, thereby affecting their self-concept [43, 44]. Self-verification theory emphasizes how healthcare professionals see themselves and what they see from their patients [45]. In order to maintain self consistency, they exhibit behaviors that are consistent with their self-concept [46]. On the one hand, it is the responsibility of healthcare workers to provide high-quality medical services to patients and care for them [47]. Their professional identity is also characterized by kindness and care [48]. Healthcare workers tend to view being mistreated as a failure of service, thereby reducing their self-esteem and self-concept [49]. However, when workers witness patients frequently expressing anger toward themselves, other healthcare providers, and/or shelter hospital managers, they may catch those signals through their empathic abilities. Previous studies have found that healthcare professionals with high empathy skills are more likely to interpret patients' "indiscriminately" attacks as a result of their dilemma, rather than intentionally mistreating others [10]. We predict that when healthcare workers encounter DAP, they tend to regulate their emotions with a high level of care due to seeking consistence between environment and their self-concept. On the other hand, self verification assessments can also reduce emotional exhaustion by confirming a person's self-concept [50]. People hope to reduce uncertainty about their self-concept and ensure that they maximize their enthusiasm for self-awareness [51]. Subsequently, they may construct a personal understanding of the mistreatment and build an interpretation that patients "indiscriminately" attack people around because of anxiety, nervousness, or depression rooted in the treatment of coronavirus disease in Fangcang shelter hospitals. Being mistreated by patients should not be attributed to the workers’ own professional and technical competence, thus reducing the risk of depletion of their self-concept and the consumption of their own resources. Accordingly, we propose the following hypothesis:
-
H4: DAP moderates the relationship between patient mistreatment and emotional exhaustion such that the relationship is weaker when DAP is high versus low.
Combining H3a, H3b and H4, we propose a moderated mediation model of DAP. If the mediation hypotheses H3a, H3b and the first-stage moderation hypothesis H4 hold, it is reasonable to expect indirect effects of patient mistreatment on role behaviors through emotional exhaustion would also vary according to the different levels of DAP. Therefore, we put forward the following hypotheses:
-
H5a: DAP moderates the indirect effect of patient mistreatment on service performance through emotional exhaustion such that the indirect effect is weaker when DAP is high versus low.
-
H5b: DAP moderates the indirect effect of patient mistreatment on patient-oriented OCB through emotional exhaustion such that the indirect effect is weaker when DAP is high versus low.
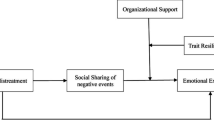
We summarize our theoretical model in Fig. 1.

The proposed moderated mediation model
Methods
Participants and procedure
The online survey was administered through a questionnaire website (https://www.wjx.cn/), with the link delivered to qualified participants with the help of medical team leaders and nursing team leaders in Fangcang Shelter Hospital in December 2022. To prevent unnecessary administrative coercion, each questionnaire was anonymized, and each IP address could only be submitted once. The sample consisted of medical and nursing staff from the Yinglong, Yutong, Yuelai, and Nanping shelter hospitals. In total, 639 questionnaires were distributed. After excluding invalid questionnaires that failed to pass the attention check, 493 valid responses were obtained. The demographic characteristics of the participants are presented in Table 1.
Measures
A back-translation procedure was conducted to ensure the accuracy and consistency of the translated scales [52]. A bilingual management professor translated items into Chinese from the original English, and then another management professor translated items from Chinese back into English. Discrepancies were checked, discussed, and finalized by both professors. The scales used in this study have been widely applied in academic research. The original scales were modified appropriately to fit the research situation. The specific scales were as follows:
-
Patient mistreatment was measured by a 5-item scale (1 = never to 5 = always) developed by Shao et al. (2014) [53]. Participants were asked, “How often over the past month have you had the following occur from a patient?” Sample items included “said inappropriate things.” Cronbach's α for the scale was 0.929.
-
Emotional exhaustion was measured by a 6-item scale (1 = strongly disagree; 5 = strongly agree) developed by Aryee et al. (2008) [54]. Sample items included “I feel emotionally drained from my work”. Cronbach's α for the scale was 0.931.
-
Service performance was measured by a 5-item scale (1 = strongly disagree; 5 = strongly agree) developed by Bettencourt et al. (1997) [55]. Sample items included “I can perform all those tasks for patients who are required of me”. Cronbach's α for the scale was 0.936.
