
Abstract
Background
Nurses are one of the most critical members of advance care planning (ACP) discussion. The evaluation of ACP self-efficacy is of great significance for developing targeted ACP interventions among clinical nurses and update their professional roles. However, there are few instruments to evaluate their ACP self-efficacy in mainland China. The purpose of this study was to translate the ACP self-efficacy scale into Chinese and evaluate its psychometric properties among clinical nurses.
Methods
A methodological study of the translation and validation of the ACP self-efficacy scale was conducted from January to March 2022. It involved three phases: (1) the translation and revision of the scale; (2) the exploration and evaluation of the item (n = 436); (3) the psychometric evaluation of the scale (n = 674).
Results
After a rigorous translation and revision, the ACP self-efficacy scale with three dimensions and 16 items was finally formed. In this study, the critical ratios of the item ranged from 8.226 to 17.499, and the item-total correlation coefficients ranged from 0.437 to 0.732, and the factor loadings of the item ranged from 0.638 to 0.882. The content validity index of the scale was 0.946. Supported by the eigenvalues, the three-factor structure explained the cumulative 61.131% of the overall variance. As the results of confirmatory factor analysis, all the recommended fitting indexes were appropriate. The average variance extracted values ranged from 0.570 to 0.756, and the composite reliability values ranged from 0.858 to 0.925. The total Cronbach's α coefficient, split-half reliability coefficient and test–retest reliability coefficient of the scale were 0.896, 0.767 and 0.939, respectively.
Conclusion
The Chinese version of ACP self-efficacy scale was successfully introduced into China, showing good psychometric properties among clinical nurses, and can effectively assess the ACP self-efficacy. Also, the scale can provide nursing educators with a significant strategy to develop ACP educational procedure and post-intervention measures for clinical nurses to improve nurse-led ACP practice.
Similar content being viewed by others


Introduction
Advance care planning (ACP) refers to a process in which individuals can communicate with their surrogate decision-makers and healthcare providers to express future medical care preferences according to their own experiences or values when they are conscious and have the ability to make decisions [1, 2]. ACP circumvented the limitations of advance directives (ADs) as a written document and more flexibly emphasized the process of multi-party communication rather than signing the specific legal document [3]. ACP aims to assist individuals to express their future medical care preferences to reduce decision-making conflicts between individuals and surrogate decision-makers, and it ensure patients' right to know and independent decision-making about future medical care [4, 5]. More significantly, ACP also provides health care professionals with an effective reference for their clinical ethical decision-making [6].
Clinical nurses are one of the most critical members of ACP discussion, serving as full collaborators, participating in the ACP preparation and implementation [7]. Lam et al. [8] reported that 95% of participants did not agree that ACP was solely the responsibility of doctors, and proposed that the initiator of ACP should be nurses. In recent years, there have been more and more studies proving the effectiveness and acceptability of nurse-led ACP practice [9,10,11]. In addition, nurses are also information providers and educators in ACP communication, and can provide positive ACP guidance and effective ACP interventions for patients and surrogate decision-makers [12]. Hilgeman et al. [13] proposed the patient-centered ACP education intervention program supported by video, the core of which was to provide patients with information about the options, risks and benefits of medical care procedures to help patients make more informed choices and complete ACP discussions. Therefore, nurse-led ACP practice is appropriate and significant.
ACP self-efficacy was the key predictor for patients and clinical nurses to participate in and benefit from ACP discussions [14,15,16]. Self-efficacy refers to the degree to which individuals are confident that they can use the skills they possess to perform certain behaviors [17]. Clinical nurses with a low ACP self-efficacy may be reluctant to lead or participate in ACP discussions with patients and surrogate decision-makers, or to expend effort in developing ACP skills and addressing barriers to ACP discussions [18]. Therefore, it may be a key component for overcoming the barriers to ACP discussion to improve ACP self-efficacy among clinical nurses. Given the importance of this issue and the urgency of ACP best practices, Baughman et al. [19] developed and validated a scale to assess ACP self-efficacy (ACP-SE) among healthcare providers. The ACP-SE scale had a single dimension with 17 items that explained 58.38% of the total variation and satisfactory reliability and validity [19]. Subsequently, the ACP-SE scale was translated into Spanish and validated its psychometric properties in primary care providers and social workers [20]. To our knowledge, the Chinese version of the ACP-SE scale has not yet been developed. Based on the importance of nurse-led ACP practice, a validated Chinese version of the ACP-SE scale is required to evaluate ACP self-efficacy levels and the effectiveness of ACP-related educational intervention programs among clinical nurses.
