
Abstract
Background
Unintended pregnancy predisposes women to unsafe abortion, malnutrition, mental illness, and even death. Though adolescent girls and young women are at higher risk of unintended pregnancy, there is a paucity of evidence in its burden and associated factors in sub-Saharan Africa. Therefore, this study aimed to assess the prevalence and factors associated with unintended pregnancy among adolescent girls and young women in sub-Saharan Africa.
Method
This study was a secondary data analysis of 36 sub-Saharan African countries with a total weighted sample of 17,797 adolescent girls and young women. A multilevel logistic regression model was fitted and, the Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI) was reported to assess the association between the independent variables and unintended pregnancy in Sub-Saharan Africa.
Result
The pooled prevalence of unintended pregnancy in sub-Saharan Africa was 30.01 with 95% CI (29.38–30.74). In multivariable multilevel logistic regression analysis, adolescent girls, and young women with higher education (AOR = 0.71 95%CI 0.52–0.97), those who know modern contraceptive methods (AOR = 0.86 95%CI 0.75–0.98), and traditional contraceptive methods (AOR = 0.90, 95%CI 0.59–0.95), married (AOR = 0.80, 95%CI 0.73–0.88), those from female-headed households (AOR = 0.86,95%CI 0.78–0.94), had lower odds of unintended pregnancy. Whereas adolescent girls and young women from Central Africa (AOR = 2.09,95%CI 1.23–3.55), southern Africa (AOR = 5.23, 95%CI 2.71–10.09), and Eastern Africa (AOR = 1.07,95%CI 1.07–2.66) had higher odds of unintended pregnancy.
Conclusion
Prevalence of unintended pregnancy in Sub-Saharan Africa is high. Therefore, educating adolescent girls and young women, and improving their knowledge about family planning services is vital. It is also better for the government of countries in sub-Saharan Africa and other global and local stakeholders to work hard to ensure universal access to sexual and reproductive healthcare services, including family planning, education, and the integration of reproductive health into national strategies and programs to reduce unintended pregnancy.
Similar content being viewed by others


Background
Unintended pregnancy is a pregnancy that is mistimed, unplanned or unwanted at the time of conception [1]. It is usually an outcome of nonuse, inconsistent use, or incorrect use of effective family planning methods [1, 2]. A recent report from the United Nations sexual and reproductive health agency notified that globally, nearly half of all pregnancies are unintended [3]. Though there has been a reduction in unintended pregnancy globally, low- and middle-income countries are still victims of unintended pregnancy [4, 5]. While the global rate of unintended pregnancies in Europe and North America was 35 per 1000 women aged 15 to 49, in sub-Saharan Africa it was 91 per 1000 women [6]. Similarly, there was a substantial heterogeneity within in sub-Saharan African countries regarding unintended pregnancy [7].
Unintended pregnancy predisposes adolescent girls and young women to several risk factors such as unsafe abortion, maternal death, malnutrition, mental illness and vertical transmission of Human Immuno Virus (HIV) to children, and school dropout [8, 9]. Besides, in sub-Saharan Africa, unintended pregnancy predisposes about 1 in 16 women to psychosocial impacts of morbidity and mortality [10]. It also induces stress, affects women’s quality of life, and the economic status of families at large [11, 12].
In previous studies education [13,14,15,16,17], parity [13, 15, 16], place of residence [13, 18], wealth [13, 18], age [14, 15, 18], healthcare decision-making [14], sexual violence [19], knowledge of contraceptive methods [15,16,17], marital status [16,17,18, 20, 21], occupation [20], sex of household head [20], birth interval [20], region and family planning message [22] have a significant association with unintended pregnancy.