-
Patient-oriented organizational citizenship behavior was also measured by a 5-item scale (1 = strongly disagree; 5 = strongly agree) developed by Bettencourt et al. (1997) [55]. Sample items included “I can voluntarily assist patients even if it means going beyond job requirements.” Cronbach's α for the scale was 0.891.
-
Displaced aggression by patients was measured by a 5-item scale (1 = strongly disagree; 5 = strongly agree) developed by Denson et al. (2006) [56]. and we selected the top three items with the highest factor loadings. Considering that the questionnaire was answered by healthcare workers, a reference-shift method was adopted to modify the subject in each item following Schuster et al. (2022) [57]. Sample items included “When someone or something makes the patient angry, he or she is likely to take it out on another person”. Cronbach's α for the scale was 0.917.
Gender, age, working years, education, technical title, working weeks in shelter hospitals and daily working hours were used as covariates.
Statistical analyses
Statistical analyses were conducted using SPSS 26.0 and Mplus 8.3, and descriptive statistics were computed for all variables. Considering common method variance (CMV hereafter) that might bias our findings, we introduced a variable that is completely unrelated to this study in theory as a marker variable [58], namely, software self-efficacy [59, 60]. This variable was measured on a 3-item scale. Sample items included “I could complete the job using the software package if there was no one around to tell me what to do as I go.” Cronbach's α for the scale was 0.834. In addition, we tested the hypotheses using hierarchical regression analysis, bootstrap test and conditional process analysis (specifically, moderated mediation in this study).
Results
As shown in Table 2, the five-factor model was better than the other models, which indicates that the model fits best (χ2/df = 2.961, TLI = 0.947, CFI = 0.954, RMSEA = 0.063, SRMR = 0.04) and that the variables have reasonable discriminant validity.
We used the Harman single-factor test to assess CMV. Specifically, the results of exploratory factor analyses showed that the first principal component explained 29.47% of the variance. This value was significantly less than the 50% benchmark, suggesting no serious problems with the CMV. This study tests CMV by controlling for software self-efficacy to compare the difference between the bias correlation coefficient and its zero-order correlation coefficient [61]. As is shown in Table 3, the correlation coefficients between the variables remained significant after controlling for the marker variable, indicating that the CMV problem was not severe in the current study.
Table 3 presents the descriptive statistics and correlations among the variables. Patient mistreatment and emotional exhaustion were positively correlated (r = 0.416, p < 0.001). Emotional exhaustion was negatively correlated with service performance (r = -0.173, p < 0.001) and patient-oriented OCB (r = -0.166, p < 0.001).
Testing for the mediating effect
We used hierarchical regression method to test the main effects [62]. As shown in Table 4, patient mistreatment was positively associated with emotional exhaustion (β = 0.526, p < 0.001), and emotional exhaustion was negatively associated with both service performance (β = -0.105, p < 0.01) and patient-oriented OCB (β = -0.095, p < 0.05). Thus, H1 and H2 are supported.
Referring to the mediation analysis steps proposed by Zhao et al. (2010) [63], Table 5 shows the results of the mediating analysis using 5,000 bootstraps. The indirect effect of patient mistreatment on service performance was -0.055, and the confidence interval was (-0.093, -0.019), which did not include the value of zero, indicating that emotional exhaustion had a mediating effect. Similarly, emotional exhaustion mediated the impact of patient mistreatment on patient-oriented OCB. Thus, both H3a and H3b are supported.
Testing for the moderating effect
Hierarchical linear regression analysis was performed to test the moderating effect of DAP. Table 6 illustrates the moderating effects of DAP. DAP weakened the impact of patient mistreatment on emotional exhaustion (β = -0.107, p < 0.05).
Figure 2 shows that for high DAP, patient mistreatment has a weaker positive impact on emotional exhaustion. Thus, H4 is supported.

Moderating effect of DAP on the PM–EE relationship. Note: PM, patient mistreatment; DAP, displaced aggression by patients; EE, emotional exhaustion
Testing for the moderated mediation model
We further tested the moderating mediation effect on the indirect path using conditional process analysis. As shown in Table 7, when service performance was the dependent variable, the bootstrap 95% confidence intervals were (-0.066, -0.017) for high DAP and (-0.109, -0.027) for low DAP, and the difference bootstrap 95% confidence intervals were (0.002, 0.064), indicating the presence of moderated mediating effects. Similarly, the difference in the indirect effects was significant when patient-oriented OCB was the dependent variable. In summary, H5a and H5b are supported.
