
Abstract
Background
Human Immunodeficiency Virus (HIV) is the major public health concern in Ethiopia with more profound effect on women. Discriminatory attitude towards people living with HIV (PLWH) impose a significant impact on patient outcomes and related issues. Hence, this study aimed to investigate the hotspot areas and determinant factors of women’s discriminatory attitude towards people living with HIV.
Methods
An in-depth secondary data analysis was conducted based on Ethiopian demographic and health survey (EDHS) 2016. A total of weighed 13,822 reproductive-age women were included in the analysis. The non-spatial analysis was conducted using Stata 16. A mixed effect multi-level logistic regression model was fitted to identify determinant factors of discriminatory attitude towards PLWH. A p-value < 0.2 and 0.05 were used as a cut-off point to declare statistical significance for the bi- and multi-variable regression models, respectively. Four separate models i.e. the null, individual, community level model, and a fourth combined model were fitted. Model comparison was done using deviance. Random effect parameters such as correlation coefficient, median odds ratio, and proportional change in variance were used to explain the variation between and within clusters. Global and local level spatial analyses were conducted using Global Moran’s index, GetisOrd Gi* statistics, and Spatial scan statistics were conducted.
Results
The magnitude of women’s discriminatory attitude towards PLWH was 62.66% (95%CI: 60.12, 65.10). The discriminatory attitude of women towards PLWH was spatially clustered (Moran’s index = 0.41, P < 0.01). The hotspots of discriminatory attitude towards PLWH were detected in most parts of the Tigray region; Northern, and southeast borders of the Amhara region; Addis Ababa city; Central, Southern, and western Oromiya region; and East, south, and northeastern parts of South Nations, Nationalities and Peoples Region (SNNPR). Being rural resident, and having no media exposure were positively associated while better educational statuses, better wealth index, unmarried, having comprehensive HIV knowledge, Orthodox religion fellow, and ever being tested for HIV were negatively associated with women’s discriminatory attitude towards people living with HIV.
Conclusion
Discriminatory attitude of women towards PLWH was high in Ethiopia. Hotspots were detected in Amhara, Oromiya, SNNPR, Tigray regions, and Addis Ababa city. Socio-demographic, socio-economic, and HIV knowledge-related factors determine the women’s discriminatory attitude towards PLWH.
Similar content being viewed by others


Background
Human immunodeficiency virus (HIV) infection is a medical as well as a social issue[1].Globally, roughly 37.6 million individuals are living with HIV by the year 2020 and around 5000 young women between the ages of 15 and 24 become infected with HIV every week [2].
In Sub-Saharan Africa, new HIV infections account 85%among teenager girls, aged 15 to 19 years [2]. Four thousand five hundred youth population become infected with HIV in Sub-Saharan Africa by the year 2019 accounting for 59% of all new HIV infections in the region [3].
Ethiopia has a concentrated epidemic, with an adult HIV incidence of 0.9% [4]. Among 360,000 reproductive age women (RAW) living with HIV, there were 6,100 newly HIV infected, 6,200 deaths due to AIDS by 2020 in Ethiopia [5].
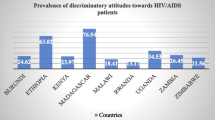
Although stigma and discrimination associated with HIV/AIDS exist globally, it is a major problem in developing countries where a strong cultural, moral, and religious values are highly practiced across communities [6]. In Ethiopia, there is regional variations in the magnitude of discrimination towards HIV/AIDS reported in Dessie (41.93%) [7], Jimma referral hospital (56%) [8], Oromiya (62%) [9], and Amhara region (34%) [10].
Stigma and discrimination within communities and families has adverse consequences including non-adherence to medications, increased psychological distress; physical and emotional/verbal abuse; low social support, isolation; and risky health behaviors such as medication hiding [11]. Moreover, stigma and discrimination is incriminated as a major barrier for the success of HIV prevention and care programs [6]. As a result, people who are at risk of HIV infection or are unsure if they have it may not be tested for HIV due to fear of being stigmatized and the fear of losing privacy and confidentiality about their HIV status in health-care settings [12, 13]. It also leads to avoidance or postponement of needed care and treatment, as well as poor adherence to antiretroviral therapy (ART) which accelerates disease progression [1, 14]. Indeed, such stigma and discrimination related to HIV significantly contributes to the continuation of the HIV epidemic by reducing HIV testing and preventing undiagnosed HIV-positive patients from receiving essential care [15]. It also has an impact on the quality of life of PLWHA, their families, and the healthcare professionals that work with them face losing their job or income, being isolated from their communities, and being unable to contribute as productive members of society [1].
