
Abstract
Background
Mobile health applications (mHealth apps) are increasingly being used to perform tasks that are conventionally performed by general practitioners (GPs), such as those involved in promoting health, preventing disease, diagnosis, treatment, monitoring, and support for health services. This raises an important question: can mobile apps replace GPs? This study aimed to systematically search for and identify mobile apps that can perform GP tasks.
Methods
A scoping review was carried out. The Google Play Store and Apple App Store were searched for mobile apps, using search terms derived from the UK Royal College of General Practitioners (RCGP) guideline on GPs’ core capabilities and competencies. A manual search was also performed to identify additional apps.
Results
The final analysis included 17 apps from the Google Play Store and Apple App Store, and 21 apps identified by the manual search. mHealth apps were found to have the potential to replace GPs for tasks such as recording medical history and making diagnoses; performing some physical examinations; supporting clinical decision making and management; assisting in urgent, long-term, and disease-specific care; and health promotion. In contrast, mHealth apps were unable to perform medical procedures, appropriately utilise other professionals, and coordinate a team-based approach.
Conclusions
This scoping review highlights the functions of mHealth apps that can potentially replace GP tasks. Future research should focus on assessing the performance and quality of mHealth apps in comparison with that of real doctors.
Similar content being viewed by others
Background
Mobile technology is rapidly transforming health care, education, and research [1, 2]. Globally, the number of smart phone subscriptions increased significantly from 1800 million in 2013 to 2600 million in 2014, and is estimated to reach 6100 million in 2020 [3]. Mobile health (mHealth) is defined as ‘medical and public health practice supported by mobile devices, such as mobile phones, patient-monitoring devices, personal digital assistants (PDAs), and other wireless devices’ [4]. The usage of mHealth has changed over time, since the first mobile phone was launched in the 1970s to the era of smart phones and wearable devices [5, 6]. mHealth has evolved beyond mobile devices to adopt diverse designs and perform a range of functions. Both patients and health professionals use mHealth for various reasons. According to a survey by the World Health Organization (WHO), mHealth is utilised for 1) communication between individuals and health services (e.g. health call centres); 2) communication between health services and individuals (e.g. appointment reminders); 3) consultation between health care professionals; 4) intersectoral communication in emergencies; 5) health monitoring and surveillance; and 6) access to information for health care professionals at the point of care [4]. The use of mobile devices in health care is considered to alter the delivery, quality, costs, and culture of health care [7, 8].
mHealth can reach large numbers of people and is not limited by borders; more than 100,000 health applications (apps) are available for mobile devices [9]. mHealth has grown dramatically and is beneficial for health care [10], performing numerous tasks such as diagnosing diseases, making appointments, keeping medical records, and supporting clinical decision-making [11,12,13]. However, the disadvantages of using mHealth in health care include the cost of technology and infrastructure, information security, lack of regulatory compliance guidelines, and the potential for serving as a workplace distraction [14, 15]. Moreover, accessibility to mHealth is a major concern in the context of equity in health care services. Evidence shows that the rate of mobile phone subscriptions among the population differs between countries worldwide. For example, in 2009, there were 202.99 subscriptions per 100 population in Estonia and 2.78 subscriptions per 100 population in Eritrea [4].
mHealth also plays important roles in primary care. A study conducted in the USA investigated the use of mobile devices and mHealth for health purposes among patients in primary care. The results showed that 90.1% of outpatients owned mobile phones, 55.3% of patients used smart phones, and 38.5% of patients (69.5% of smart phone owners) used mHealth [16]. Among all patients in this study, 35.5% sought health information from their smart phones, 22.0% accessed an mHealth app, and 20.8% tracked or managed health conditions via mobile devices [16]. Another study presented a new approach in which primary care practitioners prescribed mHealth apps to their patients and discussed the health data collected from the apps in subsequent patient visits [17]. A study of perceptions on mHealth in primary care in Belgium revealed that, among 111 adults from the general population, 41% used mHealth apps for general health check-ups, 18% for follow-up of chronic illnesses, 12% for post-hospitalisation monitoring, and 5% for tele-consultations instead of visiting doctors or hospitals [18]. Moreover, mHealth can contribute to the availability of more real-time and trended data instead of snapshots of the information based on serial visits [19].
