
Abstract
Objective
More than 2 billion women are experiencing menopause transition in China and some of them suffered from depression; while the risk factors of depression during menopause transition were still unclearin China. We aimed to investigate the risk factors in mid-life women in Southeast China.
Method
This study included 1748 Chinese women aged 40–65 years-old who visited gynecology outpatient department of Women’s hospital School of Medicine, Zhejiang University during 2010–2018. Demographic information was collected, and the modified Kupperman Menopausal Index (mKMI) and Hamilton Rating Scale for Depression were assessed. Circulating levels of sex hormones were tested. Ordinal logistic regression analysis was performed to identify risk factors for depression.
Results
The prevalence of depression symptoms was 47.43%. The majority of women had mild (38.56%) or moderate depressive symptoms (8.00%); only 0.86% had severe depressive symptoms. Compared with perimenopausal women, postmenopausal women had increased risks of more severe depression. The associations between menopausal syndromes and the intensity of depression were strongly positive (OR 6.69, 95% CI 5.39–8.29). Elder age, higher follicle stimulating hormone levels, lower estradiol levels, and fewer parity were positively related with the intensity of depression. Among postmenopausal women, underweight, mKMI > 14, earlier age at menopause, shorter reproductive period, and longer duration after menopause were risk factors for incresed intensity of depression.
Conclusions
The results demonstrated a high proportion of depression in women complaining of menopause. Menopausal symptoms were strongly related to the intensity of depression. In postmenopausal women, estrogen related events are associated with the intensity of depression. Gynecological endocrinologists in China should consider screening for depression in high-risk women.
Similar content being viewed by others


Introduction
In 2019, more than 95 million Chinese people sufffered from depression, 65% of them are female [1]. Worldwide epidemiological studies consistently showed that women had a two-times increased risk of depressive disorders compared with men. The risk was especially pronounced at life stages with sex hormones fluctuations, such as the postnatal period and the menopause transition [2]. Recent results of the Study of Women's Health across the Nation Mental Health Study (SWAN MHS) showed a three-fold increased risk of the development of major depression during the late perimenopausal or postmenopausal period compared with the pre- or early perimenopausal period [3]. China is an ageing scoiety, according to World Health Organization (WHO) statistics, there were 160 million postmenopausal women in China in 2010, and the number of postmenopausal women will reach 280 million by 2030. The incidence of depressive symptoms in women going through menopausal transition has increased significantly. Thus, recognizing depressive symptoms and disorders at an early stage is very important for the management of menopause transition.
Numerous studies have shown a wide range of risk factor domains for depressive symptoms and disorders during the menopause transition, including demographic factors (age, the body mass index (BMI), unemployment, financial problems), health factors (history of depressive disorders), psychosocial factors (upsetting life events,anxiety and depressive symptoms (for major depressive disorder)), hormonal levels (higher follicle stimulating hormone (FSH), luteinizing hormone (LH) and estradiol (E2) level) and menopausal symptoms (vasomotor symptoms, night sweats, increased number of bothersome symptoms) [4,5,6]. Recently, several studies were conducted to determine whether hormone-related events, such as duration of estrogen exposure years, reproductive events, and breast feeding history were related to the risk of depression during menopause transition [7, 8]. However, data on most of these associations are limited and controversial.
In the present study, we aimed to investigate the severity of depression among women experiencing menopause transition and analyze the relationships between demographic characteristics, menopausal symptoms, hormone levels, and depressive symptoms, and further reveal the related factors for depression. Our findings are expected to help health care providers all over the world, especially the gynecological endocrine doctors and general practitioners, to recognize and treat menopausal depressive disorders in early stage, which is very important to prevent severe depression in mid-life women.
Methods
Participants
Subjects were recruited from the gynecology outpatient department of the Women’s Hospital, School of Medicine, Zhejiang University between March 2010 and December 2018. Women who visited the outpatient clinic for the first time either because of complains about changes in their menstrual cycle or other symptoms related to menopause were asked to provide informed consent for the study. The following inclusion criteria were applied: (1) Aged between 40 and 65 years-old; (2) a perimenopausal or postmenopausal status. Women with any of the following conditions were excluded: (1) History of mental diseases or use of antipsychotic drugs; (2) History of sex steroids or oral contraceptives use within the preceding 6 months; (3) History of hysterectomy or oophorectomy; (4) History or evidence of uncontrolled hypertension, diabetes, cardiovascular disease, untreated thyroid disease, renal insufficiency, liver disease, life threatening disease, history of thrombosis, breast cancer, and inability to participate.