Important factors influencing discriminatory attitudes towards PLWHA are educational status, economic status, employment status, internet use, residence, media exposure, HIV testing, marital status, region, high-risk taking behavior, individuals associated with stigmatized identities, sources of HIV infection, stage of the disease, and relationship with an infected person [1, 6, 16, 17].
Even though HIV-related programs such as education and stigma reduction, behavior change initiatives, expanded HIV testing, and youth programs [18] have grown significantly, negative attitudes and discriminatory practices towards PLWH remain a major and persistent barriers to compressive HIV care service uptakes [3, 19,20,21].
Although large numbers of PLWH are found in Ethiopia and discrimination towards PLWH is high, determinants of discriminatory attitudes towards PLWH have not been well addressed. Few available evidences are done locally but none of them are representative at the country level. This study uses a nationally representative data which is possible to generalize to all Ethiopian reproductive age women. One nationally representative study has been done among all people aged 15–49 regardless of sex of respondents. But it didn’t answer what are determinants of the discriminatory attitude of reproductive age women towards PLWH? Therefore, this study aimed to identify the determinants of women’s discriminatory attitudes towards PLWH among reproductive-age women using the 2016 Ethiopian demographic health survey data.
Methods
Study area and setting
The study is based on 2016 Ethiopian Demographic and Health Survey (EDHS). Ethiopia is the second most populous country in Africa with more than 110 million populations and where several instabilities existed. Ethiopia is one of the high HIV/AIDS burden countries in Africa.
Study design and period
We undertake an in-depth secondary data analysis using evidence EDHS 2016 data set. The EDHS 2016 is a nationwide community-based cross-sectional study. The EDHS was based on 645 enumeration areas. Details of the EDHS methodology and measurements were available in the EDHS reports[22].
Sample size and sampling technique
The national survey used 645 enumeration areas (EAs) as study units. Each EA includes 30 households (HHs)on average. The GPS data was collected as part of the survey and it was collected at cluster (EAs) level [22].From the 645 clusters (EAs), of which 2 EA had missed GPS data, and 22 EAs had zero GPS data which is incorrectly measured and we had excluded them from our analysis. In the meantime 1,314 study participants were excluded because of the missed outcome variable. Additionally, 364 didn’t know whether or not to buy from vendors with HIV, and 263 were not sure whether to allow their children to attend school with HIV-positive children. Moreover, 323 observations were removed because of zero coordinates.
Before analysis, we weight the data using the svy Stata command as per the survey guidelines recommendation to balance the differences in response rates. A total of 13,822 weighted sample sizes were used for the final analysis (Fig. 1).

Data extraction process from EDHS 2016 maternal data
Variables of the study
The dependent variable was women’s discriminatory attitude towards PLWH reported as yes/no. Independent variables are socio-demographic characteristics like age of the woman, types of residence, educational status of women, media exposure, marital status, religion, and wealth index, and HIV-related factors such as being tested for HIV, and Comprehensive knowledge about HIV[22, 23].
Operational definitions
Women’s discriminatory attitude towards PLWHIV(yes/no)
Reproductive age women with discriminatory attitudes towards people living with HIV are those who say that they would not buy fresh vegetables from a shopkeeper or vendor if they knew that person had HIV, or who say that children living with HIV should not be allowed to attend school with children who do not have HIV[22].
Media exposure
Was considered yes, if women read the magazine, use the internet, watch television or listen to the radio at least once a week[22].
Comprehensive knowledge about HIV
Was considered as yes, if the women know that consistent use of condoms during sexual intercourse and having just one uninfected faithful partner can reduce the chances of getting HIV, knowing that a healthy-looking person can have HIV, and rejecting the two most common local misconceptions about transmission or prevention of HIV[22].