Mobile apps are a vital component of mHealth [20, 21]. mHealth apps have been used in health promotion and disease prevention, diagnosis, treatment, monitoring, and the provision of support for health services [5]. These are typically clinical tasks that are conventionally performed by general practitioners (GPs) [22, 23]. Each mHealth app can perform a specific task or several tasks. Accordingly, patients may use a combination of mHealth apps on their mobile devices, which can help them to receive their needs, instead of seeing a GP. This raises the following important question: can mobile apps replace GPs? Although mHealth-related technologies are well designed and constructed, the functionality of these technologies are yet to be compared to the abilities of real doctors. This article aims to comprehensively review mobile apps that can perform GP tasks, and presents a comparison of the possible capabilities of such apps with those of real doctors.
Methods
The authors conducted this scoping review following the PRISMA extension for scoping reviews (PRISMA-ScR) [24].
Identifying GP tasks
This review used the Royal College of General Practitioners (RCGP) guideline on GPs’ core capabilities and competencies as a review framework [25]. In this context, a task is defined as an action relating to doctor-patient interaction performed by a GP during a clinical consultation. Two authors (AW and CHT) independently identified the tasks that should be performed by a GP based on the description of the RCGP guideline. Another author (CJN) participated in conflict resolution between the first two authors. This guideline comprises 13 capabilities and 31 competencies, with 12 tasks identified (Table 1).
App search
Two authors (AW and SW) developed a search term for each task relating to doctor-patient interaction, and identified the final search terms via discussion with the rest of the authors. An author (AW) searched the Google Play Store and two authors (CHT and ET) searched the Apple App Store in July 2018, using the search term for each task. The authors used an Android device for searching Google Play Store and an iOS device for Apple App Store. The authors found some search terms yielded an uncountable list of apps, and most of them were irrelevant, especially the list after the first 20 apps. Thereafter, the author listed the first 20 apps for each task from each app database (Google Play Store and Apple App Store) for subsequent screening.
Screening and selection of apps
Apps that can be used to perform clinical tasks and provide information in English were included. Those that were developed as electronic textbooks, training apps, and games were excluded. Up to the first 20 apps identified based on the Google Play Store and Apple App Store search results for each task, after the exclusion of duplicates and non-English apps, were considered eligible apps. Within each task, two independent review teams reviewed the apps independently: Team 1 (AW and SW) reviewed Android apps from the Google Play Store, while Team 2 (CHT and WJW) reviewed iOS apps from the Apple App Store. Each team assessed the relevant apps based on the app names and descriptions to determine whether they were capable of performing the relevant tasks. In case of uncertainty, the full apps were downloaded and assessed.
Apps that were found to perform several tasks were counted separately. The eligible mHealth apps were those that could perform specific tasks independently without the requirement to consult a real doctor. The final list of mHealth apps was identified after removing duplicates for each task. The authors summarised the results and resolved disagreements through consensus. According to a small number of apps included, the authors identified additional mHealth apps for Android (Google Play Store) and iOS (Apple App Store) mobile devices by using the search terms to search on web browsers manually. The relevant apps were selected by the consensus of the authors.
Data charting process
The tasks were described using the search terms. The number of apps identified via a search of the Google Play Store and Apple App Store, as well as the total number, were presented. Additionally, the number of apps identified by the manual search was reported separately.
Results
Summary of app search results
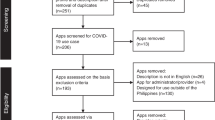
The initial search performed using the search terms for the 12 tasks revealed 437 apps from the Google Play Store (n1 = 240) and Apple App Store (n2 = 197). A total of 419 apps were excluded due to irrelevant app names, descriptions, and functions compared with the identified tasks by two independent review teams (Additional file 1). Of the 18 eligible apps, one duplicate within the same task was removed. The final analysis of apps from the Google Play Store and Apple App Store included 17 apps. The manual search on web browsers revealed an additional 21 apps. Figure 1 presents the app review flow diagram.

Flow diagram of the app review process
Summary of the comparison between mobile apps and GP tasks
This scoping review revealed that nine out of 12 tasks could be potentially replaced by mHealth apps. The apps found by searching the Google Play Store and Apple App Store addressed the following three tasks: 1) apply a structured approach to data gathering and investigation; 2) interpret findings accurately to reach a diagnosis; and 3) support people through individual experiences of health, illness, and recovery. The manual search on web browsers identified several mHealth apps that were able to replace GPs in performing more clinical tasks (Table 2). A summary of the mHealth apps that can perform clinical tasks is presented in Table 3.