The ethical committee of the the Women’s Hospital, School of Medicine, Zhejiang University approved this study.
Demographic data
Demographic and clinical data including age, residence, academic education, monthly income, parity, times of abortion, age at menarche, age at menopause (for postmenopausal women) and chronic health problem were collected by trained interviewers. The reproductive period was calculated as age at menopause minus the age at menarche; the duration after menopause was calculated as monthes between date at visit and the date at menopause. The body mass index (BMI, kg/m2) was calculated and classified according to the Chinese World Health Organization criteria: underweight, BMI < 18.5; normal, 18.5 ≤ BMI < 24; overweight, 24 ≤ BMI < 28; obesity, BMI ≥ 28.
Assessment of the Hamilton Rating Scale for Depression (24-items) (HAM-D24)
The patients were assessed for depressive symptoms and severity using HAMD-24, which contains 24 items (10 items scored from 0 to 2, and 14 items scored from 0 to 4) A total score in range of 0–8, 9–19, 20–34, and ≥ 35 were considered as an indication of non-depression, mild, moderate, and severe depression, respectively.
Assessment of menopausal symptoms and sex steroid concentrations
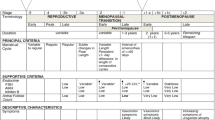
We made a diagnosis of perimenopausal or postmenopausal status according to the 2012 Stages of Reproductive Aging Workshop (STRAW) criteria [9].
Menopausal symptoms were assessed using the modified Kupperman Menopausal Index score (mKMI) [10].
For women with no menstruation, blood samples were collected for hormone tests. Women who still had an identifiable menstrual cycle were asked to undergo hormone tests on the second day of the cycle. The sample was collected from each subject the next morning between 8 and 11 am after overnight fast. Levels of E2, progesterone (P), testosterone (TE), LH and FSH were estimated by ELISA with Roche Modular E170 Analyser, Berlin, Germany. To analyze E2, there was a lower limit of detection of 18.35 pmol/L.
Statistical analysis
Continuous variables with a normal distribution were presented as the mean ± standard deviation and we used one-way analysis of variance (ANOVA) for comparisons Categorical variables were presented as frequency and proportions and compared using chi-squared tests. Ordinal logistic regression analyses with the intensity of depression as the outcome were conducted. The estimates of logistic regression were presented as odds ratios (ORs) and 95% confidence intervals (CIs). In the categorical analyses for E2, for which there was a limitation of detection, women with E2 ≤ 18.35 pmol/L were categorized separately and the remaining women were divided into two groups by median values of E2 with the highest E2 group as the reference category. For categorical analyses of other sex steroids, participants were divided into four groups according to the quartile distribution of each steroid serum level with the lowest fourth as the reference category.
SPSS 23.0 for Windows (IBM Corp., Armonk, NY, USA) was used for all statistical analyses with p < 0.05 as statistically significant.
Results
General characteristics of the participants
A total of 2304 women meeting the inclusion criteria signed informed consent for the study. We then excluded those with history of sex steroids or oral contraceptives use within the preceding 6 months (n = 302), history of mental diseases or the use of antipsychotic drugs (n = 47), history of hysterectomy or oophorectomy (n = 103), history of hysterectomy or oophorectomy (n = 65) and those with uncontroled diseases (n = 39). Thus, a total of 1,748 women were recruited.
The general characteristics of participants are summarized in Table 1. The mean age of the 1,748 women were 48.56 ± 4.60 years old. Most of them were perimenopausal (66.36%), living in urban area (83.52%), employed (73.34%), and highly educated (32.84% with high school and 45.14% with college and above). The mean BMI was 22.19 ± 3.45 kg/m2, and 69.91% of them were considered as normal. Only 4.17% of the study group had chronic health problems. Age, age at menarche, personal income per month, employment status, and depression status were significantly different among women with different menopausal statuses (p < 0.05) (Table 1).
