
Abstract
Background
Few studies have investigated oral health-related quality of life (OHRQoL) in young individuals with juvenile idiopathic arthritis (JIA). Aims were to investigate whether OHRQoL differs between children and adolescents with JIA compared to controls without JIA, while adjusting for socio-demographic-, behavioral- and oral health-related covariates. Furthermore, to explore whether socio-behavioral and oral health-related covariates of OHRQoL vary according to group affiliation and finally, specifically for individuals with JIA, to investigate whether disease-specific features associate with OHRQoL. We hypothesized that participants with JIA have poorer OHRQoL compared to participants without JIA.
Methods
In this comparative cross-sectional study participants with JIA (n = 224) were matched to controls without JIA (n = 224). OHRQoL was assessed according to Early Childhood Oral Health Impact Scale (ECOHIS) (4–11-years-olds) and the child version of Oral Impacts on Daily Performances (Child-OIDP) (12–16-years-olds). JIA-specific characteristics were assessed by pediatric rheumatologists and socio-demographic, behavioral and self-reported oral health information collected by questionnaires. Index teeth were examined for caries by calibrated dentists. Multiple variable analyses were performed using logistic regression, reporting odds ratio (OR) and 95% confidence interval (CI). Two-way interactions were tested between group affiliation and the socio-behavioral- and oral health-related variables on the respective outcome variables.
Results
In total, 96 participants with JIA and 98 controls were evaluated according to ECOHIS, corresponding numbers for Child-OIDP was 125 and 124. Group affiliation was not associated with impaired ECOHIS or Child-OIDP in adjusted analyses (OR = 1.95, 95% CI 0.94–4.04 and OR = 0.99, 95% CI 0.46–2.17, respectively). Female adolescents with JIA were more likely than males to report oral impacts according to Child-OIDP. Continued activity or flare was found to adversely affect Child-OIDP, also self-reported outcome measures in JIA associated with Child-OIDP.
Conclusions
This study did not provide consistent evidence to confirm the hypothesis that children and adolescents with JIA are more likely to have impaired OHRQoL compared to their peers without JIA. However, female adolescents with JIA were more likely than males to report impacts on OHRQoL. Furthermore, within the JIA group, adolescents with continued disease activity, flare or reporting pain, physical disability, had higher risk than their counterparts of impaired OHRQoL.
Similar content being viewed by others


Background
As the most common chronic rheumatic disease in children, juvenile idiopathic arthritis (JIA) represents a complex heterogeneous group of arthritis and might constitute an important cause of disability and reduced quality of life [1, 2]. Pooled estimates of incidence and prevalence rates for Caucasians are 8.3/100,000 and 32.6/100,000, respectively, but estimates vary greatly across countries [3]. For most children JIA is a chronic, often life-long, disease. Objectives of disease management is remission, minimizing comorbidities and harmful side-effects of medication, and achieving best possible function, growth and development, quality of life, and social involvement [4].
Several manifestations of rheumatic diseases are observed in the oral cavity such as mucosal lesions, reduced salivary flow and inflammation in periodontal tissues [5]. Previous reviews have demonstrated poor oral health indicators in children with JIA [6, 7]. A recent systematic review and meta-analysis by our research team focusing on oral disease and problems among children and adolescents with JIA, revealed, however, that dental caries in young individuals with JIA was comparable to that of the general population, whereas periodontal diseases and temporomandibular disorder (TMD) were estimated to be more prevalent, compared to individuals without JIA [8].