Though unintended pregnancy occurs at any age women, adolescent girls and young women (15–24 years) are at higher risk of unintended pregnancy [23]. Consequently, the risk of maternal mortality is likely to be higher among this age group as evidenced by pieces of literature [24, 25]. Moreover, women in this age category have higher fertility, higher frequency of sexual intercourse, lower knowledge of contraceptive methods, and higher rates of contraceptive failure relative to older women [26,27,28,29]. On the other hand, recent evidence has shown the inequalities and uneven progress in many key sexual health indicators within sub-Saharan Africa which makes adolescent girls and young women to be highly vulnerable to poor sexual health outcomes [30].
Even though they are at higher risk of unintended pregnancy and related complications, there is a paucity of information on the magnitude and its sociodemographic correlates in sub-Saharan Africa. Outside of sexual and reproductive health issues affecting adolescent girls and young women, limited research has been conducted on the broader context of adolescent health in SSA. Thus, a strengthened capacity to generate rigorous scientific evidence to inform policies and programs designed to improve young women’s health is needed. Therefore, this study is aimed to assess the prevalence and factors associated with unintended pregnancy in sub-Saharan Africa among adolescent girls and young women by using the most recent Demographic and health survey data from 36 countries.
Methods
Data source
The dataset for this study was obtained from the measure DHS program after permission was granted at http://www.dhsprogram.com. A total of 36 sub-Saharan African countries’ most recent DHS datasets from 2006 to 2019 were used in this study.
Data from the southern region of Africa (Lesotho, Namibia, Swaziland, and South Africa), the central region of Africa (Angola, Democratic Republic Congo, Congo, Cameroon, Chad, Gabon, Sao Tome & Principe), the Eastern region of Africa (Burundi, Comoros, Ethiopia, Kenya, Madagascar, Malawi, Mozambique, Rwanda, Tanzania, Uganda, Zambia, and Zimbabwe), western Africa (Burkina-Faso, Benin, Cote d’Ivoire, Ghana, Gambia, Guinea, Liberia, Mali, Nigeria, Niger, Sierra Leone, Senegal, and Togo) was included.
Each country’s survey consists of different datasets including men, women, children, birth, and household datasets. For this study, we used the individual records data set (IR file) where data on women’s health is recorded. Demographic and health survey is conducted at the five-year interval and follows a common execution procedure in each country.
A two-stage stratified sampling procedure is adopted to select study participants in each survey. In the first phase, Enumeration Areas (EAs) were selected based on the sampling frame of each respective country. In the second stage, a sample of households is drawn from each EA. Then eligible study participants were interviewed in the selected household. The detail of the sampling procedure has been documented elsewhere [31]. For the current, study a total of 17,797 (weighted sample) adolescent girls and young women [15,16,17,18,19,20,21,22,23,24] having a pregnancy at the time of the interview in 36 sub-Saharan African countries were included (Table 1). During analysis sampling weight was applied using individual sample weights recorded in the data set to produce reliable estimates by adjusting the over and under-sampled regions.
Study variables
Dependent variable
The dependent variable for this study was unintended pregnancy. It was measured in such a way, by asking women about their pregnancy to state just when they wanted their pregnancy (then, later, or not at all). Those women responding to the above question as ‘wanted later’ or ‘not wanted at all were considered to have an unintended pregnancy and those who responded by saying ‘wanted then’ were considered to have intended pregnancy. Therefore, unintended pregnancy was coded ‘1’, and intended pregnancy was coded ‘0’ for further statistical analysis.
Independent variables
Individual and community-level variables were retrieved from DHS datasets. Age [15,16,17,18,19,20,21,22,23,24], educational level (no education, primary, secondary, and higher), marital status(single, married,), wealth index (Poorest, Poorer, poor, Richer, and Richest), media exposure (yes, no), heard about family planning from media (yes, no), knowledge of contraceptive methods (no, traditional, modern), distance to health facility (big problem and not a big problem), smoking (yes, no), covered by health insurance (no, yes), sex of household head (male, female) and occupation (not working, working) were individual-level variables. Whereas residence (urban and rural) and SSA region (South Africa, Central Africa, East Africa, and West Africa) were community (country) level variables.