Data collection
The survey used pretested and validated standard tools with continuous supervision[22]. For the current analysis, to maintain the data quality, we use the codebooks available from the EDHS 2016 data to extract, clean and recode variables.
Data analysis
Descriptive analysis
we weighed the data before the actual analysis. Proportions and frequencies were used to describe the characteristics of the study participants including figures, tables and narratives.
Spatial analysis
The spatial analysis was done using ArcGIS 10.3 and SaTScanTM TM 9.4 software. The presence of spatial autocorrelation at the national level was assessed using the global morals index (Moran’s I statistics). If Moran’s I is greater than zero, we consider spatial clustering while the reverse will be spatial dispersion. After assessing the national level autocorrelation, we used the Getis-Ord Gi* statistics to identify local level spatial autocorrelation/hotspots. The Z-score was used with the null value of -1.96, + 1.96. If the Z-value is greater than 1.96 it refers to a hotspot/high-risk area while the Z-score <-1.96 indicates cold-spot/low-risk areas. Moreover, the spatial scan statistics was used to identify the most likely hotspot clusters. For spatial scan statistics, the default adjustment for the population at risk was 50% but it is also recommended to use less than 50% considering different conditions [24]. We conducted the spatial scan statistics using the Poisson model by considering the scanning window with 25% of the population at risk. Finally, the Log-likelihood ratio (LLR) with a p-value was reported for significant and most likely high-risk clusters of women’s discriminatory attitude toward PLWH in Ethiopia. The hotspot analysis was based on sampled areas only but considering the non-sampled areas too is very important. The spatial interpolation technique using the empirical Bayesian kriging approach was employed to predict high-risk clusters of women’s discriminatory attitudes towards PLWH in Ethiopia by considering the non-sampled areas.
Multivariable multilevel analysis: a two-stage mixed effect multilevel logistic regression model was used to determine the individual and community level factors affecting women’s discriminatory attitude towards PLWH and to quantify the cluster variability. We fitted four models. Model I: the null model (empty model) was fitted without any independent variable to estimate the intra cluster correlation (ICC) just to show the extent of intra-cluster variation. Model II (Individual level model): was fitted with only individual-level variables to measure the effects of individual level variables. Model III (community level model): where only community level factors like region, types of place of residence were considered, and the final (Model IV) where individual and community level variables were fitted simultaneously to determine the combined effects of individual and community level variables. The adjusted odds ratio (AOR) with 95%CI was reported for significant variables after adjusting for individual and community level variables. The chi-square and multicollinearity assumptions were tested. A P-value < 0.2, and 0.05 were used to declare the level of significance at the bi-variable and multivariable multilevel logistic regressions respectively.
Random effect analysis
The random effects were measured by ICC, median odds ratio (MOR), and proportional change in variance (PCV) [25] The ICC was calculated to evaluate whether the variation in women’s discriminatory attitude towards PLWH is primarily within or between communities. In our article, MOR shows the extent to which the individual probability of women’s discriminatory attitude towards PLWH contributed by the residential area. The PCV was used to quantify the cumulative effect of individual and community level factors on women’s discriminatory attitudes towards PLWH. The deviance (D) was estimated as two times the absolute magnitude of log likelihood to select the better-fitted model. A model with small value of deviance was used as better model to explain the data. The model IV was the better with smallest values of deviance and used for final discussion.
Results
Nearly two-thirds (62.66%: 95%CI: 60.12, 65.10%) of the women in Ethiopia had discriminatory attitudestowards PLWH.Nearly two-thirds (63.08%)of the women were unmarried. More than three-fourths (77.49%) of women had no comprehensive HIV knowledge. Regarding to the HIV test status, more than half (51.68%) of women were not ever tested (Table 1).
