
Abstract
Background
Ultrasonically-activated irrigation (UAI) is effective in root canal irrigation but may damage canal walls. EDDY is a sonic activation system with flexible working tips that cause no harm to dentinal walls. This review explores the intracanal cleaning efficacy of EDDY compared with UAI in vitro.
Methods
The systematic review was registered in the PROSPERO database (CRD42021235826). A literature search was conducted in six electronic databases. In vitro studies that compared the removal of smear layer, debris, soft tissue or microbes in root canals between EDDY and UAI were included. Data extraction and quality assessment were performed. Meta-analyses were conducted on smear layer removal and debris elimination with the standardized mean difference (SMD). Heterogeneity was measured using the I2 test and the Chi2 test. The random-effect model was used when I2 > 50%, or p < 0.1, otherwise the fixed-effect model was applied. The level of significance was set at p < 0.05.
Results
19 articles were included in this systematic review and 7 articles were included in meta-analyses. Meta-analyses on smear layer removal showed unimportant differences between EDDY and UAI at any canal third (coronal [SMD = 0.08, 95% confidence interval (95%CI): -0.29 to 0.45; p = 0.44, I2 = 0%]; middle [SMD = 0.02, 95% CI: -0.44 to 0.47; p = 0.94, I2 = 0%]; apical [SMD = 0.01, 95%CI: -0.35 to 0.38; p = 0.70, I2 = 0%]). Meta-analyses on debris removal evaluated by scanning electron microscope (coronal [SMD = 0.03, 95% CI: -0.41 to 0.46; p = 0.27, I2 = 23%]; middle [SMD = -0.24, 95% CI: -0.83 to 0.35; p = 0.80, I2 = 0%]; apical [SMD = 0.24, 95%CI: -0.20 to 0.67; p = 0.36, I2 = 2%]) and micro-CT (SMD = 0.36, 95% CI: -0.67 to 1.40; p = 0.03, I2 = 70%) both found insignificant differences. No meta-analysis was undertaken on soft-tissue removal and disinfection due to the various study designs, but the qualitative analyses implied that EDDY achieved similar performance to UAI in both aspects.
Conclusions
Limited evidence indicated that EDDY was comparable to UAI in removing smear layer, debris, soft tissue and microbes ex vivo. Considering UAI may damage canal walls, EDDY might be a substitute for UAI in irrigation activation. But more randomized clinical trials are required to explore the clinical extrapolation of the results in this review.
Similar content being viewed by others


Background
Mechanical preparation in root canal treatment produces lots of smear layer and debris [1]. The presence of smear layer will hinder irrigants and medication from entering tubules for thorough disinfection [2, 3]. Besides, restricted by the conoid shape of files, canal walls of narrow anatomic sites will stay unprepared after instrumentation [4, 5], and the soft tissue and biofilms in these areas cannot be mechanically removed. Remaining debris and soft tissue shelters microbes [6, 7], which may leave long-term potential risks if not eradicated [8]. Therefore, root canal irrigation is indispensable for a thorough and effective root canal treatment as it can clean and disinfect the unprepared areas [9].
Needles and syringes with various vent designs are the traditional instruments to conduct irrigation. However, the intracanal cleaning efficacy of needle irrigation is unsatisfactory [10,11,12,13]. Agitation of irrigants is thus required to improve the irrigation effects. Ultrasonically-activated irrigation (UAI) is the most used endodontic activation device in both America [14] and the UK [15]. With a vibration frequency of 25,000 Hz to 40,000 Hz, UAI activates irrigation solution by generating a cavitation effect [16, 17] and acoustic microstreaming [17]. The ultrasonic oscillation also gives rise to circumferential shear stress acting on canal walls [18] and may assist in removing organic remnants and byproducts produced by instrumentation. However, ultrasonic activation may damage dentinal walls and develop microcracks [19,20,21] probably due to its alloy working tips [22] and high-frequency oscillation. Therefore, an airscaler-powered activation system (EDDY; VDW GbmH, Munich, Germany) driven at a frequency of 5000 to 6000 Hz has been introduced and studied. It uses polyamide tips with only one available size (20/02) that are much more flexible than stiff metal tips. According to the manufacturer, EDDY (ED) tips move in a three-dimensional way at a high amplitude. Many studies have been carried out to compare the cleaning effects between UAI and ED [23,24,25]. However, their results are contradictory even though the vibration frequencies of the two activation systems contrast sharply.
Therefore, in view of the above factors, a systematic review is in need to appraise the relevant studies to further explore the cleaning efficacy of ED in comparison to UAI. The focused question of this review is established on the PICO framework: Does UAI (I) achieve better performance on canal cleanliness including the elimination of smear layer, debris, soft tissue and bacterial (O) compared to ED (C) in vitro (P)?
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (2020) checklist and was registered in the PROSPERO database (CRD42021235826).
Eligibility criteria
We included articles that studied UAI in comparison to ED on at least one of the following aspects: the disinfection effectiveness or the ability to remove the intracanal smear layer, debris or soft tissue. Experiments should be performed either with canal models or extracted mature permanent teeth without root canal treatment and fractures. Studies conducted on open canal systems were excluded.
Search strategy
A systematic literature search was conducted on 7 February 2023 using the following electronic database: Pubmed, Embase, Web of Science, Cochrane Library, Scopus and SinoMed (http://www.sinomed.ac.cn/). The publication date was restricted to 2015 and beyond, as EDDY was first introduced in 2015 [26]. No filter on the language was set in the search process. Eight keywords (“root canal”, “irrigation”, “EDDY”, “ultrasonic”, “smear layer”, “debris”, “tissue” and “disinfection”) were selected as the primary search terms. When similar words or expressions came up, terms were enriched or amended and the search was repeated to retrieve maximum and accurate results. An example of the final search strategy and the corresponding results in Pubmed are listed in Table 1. The references of all included articles were searched as well to avoid missing information.