According to the definition of the World Dental Federation [9, 10], reflecting the biopsychosocial view of health addressed by the World Health Organization [11], oral health encompasses “the ability to speak, smile, taste, touch, chew, swallow, and convey a range of emotions through facial expressions with confidence and without pain, discomfort, and disease of the craniofacial complex”. To capture the different dimensions of oral health, oral health-related quality of life (OHRQoL) measurements are conducive, as conventional clinical oral indices alone are insufficient to assess the multifaceted nature of oral health. Generic OHRQoL instruments have been developed to measure physical- and psycho-social consequences of various oral diseases and problems, whereas condition specific OHRQoL measures capture subtle variance in specific oral conditions [12]. Measuring OHRQoL in children are challenging due to continuous dental, facial and cognitive development [13]. Thus, age-dependent generic child OHRQoL indices have been developed for self- or proxy-reporting of children’s OHRQoL [12], such as the Child Oral Health-related Quality of Life measure (COHQoL) [14,15,16], the child version of Oral Impacts on Daily Performances (Child-OIDP) [17], and the Early Childhood Oral Health Impact Scale (ECOHIS) [18]. The latter specifically developed for younger children. Only ECOHIS and Child-OIDP have been validated in the context of a Norwegian child and adolescent population [19]. Although these indices have been used to evaluate OHRQoL in children and adolescents with chronic diseases [20, 21], studies investigating OHRQoL in children and adolescents with JIA are scarce [22,23,24,25,26].
Isola et al. [23] reported that individuals with temporomandibular joint (TMJ) arthritis had poorer OHRQoL compared to individuals with JIA without TMJ arthritis and controls, using the Child Perception Questionnaire (CPQ11-14), a component of the inventory COHQoL. Using CPQ11-14, Polizzi et al. [25] found JIA patients with periodontitis to have poorer OHRQoL, compared to JIA patients without periodontitis and controls. Santos et al. [22] observed no difference in impaired OHRQoL in individuals with JIA compared to controls using the Parental-Caregiver Perceptions Questionnaire, another component of the COHQoL inventory. The Psychosocial Impact of Dental Aesthetics Questionnaire has also been used among adolescents with JIA and controls of same age, indicating that adolescents with JIA were less concerned by dental aesthetics than controls [24]. Furthermore, Rahimi et al. [26] documented self-reported orofacial symptoms and dysfunction to be frequent in adolescents with JIA and by using CPQ11-14 they found orofacial symptoms to have a negative impact on OHRQoL.
Evidently, demographic- and socio-economic characteristics in addition to clinical indicators of oral health, play a prominent role as independent determinants of OHRQoL [27,28,29]. However, none of the previous studies assessing OHRQoL in children and adolescents with JIA [22,23,24,25,26] have included socio-economic characteristic of the participants as important covariates of OHRQoL. Thus, knowledge of the impact of social-economic characteristics on OHRQoL among young individuals with JIA and whether the impact of those characteristics differs between individuals with and without JIA is quite limited. Hence, high-quality research focusing on OHRQoL in children and adolescents with JIA is in demand [8]. Such studies are important as they facilitate comprehension of the relationship between oral health and general health [13].
The aims of this study were to investigate whether OHRQoL, assessed by the ECOHIS and Child-OIDP scale, differs between children and adolescents with JIA compared to controls without JIA, while adjusting for socio-demographic-, behavioral- and oral health-related covariates. Furthermore, to explore whether socio-behavioral and oral health-related covariates of OHRQoL vary according to group affiliation and finally, specifically for individuals with JIA, to investigate whether disease-specific features associate with OHRQoL. We hypothesized that participants with JIA have poorer OHRQoL compared to participants without JIA.
Methods
Study design and participants
NorJIAFootnote 1 is a prospective longitudinal multicenter study that contributes baseline data to the present comparative cross-sectional study. Baseline data on dental caries have recently been published [30], whereby sample size calculation and calibration are presented. A detailed description of sample size calculation (according to caries estimates) and calibration are presented in Additional files 1 and 2, respectively. Young individuals (4–16 years old) with JIA, diagnosed according to the criteria specified by the International League of Associations for Rheumatology (ILAR) [31] were invited to participate. The only exclusion criterion was the lack of written informed consent. Baseline data were collected between April 2015 and August 2018.
