
Abstract
Background
Nurses’ secondary traumatic stress, compassion satisfaction and posttraumatic growth are closely related, but for newly graduated nurses, there are few reports to evaluate the specific path between these three. The aim of this study was to investigate examine the mediating role of compassion satisfaction in secondary traumatic stress and posttraumatic growth among newly graduated nurses.
Methods
From March 2021 to May 2021, a total of 330 newly graduated nurses from five tertiary hospitals in China were enrolled, and asked to complete questionnaires regarding secondary traumatic stress, compassion satisfaction and posttraumatic growth. Descriptive statistics, independent-samples T-test, one-way analysis of variance (ANOVA), Pearson correlation analysis and structural equation model were used in this study. A STROBE checklist was used to report findings.
Results
The scores of secondary traumatic stress, compassion satisfaction and posttraumatic growth of newly graduated nurses were 27.11 ± 4.94 (score range: 10–50), 31.89 ± 6.22 (score range: 10–50) and 56.47 ± 20.41 (score range: 0-100), respectively. Additionally, structural equation modeling showed that compassion satisfaction mediated the relationship between secondary traumatic stress and posttraumatic growth with the partial mediating effect of 0.089.
Conclusions
Newly graduated nurses may experience moderate secondary traumatic stress, but their posttraumatic growth is at a low level, and compassion satisfaction significantly affects the relationship between the two. Nursing managers should strengthen psychological evaluation, and promote their posttraumatic growth by improving their level of compassion satisfaction.
Similar content being viewed by others

Introduction
The acceleration of the global population aging process has put forward higher service requirements for the medical and health care industry, while nurses, as important medical and health care personnel, are facing a shortage of personnel, which is undoubtedly a great threat to the quality of medical and health care services in various countries [1]. Some studies pointed out that recruiting newly graduated nurses was one of the effective ways to supplement nursing staff and expand the nursing team, which also helps to alleviate the continuous crisis of health care services [2, 3]. However, newly graduated nurses may experience a gap between theory and practice when they first enter the clinical environment [4]. An effective transition plan is an important support system for newly graduated nurses to pass the transition period, which is important and complex for nursing managers, such as standardized training for nurses in China [5]. Standardized training for nurses refers to nurses receiving standardized and professional nursing theory and practical training after completing basic education in medical colleges, and standardized training for nurses is an important way to cultivate a nursing talent team, and an important measure to enhance nurses’ comprehensive abilities, improve clinical nursing quality [6]. Nevertheless, due to the high risk and pressure of work in the nursing industry, newly graduated nurses may often encounter considerable challenges when transitioning to clinical practice at the initial stage of employment because of their lack of clinical work experience, such as secondary traumatic stress [7].
Secondary traumatic stress refers to a natural stressful behavior and psychological emotional result produced by the group of helpers who are indirectly exposed to the injured and their painful experiences in the process of helping or wanting to help the injured and the suffering [8]. Mangoulia et al. believed that for nurses, secondary traumatic stress was an occupational hazard, which is not only detrimental to the physical and mental health of nurses, but also reduces the ability of nurses to provide nursing services and make professional judgments, seriously affecting the personal life and work of nurses [9]. Wang et al. also pointed out that nurses with high levels of secondary traumatic stress might have emotional exhaustion and turnover intention, which directly affects the quality of clinical nursing service and the stability of nursing team [10]. Moreover, some studies showed that newly graduated nurses reported significantly higher levels of secondary traumatic stress than experienced senior nurses [3, 11]. Therefore, it is necessary to pay attention to the psychological stress response of newly graduated nurses after indirect trauma exposure.
Despite experiencing indirect trauma exposure will cause nurses to have negative psychological stress response, such as secondary traumatic stress, positive psychological changes may also occur, such as posttraumatic growth. Posttraumatic growth refers to the positive psychological changes experienced by individuals in the fight against highly challenging life events and traumatic events, including changes in self-awakening, interpersonal relations and life philosophy [12]. Relevant studies confirmed that the occurrence of posttraumatic growth could enhance nurses’ ability to adapt to the environment, which is conducive to alleviating nurses’ work pressure, and improving their job satisfaction and subjective well-being [13, 14]. As for the influencing factors of nurses’ posttraumatic growth, some studies suggested that secondary traumatic stress might become a catalyst for posttraumatic growth, that is, the higher the level of secondary traumatic stress, the stronger the nurses’ self-awakening and determination to seek change, and the higher the level of posttraumatic growth [8, 15]. Another study found that compassion satisfaction was also an important factor affecting nurses’ posttraumatic growth [16].