Assessment of depression
The mean HAMD score was 9.06 ± 7.44, and only 52.57% of the participants were considered as non-depressed (HAMD-24 less than 8). The majority of women with depression had mild (38.56%) or moderate symptoms (8.00%), only 0.86% had severe depression (Table 1). Age, employment status, menopausal status, personal income per month, and education were significantly different among women with different levels of depression (p < 0.05).
Menopausal syndrome and depression
The mean mKMI score was 15.10 ± 9.24. The mean mKMI score of 919 women into non-depressiion group was 10.81 ± 6.42. The mean mKMI scores of participants with mild, moderate and severe depressive symptoms were 18.76 ± 8.11, 24.62 ± 11.17 and 35.53 ± 13.57, respectively. The incidence of the mKMI positives (mKMI > 14) was significantly different among the depression subgroups (p < 0.001). Significantly difference of mKMI scores was obervesed between the depression subgroups as well (Table 2).
Sex steroids and depression
Table 3 showed the E2 and FSH serum levels according to the categorical distribution of depression The mean value of serum E2 was 82.45 ± 137.97 (pmol/L). The population was divided into three groups as T1 (E2 ≤ 18.35), T2 (18.35 < E2 ≤ 62.16), T3 (E2 > 62.16). A significant decrease of depression severity was observed with increasing level of serum estradiol (Table 3).
The mean value of serum FSH level was 72.53 ± 35.63 (IU/L). The population was divided into four groups according to the FSH serum levels as Q1 (0 < FSH ≤ 40), Q2 (40 < FSH ≤ 80), Q3 (80 < FSH ≤ 120), Q4 (FSH > 120). No significant difference in the severity of depression was found in each FSH category (Table 3).
No significant associations were observed between depression and P(p = 0.359), TE(p = 0.404), and LH(p = 0.625) levels.
Factors associated with the intensity of depression
Ordinal logistic regression analyses were performed to investigate independent factors associated with the intensity of depression (Table 4, Additional file 1: Table S1).
Age, menopausal status, parity, mKMI score, serum E2, and FSH levels were significantly correlated with the intensity of depression. Postmenopausal stages was positively correlated with the intensity of depression (OR 1.34, 95% CI 1.07–1.69). Women who had never given birth to a child had an increased risk of more severe depression (OR 1.47, 95% CI 1.01–2.13), while more than two parities was negatively correlated with the intensity of depression compared with women who had only one parity (OR 0.72, 95% CI 0.53–0.97). A nearly six times increased risk was observed in women with mKMI score more than 14 (OR 6.69, 95% CI 5.39–8.29).
A significant negative association was found between circulating E2 levels and the intensity of depression. The severity of depression decreased in participants with higher levels of estradiol (T1:T3 OR 1.35, 95%CI 1.06–1.73; T2:T3 1.36, 95%CI 1.04–1.78). For FSH analysis, the opposite result was observed, serum FSH level was positively related to the severity of depression (Q4:Q1 OR 1.62, 95%CI 1.00–2.62; Q3:Q1 OR 1.60, 95%CI 1.15–2.23; Q2:Q1 OR 1.44, 95%CI 1.06–1.97).
For postmenopausal women, we also collected information about the reproductive period, age at menopause, and duration after menopause. The results supported protective effect of later menopause (OR 0.93, 95% CI 0.87–0.99), longer reproductive period (OR 0.93, 95% CI 0.87–1.00), and a potential harmful effect of longer duration after menopause (OR 1.08, 95% CI 1.01–1.16) on the intensity of depression after menopause. Consistent with the whole population, underweight (OR 2.19, 95% CI 1.04–-4.57) and mKMI > 14 (OR 6.18, 95% CI 4.25–-8.98) were also potential risk factors of incresed intensity of depression in postmenopausal women.
In perimenopausal women, age, residence in rural area, parity, and mKMI score were significantly positively related to with the intensity of depression and an mKMI > 14 (OR 7.22, 95% CI 5.52–-9.45) was strongly associated with the intensity of depression as well.