Finally, to overcome the limitation that moderated mediation can only be tested for discrete moderator values (namely, mean and mean ± one standard deviation) [64], we used the Johnson-Neyman method to depict the continuous confidence intervals of indirect effects. Figures 3 and 4 visualized the moderating mediation effect of different DAP levels (after standardization), indicating that the effect of patient mistreatment on service performance and patient-oriented OCB through emotional exhaustion was weaker when perceived displaced aggression by patients was higher.

Conditional effect of PM on SP as a function of DAP. Note: PM, patient mistreatment; DAP, displaced aggression by patients; SP, service performance

Conditional effect of PM on OCB as a function of DAP. Note: PM, patient mistreatment; DAP, displaced aggression by patients; OCB, patient-oriented organizational citizenship behavior
Discussion
This study was among the first to reveal the relationship between patient mistreatment and healthcare workers’ role behaviors in the context of the Fangcang shelter hospital. The positive emotions and attitudes of healthcare workers are conducive to their work performance [65, 66]. Existing research suggests that patient mistreatment not only affect the mood of healthcare workers [67] but also impede patient safety [68]. It may also reduce work productivity and performance [69, 70]. Given the lack of related studies on patient mistreatment in Fangcang shelter hospitals and the call by Caldas et al. (2021) to study the negative effects of public health emergencies on healthcare workers [71], we investigated the impacts of patient mistreatment on healthcare workers' in-role and extra-role behaviors in the Chinese fight against COVID-19.
Using the conservation of resources theory and self-verification theory, this study demonstrated that patient mistreatment led to exhaustion of the mental resources of healthcare workers, which in turn reduced their service performance and patient-oriented OCB. This process was moderated by healthcare workers' perceived DAP. The effect of patient mistreatment on the emotional exhaustion of healthcare workers was greater, and the indirect effect of mistreatment on the two types of role behaviors via emotional exhaustion was stronger when DAP was low versus high. This study identified the pathway and boundary condition by which patient mistreatment influences service performance and patient-oriented OCB, and verified all the hypotheses of the study.
Our study is consistent with previous work showing that patient mistreatment has a negative impact on emotional exhaustion in healthcare workers [72, 73]. Employees often consume their own emotional resources after being mistreated by customers, resulting in psychological distress, reducing service quality and increasing turnover intention [74]. Based on the above findings, we further explored the impacts of patient mistreatment on workers’ service performance and patient-oriented OCB. Previous studies have mainly documented the negative effects of customer mistreatment in the service industry. Few studies have examined the effects on healthcare workers' behaviors within shelter hospitals during the epidemic [75]. The special environment of shelter hospitals requires healthcare workers to interact with patients with the highest frequency and to have a high level of empathy. Empathetic professionals are better able to place themselves in the patient’s position, thereby making them less likely to reduce their own serving efforts [76].
The present study innovatively considered a moderating variable, namely, displaced aggression by patients. Previous research on DAP has primarily focused on antecedents and outcome variables. DAP was used in this study to illustrate the boundary condition behind the link between patient mistreatment and healthcare workers’ role behaviors, emphasizing the importance of preserving their self-efficacy after perceiving DAP. It allows healthcare workers to attribute mistreatment to patient-directed blame, such as patients’ anger, depression and other negative emotions, which results in indiscriminate attacks against the staff, rather than to their own failure to meet medical service goals. From the perspective of empathy, it also explains how patient mistreatment influences service performance and patient-oriented OCB via emotional exhaustion and how this relationship changes with displaced aggression.
Limitations and future directions
This study has several limitations. First, self-reports were used to measure the key constructs. Studies have shown good validity of the self-report measures used in this study [77]. However, the data collection was based on the overall perceptions of healthcare staff in Fangcang shelter hospitals. In the future, changes in healthcare workers’ emotional states could be explored by using a more detailed longitudinal research design or contextual experimental approach. Second, shelter hospitals are relatively narrow and confined environments in which patients tend to "indiscriminately" attack healthcare workers. Frontline healthcare workers who understand the psychological stress and negative emotions of patients are more inclined to regulate their emotions to meet the needs of patients when encountering mistreatment. Future research can be conducted in other contexts to better understand the antecedents and outcomes of patient mistreatment and develop appropriate strategies to address it in different healthcare scenarios.