Compassion satisfaction means that nurses can obtain a sense of pleasure and achievement by providing nursing services to patients [10]. Peters believed that compassion satisfaction could provide energy, insight and firm determination for nursing services, so as to promote nurses to show positive work attitude, high-level professional value and high-quality nursing services [17]. Yu, Jiang & Shen proposed that a high level of compassion satisfaction could not only improve the quality of nursing services, but also prolong the professional life of nurses and reduce the risk of nurses leaving [18]. Moreover, some studies pointed out that compassion satisfaction could be used as a regulating or buffering factor of compassion fatigue, and the higher the level of compassion satisfaction of nurses, the stronger their ability to cope with psychological stress, and the greater their relief effect on secondary traumatic stress and burnout, which is conducive to promoting the posttraumatic growth of nurses [10, 19].
Although previous studies have shown that there is a correlation between nurses’ secondary traumatic stress, compassion satisfaction and posttraumatic growth, few studies have investigated the mediating role of compassion satisfaction on the relationship between secondary traumatic stress and posttraumatic growth, especially for newly graduated nurses. Therefore, in order to provide theoretical basis for nursing managers to formulate targeted measures to improve the mental health level of newly graduated nurses, this study aims to clarify the relationship between secondary traumatic stress and posttraumatic growth of newly graduated nurses, and explore the mediating role of compassion satisfaction between the two.
This study mainly proposes the following hypothesis:
Hypothesis 1
Newly graduated nurses’ secondary traumatic stress is closely related to their posttraumatic growth.
Hypothesis 2
Newly graduated nurses’ compassion satisfaction is closely related to their posttraumatic growth.
Hypothesis 3
The relationship between newly graduated nurses’ secondary traumatic stress and posttraumatic growth is mediated by compassion satisfaction.
Methods
Aim
This study aimed to explore the relationship between secondary traumatic stress and posttraumatic growth, as well as the mediating role of compassion satisfaction in this relationship among newly graduated nurses working in Chengdu, China.
Design
This was a cross-sectional study, and to ensure the research quality, the STROBE checklist was used to report findings.
Participants
From March 2021 to May 2021, participants were selected from five tertiary grade A hospitals in Chengdu, Sichuan Province, China by convenient sampling. The inclusion criteria of participants were: (a) registered nurses, (b) with < 1 year of clinical nursing experience, and (c) volunteered to participation in this study. Exclusion criteria: (a) non formal staff of the investigated hospital, such as refresher nurses; (b) Those who are not on duty at the time of investigation. These participants work in different departments, including internal medicine, surgery, pediatrics, oncology, psychiatry, ICU, etc.
Data collection
First of all, we contacted the heads of the relevant management departments of each hospital and obtained the investigation permission. Then we sent the electronic questionnaire through the network platform to conduct a pre survey, and conducted cultural debugging on the total table through the feedback of the pre survey. After the pre survey, the final version of the electronic questionnaire was distributed again through the network platform, including a unified guide, which explained the purpose of the survey, the definition of survey related variables and precautions for filling in, and pointed out that the survey was anonymous and voluntary. According to the literature, the sample size should be 5–10 times the number of items [20, 21]. In addition, considering the possible quality problems in the questionnaire, the sample size should be expanded by 20%. Therefore, our study requires at least 282 participants. Finally, a total of 350 questionnaires were distributed and 330 valid questionnaires were recovered, with a response rate of 94.29%.