Discussion
This scoping review identified mobile apps that are capable of performing GP tasks. mHealth apps were found to exhibit the potential to replace GPs in taking medical history and making a diagnosis; performing some physical examinations; supporting clinical decision-making and management; assisting in urgent, long-term, and disease-specific care; and performing health promotion. However, mHealth apps were unable to perform medical procedures, appropriately utilise other professionals, and coordinate a team-based approach.
mHealth apps serve diverse purposes and perform a range of functions for both patients and health care providers [26, 27]. This scoping review focused on mHealth apps utilised by patients for health purposes. The findings suggest that mHealth apps have the potential to perform several specific clinical tasks that are conventionally performed by a GP. Previous studies have reported the roles of mHealth apps for patients with specific clinical goals, such as pain self-management and weight management [28, 29]. Such mobile app functions may replace several GP tasks, for example, an app for diagnosis could help users make decisions regarding further treatment options, therefore potentially replacing a GP for this purpose. However, most apps, especially apps for history taking and diagnosis, have been found to lack the potential to replace a consultation with a GP. The apps were only found to be suitable for providing primary information and health-related suggestions.
Some GP tasks could not be performed by mHealth. For example, mHealth apps could not perform medical procedures. However, mHealth apps, together with other supportive technologies, have the potential to support clinical tasks. Examples of technologies capable of supporting mHealth approaches include near-field communication (NFC) (a short-range, wireless connectivity technology), accelerometers (a technology used to measure gravitational forces and accelerations), gyroscopes (a micro-electromechanical system sensor used to measure body movement), artificial intelligence (AI), and machine learning [30,31,32]. For example, NFC can be used to monitor human’s physiological information (e.g. heart rate, body temperature) [33]. Accelerometers and gyroscopes can function as motion sensors to monitor daily activities, falls, and sleep patterns [34].
The other competencies of GPs comprise personal attributes, including attitudes, practical skills, and soft skills, which mHealth apps cannot currently replace. Nevertheless, mHealth apps may support GPs in terms of training and referencing. In the future, the development of technologies could contribute to more efficient functions of the mHealth. For example, AI and machine learning may enable machines to learn essential skills, as well as develop attitudes and a mindset similar to those of a good doctor.
Although the findings revealed that mHealth apps were able to perform some GP tasks, it could not be concluded that mHealth apps could replace GPs. Being a medical doctor requires integrative skills, art, values, and ethics [35, 36]. For example, taking history without physical examination may lead to unnecessary investigations and a misdiagnosis. From the results of this review, some apps were able to perform multiple tasks. Their integrative functionality could not replace the comprehensive functions of GPs. Using modern technologies such as mHealth can facilitate the quality of care. Many mHealth apps offer platforms for telemedicine to facilitate doctor-patient communication, which is cost-effective and timely [37]. A study explored doctor-patient communication through screen-to-screen versus face-to-face consultations showed no significantly different results regarding the quality of doctor-patient communication [38]. However, using mHealth apps without human interactions cannot replace seeing a GP.
mHealth apps may additionally present several risks to the user, including loss of privacy, poor-quality patient data, and inappropriate clinical management of the user [39]. To address these risks, basic standards should be met, including accessibility, appropriate privacy, accuracy and credibility of content, and ethical obligations [40, 41]. The differing views in regard to medical technology among patients and doctors are also an area of concern [42]. Such differing perceptions may lead to misunderstandings and arguments between patients and doctors in general practice. GPs should aim to serve as expert sources of digital health information for their patients [43]. Therefore, ‘expertise in the use of appropriate mHealth-related technologies’ should be recognised as an additional competency of GPs.
The present scoping review was conducted based on the UK RCGP guideline as a framework. This approach enabled specification of the functions of mHealth apps compared with GP tasks, which was a major strength of this study. However, there were three limitations of this review. First, the search terms used may have limited the search results. This review used only one search term for each task and did not use any alternative terms. Second, the review did not include all mHealth apps from the Google Play Store and Apple App Store because an exhaustive list of all apps for some tasks was not possible to obtain. The authors resolved these problems by including only the first 20 apps found for each task from each app database. Additionally, to identify additional apps for each task, the authors performed a manual search based on discussion. Finally, this scoping review focused on the functions of apps, however, it was unable to evaluate the quality and credibility of the apps. This reflected a characteristic of scoping review, which primarily focused on identifying knowledge gaps and key characteristics related to a concept [44].
Conclusions
mHealth apps have the potential to replace some GP tasks (nine out of 12 tasks), whereas a GP is expected to be competent in all tasks and with respect to all attributes. Innovative technologies, such as AI and machine learning, are anticipated to play important roles in improving mHealth apps to achieve the capability to perform additional GP tasks and possess more of their attributes. There is a need to balance the advantages and disadvantages of the use of mHealth in health care. GPs should understand and prevent the risks of using mHealth apps. Expertise in the use of appropriate mHealth-related technologies should be recognised as an essential competency of GPs. Future research should focus on assessing the performance and capabilities of mHealth apps compared with those of real doctors.