The aim of our study was to translate the ACP-SE scale into Chinese and evaluate its psychometric properties among clinical nurses. We expect that the Chinese version of the ACP-SE scale has satisfactory reliability and validity, and the scale can offer an effective strategy for nursing educators to develop educational interventions to improve the ACP self-efficacy of clinical nurses.
Methods
Participants
We recruited eligible clinical nurses by convenience sampling in Shenyang and Jinzhou, China, from January to March 2022. Inclusion criteria were registered nurses who have at least one year clinical work experience and gave informed consent. Exclusion criteria were clinical nurses from non-clinical departments and non-Chinese nationalities. The sample size was determined by the general guideline of factor analysis, that is, at least 10 participants responded to each item, and the 20% sample loss rate should also be considered [21]. In our study, the translated scale consists of 16 items, and at least 200 participants were needed, but a large sample is desirable [22]. According to the existing conditions, a total of 436 clinical nurses (for item analysis) and 674 clinical nurses (for psychometric evaluation) were finally recruited.
Design
A methodological study with three phases: (1) the translation and revision of the scale; (2) the exploration and evaluation of the item (n = 436); (3) the psychometric evaluation of the scale (n = 674). In addition, the samples involved in the third phase were randomly divided into two groups, one for exploratory factor analysis (EFA, n = 337) and the other for confirmatory factor analysis (CFA, n = 337). The flowchart is shown in Fig. 1.

The development procedure of the Chinese version of ACP-SE scale
The translation and revision of the scale
The Brislin double back-translation method was adopted to translate the ACP-SE scale [23]. First, two Chinese professors (one had experience of studying abroad, the other majored in English) translated the ACP-SE scale into Chinese, respectively. After they discussed with each other, the forward translation version was formed. Then, two foreign teachers translated the forward version into English, respectively. After they discussed with each other, the reverse translation version was formed. Finally, the reverse translation version and the original scale were compared and discussed by the above four translators and the research team to ensure the consistency of semantics and context to the greatest extent. The draft of the Chinese version of the ACP-SE scale was finally formed.
A total of seven experts were invited to revise the draft of the Chinese version of the ACP-SE scale by the Delphi expert consultation method [24]. Inclusion criteria of experts were as follows: (1) at least six years of hospice care study; (2) at least master degree; (3) at least intermediate title; (4) voluntary participants in the study. In this study, the seven expert members included three males and four females with the following credentials: working years (10.43 ± 2.99); four masters, three doctors; all held senior titles. After the cross-cultural adaptation, the draft of the Chinese version of the ACP-SE scale was used for a preliminary investigation among 30 clinical nurses to understand their opinions about the items [25]. Finally, the pre-test Chinese version of the ACP-SE scale was developed.
The exploration and evaluation of the item
We used the critical ratio method, correlation coefficient method and internal consistency for item analysis to evaluate the suitability for each item. The critical ratio was calculated by t-test for two independent samples (the first 27%, high-score group vs the last 27%, poor-score group) to determine the discrimination of the item. It is generally considered that when the critical ratio of each item ≥ 3 (P < 0.05), the item has satisfactory discrimination [26]. The item-total correlation coefficient was calculated to determine the homogeneity of the item, and the item-total correlation coefficient ≥ 0.4 indicates that the item has the appropriate homogeneity [26]. The Cronbach's α coefficient after deleting each item was calculated to determine the quality of the item. We require that the Cronbach's α coefficient of the scale would not increase if the item was deleted [26]. In addition, the preliminary EFA was completed to explore the factor loadings to assess the stability, and the recommended factor loading for each item should be above 0.40 and there was no cross loading. If the above requirements were not met, the corresponding item will be deleted [27].