Study selection
Two reviewers (CX and FS) screened the titles and abstracts of all the articles independently after the exclusion of duplicate records. When either reviewer found a study potentially eligible according to the inclusion criteria, the full text was obtained. Both reviewers assessed the full texts and decided on final inclusion by consensus or in consultation with a third reviewer (ZX).
Data extraction
Tables for data extraction were designed according to the following items: author(year), sample size and types, apical preparation size, parameters of activation systems, irrigation protocols, research indications, observational sites, evaluation methods and main results. Two reviewers (CX and FS) performed the data extraction independently. Study authors would be contacted for clarification if any uncertainty came up. Disagreements were resolved through discussion or with the help of a third reviewer (ZX).
Quality assessment
The assessment of the included studies was conducted based on the method used in previous systematic reviews [27, 28] with adjustments. The assessment items were as follows: (i) sample size calculation, (ii) samples with similar dimensions, (iii) standardization of procedures, (iv) blinding of sampling and assessment, (v) statistical analysis and (vi) other bias. Each item of each included study was judged as “low” (green dot) or “high” (red dot) risk of bias. Two trained reviewers (CX and ZW) performed the assessment independently. Disagreements were resolved by discussion or with the help of a third reviewer (ZX). Each included study was given an overall judgment according to the risk of bias in each domain:
-
a)
Low risk of bias: studies that had all the items with low risk of bias;
-
b)
Moderate risk of bias: studies that had 4 to 5 items with low risk of bias;
-
c)
High risk of bias: studies that had less than 4 items with low risk of bias.
Meta-analysis
Qualitative analyses were performed separately on the reduction of smear layer, debris, soft tissue and microbes. Meta-analyses were conducted only when the required data were accessible and the analyses were meaningful; that is, if the study designs and outcome variables were similar enough for the quantitative synthesis to make sense. Therefore, only the articles evaluating the smear layer removal and the debris elimination with available data were included in the respective meta-analyses, because they shared similar methodologies. Standardized mean difference (SMD) and the corresponding 95% confidence interval (95% CI) were calculated for each eligible study. Heterogeneity was measured by the Chi2 test and the I2 test. When p < 0.1 or I2 > 50%, heterogeneity was regarded as substantial and the random-effects model was used to estimate the overall effect size, otherwise the fixed-effect model was used. Statistical heterogeneity was explored by analyzing methodological diversity rather than subgroup analyses or meta-regression, on account of the inadequate number of studies in each meta-analysis. All analyses were performed using Review Manager software (Revman 5.4.1).
Results
Study selection
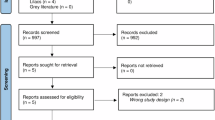
The search process was shown in Fig. 1. The database search resulted in 329 records. 173 duplicates and 115 ineligible records were removed after titles and abstracts were screened, remaining 41 records for full-text evaluation. After assessing all the full texts in detail, we excluded 12 articles [12, 29,30,31,32,33,34,35,36,37,38,39] as they did not study EDDY and other 10 articles [40,41,42,43,44,45,46,47,48,49] as apices were not sealed before root canal irrigation. 19 studies [13, 22,23,24,25, 50,51,52,53,54,55,56,57,58,59,60,61,62,63] meeting all the inclusion criteria were included in the review. No additional study was added after a manual search of the reference of the included articles.

A flowchart of the literature search process
Characteristics of the included studies
The characteristics of all the 19 included studies are listed in Tables 2 and 3. Five articles [50, 54, 57, 60, 63] compared the removal of the smear layer between EDDY and UAI. The elimination of debris was explored in 10 studies [23,24,25, 51, 54, 57, 58, 60, 62, 63]. Two articles [13, 56] compared the remnants of soft tissue, and other 6 articles [22, 52, 53, 55, 59, 61] studied the disinfection efficacy. In terms of experimental subjects, 16 studies [13, 22, 23, 25, 50,51,52,53,54,55,56,57,58, 60, 61, 63] were carried out using extracted human permanent teeth, and 3 studies [24, 59, 62] used canal models. The oscillation frequency of UAI in most included studies was set in the 28–40 kHz range, while ED was driven at a frequency of 5 kHz or 6 kHz, different from UAI at a factor of 4.7–6.7. Only 1 article [57] analyzed the activation effects after canal instrumentation and during instrumentation, while the other 18 studies explored only the former.
Description of Different Indicators
Smear layer
The effects on smear layer removal of UAI and ED were all evaluated with SEM in the 5 relevant studies. No significant differences were observed between the two activation methods in 4 studies [50, 54, 57, 60], whereas Al-Rujaib et al. [63] found significantly more smear layer was removed by ED than UAI at coronal, middle and apical thirds. Plotino et al. [57] suggested no significant differences in the removal of the smear layer when UAI or ED was used both during and after instrumentation.
Debris
Four studies [54, 57, 60, 63] evaluated the debris remnants via SEM. Other 3 studies [23, 25, 58] compared the debris reduction in curved canals with isthmus using micro-CT. Alsubait et al. [51] explored the debris reduction at the cross section of the canal isthmus observed by a stereomicroscope. Plotino et al. [24] and Al-Jadaa et al. [62]. used canal resin blocks filled with dentin debris to assess debris removal efficacy by the digital camera. Among all these 10 studies, Al-Rujaib et al. [63] observed significantly less debris left at the apical thirds after ED irrigation than UAI under SEM, while Linden et al. [23] found significantly more debris removed by UAI than ED using micro-CT analysis; the rest 8 studies found no significant differences between them.
Soft tissue
Conde et al. [13] used pigs’ palatal mucosa to mimic pulp tissue and found no significant differences in soft tissue reduction after UAI or EDDY activation. Iandolo et al. [56] conducted all the experiments with pulp tissue from premolars and showed comparable results between UAI and ED. No meta-analysis was performed due to the different methodologies of the 2 studies.