Statistical analysis
The descriptive statistics was presented in Table 2. The overall prevalence of unintended pregnancy among adolescent girls and young women in sub-Saharan Africa with 95%CI was reported. A multilevel logistic regression model was fitted to assess the factors associated with unintended pregnancy. Consequently, four models were fitted. First, the null model without explanatory variables was fitted by using the country as a group variable to assess the community (country) level variance and the applicability of multilevel analysis. Model II and model III were adjusted for individual-level variables and community-level variables respectively. In model IV, both individual-level and community-level variables were fitted simultaneously. Deviance was used for model comparison. Accordingly, the final (Model IV) was the best-fitted model. In bi-variable analysis variables which are eligible for multivariable analysis were selected at a p-value of 0.2. The multi-collinearity was checked using the variance inflation factor (VIF) to avoid the inflation of the effect size of independent variables. In the multivariable analysis, an Adjusted Odds Ratio (AOR) with 95% CI was reported and variables with a p-value ≤0.05 were considered significant determinants of unintended pregnancy.
Result
A total of 17,797 adolescent girls and young women from 36 sub-Saharan African countries were included in this study. The median age of study participants was 20 years with an interquartile range of 4. The majority (70.51%) of the study participants were rural residents. About 31.62% of them had no formal education and above three-fourths of (80.20%) of study, participants were married. Nearly 24% of study participants were from households with the poorest wealth category. About 91% of study participants knew the modern contraceptive method and two-thirds (65.65) of study participants didn’t hear about family planning from the media. Regarding the region of residence majority (36.94) of respondents were from the western part of the Sub-Saharan African region (Table 2).
The pooled prevalence of unintended pregnancy
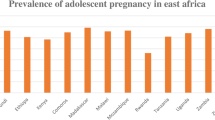
The overall prevalence of unintended pregnancy among adolescent girls and young women in sub-Saharan Africa was 30.01 with a 95% CI (29.38–30.74). The highest magnitude was observed in Southern Africa (60.01%) and the lowest in Eastern Africa (20.39%) region (Fig. 1).

Prevalence of unintended pregnancy in sub-Saharan Africa 2006–2019
Random parameter estimation
The null model indicated that there was a significant clustering of unintended pregnancy across all 36 countries SSA (country/community variance =0.56, p-vale< 0.001). The intracluster correlation coefficient (ICC) ranges from 19.59% null model to 6.9% in the final model (model IV). The Proportional Change in Variance (PCV) also increases from 20.01% from model II to 44.64% in model IV (a model adjusted for individual and community level variables), which indicates 44.64% of the community variance observed in the null model was explained by both individual and community-level factors in full model (model IV). Besides, model fitness was checked using deviance and the model with the lowest deviance (model IV) was the best-fitted model. The variance inflation factor (VIF) is 1.39 which is lower than the recommended cut-off point indicating the absence of a significant correlation between independent variables (Table 3).
Factors associated with unintended pregnancy
In multilevel logistic regression analysis, marital status, educational status, sex of household head, and knowledge of contraceptive method from individual-level variables and sub-Saharan African region from community-level factors were significantly associated with unintended pregnancy.
The odds of unintended pregnancy was decreased by 10% (AOR = 0.90, 95%CI 0.59–0.95) and 14% (AOR = 0.86 95%CI 0.75–0.98) among adolescent girls and young women who know traditional and modern contraceptive methods respectively as compared to women who didn’t know any method. Married women had 20% (AOR = 0.80, 95%CI 0.73–0.88) decreased odds of unintended pregnancy as compared to single women.
The likelihood of unintended pregnancy among adolescent girls and young women from female-headed households was decreased by 14% (AOR = 0.86,95%CI 0.78–0.94) as compared to male-headed households. Adolescent girls and young women with higher educational levels had 29% (AOR = 0.71 95%CI 0.52–0.97) decreased odds of unintended pregnancy as compared to women with no formal education.