The analyses showed storng associations between mKMI score and the severity of depression. Concerning there were some overlaping symptoms between mKMI and HAMD scales, we analyzed each menopausal symptoms in the mKMI scale sepreately. We found all the 13 symptoms were significantly related to with the severity of depression. Except the melancholia, the most related symptoms were fatigue (OR 3.09, 95% CI 2.68–3.56), vertigo (OR 2.62, 95% CI 2.27–3.02), palpitation (OR 2.51, 95% CI 2.19–2.88) and headache (OR 2.19, 95% CI 1.90–4.52) (Additional file 2: Table S2). The subgroup analysis dividing the time interval into four durations showed our results were stable (Additional file 3: Table S3).
Discussion
In the present study, we explored the risk factors associated with depression among women who had menopausal symptoms in southeast China. We found that nearly half of the participants who visited the gynecology clinic (47.43%) had depression. The majority of women with depression had mild (38.56%) or moderate symptoms (8.00%), and only 0.86% had severe depression. Compared with perimenopausal women, postmenopausal women had increased risks of more severe depression. The relationships between menopausal syndromes and the intensity of depression were strong and positive. Women with elder age, higher serum FSH levels, lower serum E2 levels, and fewer parity had an increased risk of more severe depression.
In this hospital-based study, a relatively higher prevalence of depression (47.75%) was found in middle-aged women compared with other studies conducted in China (11.4–36.3%) [1, 6, 11, 12]. This might be explained by the fact that most of our participants had complaints about menopause, which may lead to increased the risk of depression in this population [12]. Our findings suggested a positive relationship between age and depression during menopausal transition, which was consistent with previous studies in China [1, 13]. Several studies stated that poor general health status of older women might contribute to this relationship [1]. However, in our study, most of the participants had good health status (95.83% did not have disease history), which suggested that the higher prevalence of depression in older women was mainly caused by the physiological and psychological changes during menopause transition.
In our study, we found strong positive correlations between menopausal symptoms (measured by mKMI) and the intensity of depression. Certain menopausal complaints co-occurred and overlapped with the presentation of mood disturbance during this stage. The associations between menopausal symptoms and depression had been reported by several studies [11, 12, 14, 15]. However, most studies focused on vasomotor symptoms (VMS), sleeping difficulties or other symptoms separately [12, 14]. Our result showed that not only VMS and sleeping difficulties, but also the other menopausal symptoms are associated with incresed intensity of depression in this period, and women with elevated mKMI scores was strongly associated with the intensity of depression during the menopause transition and the most related symptoms are fatigue, vertigo, palpitations and headaches.
The association between menopause status and the intensity of depression has been studied extensively [16, 17], positive correlation between perimenopause and depression has been observed in both cross-sectional studies and longitudinal studies. For example, a meta-analysis reported that the OR of the presence of depressive symptoms during the perimenopause were doubled when compared with those for premenopausal women. However, the analysis comparing the occurrence of depressive symptoms in the perimenopause versus that in the postmenopause revealed negative results [17]. By contrast, our results showed positive correlation with postmenopausal state and the intensity of depression. A possible explanation for the inconsistent results is that most of the postmenopausal women in our study were in the early postmenopausal stage and had complains of menopausal symptoms; thus, these women experienced a longer period with unpleasant feelings, which may lead to more depression symptoms.
The relationship between body mass index (BMI) and depression during the menopause transition is controversial. Several studies indicated associations between overweight, obesity and depression [18, 19], while others did not [11]. Studies of BMI and depression in general Asian populations had reported a U-shaped pattern of relationship with BMI categories [20]. Our study also indicated a higher risk of incresed intensity of depression in underweight women compared with women withnormal BMI. However, we did not find a significant correlation between overweight, obesity and the intensity of depression, which could be explained by the fact that our population was generally healthy, and chronic diseases were rare, even in the obesity women.
Estrogen exposure may influence women's risk of depression [21]; therefore, we analyzed the effect of hormone-related events on the risk of incresed intensity of depression. The majority of our participants were perimenopausal women who still underwent menstruation; therefore, we collected data concerning parity, times of abortion, and age at menarche in the whole population. The results only supported the protective effect of more parity on the risk of incresed intensity of depression during the menopause transition, which was consistent with the results from some previous studies [22, 23].