The psychometric evaluation of the scale
We invited eligible seven experts to appraise the content validity of the Chinese version of the ACP-SE scale. The Likert four-point scoring system, from one point (irrelevant) to four point (very relevant), was adopted to gather responses from experts. The content validity index of the item (I-CVI) is the ratio of the number of experts giving three or four points to the total number of experts participating in this evaluation. The content validity index of the scale (S-CVI) is the average of I-CVI of all items in the scale. We require the I-CVI ≥ 0.78 and the S-CVI ≥ 0.90 [28].
EFA with principal axis factoring was completed to explore the underlying factor structure of the scale. The Bartlett’s test of sphericity was significant (P < 0.05) and the Kaiser–Meyer–Olkin (KMO) coefficient was > 0.60, indicating the suitability for EFA [29]. The requirements are as follows:(1) the factor loading of the item ≥ 0.4 and there was no cross loading, (2) each extracted common factor contains no less than three items, and (3) the cumulative explanatory variation of all common factors ≥ 40% [30, 31].
The CFA was completed to explore whether the factor model met theoretical expectations. The criteria for fitting indexes are as follows: (1) the chi-square degree of freedom (2/df) ≤ 3; (2) the root mean square error of approximation (RMSEA) ≤ 0.05; (3) the goodness-of-fit index (GFI), the adjusted goodness-of-fit index (AGFI), the tucker lewis index (TLI), the comparative fit index (CFI), and the incremental fit index (IFI) ≥ 0.9; (4) the parsimonious goodness-of-fit index (PGFI) and the parsimonious normed-of-fit index (PNFI) ≥ 0.5 [32, 33].
Also, convergent validity and discriminant validity were conducted to assess the construct validity of the scale. The average variance extracted (AVE) value and the composite reliability (CR) value were used for the convergent validity. The AVE value ≥ 0.50 and the CR value ≥ 0.70, which indicate that the scale has appropriate convergent validity [34]. The square root of the AVE value and the correlation coefficient of the factors were calculated to evaluate the discriminant validity. We require that the square root of AVE value should exceed the correlation coefficient between the corresponding factors [34].
The ACP-related attitude is closely related to ACP-SE among clinical nurses [16]. Therefore, the ACP practice preference scale for clinical nurses was adopted as a criterion instrument to appraise the criterion validity of the Chinese version of ACP-SE scale. The correlation coefficient between them was calculated as a reliable index, and the correlation coefficient ≥ 0.7, demonstrating that the Chinese version of the ACP-SE scale has optimal criterion validity [35].
The internal consistency and the test–retest reliability were performed to appraise the reliability of the Chinese version of the ACP-SE scale. In the internal consistency analysis, the Cronbach'sα coefficient and the split-half reliability coefficient were calculated to evaluate the homogeneity of the item. After two weeks, the scale was adopted to remeasure the previously labeled 80 clinical nurses, and the correlation coefficient was calculated to assess the stability of the scale across time. We require that the Cronbach’α coefficient, the split-half reliability coefficient and test–retest reliability coefficient should all be 0.7 or above [36, 37].
Instruments
The general demographic characteristics questionnaire
We developed the general demographic characteristics questionnaire after systematic literature analysis and rigorous team negotiation. The questionnaire included seven variables: age, gender, marital status, education level, working years, department, received relevant training.
The advance care planning (ACP) practice preference scale
ACP practice preference scale was previously developed by our team to evaluate ACP practice preference among clinical nurses. The scale consists of three dimensions with 24 items. The Likert five-point scoring system (very disagree to very agree) was adopted to gather responses from clinical nurses. The score ranges from 24 to 120. The higher the score is, the stronger the ACP participation preference of clinical nurses is. In our previous work, this scale was confirmed to have appropriate psychometric properties.
Data collection
After explaining the purpose and significance of the study, the researchers recruited clinical nurses with the assistance of nursing leaders in two cities, China. In phase one, seven eligible experts received the compressed package consisting of informed consent and expert consultation questionnaire via email, and were told to return within two weeks. The recovery rate of the questionnaire was satisfactory. In phase two, we invited 460 clinical nurses to participate in the survey, and 447 clinical nurses agreed to the invitation and signed the informed consent. 436 questionnaires were retained after the questionnaires with missing data were removed. In phase three, we recruited 700 clinical nurses to participate in the survey, and 682 clinical nurses agreed to participate in the study. After deleting the questionnaires with missing data, 674 questionnaires were finally retained. It takes six to eight minutes to complete the questionnaire.