Measures
Secondary traumatic stress
To assess secondary traumatic stress of nurses, the Chinese version Professional Quality of Life Scale (ProQOL-CN), which is a translated and revised by Zheng et al. of the original ProQOL, developed by Stamm, was used [22, 23]. The ProQOL-CN has three sub scales, namely, compassion satisfaction (CS), burnout (BO) and secondary traumatic stress (STS), and each sub scale has 10 items, a total of 30 items. Among the 10 items used to measure secondary traumatic stress, participants were asked to answer with a 5-point Likert scale, ranging from 1 (“never”) to 5 (“always”), and the higher the score, the higher the nurse’s secondary traumatic stress level. It was generally believed that a score ≤ 22 is a low level, 23–41 is a moderate level, and ≥ 42 is a high level [22, 23]. Regarding the reliability of the secondary traumatic stress sub scale, the Cronbach’s α of the ProQOL was 0.81, and in this study, the Cronbach’s α was 0.80.
Compassion satisfaction
To assess compassion satisfaction of nurses, the ProQOL-CN was used. Among the compassion satisfaction sub scale, participants were asked to answer with a 5-point Likert scale, ranging from 1 (“never”) to 5 (“always”), and the higher the score, the higher the nurse’s compassion satisfaction level. Similarly, the score ≤ 22 is a low level, 23–41 is a moderate level, and ≥ 42 is a high level [22, 23]. Regarding the reliability of the compassion satisfaction sub scale, the Cronbach’s α of the ProQOL was 0.88, and in this study, the Cronbach’s α was 0.91.
Posttraumatic growth
To assess posttraumatic growth of nurses, the Simplified Chinese version of the Posttraumatic Growth Inventory (C-PTGI), which is a translated and revised by Wang et al. of the original PTGI, developed by Tedeschi & Calhoun, was used [24, 25]. C-PTGI includes five subscales, namely, relating to others, new possibilities, personal strength, spiritual change, and insights on life, with a total of 20 items (the original 18th item “I have a stronger religious faith” was deleted). Participants were asked to answer with a 6-point Likert scale, ranging from 0 (no change) to 5 (great change), and the higher the score, the higher the nurse’s posttraumatic growth level. Among them, the score < 60 is a low growth level, 60–65 is a moderate growth level, and > 65 is a high growth level [25]. Regarding the reliability, the Cronbach’s α of the PTGI was 0.90 and for the subscales was 0.67 to 0.85, and in this study, the Cronbach’s α was 0.97 and for the subscales was 0.89 to 0.93.
Data analysis
SPSS 26.0 and AMOS 26.0 were used to analyze the data. Descriptive statistics were used to present the social-demographic information of participants. Since our data approximate the normal distribution, independent sample t-test or one-way analysis of variance (ANOVA) were used to test the scores of secondary traumatic stress, compassion satisfaction and posttraumatic growth of newly graduated nurses with different social-demographic information. Pearson correlation analysis was used to evaluate the relationship between variables. Structural equation model was used to explore the relationship between secondary traumatic stress, compassion satisfaction and posttraumatic growth of newly graduated nurses, and to test the mediating role of compassion satisfaction. In the study, judge whether the model fitting is reasonable by χ2/df, Tacker-Lewis index (TLI), comparative fit index (CFI), incremental fit index (IFI), relative fit index (RFI), normal fit index (NFI), and root mean square error of approximation (RMSEA). The χ2/df < 5, TLI, CFI, IFI, RFI and NFI > 0.90, RMSEA ≤ 0.08 are considered to be reasonable model fitting. In addition, p < 0.05 was considered statistically significant (two-tailed test).
Ethical consideration
The principles of anonymity and informed consent were strictly followed throughout the study, and this study has been approved by the Ethics Committee of Chengdu University of Traditional Chinese Medicine (Number: 2020-KL084).
Results
Participant characteristics
Of the 330 newly graduated nurses, 7.88% were males and 92.12% were females, with a mean age of 22.73 ± 1.89. Only 7.58% of newly graduated nurses were married. The majority of newly graduated nurses had bachelor degree or above (62.73%), were on day shift (64.24%), worked hours per day > 8 h (65.76%), slept hours per day > 7 h (65.76%). More than half (59.70%) of newly graduated nurses had workplace violence experience (Table 1).