Disinfection
Five articles [22, 52, 53, 55, 61] inoculated canals with microbes and counted colony-forming units to explore the disinfection ability of ED compared to UAI. Inoculated bacteria included Enterococcus faecalis [22, 52, 53, 55, 61], Streptococcus [22, 55], Actinomyces viscosus [22], Fusobacterium nucleatum [22], Candida albicans [22] and intracanal isolates from endodontic retreatment [22]. Two studies [22, 55] indicated that ED was more effective against microbes than UAI in root canals contaminated after instrumentation. The rest 3 articles [52, 53, 61] found no significant differences in bacterial elimination between UAI and ED. On the other hand, Swimberghe et al. [59] used biofilm-mimicking hydrogel and found that UAI removed significantly more hydrogel than ED. No meta-analysis was conducted on disinfection efficacy due to the different methods and reported outcomes of the included studies.
Meta-analysis
Four studies [50, 54, 57, 60] were included in the meta-analyses on the smear layer removal, and no significant differences were found between UAI and ED at all canal thirds (coronal [SMD = 0.08, 95% CI: -0.29 to 0.45, I2 = 0%]; middle [SMD = 0.02, 95% CI: -0.44 to 0.47, I2 = 0%]; apical [SMD = 0.01, 95%CI: -0.35 to 0.38, I2 = 0%]) (Fig. 2). Meta-analyses on the debris removal were conducted separately on the 3 SEM studies [54, 57, 60] and the 3 micro-CT studies [23, 25, 58]. Both the former (coronal [SMD = 0.03, 95% CI: -0.41 to 0.46, I2 = 23%]; middle [SMD = -0.24, 95% CI: -0.83 to 0.35, I2 = 0%]; apical [SMD = 0.24, 95%CI: -0.20 to 0.67, I2 = 2%]) (Fig. 3) and the latter (SMD = 0.36, 95% CI: -0.67 to 1.40, I2 = 70%) (Fig. 4) found no significant differences between the two activation methods.

Forest plots of smear layer removal at a coronal, b middle and c apical thirds

Forest plots of debris removal at a coronal, b middle and c apical thirds evaluated by SEM

Forest plot of debris removal evaluated by micro-CT
Quality assessment
The quality assessments on all the 19 eligible studies were listed in Figs. 5 and 6. The overall risk of bias in the included studies was evaluated as low (n = 3) [23, 51, 59], moderate (n = 12) [13, 24, 25, 50, 53,54,55,56,57,58, 62, 63] and high (n = 4) [22, 52, 60, 61]. Most studies did not conduct sample size calculation or blinding during sampling and outcome assessment.

Risk of bias of each included study

Summary of risk of bias
Discussion
This systematic review aimed to compare the cleaning efficacy of the EDDY activation system with ultrasonically-activated irrigation in root canals. We excluded the studies without closed canal systems. Root apices are naturally surrounded by periodontium, which can act as a barrier to the overflow of rinsing fluid during clinical treatments. Sealed apical foramens of extracted teeth and canal models can mimic the in vivo environment better than open ones. Tay et al. [64] found that closed canal systems achieved significantly worse cleanliness in canals than the open ones after irrigation. This might be attributed to intracanal matter flushing out through the apical foramen in the open-end system. However, it was worth noting that one-third of the excluded articles were eliminated owing to not sealing apices. More attention should be paid to the importance of apical disclosure in irrigation experiments.
The ability of ED and UAI to remove the smear layer was studied in 5 articles [50, 54, 57, 60, 63]. Four of them [50, 54, 57, 60] found no significant differences between the two activation systems at all canal thirds. These results are consistent with the outcomes of the meta-analysis on the smear layer with unimportant heterogeneity. Only Al-Rujaib et al. [63] found ED significantly better than UAI at all canal portions, but the experimental data were unobtainable, and this article was thus not included in meta-analyses. The results of the 5 studies indicated that the ability of ED to remove the smear layer was at least comparable to that of UAI, but further investigations are needed to prove the superiority of ED. Paixão et al. [65] conducted a meta-analysis comparing the smear layer removal between ultrasonically-activated irrigation and sonically-activated irrigation. The analysis found that UAI had significantly poorer performance than the latter at apical thirds with substantial heterogeneity. Nevertheless, this quantitative synthesis included only 2 articles, which applied ED and the EndoActivator activation system (33-167 Hz; Dentsply, Tulsa, OK) as the final sonic activation systems. Although both systems vibrate at acoustic frequencies, their frequencies differ by more than 30 times. So wide is the gap that it might lead to different cleaning effectiveness, which could be one of the sources of the substantial heterogeneity. Therefore, the significance of this meta-analysis remained to be discussed.
Totally 10 studies [23,24,25, 51, 54, 57, 58, 60, 62, 63] compared the debris elimination between UAI and ED using various methods. Plotino et al. [24] found ED removed significantly more debris than UAI using canal resin models filled with dentinal debris. Nevertheless, the simulated main canals and accessory canals in this study were much wider than the actual ones in human teeth. Thus, the experimental results might deviate from clinical practice. Al-Jadaa et al. [62] also conducted experiments on resin blocks but with a much more realistic canal system, and detected similar effects between ED and UAI in the closed canal system. Alsubait et al. [51] observed debris in isthmuses under a stereomicroscope at 50 × magnification and found no significant differences between the two activation methods. 3 studies [23, 25, 58] evaluated debris in curved canals connected by isthmuses using micro-CT. Their quantitative synthesis showed insignificant differences between UAI and ED but with substantial heterogeneity. This heterogeneity might arise from different canal instrumentation systems, preparation sizes and parameters of UAI. The absence of 17%EDTA in the final irrigation protocol [23] might also be accountable for the heterogeneity, as 17%EDTA was effective in debris elimination [6]. Other 4 studies [54, 57, 60, 63] conducted SEM analysis to assess debris remnants, and their meta-analyses (except Al-Rujaib et al. [63] as mentioned above) found ED as effective as UAI at any canal third with unimportant heterogeneity.