Relating to community-level characteristics, three-fourths (75.65%) of women live in rural Ethiopia. nearly half (45.44%) of the women were orthodox religion followers (Table 2)
Hotspots of women’s discriminatory attitude: The distribution of women’s discriminatory attitude was spatially clustered in Ethiopia( Moran’s I = 0.41, P < 0.01). Hence, further spatial analysis techniques were required to detect the local level spatial clusterings (Hotspots) of women’s discriminatory attitudes of women towards PLWH. As shown below by the red dots on the map, hotspots of women’s discriminatory attitudes towards PLWH have been detected in most parts of the Tigray region; Norther, and southeast borders of the Amhara region;Addis Ababa city; Central, Southern, and western Oromia region; and East, south and northeastern parts of SNNPR (Fig. 2)

Hotspot analysis of women’s discriminatory attitude towards PLWH, evidence from EDHS 2016. Shapefile from open Africa
Most likely clusters were detected indifferent regions.Most likely clusters are primary clusters detected by the spatial scan statistics found within the circle of the primary clusters of analysis. These are clusters with highest RR, LLR and lowest and significant p-value.We aggregate the number of women having discriminatory attitude towards PLWH (a case file), and the number of women who respond no for discriminatory attitude as controls. Then we used the case and control file as impute data sets to conduct the purely spatial scan statistics. The observed number of cases were directly aggregated from the data we impute for analysis in a given primary or secondary clusters while the expected number of cases was generated by the software considering the imputed data through the likelihood estimation approach. Primary and secondary clusters are the most high risk areas that should be considered/need primary attention for intervention. The primary clusters are these areas with the highest risk of discriminatory attitude towards PLWH.
The primary high-risk mostlikely clusters were detected in Addis Ababa, Central Oromia, and the Northern part of SNNPR. Secondary clusters were detected inthe Tigray region and the Northern part of the Amhara region. High risk clusters are called hotspot areas. For hotspot analysis using the Get’s Ord Gi* statistics with Z-score > 1.96 is considered as hotspot/high risk areas compared to other clusters (Fig. 3, & Table 3). This shows consistent findings with the Geti’s Ord Gi* hotspot analysis.

Spatial Scan statisticalanalysis of mostlikely significant clusters of women’s discriminatory attitude towards PLWH, evidence from EDHS 2016. Shapefile from open Africa
Empirical Bayesian interpolation was employed to predict the risk of the discriminatory attitude of women towards PLWH. The predicted high-risk clusters were found in the Central, and Northern Tigray region, Addis Ababa city, and South and North Eastern parts of SNNPR with an expected prevalence of 28.83 to 44.00% as stated by the red in the map (Fig. 4) Whereas the cold spots were predicted ineastern Somalia and west Gambela with a predicted prevalence of < 10%.

Empirical Bayesian Kriging prediction of Ethiopian women’s discriminatory attitude towards people living with HIV: Evidence from EDHS 2016. Shapefile from open Africa
The random effect analysis
As evidenced from the empty model, 39.28% (ICC = 0.3928) of variation of the odds of women’s discriminatory attitude towards PLWH was accountedby variations between cluster characteristics. The cluster variability decline successively from 39.28% in the empty model to 14.60, 19.11, and 13.84% in the individual, community level, and final combined models respectively. We found that there was an increased proportion of explained variation in women’s discriminatory attitude towards PLWH as explained by the PCV.i.e 50% increased from the empty model. This implied that 50.00% of the variance in discriminatory attitude towards PLWH was explained by the individual and community level factors together. On top of this, discriminatory attitude towards PLWH was significantly affected by community-level characteristics. Based on the empty model report, the presence of variations between communities was nearly four times (MOR = 4.02) higher than the reference. The unexplained variation in the community decreased to 2.00 in the final model when individual and community level variables were added from the empty model. We compared the model fitness using the deviance, and we found the final model was the best fitted model to explain our data (Table 4).
Fixed effect analysis of determinant factors
Rural resident women had more than two times (AOR = 2.04, 95%CI: 1.64, 2.54) higher odds of discriminatory attitude towardsPLWHcompared to the urban residents.The odds of discriminatory attitude towards PLWH among womenwho had no media exposure was increased by 30% (AOR = 1.30, 95%CI: 1.17, 1.46) as compared to their counterparts.