The level of secondary traumatic stress, compassion satisfaction and posttraumatic growth
The scores of secondary traumatic stress, compassion satisfaction and posttraumatic growth of newly graduated nurses were 27.11 ± 4.94, 31.89 ± 6.22 and 56.47 ± 20.41, respectively (Table 2). Moreover, newly graduated nurses who worked hours per day > 8 h, slept hours per day ≤ 7 h and had workplace violence experience reported higher secondary traumatic stress scores. Newly graduated nurses who slept hours per day > 7 h reported higher compassion satisfaction, while newly graduated nurses who slept hours per day ≤ 7 h and had workplace violence experience reported lower posttraumatic growth scores (p < 0.05) (Table 1).
Correlations of secondary traumatic stress, compassion satisfaction and posttraumatic growth
Pearson correlation analysis suggested that secondary traumatic stress and compassion satisfaction of newly graduated nurses were significantly positively associated with posttraumatic growth and its five subscales (p < 0.01) (Table 2).
The mediating role of compassion satisfaction on the relationships between secondary traumatic stress and posttraumatic growth
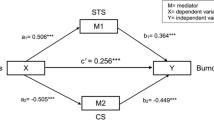
The hypothetical model was tested by structural equation modeling, which includes three latent constructs (secondary traumatic stress, compassion satisfaction and posttraumatic growth) and seven observed variables (Fig. 1). In this model, the fitting degree of the model was appropriate as follows: χ2/df = 3.006, TLI = 0.978, CFI = 0.986, IFI = 0.986, RFI = 0.967, NFI = 0.980, RMSEA = 0.078. Furthermore, all factor loads of indicators on latent constructs were significant (p < 0.05), indicating that all latent constructs were well represented by their indicators.

The mediate effect model of compassion satisfaction between secondary traumatic stress and posttraumatic growth
The mediating roles of compassion satisfaction were examined by 5000 bootstrap analyses with 95% confidence intervals. As shown in Table 3, secondary traumatic stress had a significant direct effect on compassion satisfaction (β = 0.160, p = 0.007) and posttraumatic growth (β = 0.100, p = 0.030). The direct effect of compassion satisfaction on posttraumatic growth was 0.558 (p = 0.001). The indirect effect of secondary traumatic stress → compassion satisfaction → posttraumatic growth was 0.089 (p = 0.007), which suggested that compassion satisfaction partially mediates between secondary traumatic stress and posttraumatic growth.
Discussion
In this study, we found that the scores of secondary traumatic stress and compassion satisfaction of newly graduated nurses were 27.11 ± 4.94 and 31.89 ± 6.22, respectively, which were at a moderate level, while their posttraumatic growth score was 56.47 ± 20.41, which was in the low level. Compared with previous studies, the level of secondary traumatic stress of newly graduated nurses is obviously higher, but the level of compassion satisfaction and posttraumatic growth are lower [8, 26]. The reason for this result may be that newly graduated nurses have just come into contact with clinical nursing and lack of work experience, so they can not easily view and cope with work stress, while the slow role transformation also makes nurses unable to clearly find their own position in clinical nursing work and feel the pleasure and achievement brought by helping others [27]. In addition, some studies pointed out that nurses with older age and longer working years had more nursing experience, could better deal with emergencies of patients and reflect afterwards, and their posttraumatic growth level was higher [28, 29]. In contrast, newly graduated nurses lacked both knowledge reserve and practical ability, and their posttraumatic growth level was relatively low [30].
This study revealed that newly graduated nurses who worked hours per day > 8 h had higher secondary traumatic stress level, while newly graduated nurses who slept hours per day > 8 h had lower secondary traumatic stress level, higher compassion satisfaction level and posttraumatic growth level. On the one hand, long working hours and multiple consecutive shifts may increase the risk of nurses’ burnout and secondary traumatic stress, cause occupational injury, and then affect the overall quality of nursing [31, 32]. On the other hand, nurses with sufficient sleep time are more likely to maintain good physical and mental state, better recover energy, face various emergencies at work, so as to reduce secondary traumatic stress level, improve compassion satisfaction level, and ultimately promote posttraumatic growth [8, 10]. In addition, the results of this study suggested that newly graduated nurses who had workplace violence experience had a higher level of secondary traumatic stress and a lower level of posttraumatic growth, which is consistent with the findings of Zeng et al. [16]. Even though nurses had invested a lot of energy in nursing work, they might still suffer from workplace violence, which will cause compassion fatigue of nurses and aggravate their secondary traumatic stress, and their posttraumatic growth level might also be affected [33].