Specialists in pediatrics at three out of total four university hospitals, widely distributed across Norway (western, central, and northern Norway), were responsible for the enrollment of children and adolescents with JIA. After a thorough medical examination the participants were referred for an oral examination at the corresponding Oral Health Centre of Expertise and matched 1:1 with controls based on sex, age, center site, and mothers’ country of origin (western or non-western). The controls were without JIA and underwent an oral examination at one of seven different Public Dental Service clinics, representing both rural and urban communities [30]. The controls’ appointment was coordinated with a planned regular oral health check, and as incentive for participation, two cinema tickets were provided. The term group affiliation in this article reflects participants with JIA or controls.
Oral health questionnaires
Self-administered questionnaires provided socio-demographic, behavioral and self-reported oral health information [30]. Socio-demographic variables included educational level of caregivers, number of caregivers in the household and mother’s country of origin. Behavioral variables consisted of toothbrushing and tooth flossing frequency, while self-reported oral health indicators were gingival bleeding during toothbrushing and pain or discomfort during toothbrushing. Moreover, evaluation of self-reported oral health and satisfaction with appearance of teeth (global measures) were collected (for the participants ≥ 12 years the global oral health measures were assessed by an interview). The coding of these self-reported variables is shown in Additional file 3: Table S1.
ECOHIS
A validated Norwegian version of ECOHIS [19], originally developed by Pahel et al. [18], was used to evaluate caregivers’ perception of the OHRQoL of their 4–11 years-old children and their families with reference to the child’s entire lifetime experience of oral diseases and dental treatment. ECOHIS consists of thirteen items, composing the child impact section (first nine items) and the family impact section (last four items). Each item, originally assessed in terms of never = 0 to very often = 5, was dichotomized (0 = not affected, including the original category 0 and 1 = affected, including the original categories 1–5) and dummy variables were summarized into the Child impact- and Family impact scores. The ECOHIS total score was calculated by adding the Child impact and Family impact scores. Participants having two or more items of the ECOHIS unanswered were excluded from the analysis. The response category “I don’t know” were coded as missing and not considered in the analyses. Variables and response categories as originally coded and as re-coded for analyses are shown in Additional file 4: Table S1.
Child-OIDP
Among participants 12–16 years, OHRQoL was measured by interview, using the 8-item Child-OIDP frequency inventory. The OIDP inventory was initially constructed for adults [32] and later modified for children [17]. This index considers difficulty in performing eight daily activities (eating, speaking, cleaning teeth, smiling-laughing-and showing teeth without embarrassment, sleeping and relaxing, emotional balance, social contact, schoolwork) due to problems with mouth or teeth, during the past 3 months. Each of the eight items, originally assessed in terms of never = 0 to every day/almost every day = 3, was dichotomized (0 = not affected, including the original category 0 and 1 = affected, including the original categories 1–3) and the dummy variables were summarized, forming the Child-OIDP simple count (SC) score. The Child OIDP SC score was dichotomized into 0 = no impacts and 1 = 1–8 impacts. Participants with two or more items of the Child-OIDP unanswered were excluded from the analysis. Variables and response categories as originally coded and as re-coded for analyses are shown in Additional file 5: Table S1.
Medical examinations of the participants with JIA
The participants with JIA were examined by experienced pediatric rheumatologists and the included background variables in this sub-study were JIA category according to the ILAR classification criteria [31], age at JIA onset, disease duration, medication, activity/remission status, physician’s global assessment of disease activity visual analogue scale (MDgloVAS) [33], patient/parent-reported pain intensity visual analogue scale (VAS pain) [33], patient/parent-reported global assessment of overall well-being visual analogue scale (PRgloVAS) [33]. All visual analogue scales were measured on a 21-numbered circle VAS (0 = minimal impact, 10 = maximal impact), and reported by the parent if the child were below 9 years, otherwise by the patient. Disability was reported with the Childhood Health Assessment Questionnaire (CHAQ) (0 = no disability, 3 = maximal disability) [34]. The disease-specific clinical background variables are described in detail in Additional file 6 [30] and the coding of these variables is shown in Additional file 7: Table S1.