Compared to protestants, orthodox religion fellow women had more than a third(AOR = 0.67, 95%CI: 0.57, 0.78) fewerodds of discriminatory attitude towards PLWH.Women from the middle, richer and richest households had 18%(AOR = 0.82, 95%CI: 0.69, 0.98), 27%(AOR = 0.73, 95%CI: 0.61, 0.86), and 49% (AOR = 0.51, 95%CI: 0.41, 0.63)lower odds of discriminatory attitude towards PLWHrespectively compared to the poorest households. unmarried women had 25%(AOR = 0.75, 95CI: 0.67, 0.83) lower odds of discriminatory attitude towards PLWH as compared to married women. These women who were ever been tested for HIV had 36%(AOR = 0.64, 95%CI: 0.58, 0.71) lower odds of discriminatory attitude towards PLWH compared to never tested women. Similarly, women who had comprehensive HIV knowledge had 53%(AOR = 0.47, 95%CI: 0.42, 0.52) lowerodds of discriminatory attitude as compared to their counterparts.
Additionally, women who had primary, secondary, and above secondary education had 42%(AOR = 0.58, 95%CI: 0.51, 0.65), 72%(AOR = 0.28, 95%CI: 0.24, 0.33) and 82%(AOR = 0.18, 95%CI:0.14, 0.23) lower odds of discriminatory attituderespectively compared to women with no formal education (Table 5).
Discussion
This study aimed to assess the hotspots and determinants of women’s discriminatory attitudes towards people living with HIV. Nearly two-thirds (62.66%: 95%CI: 60.12, 65.10%) of reproductive-age women in Ethiopia had a discriminatory attitude towards PLWH. This finding was lower than the study conducted among the general population of Ethiopia (62.66 vs. 74.7%) [26] which might be explained by variation in a population where the previous study was among the general public including males and discriminatory attitude was more common in males where discriminatory attitude was 93.8% and 64.5% among males and females, respectively which might have inflated the result in the previous study [27].On the other hand, our finding was higher than a study conducted in Iran [28]. This variation might be due to the difference in the population where the Iran study was on the general public in train stations with better education and socio-economical statuses.
The significant hotspots of discrimination were found in most parts of the Tigray region; Northern, and southeast borders of the Amhara region; Addis Ababa city; Central, Southern, and western Oromia region; and East, south, and northeastern parts of SNNPR. We could not find similar reports to compare.
In our study, rural residents had more than two times higher odds of discriminatory attitudes as compared to urban residents. This finding is supported by other studies conducted in Ethiopia [26, 29], Tajikistan [30], and china [31] which shows individuals who lived in rural residences were more likely to show stigma and discriminatory attitudes compared with their counter parts. Women who are living in urban have access of mass media like television, radio, newspaper, which favor their access for health promotion messages and particularly for stigma- and discrimination-related messages. In addition to this, urban women are more likely to be educated and economically empowered. As result they can have high comprehensive knowledge about HIV/AIDS. These collectively will reduce negative attitude towards PLWH [32].
Women who were not exposed to media had 1.3 times more odds of discriminatory attitudes as compared to those exposed. This is supported by other findings from Ethiopia [1, 26] which might be explained by the fact that women with better media access may have better comprehensive HIV knowledge which can prevent them to avoid unnecessary behaviors like discrimination and stigma and dilutes pre-existing misconceptions regarding HIV/AIDS [1, 33].
Regarding the educational status, women with formal education had fewer odds of discriminatory attitudes towards PLWH. This is supported by other studies findings from Ethiopia [1, 26, 34], Kenya [35],and Nigeria [36] where better educational status was negatively associated with discriminatory attitudes towards PLWH. This might be justified by those individuals with better education who may have access to better information through mass media, the internet, and access to health services related to HIV/AIDS and that will help them to care for and be compassionate for PLWH [1].
On the other hand, married individuals have a more discriminatory attitude toward HIV/AIDS than unmarried women. This is comparable with studies done in Ethiopia [1],
China [37] and Nigeria [36]. It might be due to most married people in Ethiopia living in rural settings and have not attended school to a high level and they might not access the internet, television, and radio due to workload and/or living arrangements [1].
Orthodox religion fellow had less odds of discriminatory attitude compared to Protestants. This is supported by other studies finding from Thai where the Muslim religion fellow had more odds of discriminatory attitude to PLWH [15]. It is evidenced by one study finding on several religious scales and measures of discriminatory attitudes toward blacks, women, homosexuals, and communists, Christian orthodoxy and intrinsic religious orientation were negatively related to these variables [38].