Data analysis
SPSS 26.0 and AMOS 18.0 were used to complete statistical analysis. Frequency and composition ratios were adopted to describe the general demographic characteristics of clinical nurses. Item analysis was completed to evaluate the quality of the items, and the Delphi survey was adopted to assess the content validity of the scale. EFA with principal axis factoring was completed to explore the underlying factor structure of the scale. Also, the structural equation model (SEM) with maximum likelihood was completed to validate the consistency between the underlying factor structure and the theoretical expectation. The internal consistency analysis and test–retest reliability analysis were conducted to assess the homogeneity and stability of the scale.
All participants signed informed consent and filled in the questionnaire anonymously after being informed of the purpose, significance, voluntary and anonymous nature of the study. All methods and contents of this study were performed in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the First Affiliated Hospital of China Medical University (AF-SOP-07–1. 1–01).
Results
The general demographic characteristics
In phase two, we finally recruited 436 clinical nurses for the item analysis, and the sample consists of 126 males and 310 females with an average age of (29.22 ± 6.87). In phase three, a total of 337 valid questionnaires composed of 129 males and 208 females with an average age of (29.73 ± 8.07) contributed to the EFA. A total of 337 valid questionnaires, including 135 males and 202 females with an average age of (29.45 ± 7.50) contributed to CFA. More details are showed in Table 1.
The translation and revision of the scale
After the rigorous translation, we invited seven hospice care experts to revise the draft of the Chinese version of the ACP-SE scale with 17 items. As a result of Delphi survey, the recovery rate of experts consultation questionnaire, the authority coefficient of experts and the Kendall’s concordance coefficient were 1.000, 0.893 and 0.617 respectively. Due to similar statements, we merged "Ensure that patient’s treatment preferences will be honored at your facility" and "Ensure that patient’s treatment preferences will be honored at a hospital if patient is hospitalized" into "Ensure that patient’s care preferences will be honored at your work". In addition, four items were revised due to the stronger pertinence for doctors rather than nurses. For example, "treatment goals and plans" was revised to "care goals and plans", and "life-sustaining treatments" was revised to "life-sustaining care schemes". After a preliminary survey using the revised draft of the Chinese version of the ACP-SE scale, all 30 clinical nurses reported that each item of the scale was easy to understand and answer. The Chinese pretest version of ACP-SE scale with 16 items was finally developed.
The exploration and analysis of the item
The quality of the item was estimated by the item analysis with the critical ratio, the item-scale correlation coefficient and the Cronbach's α coefficient. In this study, critical ratios of the items ranged from 8.226 to 17.499 (P < 0.001), and item-total correlation coefficients ranged from 0.437 to 0.732 (P < 0.001). The Cronbach's α coefficient did not increase after each item was deleted. A preliminary EFA was completed to explore the factor loading of each item to assess the stability of the item. As a result of the preliminary EFA, the recommended factor loadings ranged from 0.638 to 0.882 and there was no cross loading. The detailed information is shown in Table 2.
The psychometric evaluation of the scale
Content validity
Seven qualified hospice care experts were invited to assess the I-CVI and S-CVI. As a result of Delphi expert consultation, the expert response rate was 100%, and I-CVI ranged from 0.857 to 1.000, and S-CVI was 0.946.
Construct validity
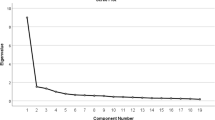
In EFA, the KMO value was 0.883, and the Bartlett sphericity test was significant (2 = 4571.576, P < 0.001). The three-factor model explained 61.131% of the total variation with eigenvalues > 1 (Table 3). Based on the meaning expressed by the item, the three factors were named preference discussion and evaluation, information guidance and disclosure, and content evaluation and determination, respectively. In CFA, the SEM with the maximum likelihood method was adopted to fit the three-factor model (Fig. 2). As the results of CFA, 2/df = 2.046, GFI = 0.929, AGFI = 0.904, RMSEA = 0.046, TLI = 0.969, CFI = 0.974, IFI = 0.974, PGFI = 0.690, PNFI = 0.800. The selected fitting indexes showed that the three-factor model has appropriate fitting. However, unlike the results of EFA, the results of CFA showed that factors 14 and 16 were weak and should be removed from the scale, and the Chinese version of ACP-SE scale with 3 dimensions and 14 items was finally developed. In convergent validity analysis, the AVE values ranged from 0.570 to 0.756, and CR values ranged from 0.858 to 0.925. In discriminant validity analysis, the square root values of AVE ranged from 0.755 to 0.869, which were all greater than the correlation coefficient between the corresponding factors (Table 4).