Conclusions
In summary, the COVID-19 has caused public panic and psychological stress. Anxiety and depressive symptoms are common psychological reactions during epidemics [78]. Patients in Fangcang shelter hospitals, due to isolation time, economic income losses, sealed environment and other factors, may develop acute stress disorder, anxiety, fear, insomnia and other psychological problems. We need to improve health promotion education and psychological guidance for patients in hospitals to alleviate the various negative emotions brought about by the pandemic and patients' aggression against healthcare workers.
Although healthcare workers in shelter hospitals have a higher capacity of empathy, they are at 3–4 times higher risk of being infected with the virus than others because of their long-term exposure to the infected population [79]. Lai et al. (2020) found that half of the healthcare workers working in Wuhan Fangcang shelter hospitals had more severe psychological symptoms due to fear of being infected [80]. Moreover, suffering from severe mistreatment by patients exacerbates the emotional exhaustion of medical personnel. It is important to pay attention to the dynamic optimization of healthcare staff shifts and provide early psychological interventions for those with psychological problems. In addition, training them to express empathy is imperative for the effective operation of shelter hospitals. When interacting with patients, workers may be required to have skills such as negotiation, stress management, and mindfulness. Hospitals need to assist the staff in learning these skills and putting them into practice. If employees are financially or non-financially compensated for being mistreated by patients, the negative impact on their service behavior may be reduced.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author.
Abbreviations
- OCB:
-
Organizational citizenship behavior
- DAP:
-
Displaced aggression by patients
References
Oerther S, Wolfe T, Lucas H, et al. Editorial: Addressing the persistent epidemic of violence against nurses. Nurse Educ Pract. 2021;54:103098. https://doi.org/10.1016/j.nepr.2021.103098.
Bhatti OA, Rauf H, Aziz N, et al. Violence against healthcare workers during the COVID-19 pandemic: a review of incidents from a lower-middle-income country. Ann Glob Heal. 2021;87(1):41. https://doi.org/10.5334/aogh.3203.
Lafta R, Qusay N, Mary M, et al. Violence against doctors in Iraq during the time of COVID-19. PLoS One. 2021;16(8). https://doi.org/10.1371/journal.pone.0254401
Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novelcoronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–13. https://doi.org/10.1016/S0140-6736(20)30211-7.
Del Mar MM, Del Carmen P-F, Jesus GJ. Analysis of the mediating role of self-efficacy and self-esteem on the effect of workload on burnout’s influence on nurses’ plans to work longer. Front Psychol. 2018;9:2605. https://doi.org/10.3389/fpsyg.2018.02605.
Duan X, Ni X, Shi L, et al. The impact of workplace violence on job satisfaction, job burnout, and turnover intention: the mediating role of social support. Health Qual Life Outcomes. 2019;17:93. https://doi.org/10.1186/s12955-019-1164-3.
Ferri P, Stifani S, Accoto A, et al. Violence against nurses in the triage area: a mixed-methods study. J Emerg Nurs. 2020;46(3):384–97. https://doi.org/10.1016/j.jen.2020.02.013.
Khan MS, Elahi NS, Abid G. Workplace incivility and job satisfaction: mediation of subjective well-being and moderation of forgiveness climate in health care sector. Eur J Investig Heal Psychol Educ. 2021;11(4):1107–19. https://doi.org/10.3390/ejihpe11040082.
Lu Y, Liu Q, Yan H, et al. Job burnout and its impact on work ability in biosafety laboratory staff during the COVID-19 epidemic in Xinjiang. BMC Psychiatry. 2021;21(1). https://doi.org/10.1186/s12888-021-03555-x
Song Y, Liu Y, Wang M, et al. A social mindfulness approach to understanding experienced customer mistreatment: a within-person field experiment. Acad Manag J. 2018;61(3):994–1020. https://doi.org/10.5465/amj.2016.0448.
Zhan X. A study on the influence mechanism of customer bullying behavior on employee work response. Contemp Financ Econ. 2015;367(06):75–84. https://doi.org/10.13676/j.cnki.cn36-1030/f.2015.06.009.