Furthermore, this study also verified the positive correlation between secondary traumatic stress, compassion satisfaction and posttraumatic growth of newly graduated nurses, and clarified more specific information among the three through structural equation model. It can be seen from the results that the three path coefficients including secondary traumatic stress → posttraumatic growth, compassion satisfaction → posttraumatic growth and secondary traumatic stress → compassion satisfaction → posttraumatic growth are statistically significant.
Hypothesis 1
proposed that secondary traumatic stress has a direct effect on posttraumatic growth, which was confirmed by this study and is consistent with prior reports [15, 34]. Chen et al. believed that when nurses’ traumatic stress experience was maintained over time, they might take some coping measures to make themselves reconstruct this experience cognitively, thus producing positive results, such as posttraumatic growth [35]. Another study showed that when nurses faced high-intensity secondary traumatic stress, their inner painful experience was triggered, while in order to obtain self-change and detachment, they could stimulate self-reflection on the existing situation, and posttraumatic growth followed [8].
Hypothesis 2
that compassion satisfaction has a positive effect on posttraumatic growth was also confirmed by this study. Zeng et al. proposed that compassion satisfaction was one of the important factors affecting the posttraumatic growth of nurses, and the higher the level of compassion satisfaction of nurses, the more they could obtain energy from nursing work, so as to handle various events more calmly and deal with psychological stress, thus promoting the improvement of their posttraumatic growth level [16].
Besides, the research results on the relationship between secondary traumatic stress, compassion satisfaction and posttraumatic growth allowed us to corroborate hypothesis 3, that is, secondary traumatic stress can not only directly affect posttraumatic growth, but also indirectly affect posttraumatic growth through the mediating effect of compassion satisfaction. Previous studies pointed out that although secondary traumatic stress might cause emotional exhaustion of nurses and have a negative impact on nursing work, it might also cause nurses to rethink their personal values and promote posttraumatic growth due to the special high-pressure environment [8, 15]. As for the impact of secondary traumatic stress on compassion satisfaction, some studies think it is negative, others think it is positive, and some studies think there is no relationship between the two, which may be related to the background of the respondents and the complex and diverse nursing environment [36,37,38]. In this study, nurses with higher levels of secondary traumatic stress can obtain a stronger sense of achievement in clinical nursing work and a higher level of compassion satisfaction, which provides the possibility for the occurrence and improvement of posttraumatic growth.
Limitations
This study has some limitations. First, the cross-sectional design could not test the causal mechanism between secondary traumatic stress, compassion satisfaction and posttraumatic growth. Next, we adopted convenient sampling when collecting data, which may limit the universality of the sample, and whether the research results are applicable to other populations or regions needs to be further verified. Finally, the scales used are self-reported, and the results may be biased.
Conclusion
As far as we know, this is the first time to explore the prevalence and internal relationship of secondary traumatic stress, compassion satisfaction and posttraumatic growth among newly graduated nurses. The results of this study suggested that the secondary traumatic stress and compassion satisfaction level of newly graduated nurses were at a moderate level, but the posttraumatic growth level was at a low level, which is affected by work hours, sleep hours and workplace violence experience. Based on this, nursing managers should pay attention to the mental health of newly graduated nurses, reasonably arrange shifts and individual working hours, establish or improve the mental health monitoring platform and work-related violence incident reporting system, regularly evaluate the trauma stress experience and various emotional reactions of newly graduated nurses. Moreover, the structural equation model showed that newly graduated nurses’ compassion satisfaction played a mediating role between secondary traumatic stress and posttraumatic growth. Therefore, nursing managers can also help the newly graduated nurses actively adapt to the environment, speed up the role transformation, improve their clinical nursing ability and pressure resistance ability by carrying out relevant induction training, so as to improve their level of compassion satisfaction, and achieve personal growth.