Looking at community-level variables, adolescent girls and young women from Central Africa, southern Africa, and Eastern Africa had 2.09 (AOR = 2.09,95%CI 1.23–3.55), 5.23 (AOR = 5.23, 95%CI 2.71–10.09) and 1.07 (AOR = 1.07,95%CI 1.07–2.66) respectively times higher odds of unintended pregnancy as compared to women in Western Africa (Table 4).
Discussion
This study investigated the prevalence and correlates of unintended pregnancy among adolescent girls and young women in sub-Saharan Africa with data from the most recent Demographic and Health Surveys of 36 Sub-Saharan countries. The estimated prevalence of unintended pregnancy was 30.10% with a 95% CI (29.38–30.74). This estimate is higher than the previous pieces of evidence in India (16.9%) [32], Nepal (22.7%) [19], Sri Lanka (17.2%) [16], and South Asian countries (19.1%) [18]. However, it is lower than the prevalence in Pakistan (38.2%) [15], Kenya (41%) [21], and Uganda (37%) [22]. This difference could be attributed to the variation in intervention to reduce the unmet need for contraception, and unintended pregnancies among women which are critical components of family planning programs in developing countries [33].
The odds of untended pregnancy among adolescent girls and young women who know contraceptive methods (traditional and modern) decreased as compared to those who didn’t know any methods. This finding is in line with studies in Pakistan [15] and Sri Lanka [16]. Besides, Studies in Bangladesh and, Nepal reported that poor contraceptive knowledge was significantly associated with unplanned pregnancy [34, 35]. Since contraceptive awareness is directly related to its utilization [36,37,38], women with knowledge of any contraceptive method may have better utilization of family planning methods which help to avoid unintended pregnancy. Thus, it is essential to implement initiatives to improve community knowledge about contraceptive methods with a primary focus on adolescent girls and young women.
This study revealed that education was an important predictor of unintended pregnancy where the odds of unintended pregnancy was decreased among women with higher education. This finding is consistent with a study in Ghana [13, 14], Pakistan [15], and Sri Lanka [16]. The documented pieces of evidence indicated that literate women have a better understanding of their rights and responsibilities and have more freedom, control, and participation in decisions primarily focusing on contraception use and family planning [39,40,41,42]. On the contrary, a study in Nigeria found that better-educated women had higher odds of reported unplanned pregnancies [43].
Consistent with previous pieces of literature [16, 18, 20] married women had lower odds of unintended pregnancy as compared to single ones. This may reflect that a more stable relationship between the couples might have encouraged them to have better decision-making and utilization of family planning methods and timing of conception [44].
Similarly, the odds of unintended pregnancy among adolescent girls and young women from female-headed households was lower as compared to those of male-headed households. This might be due to shared family planning decisions in those female-headed households [20] since the women’s capacity of making reproductive health decisions has a significant effect on unintended pregnancy in the previous study [14]. Besides, the evidence shows that husband-only or wife-only decision-making is associated with a higher risk for women in having both unmet needs for contraception and unintended pregnancy [45]. The region was also a significant predictor of unintended pregnancy in sub-Saharan Africa. Those adolescent girls and young women from central, southern, and eastern Africa had higher odds of unintended pregnancy as compared to those from the western region. This might have happened due to the geographic variation of reproductive health services like contraceptive practice in the region since SSA’s family planning situation remains challenged by weak health systems [46]. For instance, in eastern and southern Africa adolescent sexual and reproductive health services require much promotion to ensure explicit understanding in the community by overcoming diverse cultural confrontations [47]. On the other hand, a recent study has shown that adolescent health services including family planning are increasingly available in West Africa [48].
In general, a closer look at sub-Saharan Africa shows how far behind African countries are in preventing these unplanned pregnancies. The relationship between social and economic development and unintended pregnancy goes both ways. When women and girls are not empowered or lack autonomy, they are less likely to use contraceptives, and then they are prone to unintended pregnancy.