Standardized three-factor model of the Chinese version of ACP-SE scale
Criterion validity
The ACP practice preference scale was adopted as the criterion instrument to measure the criterion validity of the Chinese version of the ACP-SE scale. As a result of the correlation analysis, the ACP-SE was highly positively correlated with the ACP practice preference, and the correlation coefficient was 0.889 (P < 0.001).
Internal consistency and test–retest reliability
The homogeneity and stability of the Chinese version of the ACP-SE scale were evaluated by the internal consistency and the test–retest reliability. As a result of reliability analysis, the total Cronbach's α coefficient of the scale was 0.896 with three dimensions of 0.885, 0.849 and 0.927, respectively. The total split-half reliability coefficient of the scale was 0.767 with three dimensions of 0.912, 0.827 and 0.917, respectively. The total test–retest reliability coefficient of the scale was 0.939 with three dimensions of 0.924, 0.835, 0.849, respectively.
Discussion
There are lacks of instruments to assess ACP-SE among clinical nurses in China. This study translated the ACP-SE scale into Chinese for the first time [23], and validated its psychometric properties among clinical nurses by factor analysis [30]. The Chinese version of the ACP-SE scale with appropriate reliability and validity could be considered as an effective instrument for assessing ACP-SE among clinical nurses. Moreover, it can also provide nursing educators with a significant strategy to develop ACP education interventions for clinical nurses and to assess ACP-SE after intervention based on the items and dimensions to improve their ACP participation and the competence of hospice care.
The practicality of the scale
The original version of the ACP-SE scale consists of a single dimension with seventeen items [19]. In this study, after rigorous translation and cross-cultural adaptation [24], the Chinese version of the ACP-SE scale with the three-factor structure was developed. Based on the connotation reflected by the item, the common factors were assigned to different aspects of the nurse-led ACP practice, which were named as preference discussion and evaluation, information guidance and disclosure, and content evaluation and determination respectively. Compared with the original version [19], the Chinese version of the ACP-SE scale with a three-factor structure further detailed and clarified the different aspects of ACP-SE in clinical nurses, which can measure the shortcomings of clinical nurses in a certain aspect of ACP practice, and also pointed out the direction of the targeted intervention. Therefore, the Chinese version of the ACP-SE scale had a certain practicality, that was, it could comprehensively assess the ACP-SE level of clinical nurses.
The scientificity of the scale
Based on strict evaluation and revision of the items, the Chinese version of the ACP-SE scale with three dimensions and sixteen items was developed. In item analysis, the critical ratios of the items met the reference standard [26], and there was a moderate to high correlation between item-total scores. In addition, when the item was deleted, the Cronbach's α coefficient on the scale did not increase. Therefore, the above information proved that the items have optimal applicability [26, 27].
In content validity, I-CVI and S-CVI were superior to the standard value, supporting the suitable content validity of the scale [28]. The total variation is well explained by the three-factor structure extracted from EFA. Also, the expected theoretical model was further confirmed by CFA, and the model fitting indexes were satisfactory [32, 33]. Moreover, the AVE and CR values were appropriate, and the square root of AVE values was greater than the correlation coefficient between the corresponding factors, which showed that the scale has good convergent validity and discrimination validity [34]. The above information strongly proves that the construct validity of the scale is appropriate. In calibration validity, the high correlation between the ACP-SE and the ACP participation preference also demonstrated that the scale has suitable calibration validity.
In reliability analysis, the Cronbach's α coefficient and the split-half reliability coefficient of the scale were both above the reference value [36] but slightly lower than the original version and the Spanish version [19, 20], which indicated the scale has an optimal internal consistency. Moreover, the previously labeled nurses were remeasured two weeks later, and the test–retest reliability coefficient reached an acceptable range [36], indicating that the scale has measurement stability across time [38].