Availability of data and materials
All data analysed during this study are included in this published article and its additional files.
Abbreviations
- AI:
-
Artificial intelligence
- Apps:
-
Applications
- GPs:
-
General practitioners
- mHealth:
-
Mobile health
- NFC:
-
Near-field communication
- PDAs:
-
Personal digital assistants
- RCGP:
-
Royal College of General Practitioners
- UK:
-
United Kingdom
- USA:
-
United States of America
- WHO:
-
World Health Organization
References
Marcolino SM, Oliveira QJA, D'Agostino M, Ribeiro LA, Alkmim MMB, Novillo-Ortiz D. The impact of mHealth interventions: systematic review of systematic reviews. JMIR Mhealth Uhealth. 2018;6(1):e23.
Mohapatra D, Mohapatra M, Chittoria R, Friji M, Kumar S. The scope of mobile devices in health care and medical education. Int J Adv Med Health Res. 2015;2(1):3–8.
Ericsson. Ericsson Mobility Report: On the pulse of the networked society. 2015. https://www.ericsson.com/assets/local/mobility-report/documents/2015/ericsson-mobility-report-june-2015.pdf. Accessed 11 July 2018.
World Health Organization. mHealth: new horizons for health through mobile technologies: second global survey on eHealth. Geneva: World Health Organization; 2011.
Ali EE, Chew L, Yap KY-L. Evolution and current status of mhealth research: a systematic review. BMJ Innov. 2016;2(1):33.
Bradway M, Carrion C, Vallespin B, Saadatfard O, Puigdomènech E, Espallargues M, et al. mHealth assessment: conceptualization of a global framework. JMIR mHealth and uHealth. 2017;5(5):e60.
Meskó B, Drobni Z, Bényei É, Gergely B, Győrffy Z. Digital health is a cultural transformation of traditional healthcare. mHealth. 2017;3:38.
West D. How mobile devices are transforming healthcare. Issues Technol Innov. 2012;18:1–14.
Carroll JK, Moorhead A, Bond R, LeBlanc WG, Petrella RJ, Fiscella K. Who uses mobile phone health apps and does use matter? A secondary data analytics approach. J Med Internet Res. 2017;19(4):e125.
Klasnja P, Pratt W. Healthcare in the pocket: mapping the space of mobile-phone health interventions. J Biomed Inform. 2012;45(1):184–98.
Boulos MNK, Brewer AC, Karimkhani C, Buller DB, Dellavalle RP. Mobile medical and health apps: state of the art, concerns, regulatory control and certification. Online J Public Health Inform. 2014;5(3):229.
Hsu J, Liu D, Yu YM, Zhao HT, Chen ZR, Li J, et al. The top Chinese mobile health apps: a systematic investigation. J Med Internet Res. 2016;18(8):e222.
Mosa ASM, Yoo I, Sheets L. A systematic review of healthcare applications for smartphones. BMC Med Inform Decis Mak. 2012;12:67.
Bajwa M. mHealth security. Pak J Med Sci. 2014;30(4):904–7.
Katz-Sidlow RJ, Ludwig A, Miller S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595–9.
Bauer AM, Rue T, Keppel GA, Cole AM, Baldwin L-M, Katon W. Use of mobile health (mHealth) tools by primary care patients in the WWAMI region practice and research network (WPRN). J Am Board Fam Med. 2014;27(6):780–8.
Lopez Segui F, Pratdepadua Bufill C, Abdon Gimenez N, Martinez Roldan J, Garcia CF. The prescription of mobile apps by primary care teams: a pilot project in Catalonia. JMIR Mhealth Uhealth. 2018;6(6):e10701.
Mutebi I, Devroey D. Perceptions on mobile health in the primary healthcare setting in Belgium. mHealth. 2018;4:44.
Shaw RJ, Bonnet JP, Modarai F, George A, Shahsahebi M. Mobile health technology for personalized primary care medicine. Am J Med. 2015;128(6):555–7.
Lu C, Hu Y, Xie J, Fu Q, Leigh I, Governor S, et al. The use of mobile health applications to improve patient experience: cross-sectional study in Chinese public hospitals. JMIR mHealth and uHealth. 2018;6(5):e126.
Ventola CL. Mobile devices and apps for health care professionals: uses and benefits. P T. 2014;39(5):356–64.
Grol SM, Molleman GRM, Kuijpers A, van der Sande R, Fransen GAJ, Assendelft WJJ, et al. The role of the general practitioner in multidisciplinary teams: a qualitative study in elderly care. BMC Fam Pract. 2018;19(1):40.