Devices like digital cameras or stereoscopes allow for rough observation of canal walls but can hardly discover tiny chips due to their low resolution. In this regard, scanning electron microscopes and micro-CT with high resolution can perform better. However, it is undeniable that SEM and micro-CT have their limitations when applied to canal irrigation experiments. Longitudinal observation for pre- and post-irrigation comparison is impracticable in SEM analysis [66] due to the necessary process of dehydration and metallization. Orlowski et al. [67] evaluated the smear layer before the final irrigation using low-vacuum SEM after only dehydration without gold sputtered, and observed the same areas after irrigation under high-vacuum SEM. Although this method allowed for longitudinal evaluation, the process of desiccation may alter the structure of smear layer, which contains water-bearing soft tissue, biofilms and dentinal debris [68]. Desiccation may lead to greater brittleness [69] of smear layer and debris and makes them more removable. Given the drawbacks of SEM, micro-CT was recommended as it was capable of non-destructive three-dimensional imaging and allowed for longitudinal observation [6]. However, micro-CT omits debris with low radiopacity such as soft-tissue chips and biofilms that are distinguishable under SEM [70]. From this perspective, it can be deduced that although each observational method has its defects, the overall consideration of all the results from different methods may offset their weakness and improve the reliability. Consequently, in view of all the results and factors mentioned above, a conclusion can be drawn that ED is comparable to UAI in removing the smear layer and debris.
The efficacy of soft tissue removal was studied in only 2 included articles. Conde et al. [13] found ED was as effective as UAI in eliminating soft tissue placed in artificial grooves by weighing the tissue pre- and post-irrigation. Iandolo et al. [56] calculated the area of the pulps placed in the isthmus and also found no significant differences. These results suggested that ED might have similar effects to UAI on removing soft tissue in complex anatomic sites in root canals.
Six studies explored the disinfection effects. Neuhaus et al. [22] introduced different species of microbes into both straight and curved root canals. The results showed that EDDY was significantly more effective than that of UAI in all the short-term disinfection experiments. But these results were based on the experiments conducted with only normal saline as the final irrigant, which might greatly reduce the disinfection efficacy. Moreover, EDDY tips were placed at the working length, which was different from the depth of UAI tips and might cause severer apical extrusion in clinical practice [71]. Thus, the clinical extrapolation of the results should be done with caution. Hoedke et al. [55] found ED significantly better than UAI at disinfection when the canals were contaminated after the entire instrumentation process. But it also found no significant difference when the contamination was done before the instrumentation of the final file. This contradiction might be attributed to the partial removal of bacteria during the mechanical preparation. The gap between ED and UAI in disinfection ability might thus be narrowed down to insignificance. However, the above-mentioned two experiments were short-term (3 and 5 days respectively) infection models, where the microbes had not yet penetrated deeply into dentinal tubules [72, 73]. In long-term (28 days) infection models [52, 61], ED and UAI showed comparable results in eliminating Enterococcus faecalis. On the other hand, Swimberghe et al. [59] used hydrogel to mimic pulp tissue in complex anatomic sites. This study found that UAI removed significantly more hydrogel than ED in canal models with a curvature of 45 degrees. Although the hydrogel mixture was demonstrated to share similar viscoelastic behaviors to biofilms, whether the shear stress required to remove the hydrogel was similar to that of biofilms remains unknown. Shear stress also plays a role in microbe elimination [74]. Furthermore, disinfection not only lies on the smash and removal of biofilms by mechanical washing, but also counts on sufficient contact of antimicrobial irrigants with intracanal microbes to disable their toxicity and fertility. To sum up, despite the different experimental designs and outcomes, it can be inferred that ED was as effective as UAI in disinfection.
The oscillation frequency of UAI is more than four times higher than that of ED. UAI can generate cavitation and acoustic streaming in water with its high-frequency vibration [16]. But no cavitation was detected during EDDY activation [45]. And ED might not be able to produce acoustic streaming due to its high amplitude (approximately 350 μm [45, 75]) according to the theoretical analysis [76]. However, despite the inability to generate cavitation and acoustic streaming, ED seemed to achieve comparable cleaning efficacy as UAI did according to the results in the present review. This implied that oscillation frequency might not be the most crucial factor for root canal irrigation. ED has a higher amplitude than UAI [45]. EDDY tips make three-dimensional orbital movements [45], while UAI files oscillate transversely in one plane [77]. These facts suggested that the amplitude or the oscillation direction might also play an important role in root canal irrigation. But more basic researches are needed to further explore the mechanism of ED for irrigation activation. On the other hand, too high a frequency of UAI might cause damage to canal walls. Al-Jadaa et al. [78] applied irrigation to resin blocks and found that ultrasonic stainless steel tips produced canal ledgings and transportation while polymer tips of sonic activation did not. Experiments on extracted teeth also detected unintentional removal of dentin after UAI in both straight [79] and curved [80] canals. It could be inferred from these findings that UAI assisted in removing the smear layer and debris but meanwhile probably produced them. In addition, although the high frequency of UAI led to a greater increase in flow rate and changed liquid from laminar to turbulent flow, the laminar was more conducive to irrigants flowing into narrow anatomic sites because of its regularity [81]. This could be one of the reasons why most included articles that explored cleaning efficacy in isthmus found no superiority of UAI over ED. Another difference between UAI and ED was that the former could result in a higher temperature rise in sodium hypochlorite solution than the latter [82]. But this small temperature difference (< 10 ℃) caused by activation was insufficient to enhance the reaction rate of NaOCl [83]. However, the temperature rise by more than 15 ℃ in the solution could reduce viscosity and increase mobility [81]. This change might improve the ability to eliminate soft tissue [56] and microbes [61]. The combination of activation and heating of irrigants could therefore enhance the effects of root canal irrigation.