Wang M, Liao H, Zhan Y, et al. Daily customer mistreatment and employee sabotage against customers: examining emotion and resource perspectives. Acad Manag J. 2011;54(2):312–34. https://doi.org/10.5465/AMJ.2011.60263093.
Walker DD, van Jaarsveld DD, Skarlicki DP. Exploring the effects of individual customer incivility encounters on employee incivility: the moderating roles of entity (in) civility and negative affectivity. J Appl Psychol. 2014;99(1):151–61. https://doi.org/10.1037/a0034350.
Garcia PRJM, Restubog SLD, Lu VN, et al. Attributions of blame for customer mistreatment: implications for employees’ service performance and customers’ negative word of mouth. J Vocat Behav. 2019;110:203–13. https://doi.org/10.1016/j.jvb.2018.12.001.
Hobfoll SE. The influence of culture, community, and the nested-self in the stress process: advancing conservation of resources theory. Appl Psychol. 2001;50(3):337–421. https://doi.org/10.1111/1464-0597.00062.
Prapanjaroensin A, Patrician PA, Vance DE. Conservation of resources theory in nurse burnout and patient safety. J Adv Nurs. 2017;73(11):2558–65. https://doi.org/10.1111/JAN.13348.
Lahana E, Papadopoulou K, Roumeliotou O, et al. Burnout among nurses working in social welfare centers for the disabled. BMC Nurs. 2017;16(1):1–10. https://doi.org/10.1186/S12912-017-0209-3/TABLES/4.
Yildirim N, Bulut M. Resources, stressors and coping strategies of nurses caring for patients with coronavirus from the perspective of conservation of resources theory: a qualitative study. J Psychiatr Nurs. 2022;13(2). https://doi.org/10.14744/phd.2021.24434.
Tang L, Yu XT, Wu YW, et al. Burnout, depression, anxiety and insomnia among medical staff during the COVID-19 epidemic in Shanghai. Front Public Heal. 2023;10:1019635. https://doi.org/10.3389/FPUBH.2022.1019635/BIBTEX.
Liu B, Zhu N, Wang H, et al. Protecting nurses from mistreatment by patients: a cross-sectional study on the roles of emotional contagion susceptibility and emotional regulation ability. Int J Environ Res Public Health. 2021;18(12):6331. https://doi.org/10.3390/IJERPH18126331.
Wang X, Wang H. How to survive mistreatment by customers: employees’ work withdrawal and their coping resources. Int J Confl Manag. 2017;28(4):464–82. https://doi.org/10.1108/IJCMA-11-2016-0089.
Zhan Y, Wang M, Shi J. Interpersonal process of emotional labor: the role of negative and positive customer treatment. Pers Psychol. 2016;69(3):525–57. https://doi.org/10.1111/peps.12114.
Rostamabadi A, Shouroki FK, Jalilian H, et al. The relationship between work-related psychosocial factors and burnout among Iranian nurses: job demand-control-support model. Med DEL Lav. 2019;110(4):312–320. https://doi.org/10.23749/mdl.v110i4.8025
Poku CA, Donkor E, Naab F. Determinants of emotional exhaustion among nursing workforce in urban Ghana: a cross-sectional study. BMC Nurs. 2020;19(1):1–10. https://doi.org/10.1186/s12912-020-00512-z.
Maunder RG, Heeney ND, Greenberg RA, et al. The relationship between moral distress, burnout, and considering leaving a hospital job during the COVID-19 pandemic: a longitudinal survey. BMC Nurs. 2023;22(1):1–10. https://doi.org/10.1186/S12912-023-01407-5/TABLES/5.
Griffin MA, Neal A, Parker SK. A new model of work role performance: positive behavior in uncertain and interdependent contexts. Acad Manag J. 2007;50(2):327–47. https://doi.org/10.5465/AMJ.2007.24634438.
Liu D, Gao W, Zhou C. How to respond to complaints? The impact of customer complaints on employee prosocial service behaviors. Foreign Econ Manag. 2023;45(2):57–81. https://doi.org/10.16538/j.cnki.fem.20220729.301.
Becker TE, Kernan MC. Matching commitment to supervisors and organizations to in-role and extra-role performance. Hum Perform. 2003;16(4):327–48. https://doi.org/10.1207/S15327043HUP1604_1.
Tu X, Zhang Y, Wang Y. The mechanism of individualism tendency on employee’s in-role behavior. Chinese J Manag. 2021;18(04):531–8. https://doi.org/10.3969/j.issn.1672-884x.2021.04.007.