Oral examination of all participants
The oral assessment was performed by calibrated dentists (n = 5) [30]. For this sub-study, the examination was restricted to caries in the primary second molars in the youngest age group [4–9-year-olds] and in permanent first molars in the oldest age group [10–16-year-olds]. A detailed 5-graded diagnostic tool was applied for decayed lesions, in which grades 1–2 represented enamel lesions and grades 3–5 dentin lesions [35]. Filled surfaces were also reported. Missing teeth were not included in this sub-study as very few teeth (primary teeth: n = 5) were extracted or indicated for extraction due to caries [30]. The caries examination consisted of both visual inspection and bitewing (BW) radiographs. BW was not taken if intermolar contact was lacking, the participants were younger than 5 years or in case of fixed orthodontic appliances when only occlusal surfaces were examined. As a background variable, caries was dichotomized as presence (d1-5f/D1-5F > 0) or absence (d1-5f/D1-5F = 0) of caries.
Statistical methods
SPSS version 25.0 (IBM Corp. Released 2013, IBM SPSS Statistics for Windows, Armonk NY: IBM Corp) and STATA version 16 (Stata Corp LP, College Station, TX) were used for data analysis. Linear weighted Cohen's kappa was used to evaluate inter- and intra-rater reliability for the caries measurements. Mean and standard deviations (SD) were used to describe continuous demographic variables. Categorical variables were compared between individuals with JIA and controls by Cross tabulation and Chi-squared tests. Logistic regression analyses were applied with ECOHIS total score and Child-OIDP SC score as binary outcome measures reporting odds ratio (OR) and 95% confidence interval (CI). Negative binomial regression was implemented as a supplementary analysis with ECOHIS total score and Child-OIDP SC score as count variables reporting incidence rate ratios (IRR) with 95% CI. The multiple variable regression analyses included the main exposure variable, group affiliation, adjusted for covariates in terms of socio-behavioral- and clinical oral health-related variables that were statistically significantly associated with group affiliation and/or the respective OHRQoL outcomes in the unadjusted analysis. The adjusted regression analyses specifically for participants with JIA, included the covariates age, gender and parental educational level, and the JIA-specific variables were adjusted separately. McFadden's R2 was applied as a measure for the goodness of fit of the logistic regression models. The JIA categories, systemic arthritis (n = 7) and undifferentiated arthritis (n = 31) were not included in the statistical analysis. Internal consistency reliability of the OHRQoL inventories was assessed using Cronbach’s alpha. Discriminant validity was assessed by comparing the OHRQoL inventories with global measures of oral health. Two-way interactions were tested between group affiliation and the socio-behavioral- and oral health-related variables on ECOHIS and Child-OIDP. P-values less than 0.05 were considered statistically significant.
Ethical approval
The regional ethics committee (2012/542/REC) approved the study. Approval was also obtained by leaders of different County Dental Health Authorities, at different Oral Health Centre of Expertise, and at the three pediatric departments at the university hospitals. Written informed consent was signed prior to participation. The NorJIA study is registered at ClinicalTrials.gov (No: NCT03904459, 05.04.2019).
Results
Sample characteristics
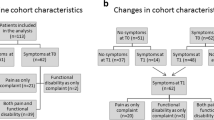
As depicted in Fig. 1, 228 individuals with JIA were submitted to the medical examination, resulting in a response rate of 63.3% (228/360) [30]. Concerning potential non-response bias, the mean age of the 132 eligible individuals with JIA who declined participation was 10.5 (SD = 3.5) years (p < 0.001). The proportion of females was slightly lower amongst the individuals with JIA who declined participation, compared to the participants with JIA (58.3% vs 59.2%, p = 0.027) [30].

Participant flow diagram of children and adolescents with juvenile idiopathic arthritis (JIA) and controls. *Oral health related quality of life (OHRQoL) inventories having two or more unanswered items were excluded from the analysis. ECOHIS = Early Childhood Oral Health Impact Scale, Child-OIDP = Child Oral Impacts on Daily Performance
Four participants with JIA did not undergo the oral examination, hence 224 participants were matched to controls (Fig. 1). The controls’ response rate was 76.2% (224/294) [30]. The matching resulted in 133 (59.4%) females in the JIA group and 134 (59.8%) females in the control group. The mean age for both groups was 12.0 years (both SD = 3.2) (p = 0.974) [30]. According to mother’s background of origin, 94.2% (211/224) of the pairs were matched [30]. As depicted in Fig. 1, 96 individuals with JIA and 98 controls were evaluated according to ECOHIS and 125 individuals with JIA and 124 controls were evaluated according to Child-OIDP.