Limitations
We consider some limitations that need to be paid attention to and discussed in our study. First, a large multi-center sample is worth considering to improve the sample representativeness and explore the cultural differences represented by different regions, although the sample size of the study met the statistical requirements. Second, bias from the nature of convenience sampling is inevitable.Based on this, the rigorous data collection procedure were considered to reduce selection bias, and the 20% sample loss rate was also considered in our study. Finally, as the focus of our future work, the Chinese version of the ACP-SE scale was used to evaluate its predictive effectiveness.
Conclusion
The Chinese version of ACP-SE scale was successfully introduced into China. It showed good psychometric properties among clinical nurses and can effectively assess the ACP-SE. It can also provide a significant strategy for nursing educators to develop ACP education interventions and post-intervention measures among clinical nurses to improve their ACP participation.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACP:
-
Advance Care Planning
- ADs:
-
Advance Directives
- ACP-SE:
-
ACP Self-Efficacy
- SEM:
-
Structural Equation Model
- I-CVI:
-
Content Validity Index of the Item
- S-CVI:
-
Content Validity Index of the Scale
- KMO:
-
Kaiser–Meyer–Olkin; EFA: Exploratory Factor Analysis
- CFA:
-
Confirmatory Factor Analysis
- χ2/df:
-
Chi-Square Degree of Freedom
- RMSEA:
-
Root Mean Square Error of Approximation
- GFI:
-
Goodness-of-Fit Index
- AGFI:
-
Adjusted Goodness-of-Fit Index
- TLI:
-
Tucker Lewis Index
- CFI:
-
Comparative Fit Index
- IFI:
-
Incremental Fit Index
- PGFI:
-
Parsimonious Goodness-of-Fit Index
- PNFI:
-
Parsimonious Normed-of-Fit Index
- AVE:
-
Average Variance Extracted
- CR:
-
Composite Reliability
References
Rietjens J, Korfage I, Taubert M. Advance care planning: the future. BMJ Support Palliat Care. 2021;11(1):89–91. https://doi.org/10.1136/bmjspcare-2020-002304.
Yang Z, Chen P, Hou B, Zhang H. Advance care planning among elderly acquired immunodeficiency syndrome patients: a qualitative preference study. J Hosp Palliat Nurs. 2022;24(2):E10–7. https://doi.org/10.1097/NJH.0000000000000824.
Piers R, Albers G, Gilissen J, et al. Advance care planning in dementia: recommendations for healthcare professionals. BMC Palliat Care. 2018;17(1):88. https://doi.org/10.1186/s12904-018-0332-2.
Fleuren N, Depla MFIA, Janssen DJA, Huisman M, Hertogh CMPM. Underlying goals of advance care planning (ACP): a qualitative analysis of the literature. BMC Palliat Care. 2020;19(1):27. https://doi.org/10.1186/s12904-020-0535-1.
Cheng SY, Lin CP, Chan HY, et al. Advance care planning in Asian culture. Jpn J Clin Oncol. 2020;50(9):976–89. https://doi.org/10.1093/jjco/hyaa131.
Hammes B, Meier DE. Advance Care Planning Requires Training. J Am Geriatr Soc. 2019;67(1):189. https://doi.org/10.1111/jgs.15610.
Fliedner M, Halfens RJG, King CR, Eychmueller S, Lohrmann C, Schols JMGA. Roles and Responsibilities of Nurses in Advance Care Planning in Palliative Care in the Acute Care Setting: A Scoping Review. J Hosp Palliat Nurs. 2021;23(1):59–68. https://doi.org/10.1097/NJH.0000000000000715.
Lam L, Ansari AS, Baquir PJ, Chowdhury N, Tran K, Bailey J. Current practices, barriers and enablers for advance care planning among healthcare workers of aged care facilities in western New South Wales, Australia. Rural Remote Health. 2018;18(4):4714. https://doi.org/10.22605/RRH4714.
Ohr SO, Cleasby P, Jeong SY, Barrett T. Nurse-led normalised advance care planning service in hospital and community health settings: a qualitative study. BMC Palliat Care. 2021;20(1):139. https://doi.org/10.1186/s12904-021-00835-x.