Data Availability
The data that support the finding of this study are available from the corresponding author upon reasonable request.
Change history
09 January 2024
A Correction to this paper has been published: https://doi.org/10.1186/s12912-023-01681-3
References
Xie J, Li J, Wang S, Li L, Wang K, Duan Y,…, Cheng A. Job burnout and its influencing factors among newly graduated nurses: a cross-sectional study. J Clin Nurs. 2021;30(3–4):508–17. https://doi.org/10.1111/jocn.15567.
Cao X, Chen L. Relationships between resilience, empathy, compassion fatigue, work engagement and turnover intention in haemodialysis nurses: a cross-sectional study. J Nurs Manag. 2021;29(5):1054–63. https://doi.org/10.1111/jonm.13243.
Gong S, Li J, Tang X, Cao X. Associations among professional quality of life dimensions, burnout, nursing practice environment, and turnover intention in newly graduated nurses. Worldviews Evid Based Nurs. 2022;19(2):138–48. https://doi.org/10.1111/wvn.12568.
Monaghan T. A critical analysis of the literature and theoretical perspectives on theory-practice gap amongst newly qualified nurses within the United Kingdom. Nurse Educ Today. 2015;35(8):e1–e7. https://doi.org/10.1016/j.nedt.2015.03.006.
Xie J, Wu X, Li J, Li X, Xiao P, Wang S, Zhong Z, Ding S, Yan J, Li L, Cheng A. Time management disposition and relevant factors among new nurses in chinese tertiary hospitals: a cross-sectional study. Front Psychol. 2022;13:956945. https://doi.org/10.3389/fpsyg.2022.956945.
Guo N, Zhang M, Wu X, Li Z, Zhang Y. Satisfaction and influencing factors of standardized training for new nurses. Chin Nurs Manage. 2022;22(1):101–6.
Woo M, Newman SA. The experience of transition from nursing students to newly graduated registered nurses in Singapore. Int J Nurs Sci. 2020;7(1):81–90. https://doi.org/10.1016/j.ijnss.2019.11.002.
Lin M, Wang JL, He HJ, Li JW, Zhuang LL. Study on the current status and influencing factors of clinical nurses’ posttraumatic growth. Med Soc. 2020;33(7):82–5.
Mangoulia P, Koukia E, Alevizopoulos G, Fildissis G, Katostaras T. Prevalence of secondary traumatic stress among Psychiatric Nurses in Greece. Arch Psychiatr Nurs. 2015;29(5):333–8. https://doi.org/10.1016/j.apnu.2015.06.001.
Wang J, Okoli C, He H, Feng F, Li J, Zhuang L,…, Lin M. Factors associated with compassion satisfaction, burnout, and secondary traumatic stress among chinese nurses in tertiary hospitals: a cross-sectional study. Int J Nurs Stud. 2020;102:103472. https://doi.org/10.1016/j.ijnurstu.2019.103472.
Cavanagh N, Cockett G, Heinrich C, Doig L, Fiest K, Guichon JR,…, Doig CJ. Compassion fatigue in healthcare providers: a systematic review and meta-analysis. Nurs Ethics. 2020;27(3):639–65. https://doi.org/10.1177/0969733019889400.
Tedeschi RG, Cann A, Taku K, Senol-Durak E, Calhoun LG. The posttraumatic growth inventory: a revision integrating existential and spiritual change. J Trauma Stress. 2017;30(1):11–8. https://doi.org/10.1002/jts.22155.
Veronese G, Pepe A, Massaiu I, De Mol AS, Robbins I. Posttraumatic growth is related to subjective well-being of aid workers exposed to cumulative trauma in Palestine. Transcult Psychiatry. 2017;54(3):332–56. https://doi.org/10.1177/1363461517706288.
Lee J, Blackmon BJ, Lee JY, Cochran DJ, Rehner TA. An exploration of posttraumatic growth, loneliness, depression, resilience, and social capital among survivors of Hurricane Katrina and the Deepwater Horizon Oil spill. J Community Psychol. 2019;47(2):356–70. https://doi.org/10.1002/jcop.22125.