Women with middle, rich, and richest household wealth index had lower odds of discriminatory attitude as compared with the poorest. This is comparable with findings from Thai, Indonesia [39], and Malaysia [17].This might be due to rich people may have better knowledge of HIV, and accessing different behavioral change communications through mass media or social media [40].
Related to HIV-related conditions, women who were ever tested for HIV had lower odds of discriminatory attitudes about PLWH. This is supported by study findings from Ethiopia [26]. Individuals might gain HIV-related information during counseling at the time of HIV testing which may reduce negative attitudes towards HIV-infected people [41].
Women with comprehensive HIV knowledge had lower odds of discriminatory attitudes against PLWH. This was supported by findings from Ethiopia [26], this may be explained by individuals who have no comprehensive HIV knowledge may have misconceptions about modes of transmission and may have a poor understanding of the consequence of discriminatory attitudes [42].
Strengths and limitations
We believe our study had several strengths such as we used nationwide data with better statistical power, and using spatial and multilevel approaches. We don’t hide that the geographic distortion of coordinate data for security purposes may affect the spatial analysis. Additionally, we rely on the available secondary data and important cultural practices, and their HIV statuses were not included. But accuracy of the data could be affected by recall bias since the source of the data was self-report. In addition to this using secondary data limit the researcher to measure all possible determinants like culture and tradition related factors.
Conclusion
Discriminatory attitude of women toward PLWH was high. Hotspots of discriminatory attitudes were identified in Addis Ababa, Oromiya, SNNPR, and Tigray regions of Ethiopia. Different socio-demographic and economic characteristics significantly affect the women’s discriminatory attitude towards PLWH in Ethiopia. Our results suggest that strategies to reduce discriminatory attitudes towards PLWH are needed and very important information, education and communication programmes focusing on stigma and discrimination are needed to reduce misconceptions. Economic empowerment of women should also be considered. In addition, expanding access to HIV counseling and testing services should be done.
Data Availability
The data used for the preparation of this manuscript are available from http://www.dhsprogram.comand anyone can access it through an online request as an authorized user. The authors prepared the data that was used for the preparation of this manuscript can be shared if required.
Abbreviations
- AOR:
-
adjusted odds ratio.
- EDHS:
-
Ethiopian Demographic and Health Survey.
- AIC:
-
Akakie information criterion.
- ICC:
-
Intra class correlation.
- DIC:
-
deviance information criteria.
- MOR:
-
Median Odds Ratio.
- PCV:
-
percentage change in variance.
- PLWH:
-
people living with HIV
- EAs:
-
Enumeration Areas
- RR:
-
Relative Risk
- LLR:
-
log likelihood ratio.
References
Arefaynie M, Damtie Y, Kefale B, Yalew MJHA. Predictors of Discrimination Towards People Living with HIV/AIDS Among People Aged 15–49 Years in Ethiopia. Multilevel Anal. 2021;13:283.
UNAIDS. Global HIV. & AIDS statistics — Fact sheet; 2021. https://www.unaids.org/en/resources/fact-sheet. Accessed 02 Iuly.
Mirkuzie AH, Ali S, Abate E, Worku A, Misganaw A. Progress towards the 2020 fast track HIV/AIDS reduction targets across ages in Ethiopia as compared to neighboring countries using global burden of diseases 2017 data. BMC Public Health. 2021;21(1):285.
UNAIDS. Country factsheets on HIV/AIDS 2020 [Available from: https://www.unaids.org/en/regionscountries/countries/ethiopia.
Wong L, Nur Syuhada AJSAJoTMPH. Stigmatization and discrimination towards people living with or affected by HIV/AIDS by the general public in Malaysia. 2011;42(5):1119.
Adane B, Yalew M, Damtie Y, Kefale B. Perceived Stigma and Associated Factors Among People Living with HIV Attending ART Clinics in Public Health Facilities of Dessie City, Ethiopia. HIV/AIDS (Auckland, NZ). 2020;12:551.
Fido NN, Aman M, Brihnu Z. HIV stigma and associated factors among antiretroviral treatment clients in Jimma town, Ethiopia S. HIV/AIDS (Auckland, NZ). 2016;8:183.
Parcesepe A, Tymejczyk O, Remien R, Gadisa T, Kulkarni SG, Hoffman S, et al. HIV-related stigma, social support, and psychological distress among individuals initiating ART in Ethiopia. AIDS Behav. 2018;22(12):3815–25.