Table 1 depicts the distribution of socio-demographic-, behavioral and oral health-related characteristics according to group affiliation for all participants aged 4–16 years. Higher proportions of mothers in the control group had high educational level compared to mothers of participants with JIA (73.8% versus 64.3%, p = 0.036). Corresponding figures among fathers were 57.1% vs. 42.5% (p = 0.003). Higher proportions of individuals with than without JIA reported gingival bleeding during toothbrushing (56.9% vs. 46.6%, p = 0.033). Concomitant diagnoses and medication use among the participants that may constitute an oral health threat are presented in a recently published article on dental caries in this study population [30].
Calibration
Four caries calibration exercises (described in Additional file 2) resulted in weighted Cohen’s kappa values of 0.61, 0.61, 0.91, and 0.65, respectively.
Distribution of OHRQoL according to group affiliation
Table 2 depicts the distribution of the single items of ECOHIS and the total ECOHIS scores among the 4–11-year-olds according to group affiliation. Some single items (n = 6) differed significantly between the JIA group and controls with higher proportions of individuals being affected in the JIA group compared to the controls. The family impact score > 0 was also more frequently reported among participants with JIA (45.8% vs. 25.5%, p < 0.05). Internal consistency reliability of the ECOHIS total score in terms of Cronbach’s alpha was 0.87 in participants with JIA and 0.79 in the control group (Table 2).
As shown in Table 3, neither the Child-OIDP SC nor the single item scores differed significantly between adolescents 12–16-years old with and without JIA, although a pattern towards more frequent impacts was observed in the JIA group compared to the controls. Cronbach’s alpha values of the Child-OIDP SC score were 0.83 in the participants with JIA and 0.79 in the control group (Table 3).
Discriminant validity of the OHRQoL measures
Additional file 8: Table S1 shows the frequency distribution of the ECOHIS- and Child-OIDP SC scores according to global measures of oral health, separately in children and adolescents with and without JIA. Among participants with JIA and controls, the ECOHIS scores were higher in parents who rated their child’s oral health as bad/reported dissatisfaction with appearance of teeth, compared to those who perceived their child’s oral health as good/ reported satisfaction with the appearance. The Child-OIDP SC scores were higher among participants reporting dissatisfaction with appearance of teeth, compared to participants reporting satisfaction with appearance of teeth.
OHRQoL by group affiliation adjusted for socio-behavioral and clinical variables
Table 4 shows the results from unadjusted and adjusted ordinary logistic regression analyses of ECOHIS and Child-OIDP according to group affiliation. Increased odds ratios of having ECOHIS > 0 or OIDP > 0 were not statistically significant among participants with JIA in adjusted logistic regression analyses. Adjusted ordinary logistic regression analyses revealed a statistically significant association between d1-5ft/D1-5FT > 0 and ECOHIS total score > 0 (OR = 3.39, 95% CI 1.40–8.22). Reporting pain or discomfort occurring during toothbrushing increased the likelihood of having Child-OIDP SC score > 0 (OR = 7.76, 95% CI 3.09–19.50). Adolescents with mothers reporting low educational level had significantly lower odds ratio for oral impacts according to Child-OIDP SC score (OR = 0.32, 95% CI 0.13–0.82). Corresponding to Table 4, negative binomial regression revealed almost similar results (Additional file 9: Table S1). However, adjusted negative binomial regressions showed a statistically significant increased incidence rate ratio of negatively impacted ECOHIS among participants with JIA compared to controls (IRR = 1.61, 95% CI 1.16–2.23) (Additional file 9).