Chan HY, Ng JS, Chan KS, et al. Effects of a nurse-led post-discharge advance care planning programme for community-dwelling patients nearing the end of life and their family members: A randomised controlled trial. Int J Nurs Stud. 2018;87:26–33. https://doi.org/10.1016/j.ijnurstu.2018.07.008.
Gabbard J, Pajewski NM, Callahan KE, et al. Effectiveness of a Nurse-Led Multidisciplinary Intervention vs Usual Care on Advance Care Planning for Vulnerable Older Adults in an Accountable Care Organization: A Randomized Clinical Trial. JAMA Intern Med. 2021;181(3):361–9. https://doi.org/10.1001/jamainternmed.2020.5950.
Christensen KL, Winters CA, Colclough Y, Oley E, Luparell S. Advance Care Planning in Rural Montana: Exploring the Nurse’s Role. J Hosp Palliat Nurs. 2019;21(4):264–71. https://doi.org/10.1097/NJH.0000000000000556.
Hilgeman MM, Uphold CR, Collins AN, et al. Enabling Advance Directive Completion: Feasibility of a New Nurse-Supported Advance Care Planning Intervention. J Gerontol Nurs. 2018;44(7):31–42. https://doi.org/10.3928/00989134-20180614-06.
Duckworth KE, Forti AM, Russell GB, Naik S, Hurd D, McQuellon RP. The process of advance care planning in HCT candidates and proxies: self-efficacy, locus of control, and anxiety levels. Am J Hosp Palliat Care. 2014;31(7):710–6. https://doi.org/10.1177/1049909113499815.
Seiter CR. Benefit, Barrier, and Self-Efficacy Messages in Advance Care Planning Education Materials. Health Commun. 2021;36(11):1397–404. https://doi.org/10.1080/10410236.2020.1754601.
Gilissen J, Pivodic L, Wendrich-van Dael A, et al. Nurses’ self-efficacy, rather than their knowledge, is associated with their engagement in advance care planning in nursing homes: A survey study. Palliat Med. 2020;34(7):917–24. https://doi.org/10.1177/0269216320916158.
Liu L, Zhao YY, Zhang LH, Chan HY. Measuring Self-Efficacy and Readiness for Advance Care Planning in Chinese Older Adults. J Pain Symptom Manage. 2020;60(3):622–9. https://doi.org/10.1016/j.jpainsymman.2020.06.013.
Kuusisto A, Santavirta J, Saranto K, Haavisto E. Healthcare professionals’ perceptions of advance care planning in palliative care unit: a qualitative descriptive study. J Clin Nurs. 2021;30(5–6):633–44. https://doi.org/10.1111/jocn.15578.
Baughman KR, Ludwick R, Fischbein R, et al. Development of a Scale to Assess Physician Advance Care Planning Self-Efficacy. Am J Hosp Palliat Care. 2017;34(5):435–41. https://doi.org/10.1177/1049909115625612.
Lasmarías C, Subirana-Casacuberta M, Mancho N, Aradilla-Herrero A. Spanish Cross-Cultural Adaptation and Psychometric Properties of the Advance Care Planning Self-Efficacy: A Cross-Sectional Study. J Palliat Med. 2021;24(12):1807–15. https://doi.org/10.1089/jpm.2020.0653.
Knapp TR, Sawilowsky SS. Minimizing sample size when using exploratory factor analysis for measurement. J Nurs Meas. 2004;12(2):95–9. https://doi.org/10.1891/jnum.2004.12.2.95.
Yang Z, Chen F, Lu Y, Zhang H. Psychometric evaluation of medication safety competence scale for clinical nurses. BMC Nurs. 2021;20(1):165. https://doi.org/10.1186/s12912-021-00679-z.
Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. https://doi.org/10.1177/135910457000100301.
Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. 2011;17(2):268–74. https://doi.org/10.1111/j.1365-2753.2010.01434.x.
Perneger TV, Courvoisier DS, Hudelson PM, Gayet-Ageron A. Sample size for pre-tests of questionnaires. Qual Life Res. 2015;24(1):147–51. https://doi.org/10.1007/s11136-014-0752-2.
Raykov T, Marcoulides GA. On the Relationship Between Classical Test Theory and Item Response Theory: From One to the Other and Back. Educ Psychol Meas. 2016;76(2):325–38. https://doi.org/10.1177/0013164415576958.