Harrell-Cook G. Manufacturing advantage: why high-performance work systems pay off. Acad Manag Rev. 2001;26(3):459–62. https://doi.org/10.2307/259189.
Halbesleben JRB, Neveu JP, Paustian-Underdahl SC, et al. Getting to the “COR”: understanding the role of resources in conservation of resources theory. J Manage. 2014;40(5):1334–64. https://doi.org/10.1177/0149206314527130.
Wen T, Liang Y. Customers bullying and resignation intention of tour guides: a study based resource conservation theory. Tour Sci. 2020;34(03):47–62. https://doi.org/10.16323/j.cnki.lykx.2020.03.004.
Yan W, Zhou X, Song C, et al. Emotional exhaustion and unhealthy eating among COVID-19 front-line healthcare workers during recuperation: a cross-sectional study. Front Public Heal. 2022;10:926395. https://doi.org/10.3389/fpubh.2022.926395.
Hobfoll SE. Social and psychological resources and adaptation. Rev Gen Psychol. 2002;6(4):307–24. https://doi.org/10.1037/1089-2680.6.4.307.
Ye Y, Zhu H, Chen Y, et al. Family ostracism and proactive customer service performance: an explanation from conservation of resources theory. Asia Pacific J Manag. 2021;38(2):645–67. https://doi.org/10.1007/S10490-019-09677-X.
Chi H, Liang SG. When do subordinates’ emotion-regulation strategies matter? abusive supervision, subordinates’ emotional exhaustion, and work withdrawal. Leadersh Q. 2013;24:125–37. https://doi.org/10.1016/j.leaqua.2012.08.006.
Cheng B, Dong Y, Zhou X, et al. Does customer incivility undermine employees’ service performance? Int J Hosp Manag. 2020;89: 102544. https://doi.org/10.1016/j.ijhm.2020.102544.
Dodge KA, Coie JD. Social-information-processing factors in reactive and proactive aggression in children’s peer groups. J Personal Soc Psychol. 1987;53(6):1146. https://doi.org/10.1037/0022-3514.53.6.1146.
Moghaddam FM. Great ideas in psychology: a cultural and historical introduction. Oxford, UK: Oneworld Publication; 2007. p. 353.
Courtright SH, Gardner RG, Smith TA, et al. My family made me do it: a cross-domain, self-regulatory perspective on antecedents to abusive supervision. Acad Manag J. 2016;59(5):1630–52. https://doi.org/10.5465/amj.2013.1009.
Chan XW, Kalliath T, Cheng D. When the boss is blue: examining the effects of supervisors’ negative emotions on subordinates’ cognitive work engagement and family undermining. Pers Rev. 2021;50(2):575–95. https://doi.org/10.1108/PR-04-2019-0177.
Liu Y, Wang M, Chang CH, et al. Work-family conflict, emotional exhaustion, and displaced aggression toward others: the moderating roles of workplace interpersonal conflict and perceived managerial family support. J Appl Psychol. 2015;100(3):793–808. https://doi.org/10.1037/a0038387.
Korman AK. Toward an hypothesis of work behavior. J Appl Psychol. 1970;54(1):31–41. https://doi.org/10.1037/h0028656.
Swann WB. The trouble with change: self-verification and allegiance to the self. Psychol Sci. 1997;8(3):177–80. https://doi.org/10.1111/j.1467-9280.1997.tb00407.x.
Amarnani RK, Restubog SLD, Shao R, et al. A self-verification perspective on customer mistreatment and customer-directed organizational citizenship behaviors. J Organ Behav. 2022;43(5):912–31. https://doi.org/10.1002/job.2610.
Swann WB, Brooks M. Why threats trigger compensatory reactions: the need for coherence and quest for self-verification. Soc Cogn. 2012;30(6):758–77. https://doi.org/10.1521/soco.2012.30.6.758.
Niland M. Expertise in nursing practice: caring, clinical judgment, and ethics. J Contin Educ Nurs. 1996;27(4):196. https://doi.org/10.3928/0022-0124-19960701-10.