Although the frequency of EDDY is within the range of sonic vibration, the results in the present review cannot be extended to other sonically-activated systems, as they are widely different in the oscillation frequency as mentioned above, and even diverse in the operating modes [84,85,86,87].
The studies included in the present review varied widely in experimental methods and outcome measures, especially in the aspects of debris and soft-tissue removal and disinfection, which greatly limited the availability of meta-analyses. Also, the small sample size of each dimension might impair the reliability of this research. Another limitation of this review is that the effectiveness of root canal irrigation was evaluated from an in vitro perspective. The in vitro environments differed from the in vivo ones considerably. Patient factors such as tooth position, mouth opening and systemic diseases might affect the application of UAI and ED, and thus might result in different irrigation effects from that of in vitro experiments. Besides, most included studies decorated the extracted teeth to standardize the sample length, which deviated from clinical practice because the normal coronal approach of working tips was altered. Therefore, caution must be taken in the interpretation and the clinical extrapolation of the results in this review.
Conclusions
After the qualitative and quantitative analysis of the included articles, it could be concluded from the limited evidence that ED was at least equivalent to UAI in root canal irrigation concerning the removal of smear layer, debris, soft tissue and bacteria ex vivo. Considering the metal tips of UAI may damage canal walls, EDDY might be a substitute for UAI to activate irrigation solutions. However, owing to the different circumstances between in vitro experiments and clinical practice, more randomized clinical trials are required to explore the clinical extrapolation of the conclusion in the present review.
Availability of data and materials
All data generated or analyzed during this study are included in the present review.
Abbreviations
- UAI:
-
Ultrasonically-activated irrigation
- ED:
-
EDDY activation system
- SMD:
-
Standardized mean difference
- SEM:
-
Scanning electron microscope
- CI:
-
Confidence interval
- WL:
-
Working length
- Exp:
-
Experiment; NM: not mentioned
References
Mader CL, Baumgartner JC, Peters DD. Scanning electron microscopic investigation of the smeared layer on root canal walls. J Endod. 1984;10(10):477–83.
Yamada RS, Armas A, Goldman M, Lin PS. A scanning electron microscopic comparison of a high volume final flush with several irrigating solutions: part 3. J Endod. 1983;9(4):137–42.
Wayman BE, Kopp WM, Pinero GJ, Lazzari EP. Citric and lactic acids as root canal irrigants in vitro. J Endod. 1979;5(9):258–65.
Paqué F, Barbakow F, Peters OA. Root canal preparation with Endo-Eze AET: changes in root canal shape assessed by micro-computed tomography. Int Endod J. 2005;38(7):456–64.
Augusto CM, Barbosa AFA, Guimarães CC, Lima CO, Ferreira CM, Sassone LM, et al. A laboratory study of the impact of ultraconservative access cavities and minimal root canal tapers on the ability to shape canals in extracted mandibular molars and their fracture resistance. Int Endod J. 2020;53(11):1516–29.
Guerreiro MYR, Belladonna FG, Monteiro LPB, Lima CO, Silva E, Brandão JMS. The influence of the addition of surfactants to sodium hypochlorite on the removal of hard tissue debris. Int Endod J. 2020;53(8):1131–9.
Love RM, Jenkinson HF. Invasion of dentinal tubules by oral bacteria. Crit Rev Oral Biol Med. 2002;13(2):171–83.
Sedgley CM, Lennan SL, Appelbe OK. Survival of Enterococcus faecalis in root canals ex vivo. Int Endod J. 2005;38(10):735–42.
Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014;216(6):299–303.
Arslan H, Capar ID, Saygili G, Gok T, Akcay M. Effect of photon-initiated photoacoustic streaming on removal of apically placed dentinal debris. Int Endod J. 2014;47(11):1072–7.
Li Q, Zhang Q, Zou X, Yue L. Evaluation of four final irrigation protocols for cleaning root canal walls. Int J Oral Sci. 2020;12(1):29.
Neelakantan P, Ounsi HF, Devaraj S, Cheung GSP, Grandini S. Effectiveness of irrigation strategies on the removal of the smear layer from root canal dentin. Odontology. 2019;107(2):142–9.
Conde AJ, Estevez R, Loroño G, Valencia de Pablo Ó, Rossi-Fedele G. Effect of sonic and ultrasonic activation on organic tissue dissolution from simulated grooves in root canals using sodium hypochlorite and EDTA. Int Endod J. 2017;50(10):976–82.
Dutner J, Mines P, Anderson A. Irrigation trends among American Association of Endodontists members: a web-based survey. J Endod. 2012;38(1):37–40.
Virdee SS, Ravaghi V, Camilleri J, Cooper P, Tomson P. Current trends in endodontic irrigation amongst general dental practitioners and dental schools within the United Kingdom and Ireland: a cross-sectional survey. Br Dent J. 2020. https://doi.org/10.1038/s41415-020-1984-x.
Halford A, Ohl CD, Azarpazhooh A, Basrani B, Friedman S, Kishen A. Synergistic effect of microbubble emulsion and sonic or ultrasonic agitation on endodontic biofilm in vitro. J Endod. 2012;38(11):1530–4.
van der Sluis LW, Versluis M, Wu MK, Wesselink PR. Passive ultrasonic irrigation of the root canal: a review of the literature. Int Endod J. 2007;40(6):415–26.
Jiang L-M, Verhaagen B, Versluis M, van der Sluis LWM. Influence of the oscillation direction of an ultrasonic file on the cleaning efficacy of passive ultrasonic irrigation. J Endod. 2010;36(8):1372–6.
Rainwater A, Jeansonne BG, Sarkar N. Effects of ultrasonic root-end preparation on microcrack formation and leakage. J Endod. 2000;26(2):72–5.