This study has strengths and limitations. It is a pooled data analysis that yields a high sample size and then high power. The other strength is the study considers the clustering effect by applying an advanced model to get reliable standard error and estimates. However, it has the following limitations. Due to the cross-sectional study design, it is difficult to establish the temporal relationship between the predictors and the outcome variable. Besides, there could be a possibility of social desirability bias when women report whether their pregnancy was intended or not.
Conclusion
Unintended pregnancy is a public health problem in sub-Saharan Africa. Educational status, knowledge of contraceptive methods, marital status, sex of household head, and sub-Saharan African region had a significant statistical association with unintended pregnancy.
Therefore, focusing on educating adolescent girls and young women, and improving their knowledge about family planning services through youth-friendly services is vital to reduce unintended pregnancy in sub-Saharan Africa. Moreover, the findings in this study have valuable input to policymakers to reframe their focus on strengthening women’s empowerment in decision-making through education, and in providing youth-friendly services for adolescent girls and young women. In general, the government of countries in sub-Saharan Africa and other global and local stakeholders should work hard on achieving target 3.7 of the Sustainable Development Goals (SDGs) which states: “by 2030, to ensure universal access to sexual and reproductive health-care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programs” [49].
Availability of data and materials
Data is available online and it is possible to access it from www.measuredhs.com.
Abbreviations
- AOR:
-
Adjusted Odds Ratio
- DHS:
-
Demographic health survey
- CI:
-
Confidence Interval
- EAs:
-
Enumeration areas
- ICC:
-
Intra-cluster Correlation
- LLR:
-
Log likelihood ratio
- LR:
-
Likelihood ratio
- SSA:
-
Sub-Saharan Africa
References
[CDC]. CfDCaP. Unintended pregnancy prevention; 2015. 2021. Available from https://www.cdc.gov/reproductivehealth/unintendedpregnancy/ [cited 17 May 2021].
Sserwanja Q, Musaba MW, Mukunya D. Prevalence and factors associated with modern contraceptives utilization among female adolescents in Uganda. BMC Womens Health. 2021;21(1):1–7.
New York. Nearly half of all pregnancies are unintended—a global crisis, says new UNFPA report. 2022. Report No.
Bearak J, Popinchalk A, Alkema L, Sedgh G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical model. Lancet Glob Health. 2018;6(4):e380–e9.
Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plan. 2010;41(4):241–50.
https://theconversation.com/au. https://theconversation.com/unintended-pregnancy-rates-are-highest-in-africa-a-look-at-the-complex-reasons-180454. 2022. Report No.
Bearak JM, Popinchalk A, Beavin C, Ganatra B, Moller A-B, Tunçalp Ö, et al. Country-specific estimates of unintended pregnancy and abortion incidence: a global comparative analysis of levels in 2015–2019. BMJ Glob Health. 2022;7(3):e007151.
Baschieri A, Machiyama K, Floyd S, Dube A, Molesworth A, Chihana M, et al. Unintended childbearing and child growth in northern Malawi. Matern Child Health J. 2017;21(3):467–74.
Claridge AM, Chaviano CL. Consideration of abortion in pregnancy: demographic characteristics, mental health, and protective factors. Women Health. 2013;53(8):777–94.
Abou Zahr C, Wardlaw TM, Choi Y. Maternal mortality in 2000: estimates developed by WHO, UNICEF and UNFPA: World Health Organization; 2004.
Messer LC, Dole N, Kaufman JS, Savitz DA. Pregnancy intendedness, maternal psychosocial factors and preterm birth. Matern Child Health J. 2005;9(4):403–12.
Shah PS, Balkhair T, Ohlsson A, Beyene J, Scott F, Frick C. Intention to become pregnant and low birth weight and preterm birth: a systematic review. Matern Child Health J. 2011;15(2):205–16.
Ameyaw EK. Prevalence and correlates of unintended pregnancy in Ghana: analysis of 2014 Ghana demographic and health survey. Matern Health Neonatol Perinatol. 2018;4(1):1–6.