Gorsuch RL. Exploratory factor analysis: its role in item analysis. J Pers Assess. 1997;68(3):532–60. https://doi.org/10.1207/s15327752jpa6803_5.
Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity. Res Social Adm Pharm. 2019;15(2):214–21. https://doi.org/10.1016/j.sapharm.2018.03.066.
Tobias S, Carlson JE. Brief report: Bartlett’s test of sphericity and chance findings in factor analysis. Multivariate Behav Res. 1969;4(3):375–7. https://doi.org/10.1207/s15327906mbr0403_8.
Schreiber JB. Issues and recommendations for exploratory factor analysis and principal component analysis. Res Social Adm Pharm. 2021;17(5):1004–11. https://doi.org/10.1016/j.sapharm.2020.07.027.
Alavi M, Visentin DC, Thapa DK, Hunt GE, Watson R, Cleary M. Exploratory factor analysis and principal component analysis in clinical studies: Which one should you use? J Adv Nurs. 2020. https://doi.org/10.1111/jan.14377.10.1111/jan.14377.
Shi D, DiStefano C, Maydeu-Olivares A, Lee T. Evaluating SEM Model Fit with Small Degrees of Freedom. Multivariate Behav Res. 2021;1–36. https://doi.org/10.1080/00273171.2020.1868965
Hooper D, Coughlan J, Mullen MR. Structural equation modelling: guidelines for determining model fit. Electron J Bus Res Methods. 2008;6(1):141–46. https://doi.org/10.3109/03005364000000039.
Kline R. Principles and practice of structural equation modeling, 3rd ed. London: New York Guilford Press; 2011.
Guo B, Aveyard P, Fielding A, Sutton S. Testing the convergent and discriminant validity of the Decisional Balance Scale of the Transtheoretical Model using the Multi-Trait Multi-Method approach. Psychol Addict Behav. 2008;22(2):288–94. https://doi.org/10.1037/0893-164X.22.2.288.
Marques LBF, Moreira BS, Ocarino JM, Sampaio RF, Bastone AC, Kirkwood RN. Construct and criterion validity of the functional gait assessment-Brazil in community-dwelling older adults. Braz J Phys Ther. 2021;25(2):186–93. https://doi.org/10.1016/j.bjpt.2020.05.008.
Frost MH, Reeve BB, Liepa AM, Stauffer JW, Hays RD; Mayo/FDA Patient-Reported Outcomes Consensus Meeting Group;. What is sufficient evidence for the reliability and validity of patient-reported outcome measures?. Value Health. 2007;10 Suppl 2:S94-S105. https://doi.org/10.1111/j.1524-4733.2007.00272.x
Wang T, Molassiotis A, Chung BPM, Tan JY. Psychometric assessment of the Chinese version of the Problems and Needs in Palliative Care questionnaire-short version in advanced cancer patients. BMC Palliat Care. 2019;18(1):68. https://doi.org/10.1186/s12904-019-0450-5.
Acknowledgements
The authors are grateful to clinical nurses who participated in this study, and also to the nursing directors for their strong support in collecting samples. We also thank the invited experts for taking the time to revise this scale. In addition, we are very grateful to prof. Baughman who provided us with the original scale. At the same time, we would like to thank the editor and reviewers from the bottom of our hearts for their valuable comments and suggestions, which have greatly improved the quality of our manuscript.
Funding
None.
Author information
Authors and Affiliations
Contributions
ZY performed research design, data collection, the analysis and interpretation of results, and manuscript preparation. HW performed data collection and the analysis and interpretation of results. APW contributed to the research idea and designed, analysed, and interpreted the results, advised the whole research process, and helped prepare the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants signed informed consent and filled in the questionnaire anonymously after being informed of the purpose, significance, voluntary and anonymous nature of the study. All methods and contents of this study were performed in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the First Affiliated Hospital of China Medical University (AF-SOP-07–1. 1–01).
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, Z., Wang, H. & Wang, A. Psychometric evaluation of the Chinese version of advance care planning self-efficacy scale among clinical nurses. BMC Palliat Care 21, 175 (2022). https://doi.org/10.1186/s12904-022-01064-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12904-022-01064-6