Zhu Y, Chen T, Wang J, et al. How critical activities within COVID-19 intensive care units increase nurses’ daily occupational calling. 2020;106(1):4–14. https://doi.org/10.1037/apl0000853
Zhao H, Wu Z, Liu W. Displaced aggression: how does customer mistreatment influence employees’ counterproductive work behaviors? Manage Rev. 2020;32(05):243–54. https://doi.org/10.14120/j.cnki.cn11-5057/f.2020.05.020.
Talaifar S, Buhrmester MD, Ayduk Ö, et al. Asymmetries in mutual understanding: people with low status, power, and self-esteem understand better than they are understood. Perspect Psychol Sci. 2020;16(2):338–57. https://doi.org/10.1177/1745691620958003.
Sedikides C, Strube MJ. Self-evaluation: To thine own self be good, to thine own self be sure, to thine own self be true, and to thine own self be better. Adv Exp Soc Psychol. 1997;29:209–69. https://doi.org/10.1016/S0065-2601(08)60018-0.
Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. https://doi.org/10.1177/135910457000100301.
Shao R, Skarlicki DP. Service employees’ reactions to mistreatment by customers: A comparison between North America and East Asia. Pers Psychol. 2014;67(1):23–59. https://doi.org/10.1111/peps.12021.
Aryee S, Sun LY, Chen ZXG, et al. Abusive supervision and contextual performance: the mediating role of emotional exhaustion and the moderating role of work unit structure. Manag Organ Rev. 2008;4(3):393–411. https://doi.org/10.1111/j.1740-8784.2008.00118.x.
Bettencourt LA, Brown SW. Contact employees: relationships among workplace fairness, job satisfaction and prosocial service behaviors. J Retail. 1997;73(1):39–61. https://doi.org/10.1016/S0022-4359(97)90014-2.
Denson TF, Pedersen WC, Miller N. The displaced aggression questionnaire. J Pers Soc Psychol. 2006;90(6):1032–51. https://doi.org/10.1037/0022-3514.90.6.1032.
Schuster T, Bader AK, Bader B, et al. Does what happens abroad stay abroad? Displaced aggression and emotional regulation in expatriate psychological contracts. J Occup Organ Psychol. 2022;95(4):867–88. https://doi.org/10.1111/joop.12405.
Lindell MK, Whitney DJ. Accounting for common method variance in cross-sectional research designs. J Appl Psychol. 2001;86(1):114–21. https://doi.org/10.1037/0021-9010.86.1.114.
Williams LJ, Hartman N, Cavazotte F. Method variance and marker variables: a review and comprehensive CFA marker technique. Organ Res Methods. 2010;13(3):477–514. https://doi.org/10.1177/1094428110366036.
Simmering MJ, Fuller CM, Richardson HA, et al. Marker variable choice, reporting, and interpretation in the detection of common method variance. Organ Res Methods. 2014;18(3):473–511. https://doi.org/10.1177/1094428114560023.
Lindell MK, Brandt CJ. Assessing interrater agreement on the job relevance of a test: Acomparison of the CVI, T, (rWG(J)), and r*(WG(J)) indexes. J Appl Psychol. 1999;84(4):640–7. https://doi.org/10.1037/0021-9010.84.4.640.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. 1986;51(6):1173-1182. https://doi.org/10.1037/0022-3514.51.6.1173.
Zhao X, Lynch JG, Chen Q. Reconsidering Baron and Kenny: myths and truths about mediation analysis. J Consum Res. 2010;37(2):197–206. https://doi.org/10.1086/651257.
Fang J, Wen Z, Liang D, et al. Moderation effect analyses based on multiple linear regression. J Psychol Sci. 2015;38(03):715–20. https://doi.org/10.16719/j.cnki.1671-6981.2015.03.001.
GholamiMotlagh F, Nobahar M, Raiesdana N. The relationship of moral intelligence and social capital with job satisfaction among nurses working in the emergency department. Int Emerg Nurs. 2020;52:100911. https://doi.org/10.1016/j.ienj.2020.100911.
González-Gancedo J, Fernández-Martínez E, Rodríguez-Borrego MA. Relationships among general health, job satisfaction, work engagement and job features in nurses working in a public hospital: a cross-sectional study. J Clin Nurs. 2019;28(7–8):1273–88. https://doi.org/10.1111/jocn.14740.
Diefendorff JM, Gabriel AS, Nolan MT, et al. Emotion regulation in the context of customer mistreatment and felt affect: an event-based profile approach. J Appl Psychol. 2019;104(7):965–83. https://doi.org/10.1037/apl0000389.