In postmenopausal women in whom menstrual events reflected endogenous hormone exposure, clinical and epidemiologic data supported a protective role for a longer estrogen exposure period in mood disorders [21, 24]. Consistent with these studies we observed a protective effect of longer reproductive period and later age at menopause on the risk of incresed intensity of depression after menopause. Interestingly, in our study, longer duration after menopause was found to have harmful effect after adjusting for demographic variables. Previous studies examining this association in postmenopausal women were scarce, only one American cohort study recruiting 203 women evaluated the depressive symptoms around natural menopause and indicated a decrease of approximately 15% of baseline per year of the CES-D score [25]. As in our study, the negative association of duration after menopause and the intensity of depression might be an indirect indication of the early use of HRT after menopause to prevent depression, which was proven by a recent clinical trial [26]. However, because of the limited evidence, further studies should be conducted to discuss the development of depression after menopause.
Numerous studies on animals and cells demonstrated a beneficial effect of estrogen on mood. Epidemiological studies found heterogeneous results, lower serum levels of E2 [28, 29] and higher levels of FSH [5, 27] have been associated with depressive symptoms in perimenopausal and postmenopausal women. However, other studies found no relation between estrogen or FSH levels and mood or depression [29, 30]. Meanwhile, some investigators identified that fluctuations in estrogen levels over time were more closely linked to depression than absolute hormone levels [31, 32]. Our results suggested women with higher level of serum E2 and lower serum FSH had less intensity of depression. Together with our findings of the associations between depression and hormone-related events, our results supported the view that more estrogen exposure decreased the risk of incresed intensity of depression in midlife women in China.
This study has several strengths. First, our study is one of the few studies to show factors related to the intensity of depression during the menopausal transition in southeast China. Second, this is the first study to comprehensively measure the demographic, symptomatic, and hormonal risk factors of the the intensity of depression, as well as historical events in Chinese population. Third, some important new findings were revealed, including the association between the mKMI score, duration after menopause, and the risk of incresed intensity of depression. Further, our study showed a relatively high prevalence of depression in women who had complaints about menopause; therefore, gynecologists as the first health care providers for these women not only in China,but also in the whole world should not only focus on the treatment of menopausal symptoms, but also concerned about the mental state of the patients. Thus screening for depression during consultations in mid-life women with menopausal symptoms should be considered for the early detection and prevention of severe depressive disorders.
While, there are several limitations of the present study. First, our findings were based on a cross-sectional study; therefore, we could only report the potential risk factors of depression and causal inferences could not be made. The time interval of the study was relatively long, thus, we did the subgroup analysis dividing the time interval into four durations, the result showed our results were stable. Second, some the data were collected by self-reporting. This could lead to inaccurate information such as childbearing history and menstrual history, which occurred many decades before. However, a high degree of accuracy has been reported for women recalling their reproductive events [33]. Third, our population was hospital based, most of the patients came to us because of menopausal symptoms, our population could not represent all the women experiencing menopausal transition, which might cause selection bias. Further population-based studies and meta-analyses are expected to minimize bias and systematic error.
Conclusions
The present study showed elder age, underweight, postmenopause, lower serum level of E2, and higher serum level of FSH were positively associated with the intensity of depression, and increased mKMI score was strongly related with the intensity of depression. Increased number of parities was negatively associated with the intensity of depression in Chinese women during menopausal transition.
Sometimes, depression during menopause transition may be hard to be identified, The results of the present study might be helpful to improve the understandings of the associated factors with depression during menopause transition and to improve clinical management and public health programs to prevent and detect depression in the very early phase in high-risk mid-life women.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- mKMI:
-
Kupperman Menopausal Index
- HAMD-24:
-
24-Item Hamilton Rating Scale for Depression
- WHO:
-
World Health Organization
- SWAN MHS:
-
Study of Women's Health across the Nation Mental Health Study
- E2:
-
Estradiol
- P:
-
Progesterone
- TE:
-
Testosterone
- LH:
-
Luteinizing hormone
- FSH:
-
Follicle stimulating hormone
- STRAW:
-
2012 Stages of Reproductive Aging Workshop
- ANOVA:
-
One-way analysis of variance
- OR:
-
Odds ratio
- CI:
-
Confidence interval
References
Zeng LN, Yang Y, Feng Y, et al. The prevalence of depression in menopausal women in China: a meta-analysis of observational studies. J Affect Disord. 2019;256:337–43.