Layton CA, Marshall JG, Morgan LA, Baumgartner JC. Evaluation of cracks associated with ultrasonic root-end preparation. J Endod. 1996;22(4):157–60.
Rodríguez-Martos R, Torres-Lagares D, Castellanos-Cosano L, Serrera-Figallo MA, Segura-Egea JJ, Gutierrez-Perez JL. Evaluation of apical preparations performed with ultrasonic diamond and stainless steel tips at different intensities using a scanning electron microscope in endodontic surgery. Med Oral Patol Oral Cir Bucal. 2012;17(6):e988–93.
Neuhaus KW, Liebi M, Stauffacher S, Eick S, Lussi A. Antibacterial efficacy of a New Sonic irrigation device for root canal disinfection. J Endod. 2016;42(12):1799–803.
Linden D, Boone M, De Bruyne M, De Moor R, Versiani MA, Meire M. Adjunctive steps for the removal of hard tissue debris from the anatomic complexities of the mesial root canal system of mandibular molars: a micro-computed tomographic study. J Endod. 2020;46(10):1508–14.
Plotino G, Grande NM, Mercade M, Cortese T, Staffoli S, Gambarini G, et al. Efficacy of sonic and ultrasonic irrigation devices in the removal of debris from canal irregularities in artificial root canals. J Appl Oral Sci. 2019;27: e20180045.
Rödig T, Koberg C, Baxter S, Konietschke F, Wiegand A, Rizk M. Micro-CT evaluation of sonically and ultrasonically activated irrigation on the removal of hard-tissue debris from isthmus-containing mesial root canal systems of mandibular molars. Int Endod J. 2019;52(8):1173–81.
Zeppenfeld W. Endodontischer Einsatz der mittels Airscaler aktivierbaren Kunststoffspülspitze EDDY in der Praxis. Quintessenz Zahnmedizin. 2019;1:26–35.
Silva E, Prado MC, Soares DN, Hecksher F, Martins JNR, Fidalgo TKS. The effect of ozone therapy in root canal disinfection: a systematic review. Int Endod J. 2020;53(3):317–32.
Ballester B, Giraud T, Ahmed HMA, Nabhan MS, Bukiet F, Guivarc’h M. Current strategies for conservative endodontic access cavity preparation techniques-systematic review, meta-analysis, and decision-making protocol. Clin Oral Investig. 2021;25(11):6027–44.
Ertugrul IF, Maden M, Orhan EO, Ozkorucuklu SP. The effect of micro-electric current and other activation techniques on dissolution abilities of sodium hypochlorite in bovine tissues. BMC Oral Health. 2015;15:161.
Hülsmann M, Beckmann C, Baxter S. Debris removal using a hydroxyapatite nanoparticle-containing solution (Vector Polish) with sonic or ultrasonic agitation. Materials (Basel). 2021;14(16):4750.
Karade P, Chopade R, Patil S, Hoshing U, Rao M, Rane N, et al. Efficiency of different endodontic irrigation and activation systems in removal of the smear layer: a scanning electron microscopy study. Iran Endod J. 2017;12(4):414–8.
Kun-Hwa S, Young PT, Ho-Keel H, Hoon JH. Comparison of various activation methods of root canal irrigants for soft-tissue removal. Oral Biol Res. 2021;45(1):16–21.
Mobaraki B, Yeşildal YK. Quantitative analysis of SmearOFF and different irrigation activation techniques on removal of smear layer: a scanning electron microscope study. Microsc Res Tech. 2020;83(12):1480–6.
Mohmmed SA, Vianna ME, Penny MR, Hilton ST, Mordan N, Knowles JC. A novel experimental approach to investigate the effect of different agitation methods using sodium hypochlorite as an irrigant on the rate of bacterial biofilm removal from the wall of a simulated root canal model. Dent Mater. 2016;32(10):1289–300.
Mohmmed SA, Vianna ME, Penny MR, Hilton ST, Mordan N, Knowles JC. Confocal laser scanning, scanning electron, and transmission electron microscopy investigation of Enterococcus faecalis biofilm degradation using passive and active sodium hypochlorite irrigation within a simulated root canal model. Microbiologyopen. 2017;6(4): e00455.
Mohmmed SA, Vianna ME, Penny MR, Hilton ST, Mordan NJ, Knowles JC. Investigations into in situ Enterococcus faecalis biofilm removal by passive and active sodium hypochlorite irrigation delivered into the lateral canal of a simulated root canal model. Int Endod J. 2018;51(6):649–62.
Santos Nogueira L, Amaral G, Silva EJNL, Tinoco JMM, Alves FRF, Sassone LM. Bacterial reduction in oval-shaped root canals after different irrigant agitation methods. Eur Endod J. 2021;6(1):110–6.
Susan A, Bharathraj A, Praveen M, Mohan Kumar N, Karunakaran J. Intraradicular smear removal efficacy of triphala as a final rinse solution in curved canals: a scanning electron microscope study. J Pharm Bioallied Sci. 2019;11(6):S420–8.
Yilmaz M, Yilmaz S, Dumani A, Kuden C, Yoldas O. Effects of seven different irrigation techniques on debris and the smear layer: a scanning electron microscopy study. Niger J Clin Pract. 2017;20(3):328–34.
Xiao F, Zhu Y, Dai Q. Effectiveness of ultrasonic, sonic and conventional irrigation in removing smear layer: a comparative study. Jiangxi Med J. 2021;56(5):557-8,70.
Al-Obaida MI, Moukaddem R, Allahem Z, AbdulWahed A, AlOnaizan FA, Al-Madi EM. Comparison of bacterial removal from dentinal tubules with different irrigant agitation techniques: an in vitro study. Saudi Dent J. 2019;31(4):431–6.