Ahinkorah BO, Seidu A-A, Appiah F, Baatiema L, Sambah F, Budu E, et al. What has reproductive health decision-making capacity got to do with unintended pregnancy? Evidence from the 2014 Ghana demographic and health survey. PLoS One. 2019;14(10):e0223389.
Habib MA, Raynes-Greenow C, Nausheen S, Soofi SB, Sajid M, Bhutta ZA, et al. Prevalence and determinants of unintended pregnancies amongst women attending antenatal clinics in Pakistan. BMC Pregnancy Childbirth. 2017;17(1):1–10.
Ranatunga IDJC, Jayaratne K. Proportion of unplanned pregnancies, their determinants and health outcomes of women delivering at a teaching hospital in Sri Lanka. BMC Pregnancy Childbirth. 2020;20(1):1–15.
Calvert C, Baisley K, Doyle AM, Maganja K, Changalucha J, Watson-Jones D, et al. Risk factors for unplanned pregnancy among young women in Tanzania. J Fam Plann Reprod Health Care. 2013;39(4):e2.
Sarder A, Islam SMS, Talukder A, Ahammed B. Prevalence of unintended pregnancy and its associated factors: evidence from six south Asian countries. PLoS One. 2021;16(2):e0245923.
Acharya K, Paudel YR, Silwal P. Sexual violence as a predictor of unintended pregnancy among married young women: evidence from the 2016 Nepal demographic and health survey. BMC Pregnancy Childbirth. 2019;19(1):1–10.
Kluckow H, Panisi L, Larui J, Jatobatu A, Kim D, Hodges L, et al. Socio-demographic predictors of unintended pregnancy and late antenatal booking in Honiara, Solomon Islands. Aust N Z J Obstet Gynaecol. 2018;58(3):349–57.
Beguy D, Mumah J, Gottschalk L. Unintended pregnancies among young women living in urban slums: evidence from a prospective study in Nairobi city, Kenya. PLoS One. 2014;9(7):e101034.
Wasswa R, Kabagenyi A, Atuhaire L. Determinants of unintended pregnancies among currently married women in Uganda. J Health Popul Nutr. 2020;39(1):1–17.
Kornides ML, Kitsantas P, Lindley LL, Wu H. Factors associated with young adults’ pregnancy likelihood. J Midwifery Womens Health. 2015;60(2):158–68.
Williamson LM, Parkes A, Wight D, Petticrew M, Hart GJ. Limits to modern contraceptive use among young women in developing countries: a systematic review of qualitative research. Reprod Health. 2009;6(1):1–12.
Hubacher D, Mavranezouli I, McGinn E. Unintended pregnancy in sub-Saharan Africa: magnitude of the problem and potential role of contraceptive implants to alleviate it. Contraception. 2008;78(1):73–8.
Ikamari L, Izugbara C, Ochako R. Prevalence and determinants of unintended pregnancy among women in Nairobi, Kenya. BMC Pregnancy Childbirth. 2013;13(1):1–9.
Chandra-Mouli V, McCarraher DR, Phillips SJ, Williamson NE, Hainsworth G. Contraception for adolescents in low and middle income countries: needs, barriers, and access. Reprod Health. 2014;11(1):1–8.
Trussell J. Contraceptive failure in the United States. Contraception. 2004;70(2):89–96.
Henshaw SK. Unintended pregnancy in the United States. Fam Plan Perspect. 1998:24–46.
Melesse DY, Mutua MK, Choudhury A, Wado YD, Faye CM, Neal S, et al. Adolescent sexual and reproductive health in sub-Saharan Africa: who is left behind? BMJ Glob Health. 2020;5(1):e002231.
Corsi DJ, Neuman M, Finlay JE, Subramanian S. Demographic and health surveys: a profile. Int J Epidemiol. 2012;41(6):1602–13.
Dehingia N, Dixit A, Atmavilas Y, Chandurkar D, Singh K, Silverman J, et al. Unintended pregnancy and maternal health complications: cross-sectional analysis of data from rural Uttar Pradesh, India. BMC Pregnancy Childbirth. 2020;20:1–11.