Wodajo BS, Thupayagale-Tshweneagae G, Akpor OA. HIV and AIDS-related stigma and discrimination in two referral hospitals in Ethiopia. Afr J AIDS Res. 2017;16(2):137–44.
Kip EC, Udedi M, Kulisewa K, Go VF, Gaynes BN. Stigma and mental health challenges among adolescents living with HIV in selected adolescent-specific antiretroviral therapy clinics in Zomba District, Malawi. BMC Pediatr. 2022;22(1):253.
Dapaah JM. SKHAc, privacy and confidentiality; the case of two health centres in, https://doi.org/10.1186/s12910- tARoGBe, 27422295 --P.
Musheke MNH, Gari S, McKenzie O, Bond V, Martin-Hilber A, et al. A systematic review of, Africa.BMC qfofeaduoHtiS-S, 23497196 phhdo—P.
Steward WTBS, Ramakrishna J, Heylen E, Ekstrand ML. Stigma is associated with delays in, Providers scaH-ipiIJotIAo, 22282878 oAChdoP.
Srithanaviboonchai K, Chariyalertsak S, Nontarak J, Assanangkornchai S, Kessomboon P, Putwatana P, et al. Stigmatizing attitudes toward people living with HIV among general adult Thai population: Results from the 5th Thai National Health Examination Survey (NHES). 2017;12(11):e0187231.
Harapan H, Feramuhawan S, Kurniawan H, Andalas M, Hossain MB, editors. Factors affecting the level of health care worker’s stigmatized and discriminatory attitude towards people living with HIV: A study at the Dr. Zainoel Abidin General Hospital, Banda Aceh, Indonesia. Proceedings of The Annual International Conference, Syiah Kuala University-Life Sciences & Engineering Chapter; 2011.
Wong LPJPm. Prevalence and factors associated with HIV/AIDS-related stigma and discriminatory attitudes: a cross-sectional nationwide study. 2013;57:S60-S3.
Kibret GD, Ferede A, Leshargie CT, Wagnew F, Ketema DB, Alebel A. Trends and spatial distributions of HIV prevalence in Ethiopia. Infect Dis Poverty. 2019;8(1):90.
Vaishali Mahendra M, Reducing HIV-Related, Stigma. Lessons Learned from Horizons Research and Programs. Public Health Reports. 2010;125.
Assefa Y, Damme WV, Mariam DH, Kloos H. Toward universal access to HIV counseling and testing and antiretroviral treatment in Ethiopia: looking beyond HIV testing and ART initiation. AIDS Patient Care STDs. 2010;24(8):521–5.
Lifson AR, Demissie W, Tadesse A, Ketema K, May R, Yakob B, et al. HIV/AIDS stigma-associated attitudes in a rural Ethiopian community: characteristics, correlation with HIV knowledge and other factors, and implications for community intervention. BMC International Health and Human Rights. 2012;12(1):1–8.
Central Statistical Agency - CSA/Ethiopia ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa: CSA and ICF; 2017.
Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa: CSA and ICF; 2016.
Kulldorff M. SaTScanTM user guide. March; 2018.
Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Commun Health. 2006;60(4):290–7.
Diress GA, Ahmed M, Linger M. Factors associated with discriminatory attitudes towards people living with HIV among adult population in Ethiopia: analysis on Ethiopian demographic and health survey. SAHARA J: Journal of Social Aspects of HIV/AIDS Research Alliance. 2020;17(1):38–44.
Diress GA, Ahmed M, Linger M. Factors associated with discriminatory attitudes towards people living with HIV among adult population in Ethiopia: analysis on Ethiopian demographic and health survey. SAHARA-J: J Social Aspects HIV/AIDS. 2020;17(1):38–44.
Masoudnia E. Public perceptions about HIV/AIDS and discriminatory attitudes toward people living with acquired immunodeficiency syndrome in Iran. SAHARA J: journal of Social Aspects of HIV/AIDS Research Alliance. 2015;12:116–22.
Lifson AR, Demissie W, Tadesse A, Ketema K, May R, Yakob B, et al. HIV/AIDS stigma-associated attitudes in a rural Ethiopian community: characteristics, correlation with HIV knowledge and other factors, and implications for community intervention. BMC Int Health Hum Rights. 2012;12(1):1–8.