Jasrotia A, Bhagat K, Bhagat N, Bhagat RK. Comparison of Five Different irrigation techniques on smear layer removal in apical thirds of root canals of mandibular first premolar: a scanning electron microscopic study. J Int Soc Prev Commun Dentistry. 2019;9(6):630–6.
Khaord P, Amin A, Shah MB, Uthappa R, Raj N, Kachalia T, et al. Effectiveness of different irrigation techniques on smear layer removal in apical thirds of mesial root canals of permanent mandibular first molar: a scanning electron microscopic study. J Conserv Dent. 2015;18(4):321–6.
Nogueira L, Amaral G, Silva E, Tinoco J, Alves F, Sassone LM. Bacterial reduction in oval-shaped root canals after different irrigant agitation methods. Eur Endod J. 2021;6(1):110–6.
Swimberghe RCD, De Clercq A, De Moor RJG, Meire MA. Efficacy of sonically, ultrasonically and laser-activated irrigation in removing a biofilm-mimicking hydrogel from an isthmus model. Int Endod J. 2019;52(4):515–23.
Mei X, Liu J, Cheng X, Fan X, You S, Tan M, et al. Bactericidal effect of ultrasound, sonic device and laser radiation on root canal irrigation in root infection model in vitro. Chin J Pract Stomatol. 2021;14(6):686–92.
Al-Zuhair H, Su Z, Liu H, Wang Z, Haapasalo M, Hieawy A, et al. Antimicrobial effects of agitational irrigation on single- and multispecies biofilms in dentin canals. Odontology. 2023;111(1):49–56.
Liu C, Li Q, Yue L, Zou X. Evaluation of sonic, ultrasonic, and laser irrigation activation systems to eliminate bacteria from the dentinal tubules of the root canal system. J Appl Oral Sci. 2022;30: e20220199.
Uslu G, Gündoğar M, Üngör M, Özyürek T, Erkan E, Keskin NB. Investigation of the effectiveness of sonic, ultrasonic and new laser-assisted irrigation activation methods on smear removal and tubular penetration. Lasers Med Sci. 2023;38(1):30.
Zhang H, Wang S, Ren Y, Kong X, Wang D Y. X. Cleaning effectiveness of different irrigation techniques on root canal walls: an in vitro study. J Oral Sci Res. 2021;37(9):805–9.
Alsubait S, Alshaibani Y, Alshehri N, Alnuwaiser N, Alajimi T, Almaflehi N, et al. Efficacy of different endodontic irrigant activation techniques on debris removal from the mesial root canal system of mandibular molars. J Contemp Dent Pract. 2021;22(3):231–6.
Eneide C, Castagnola R, Martini C, Grande NM, Bugli F, Patini R, et al. Antibiofilm activity of three different irrigation techniques: an in vitro study. Antibiotics (Basel). 2019;8(3):112.
Hage W, De Moor RJG, Hajj D, Sfeir G, Sarkis DK, Zogheib C. Impact of different irrigant agitation methods on bacterial elimination from infected root canals. Dent J (Basel). 2019;7(3):64.
Haupt F, Meinel M, Gunawardana A, Huelsmann M. Effectiveness of different activated irrigation techniques on debris and smear layer removal from curved root canals: a SEM evaluation. Aust Endod J. 2020;46(1):40–6.
Hoedke D, Kaulika N, Dommisch H, Schlafer S, Shemesh H, Bitter K. Reduction of dual-species biofilm after sonic- or ultrasonic-activated irrigation protocols: a laboratory study. Int Endod J. 2021;54(12):2219–28.
Iandolo A, Amato M, Abdellatif D, Barbosa AFA, Pantaleo G, Blasi A, et al. Effect of different final irrigation protocols on pulp tissue dissolution from an isthmus model. Aust Endod J. 2021;47(3):538–43.
Plotino G, Colangeli M, Özyürek T, DeDeus G, Panzetta C, Castagnola R, et al. Evaluation of smear layer and debris removal by stepwise intraoperative activation (SIA) of sodium hypochlorite. Clin Oral Investig. 2021;25(1):237–45.
Rodrigues CT, EzEldeen M, Jacobs R, Lambrechts P, Alcalde MP, Hungaro Duarte MA. Cleaning efficacy and uncontrolled removal of dentin of two methods of irrigant activation in curved canals connected by an isthmus. Aust Endod J. 2021;47(3):631–8.
Swimberghe RCD, Buyse R, Meire MA, De Moor RJG. Efficacy of different irrigation technique in simulated curved root canals. Lasers Med Sci. 2021;36(6):1317–22.
Urban K, Donnermeyer D, Schäfer E, Bürklein S. Canal cleanliness using different irrigation activation systems: a SEM evaluation. Clin Oral Investig. 2017;21(9):2681–7.
Yared G, Al Asmar Ramli G. Antibacterial ability of sodium hypochlorite heated in the canals of infected teeth: an ex vivo study. Cureus. 2020;12(2):e6975.
Al-Jadaa A, Saidi Z, Mahmoud M, Al-Taweel R, Zehnder M. Assessment of irrigant agitation devices in simulated closed and open root canal systems. J Endod. 2023. https://doi.org/10.1016/j.joen.2023.01.002.
Al-Rujaib BA, Zaghloul MH, Reda A, Badr AE. Efficacy of different endodontic irrigant activation systems on smear layer removal and canal cleanliness: comparative scanning electron microscopic study. Open Access Maced J Med Sci. 2022;10:295–302.
Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, Zhang K, et al. Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J Endod. 2010;36(4):745–50.
Paixão S, Rodrigues C, Grenho L, Fernandes MH. Efficacy of sonic and ultrasonic activation during endodontic treatment: a meta-analysis of in vitro studies. Acta Odontol Scand. 2022. https://doi.org/10.1080/00016357.2022.2061591:1-8.
De-Deus G, Reis C, Paciornik S. Critical appraisal of published smear layer-removal studies: methodological issues. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(4):531–43.