Kim K. Exploring the influence of workplace violence and bystander behaviour on patient safety in Korea: a pilot study. J Nurs Manag. 2020;28(3):735–43. https://doi.org/10.1111/jonm.12991.
Lin WQ, Wu J, Yuan LX, et al. Workplace violence and job performance among community healthcare workers in China: The mediator role of quality of life. Int J Environ Res Public Health. 2015;12(11):14872–86. https://doi.org/10.3390/ijerph121114872.
Liu J, Zheng J, Liu K, et al. Workplace violence against nurses, job satisfaction, burnout, and patient safety in Chinese hospitals. Nurs Outlook. 2019;67(5):558–66. https://doi.org/10.1016/j.outlook.2019.04.006.
Caldas MP, Ostermeier K, Cooper D. When helping hurts: COVID-19 critical incident involvement and resource depletion in health care workers. J Appl Psychol. 2020;106(1):29. https://doi.org/10.1037/apl0000850.
Cai D, Li F, Feng T, et al. Mistreatment from patients and nurses’ career withdrawal intention: does political skill matter? Asia Pacific J Hum Resour. 2022;60(2):342–61. https://doi.org/10.1111/1744-7941.12253.
Giusti EM, Pedroli E, D’Aniello GE, et al. The psychological impact of the covid-19 outbreak on health professionals: a cross-sectional study. Front Psychol. 2020;11:1684. https://doi.org/10.3389/fpsyg.2020.01684.
Asaoka H, Sasaki N, Kuroda R, et al. Workplace bullying and patient aggression related to COVID-19 and its association with psychological distress among health care professionals during the COVID-19 pandemic in Japan. Tohoku J Exp Med. 2021;255(4):283–9. https://doi.org/10.1620/tjem.255.283.
Zhou X, Li X, Yin L, et al. Studying on the impact of patients’mistreatment on nurses’job burnout and intention to demission. Chinese Heal Serv Manag. 2017;34(07):543–5.
Wang T, Wang W, Hong J, et al. Subjective well-being and job burnout of clinical nurses: the role of empathy. Chinese Nurs Manag. 2015;15(03):280–4.
Gollwitzer A, McLoughlin K, Martel C, et al. Linking self-reported social distancing to real-world behavior during the COVID-19 pandemic. Soc Psychol Personal Sci. 2022;13(2):656–68. https://doi.org/10.1177/19485506211018132.
Dai LL, Wang X, Jiang TC, et al. Anxiety and depressive symptoms among COVID-19 patients in Jianghan Fangcang shelter hospital in Wuhan, China. PLoS One. 2020;15(8). https://doi.org/10.1371/journal.pone.0238416.
Hannemann J, Abdalrahman A, Erim Y, et al. The impact of the COVID-19 pandemic on the mental health of medical staff considering the interplay of pandemic burden and psychosocial resources-a rapid systematic review. PLoS One. 2022;17(2). https://doi.org/10.1371/journal.pone.0264290.
Lai J, Ma S, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020;3(3). https://doi.org/10.1001/jamanetworkopen.2020.3976.
Acknowledgements
The authors thank all interviewees who showed great patience in answering the questionnaires.
Funding
This research was supported by grants funded by the National Social Science Foundation of China (Grant number: 19BJY052, 22BGL141), National Natural Science Foundation of China (Grant number: 72110107002, 71974021), Natural Science Foundation of Chongqing (Grant number: cstc2021jcyj-msxmX0689), Fundamental Research Funds for the Central Universities (Grant number: 2022CDJSKJC14), and Chongqing Social Science Planning Project (Grant number: 2018PY76).
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. Study design, questionnaire collection, data acquisition were performed by WY and HW. Data analysis and the first draft of the manuscript was written by WY and NB. SJZ, DMY and LC commented on the manuscript and revised it critically for important intellectual content.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Review Committee of the School of Economics and Business Administration, Chongqing University (IRB No. SEBA201906). All methods were carried out in accordance with relevant guidelines and regulation. Informed consent was obtained from all subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yan, W., Bao, N., Zheng, S. et al. The impacts of patient mistreatment on healthcare workers’ role behaviors: a study in Chinese Fangcang shelter hospitals. BMC Nurs 22, 444 (2023). https://doi.org/10.1186/s12912-023-01574-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-023-01574-5