Zerach G, Shalev TB. The relations between violence exposure, posttraumatic stress symptoms, secondary traumatization, vicarious post traumatic growth and illness attribution among psychiatric nurses. Arch Psychiatr Nurs. 2015;29(3):135–42. https://doi.org/10.1016/j.apnu.2015.01.002.
Zeng L, Zhang X, Wang F, Yun J, Lai L, Jin M,…, Wang J. Prevalence and influencing factors of posttraumatic growth among nurses suffering from workplace violence: a cross-sectional study. Int J Ment Health Nurs. 2022;31(3):639–49. https://doi.org/10.1111/inm.12984.
Peters E. Compassion fatigue in nursing: a concept analysis. Nurs Forum. 2018;53(4):466–80. https://doi.org/10.1111/nuf.12274.
Yu H, Jiang A, Shen J. Prevalence and predictors of compassion fatigue, burnout and compassion satisfaction among oncology nurses: a cross-sectional survey. Int J Nurs Stud. 2016;57:28–38. https://doi.org/10.1016/j.ijnurstu.2016.01.012.
Stokar YN, Pat-Horenczyk R. Effects of end-of-life care on medical health professionals: a dialectical approach. Palliat Support Care. 2022;20(1):76–83. https://doi.org/10.1017/S1478951521000365.
Osborne JW, Costello AB. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Practical Assess Res Evaluation. 2009;10(7):1–9.
Jin, M., Zhang, Y., Wang, F., Huang, J., Feng, F., Gong, S.,… Wang, J. (2022). A cross sectional study of the impact of psychological capital on organisational citizenship behaviour among nurses: Mediating effect of work engagement. J Nurs Manag, 30(5), 1263–1272. doi: 10.1111/jonm.13609.
Stamm BH. (2010). The Concise Proqol Manual, 2nd edn. Pocatello, ID. [Cited 1 January 2021]. Available from: http://www.proqol.org/uploads/ProQOL_Concise_2ndEd_12-2010.pdf.
Zheng X, Yang M, Gao W, Chen FF. The chinese version Professional Quality of Life Scale: testing of reliability and validity in nurses. J Nurs Sci. 2013;28(5):13–5.
Tedeschi RG, Calhoun LG. The Posttraumatic Growth Inventory: measuring the positive legacy of trauma. J Trauma Stress. 1996;9(3):455–71. https://doi.org/10.1007/BF02103658.
Wang J, Chen Y, Wang YB, Liu XH. Revision of the posttraumatic growth inventory and testing its reliability and validity. J Nurs Sci. 2011;26(14):26–8.
Xie, W., Chen, L., Feng, F., Okoli, C., Tang, P., Zeng, L.,… Wang, J. (2021). The prevalence of compassion satisfaction and compassion fatigue among nurses: A systematic review and meta-analysis. Int J Nurs Stud, 120, 103973. https://doi.org/10.1016/j.ijnurstu.2021.103973.
Jang I, Kim Y, Kim K. Professionalism and professional quality of life for oncology nurses. J Clin Nurs. 2016;25(19–20):2835–45. https://doi.org/10.1111/jocn.13330.
Chang AK, Yoon H, Jang JH. Predictors of posttraumatic growth of intensive care unit nurses in Korea. Jpn J Nurs Sci. 2021;18(4):e12427. https://doi.org/10.1111/jjns.12427.
Jung SY, Park JH. Association of nursing work environment, relationship with the Head Nurse, and resilience with post-traumatic growth in Emergency Department Nurses. Int J Environ Res Public Health. 2021;18(6). https://doi.org/10.3390/ijerph18062857.
Cui PP, Wang PP, Wang K, Ping Z, Wang P…, Chen C. Post-traumatic growth and influencing factors among frontline nurses fighting against COVID-19. Occup Environ Med. 2021;78(2):129–35. https://doi.org/10.1136/oemed-2020-106540.
Dall’Ora C, Griffiths P, Ball J, Simon M, Aiken LH. Association of 12 h shifts and nurses’ job satisfaction, burnout and intention to leave: findings from a cross-sectional study of 12 european countries. BMJ Open. 2015;5(9):e8331. https://doi.org/10.1136/bmjopen-2015-008331.