Soares CN, Zitek B. Reproductive hormone sensitivity and risk for depression across the female life cycle: a continuum of vulnerability. J Psychiatry Neurosci. 2008;33:331–43.
Colvin A, Richardson GA, Cyranowski JM, Youk A, Bromberger JT. The role of family history of depression and the menopausal transition in the development of major depression in midlife women: study of women’s health across the nation mental health study (SWAN MHS). Depress Anxiety. 2017;34:826–35.
Maartens LW, Knottnerus JA, Pop VJ. Menopausal transition and increased depressive symptomatology: a community based prospective study. Maturitas. 2002;42:195–200.
Freeman EW, Sammel MD, Lin H, Nelson DB. Associations of hormones and menopausal status with depressed mood in women with no history of depression. Arch Gen Psychiatry. 2006;63:375–82.
Maki PM, Kornstein SG, Joffe H, et al. Guidelines for the evaluation and treatment of perimenopausal depression: summary and recommendations. Menopause. 2018;25:1069–85.
Jung SJ, Shin A, Kang D. Menarche age, menopause age and other reproductive factors in association with post-menopausal onset depression: results from Health Examinees Study (HEXA). J Affect Disord. 2015;187:127–35.
Li F, He F, Sun Q, et al. Reproductive history and risk of depressive symptoms in postmenopausal women: A cross-sectional study in eastern China. J Affect Disord. 2019;246:174–81.
Harlow SD, Gass M, Hall JE, et al. Executive summary of the stages of reproductive aging workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012;19:387–95.
Tao M, Shao H, Li C, Teng Y. Correlation between the modified Kupperman Index and the menopause rating scale in Chinese women. Patient Prefer Adherence. 2013;7:223–9.
Li RX, Ma M, Xiao XR, Xu Y, Chen XY, Li B. Perimenopausal syndrome and mood disorders in perimenopause: prevalence, severity, relationships, and risk factors. Medicine (Baltimore). 2016;95:e4466.
Zang H, He L, Chen Y, Ge J, Yao Y. The association of depression status with menopause symptoms among rural midlife women in China. Afr Health Sci. 2016;16:97–104.
Azizi M, Fooladi E, Bell RJ, et al. Depressive symptoms and associated factors among Iranian women at midlife: a community-based, cross-sectional study. Menopause. 2019;26:1125–32.
Bromberger JT, Matthews KA, Schott LL, et al. Depressive symptoms during the menopausal transition: the Study of Women’s Health Across the Nation (SWAN). J Affect Disord. 2007;103:267–72.
Tomida M, Otsuka R, Tange C, et al. Vasomotor symptoms, sleep problems, and depressive symptoms in community-dwelling Japanese women. J Obstet Gynaecol Res. 2021;47(10):3677–90.
Shea AK, Sohel N, Gilsing A, et al. Depression, hormone therapy, and the menopausal transition among women aged 45 to 64 years using Canadian Longitudinal Study on aging baseline data. Menopause. 2020;27(7):763–70.
de Kruif M, Spijker AT, Molendijk ML. Depression during the perimenopause: a meta-analysis. J Affect Disord. 2016;206:174–80.
Woods NF, Smith-DiJulio K, Percival DB, Tao EY, Mariella A, Mitchell S. Depressed mood during the menopausal transition and early postmenopause: observations from the Seattle Midlife Women’s Health Study. Menopause. 2008;15:223–32.
Morrison MF, Freeman EW, Lin H, Sammel MD. Higher DHEA-S (dehydroepiandrosterone sulfate) levels are associated with depressive symptoms during the menopausal transition: results from the PENN Ovarian Aging Study. Arch Womens Ment Health. 2011;14:375–82.
Lee JH, Park SK, Ryoo JH, et al. U-shaped relationship between depression and body mass index in the Korean adults. Eur Psychiatry. 2017;45:72–80.
Georgakis MK, Thomopoulos TP, et al. Association of age at menopause and duration of reproductive period with depression after menopause: a systematic review and meta-analysis. JAMA Psychiat. 2016;73:139–49.