Orlowski NB, Schimdt TF, Teixeira CD, Garcia LFR, Savaris JM, Tay FR, et al. Smear layer removal using passive ultrasonic irrigation and different concentrations of sodium hypochlorite. J Endod. 2020;46(11):1738–44.
Goldman LB, Goldman M, Kronman JH, Lin PS. The efficacy of several irrigating solutions for endodontics: a scanning electron microscopic study. Oral Surg Oral Med Oral Pathol. 1981;52(2):197–204.
Bajaj D, Sundaram N, Nazari A, Arola D. Age, dehydration and fatigue crack growth in dentin. Biomaterials. 2006;27(11):2507–17.
Siqueira JF Jr, Pérez AR, Marceliano-Alves MF, Provenzano JC, Silva SG, Pires FR, et al. What happens to unprepared root canal walls: a correlative analysis using micro-computed tomography and histology/scanning electron microscopy. Int Endod J. 2018;51(5):501–8.
Magni E, Jäggi M, Eggmann F, Weiger R, Connert T. Apical pressures generated by several canal irrigation methods: a laboratory study in a maxillary central incisor with an open apex. Int Endod J. 2021;54(10):1937–47.
Kirsch J, Basche S, Neunzehn J, Dede M, Dannemann M, Hannig C, et al. Is it really penetration? Locomotion of devitalized Enterococcus faecalis cells within dentinal tubules of bovine teeth. Arch Oral Biol. 2017;83:289–96.
Kirsch J, Basche S, Neunzehn J, Dede M, Dannemann M, Hannig C, et al. Is it really penetration? Part 2. Locomotion of Enterococcus faecalis cells within dentinal tubules of bovine teeth. Clin Oral Investig. 2019;23(12):4325–34.
Broekman S, Pohlmann O, Beardwood ES, de Meulenaer EC. Ultrasonic treatment for microbiological control of water systems. Ultrason Sonochem. 2010;17(6):1041–8.
Baars S. Development and analysis of a sonically activated instrument for cleaning dental root canals (in German) [PhD thesis]. Munich: Technical University of Munich; 2014.
Verhaagen B, Boutsioukis C, van der Sluis LWM, Versluis M. Acoustic streaming induced by an ultrasonically oscillating endodontic file. J Acoust Soc Am. 2014;135(4):1717–30.
Ahmad M, Roy RA, Kamarudin AG, Safar M. The vibratory pattern of ultrasonic files driven piezoelectrically. Int Endod J. 1993;26(2):120–4.
Al-Jadaa A, Paqué F, Attin T, Zehnder M. Acoustic hypochlorite activation in simulated curved canals. J Endod. 2009;35(10):1408–11.
Boutsioukis C, Tzimpoulas N. Uncontrolled removal of dentin during in vitro ultrasonic irrigant activation. J Endod. 2016;42(2):289–93.
Retsas A, Koursoumis A, Tzimpoulas N, Boutsioukis C. Uncontrolled removal of dentin during in vitro ultrasonic irrigant activation in curved Root Canals. J Endod. 2016;42(10):1545–9.
Bukiet F, Soler T, Guivarch M, Camps J, Tassery H, Cuisinier F, et al. Factors affecting the viscosity of sodium hypochlorite and their effect on irrigant flow. Int Endod J. 2013;46(10):954–61.
Donnermeyer D, Schäfer E, Bürklein S. Real-time intracanal temperature measurement comparing mechanically and laser-activated irrigation to syringe irrigation. Aust Endod J. 2021;47(1):59–66.
Macedo RG, Verhaagen B, Wesselink PR, Versluis M, van der Sluis LW. Influence of refreshment/activation cycles and temperature rise on the reaction rate of sodium hypochlorite with bovine dentine during ultrasonic activated irrigation. Int Endod J. 2014;47(2):147–54.
Kharouf N, Pedullà E, La Rosa GRM, Bukiet F, Sauro S, Haikel Y, et al. In vitro evaluation of different irrigation protocols on intracanal smear layer removal in teeth with or without pre-endodontic proximal wall restoration. J Clin Med. 2020;9(10):1–15.
Seven N, Cora S. Effectiveness of different irrigation systems in the presence of intracanal-separated file. Microsc Res Tech. 2019;82(3):238–43.
Mancini M, Cerroni L, Iorio L, Dall’Asta L, Cianconi L. FESEM evaluation of smear layer removal using different irrigant activation methods (EndoActivator, EndoVac, PUI and LAI). An in vitro study. Clin Oral Investig. 2018;22(2):993–9.
Capar ID, Aydinbelge HA. Effectiveness of various irrigation activation protocols and the self-adjusting file system on smear layer and debris removal. Scanning. 2014;36(6):640–7.
Acknowledgements
The authors wish to thank Dr. Shengli An (Department of Bio-Statistics, Guangdong Provincial Key Laboratory of Tropical Disease Research, School of Public Health and Tropical Medicine, Southern Medical University, Guangzhou, Guangdong, China) and Dr. Tingting Ning (Department of Endodontics, Stomatological Hospital, Southern Medical University, Guangzhou, China) for the valuable suggestions on the study design and statistical analysis.
Funding
This study was supported by National Natural Science Foundation of China (grant no. 81800957) in relation to English proofreading.
Author information
Authors and Affiliations
Contributions
CX and ZX designed the research. CX conducted the literature search. CX and FS conducted the study selection and data extraction. CX and ZW performed the quality assessment and data analysis. CX was a major contributor to the manuscript. FS prepared all the tables and figures. ZX and XS critically revised the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chu, X., Feng, S., Zhou, W. et al. Cleaning efficacy of EDDY versus ultrasonically-activated irrigation in root canals: a systematic review and meta-analysis. BMC Oral Health 23, 155 (2023). https://doi.org/10.1186/s12903-023-02875-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-02875-6