Stimpfel AW, Fletcher J, Kovner CT. A comparison of scheduling, work hours, overtime, and work preferences across four cohorts of newly licensed registered nurses. J Adv Nurs. 2019;75(9):1902–10. https://doi.org/10.1111/jan.13972.
Kwak Y, Han Y, Song JS, Kim JS. Impact of emotional labour and workplace violence on professional quality of life among clinical nurses. Int J Nurs Pract. 2020;26(1):e12792. https://doi.org/10.1111/ijn.12792.
Kalaitzaki A, Tamiolaki A, Tsouvelas G. From secondary traumatic stress to vicarious posttraumatic growth amid COVID-19 lockdown in Greece: the role of health care workers’ coping strategies. Psychol Trauma. 2022;14(2):273–80. https://doi.org/10.1037/tra0001078.
Chen, R., Sun, C., Chen, J. J., Jen, H. J., Kang, X. L., Kao, C. C.,… Chou, K. R.(2021). A Large-Scale Survey on Trauma, Burnout, and Posttraumatic Growth among Nurses during the COVID-19 Pandemic. Int J Ment Health Nurs, 30(1), 102–116. doi: 10.1111/inm.12796.
Zhang, Y. Y., Han, W. L., Qin, W., Yin, H. X., Zhang, C. F., Kong, C.,… Wang, Y. L.(2018). Extent of compassion satisfaction, compassion fatigue and burnout in nursing:A meta-analysis. J Nurs Manag, 26(7), 810–819. doi: 10.1111/jonm.12589.
Zakeri, M. A., Bazmandegan, G., Ganjeh, H., Zakeri, M., Mollaahmadi, S., Anbariyan,A.,… Kamiab, Z. (2021). Is nurses’ clinical competence associated with their compassion satisfaction, burnout and secondary traumatic stress? A cross-sectional study. Nurs Open, 8(1), 354–363. doi: 10.1002/nop2.636.
Bahari G, Asiri K, Nouh N, Alqahtani N. Professional Quality of Life among Nurses: Compassion satisfaction, Burnout, and secondary traumatic stress: a Multisite Study. SAGE Open Nurs. 2022;8:2095765513. https://doi.org/10.1177/23779608221112329.
Acknowledgements
We are grateful to all participants and funders who took part in the study for their support. This study was supported by Natural Science Project of Sichuan Nursing Vocational College in 2023 (Number: 2023ZRY12) and Humanities and social sciences research planning fund of the Ministry of Education (Number: 22YJA630087).
Funding
This study was supported by Natural Science Project of Sichuan Nursing Vocational College in 2023 (Number: 2023ZRY12) and Humanities and social sciences research planning fund of the Ministry of Education (Number: 22YJA630087).
Author information
Authors and Affiliations
Contributions
Li Zeng: Conceptualization; Data curation; Formal analysis; Methodology; Visualization; Writing - original draft; Writing - review & editing. Jialin Wang: Conceptualization; Investigation; Supervision; Writing - review & editing. Xiangeng Zhang: Investigation; Supervision; Investigation; Resources. Guiling Liu: Writing - review & editing; Formal analysis; Validation. Dong Liu: Data curation; Methodology; Validation. Lan Li: Methodology; Formal analysis; Validation. Man Jin: Investigation; Data curation; Methodology. Xin Li: Formal analysis; Software; Validation.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
In this study, all methods were carried out in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Chengdu University of Traditional Chinese Medicine (Number: 2020-KL084). All participants signed the electronic informed consent form on the front page of the online questionnaire and promised to participate in the study voluntarily. In addition, our research is anonymous. During the survey, we only collected questionnaire information, but not personal information, such as address and account ID.
Consent for publication
Not applicable.
Competing interests
The authors declare that they do not have any conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The affiliations of the first author have been updated.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zeng, L., Zhang, X., Liu, G. et al. Secondary traumatic stress and posttraumatic growth in newly graduated nurses: the mediating role of compassion satisfaction. BMC Nurs 22, 295 (2023). https://doi.org/10.1186/s12912-023-01456-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-023-01456-w