Zainiddinov H. Trends and determinants of attitudes Towards People living with HIV/AIDS Among women of reproductive Age in Tajikistan. Central Asian journal of global health. 2019;8(1).
Li X, Yuan L, Li X, Shi J, Jiang L, Zhang C, et al. Factors associated with stigma attitude towards people living with HIV among general individuals in Heilongjiang, Northeast China. BMC Infect Dis. 2017;17(1):1–6.
Khan R, Bilal A, Siddiqui, sH. KNOWLEDGE ABOUT HIV AND DISCRIMINATORY ATTITUDES TOWARD PEOPLE LIVING WITH HIV IN PAKISTAN. Pakistan J Public Health. 2019;9(1):37–41.
Agegnehu CD, Tesema GA. Effect of mass media on comprehensive knowledge of HIV/AIDS and its spatial distribution among reproductive-age women in Ethiopia: a spatial and multilevel analysis. BMC Public Health. 2020;20(1):1420.
Feyissa GT, Abebe L, Girma E, Woldie MJBPH. Stigma and discrimination against people living with HIV by healthcare providers. Southwest Ethiopia. 2012;12(1):1–12.
Kingori C, Haile ZT, Ngatia P, Nderitu R. Factors that can influence feelings towards and interactions with people living with HIV/AIDS in rural Central Kenya. Int J STD AIDS. 2017;28(9):910–9.
Dahlui M, Azahar N, Bulgiba A, Zaki R, Oche OM, Adekunjo FO, et al. HIV/AIDS related stigma and discrimination against PLWHA in Nigerian population. PLoS ONE. 2015;10(12):e0143749.
Chen J, Choe M, Chen S, Zhang S. The effects of individual-and community-level knowledge, beliefs, and fear on stigmatization of people living with HIV/AIDS in China. AIDS Care. 2007;19(5):666–73.
Kirkpatrick LA. Fundamentalism. Christian orthodoxy, and intrinsic religious orientation as predictors of discriminatory attitudes. Journal for the Scientific Study of Religion. 1993:256–68.
Iga PD. Knowledge of HIV/AIDS and discriminatory attitude towards people with HIV/AIDS: analysis of 2017 Indonesia demographic and health survey. Graduate School of Public Health; 2020.
Jung M, Arya M, Viswanath K. Effect of media use on HIV/AIDS-related knowledge and condom use in sub-Saharan Africa: a cross-sectional study. PLoS ONE. 2013;8(7):e68359.
Genberg, B. L, Hlavka, Z, Konda, K. A, Maman, S, Chariyalertsak, S, Chingono, A, Celentano, D. D. (2009). A comparison of HIV/AIDS-related stigma in four countries: Negative attitudes and perceived acts of discrimination towards people living with HIV/AIDS. Social Science & Medicine. 1982;68(12):2279-2287.
Iqbal S, Maqsood S, Zafar A, Zakar R, Zakar MZ, Fischer F. Determinants of overall knowledge of and attitudes towards HIV/AIDS transmission among ever-married women in Pakistan: evidence from the Demographic and Health Survey 2012–13. BMC Public Health. 2019;19(1):1–14.
Acknowledgements
The authors acknowledge the Institute of Public Health, College of Medicine and Health Science, University of Gondar. Our thanks also extend to the international Measure DHS program for permitting data access.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
AGM selects the title, develops the proposal, extracts the data, analysis the data, interpreted the results, and prepared the manuscript first draft. MWM, GMK, MGF and DAB assist in the design, comment, approval of the proposal, and prepare the manuscript. All authors read and approve the final manuscript before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval is not applicable for this study. Because we use secondary (EDHS) data through online requests on the major DHS program website (http://www.dhsprogram.com) in which the primary data was collected following ethical principles. All methods of this research were done following the declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Muluneh, A.G., Merid, M.W., Kassa, G.M. et al. Hotspots and determinants of women’s discriminatory attitude towards people living with HIV; evidence from ethiopian demographic and health survey data. BMC Women's Health 22, 420 (2022). https://doi.org/10.1186/s12905-022-01997-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-01997-3