Mash R, Ogunbanjo G, Naidoo S, Hellenberg D. The contribution of family physicians to district health services: a national position paper for South Africa. S Afr Fam Pract. 2015;57(3):54–61.
Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Royal College of General Practitioners. Core capabilities and competences. http://www.rcgp.org.uk/training-exams/training/gp-curriculum-overview/online-curriculum/1-being-a-gp/core-capabilities-and-competences.aspx. Accessed 31 July 2018.
Mendiola MF, Kalnicki M, Lindenauer S. Valuable features in mobile health apps for patients and consumers: content analysis of apps and user ratings. JMIR Mhealth Uhealth. 2015;3(2):e40.
Seabrook HJ, Stromer JN, Shevkenek C, Bharwani A, de Grood J, Ghali WA. Medical applications: a database and characterization of apps in apple iOS and android platforms. BMC Res Notes. 2014;7:573.
Lalloo C, Shah U, Birnie KA, Davies-Chalmers C, Rivera J, Stinson J, et al. Commercially available smartphone apps to support postoperative pain self-management: scoping review. JMIR Mhealth Uhealth. 2017;5(10):e162.
Rivera J, McPherson A, Hamilton J, Birken C, Coons M, Iyer S, et al. Mobile apps for weight management: a scoping review. JMIR Mhealth Uhealth. 2016;4(3):e87.
Bravo J, Hervás R, Fontecha J, González I. M-health: lessons learned by m-experiences. Sensors (Basel). 2018;18(5):1569.
Guo J, Li B. The application of medical artificial intelligence technology in rural areas of developing countries. Health Equity. 2018;2(1):174–81.
Wahl B, Cossy-Gantner A, Germann S, Schwalbe NR. Artificial intelligence (AI) and global health: how can AI contribute to health in resource-poor settings? BMJ Glob Health. 2018;3(4):e000798.
Cao Z, Chen P, Ma Z, Li S, Gao X, Wu RX, et al. Near-field communication sensors. Sensors (Basel). 2019;19(18):E3947.
Majumder S, Deen MJ. Smartphone sensors for health monitoring and diagnosis. Sensors (Basel). 2019;19(9):E2164.
Faustinella F, Jacobs RJ. The decline of clinical skills: a challenge for medical schools. Int J Med Educ. 2018;9:195–7.
Gallagher S, Little M, Hooker C. The values and ethical commitments of doctors engaging in macroallocation: a qualitative and evaluative analysis. BMC Med Ethics. 2018;19(1):75.
Di Cerbo A, Morales-Medina JC, Palmieri B, Iannitti T. Narrative review of telemedicine consultation in medical practice. Patient Prefer Adherence. 2015;9:65–75.
Tates K, Antheunis ML, Kanters S, Nieboer TE, Gerritse MB. The effect of screen-to-screen versus face-to-face consultation on doctor-patient communication: an experimental study with simulated patients. J Med Internet Res. 2017;19(12):e421.
Lewis TL, Wyatt JC. mHealth and mobile medical apps: a framework to assess risk and promote safer use. J Med Internet Res. 2014;16(9):e210.
Larson RS. A path to better-quality mHealth apps. JMIR Mhealth Uhealth. 2018;6(7):e10414.
Cvrkel T. The ethics of mHealth: moving forward. J Dent. 2018;74:S15–20.
Boeldt DL, Wineinger NE, Waalen J, Gollamudi S, Grossberg A, Steinhubl SR, et al. How consumers and physicians view new medical technology: comparative survey. J Med Internet Res. 2015;17(9):e215.
Baird A, Nowak S. Why primary care practices should become digital health information hubs for their patients. BMC Fam Pract. 2014;15(1):190.
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143.
Acknowledgments
We wish to thank Ms. Atchara Aidwang for her assistance with the search results.
Funding
This work was partially supported by Walailak University under the new strategic research (P2P) project (grant number: CGS-2019-047). The funding body had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
AW, CHT, and SW initiated and developed the review strategy. AW, CHT, SW, ET, and WJW performed searches and screenings. AW, CHT, and CJN contributed to data charting process. AW, CHT, SW, CJN wrote the first draft of the manuscript. All authors approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Summary of screening and selection of apps.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wattanapisit, A., Teo, C.H., Wattanapisit, S. et al. Can mobile health apps replace GPs? A scoping review of comparisons between mobile apps and GP tasks. BMC Med Inform Decis Mak 20, 5 (2020). https://doi.org/10.1186/s12911-019-1016-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12911-019-1016-4