Obare F, Kabiru CW, Chandra-Mouli V. Reducing early and unintended pregnancies among adolescents; 2018.
Adhikari R, Soonthorndhada K, Prasartkul P. Correlates of unintended pregnancy among currently pregnant married women in Nepal. BMC Int Health Hum Rights. 2009;9(1):1–10.
Roy TK, Singh BP. Correlates of unwanted births in Bangladesh: a study through path analysis. PLoS One. 2016;11(10):e0164007.
Saleem S, Bobak M. Women's autonomy, education and contraception use in Pakistan: a national study. Reprod Health. 2005;2(1):1–8.
Al Riyami A, Afifi M, Mabry RM. Women's autonomy, education and employment in Oman and their influence on contraceptive use. Reprod Health Matters. 2004;12(23):144–54.
Moursund A, Kravdal Ø. Individual and community effects of women's education and autonomy on contraceptive use in India. Popul Stud. 2003;57(3):285–301.
Acharya Y. Women’s education and intra-household autonomy: evidence from Nepal. J Dev Soc Transform. 2008;5(1):5–12.
Maitra P. Effect of socioeconomic characteristics on age at marriage and total fertility in Nepal. J Health Popul Nutr. 2004;22:84–96.
Boonto P. Women’s decision-making power in the rural family in northeastern Thailand. Bangkok: Diss NIDA; 2008.
Chanda SK, Howlader MH, Nahar N. Educational status of the married women and their participation at household decision making in rural Bangladesh. Int J Adv Res Technol. 2012;1(6):137–46.
Sedgh G, Bankole A, Oye-Adeniran B, Adewole IF, Singh S, Hussain R. Unwanted pregnancy and associated factors among Nigerian women. Int Fam Plan Perspect. 2006;32:175–84.
Sanga K, Mola G, Wattimena J, Justesen A. I black K. unintended pregnancy amongst women attending antenatal clinics at the Port Moresby general hospital. Aust N Z J Obstet Gynaecol. 2014;54(4):360–5.
Uddin J, Pulok MH, Sabah M. Couple’s reports of household decision-making, unmet need for contraception, and unintended pregnancy in Bangladesh; 2015.
Tsui AO, Brown W, Li Q. Contraceptive practice in sub-Saharan Africa. Popul Dev Rev. 2017;43(Suppl Suppl 1):166.
Flisher AJ, Mukoma W, Louw J. Evaluating adolescent sexual and reproductive health interventions in southern and eastern Africa, Promoting adolescent sexual and reproductive health in east and southern Africa; 2008. p. 249–66.
Ogundele OJ, Pavlova M, Groot W. Inequalities in reproductive health care use in five west-African countries: a decomposition analysis of the wealth-based gaps. Int J Equity Health. 2020;19(1):1–20.
ECONOMIC UNDF, AFFAIRS. S. Family Planning and the 2030 Agenda for Sustainable Development (data Booklet). UN; 2019.
Acknowledgments
We would like to thank the measure DHS program for providing the data set.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
HGA and AML: Conceptualization, data curation, formal analysis, investigation, methodology, resources, software, validation, visualization, writing original draft, Writing review & editing. YY, MGW, AZA, GAT, TSA, ZTT, and ABT: Data curation, formal analysis, investigation, methodology, resources, software, validation, visualization, writing review & editing. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The DHS data is available to the general public by request in different formats from the Measure DHS website http://www.measuredhs.com. We submitted a request to Measure DHS by briefly stating the objectives of this analysis and thereafter received permission to download the maternal and children’s dataset in STATA format.
Consent for publication
Not applicable.
Competing interests
Authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ayalew, H.G., Liyew, A.M., Tessema, Z.T. et al. Prevalence and factors associated with unintended pregnancy among adolescent girls and young women in sub-Saharan Africa, a multilevel analysis. BMC Women's Health 22, 464 (2022). https://doi.org/10.1186/s12905-022-02048-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-02048-7