Unsal A, Tozun M, Ayranci U. Prevalence of depression among postmenopausal women and related characteristics. Climacteric. 2011;14:244–51.
Perquier F, Ryan J, Ancelin ML, Mesrine S, Clavel-Chapelon F. Lifetime endogenous reproductive factors and severe depressive symptoms in postmenopausal women: findings from the E3N cohort. Menopause. 2013;20:1154–63.
Marsh WK, Bromberger JT, Crawford SL, et al. Lifelong estradiol exposure and risk of depressive symptoms during the transition to menopause and postmenopause. Menopause. 2017;24:1351–9.
Freeman EW, Sammel MD, Boorman DW, Zhang R. Longitudinal pattern of depressive symptoms around natural menopause. JAMA Psychiat. 2014;71:36–43.
Gordon JL, Rubinow DR, Eisenlohr-Moul TA, Xia K, Schmidt PJ, Girdler SS. Efficacy of transdermal estradiol and micronized progesterone in the prevention of depressive symptoms in the menopause transition: a randomized clinical trial. JAMA Psychiat. 2018;75:149–57.
Harlow BL, Wise LA, Otto MW, Soares CN, Cohen LS. Depression and its influence on reproductive endocrine and menstrual cycle markers associated with perimenopause: the Harvard Study of Moods and Cycles. Arch Gen Psychiatry. 2003;60:29–36.
Almeida OP, Lautenschlager N, Vasikaram S, Leedman P, Flicker L. Association between physiological serum concentration of estrogen and the mental health of community-dwelling postmenopausal women age 70 years and over. Am J Geriatr Psychiatry. 2005;13:142–9.
Bromberger JT, Schott LL, Kravitz HM, et al. Longitudinal change in reproductive hormones and depressive symptoms across the menopausal transition: results from the Study of Women’s Health Across the Nation (SWAN). Arch Gen Psychiatry. 2010;67:598–607.
Henderson VW, St John JA, Hodis HN, et al. Cognition, mood, and physiological concentrations of sex hormones in the early and late postmenopause. Proc Natl Acad Sci USA. 2013;110:20290–5.
Ryan J, Burger HG, Szoeke C, et al. A prospective study of the association between endogenous hormones and depressive symptoms in postmenopausal women. Menopause. 2009;16:509–17.
Gordon JL, Rubinow DR, Eisenlohr-Moul TA, Leserman J, Girdler SS. Estradiol variability, stressful life events, and the emergence of depressive symptomatology during the menopausal transition. Menopause. 2016;23:257–66.
Bean JA, Leeper JD, Wallace RB, Sherman BM, Jagger H. Variations in the reporting of menstrual histories. Am J Epidemiol. 1979;109:181–5.
Acknowledgements
We would like to show our great appreciation to Dr Mengling Tang from Department of Epidemiology and Biostatistics, Zhejiang University School of Medicine for her help within the statistics, Chief officer Wenjun Zhu from the Medical-record Department and Shumin Xu from the Zhejiang University Health Care Fund for women for their help with the data management.
Funding
This work was supported by the National Natural Science Foundation [Grant Number: 82003469]; Science and Technology Planning Project of Zhejiang Province, China [Grant Number: 2019C03026]; Zhejiang Provincial Natural Science Foundation of China [Grant Number: LY18H040003]; and Zhejiang Provincial Natural Science Foundation of China [Grant Number: LGF20H040009].
Author information
Authors and Affiliations
Contributions
JZ and FR designed the project and contributed to the paper writing. KC and JS performed data analysis and write the paper. LM, YH and FW conducted the scale and the interviews. XM and JL collected the data. FW contributed to data processing. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Ethics Committee of Women’s Hospital, Zhejiang University School of Medicine. All participating women provided written informed consent for this study. All methods were performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Table of multivariable logistic regression analyses for factors not meaningful.
Additional file 2
. Table of multivariable logistic regression analyses for menopausal symptoms with depression according to the HAMD.
Additional file 3
. Subgroup analysis of factors associated with depression according to the HAMD in each time intervals.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chu, K., Shui, J., Ma, L. et al. Biopsychosocial risk factors of depression during menopause transition in southeast China. BMC Women's Health 22, 273 (2022). https://doi.org/10.1186/s12905-022-01710-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-022-01710-4