A significant two-way interaction between group affiliation and gender on Child-OIDP SC score was revealed by logistic regression (p = 0.015). Stratified analyses revealed that females had higher odds ratio for having Child-OIPD SC score > 0 compared to males, among participants with JIA (OR = 6.12, 95% CI 2.29–16.30, p < 0.001) (not presented in any table). Amongst the controls, females had higher odds ratio for having Child-OIPD SC > 0 compared to males (OR = 1.23, 95% CI 0.52–2.90), although not statistically significant (not presented in any table).
Disease-specific features in relation to OHRQoL
Table 5 shows the results from adjusted ordinary logistic regression analyses of disease-specific features in relation to ECOHIS and Child-OIDP among children and adolescents with JIA. Covariates were age, gender and parental educational level, and the JIA-specific variables were adjusted separately. Children with ongoing or ever used biologic DMARDs (disease-modifying antirheumatic drugs) were more likely than their counterparts without ongoing or ever used biologic DMARDs to have ECOHIS > 0 (OR = 7.59, 95% CI 1.77–32.67, p = 0.006 and OR = 9.20, 95% CI 1.93–43.97, p = 0.005). Adolescents categorized ‘not oligoarthritis persistent’ (comprising oligoarthritis extended, polyarthritis RF positive and RF negative, psoriatic arthritis, and enthesitis-related arthritis) had statistically significantly increased odd ratio of having Child-OIDP SC > 0, compared to participants in the JIA category oligoarthrits persistent (OR = 6.29, 95% CI 1.83–21.63). Adolescents with continued activity or flare revealed statistically significantly increased odds ratio of having Child-OIDP SC > 0, compared to participants with inactive disease or remission (OR = 3.01, 95% CI 1.15–7.89). This also applied to the self-reported pain (VAS pain > 0), compared to no pain (VAS pain = 0), and self-reported physical disability (CHAQ > 0), compared to no disability (CHAQ = 0) (OR = 4.39, 95% CI 1.20–16.14, OR = 4.21, 95% CI 1.40–12.68, respectively). Corresponding to Table 5, negative binomial regression revealed almost similar results (Additional file 10: Table S1).
Discussion
To our knowledge, this is one of the first studies to estimate the proportion and socio-, behavioral and clinical covariates of OHRQoL in young people with and without JIA. Present findings based on multiple variable logistic regression analysis did not confirm the hypothesis that children and adolescents with JIA have poorer OHRQoL than their counterparts without JIA. According to the ECOHIS scores this conclusion is unsure, since the adjusted binominal regression analyses showed an increased risk of impaired ECOHIS scores amongst the 4–11-year-olds with JIA compared to controls. Although the proportions who confirmed impacts according to ECOHIS and Child- OIDP scores were substantial across both groups, and always tended to be higher among children and adolescents with than without JIA, neither scale scores varied by group affiliation in the adjusted logistic regression analyses. Independent of JIA status, the likelihood of impaired OHRQoL increased by caries experience among the younger participants. Among the older participants, Child OIDP associated negatively and positively with maternal education and having pain/discomfort during toothbrushing, respectively. Although the socio-behavioral and clinical distribution of OHRQoL scores were less variant across the two groups of participants, female adolescents with JIA were more likely than males to report oral impacts according to Child OIDP. The corresponding association in the control group was not significant. Specifically, for adolescents with JIA, continued activity or flare was found to adversely affect Child-OIDP, indicating that sub-groups of JIA may have reduced OHRQoL, Also, self-reported outcome measures of the disease (VAS pain and CHAQ) associated with Child-OIDP.
Important strengths of the study were that the study group of individuals with JIA was relatively large and might be representative of the Norwegian population of children and adolescents with JIA. Also, a well-matched control group and the adjustment of various socio-demographic, behavioral, and clinical covariates strengthened the results [27, 36]. The present study revealed that both ECOHIS and Child-OIDP discriminated significantly according to global measures of oral health indicating satisfactory psychometrical properties of both instruments across the investigated groups. Other strengths were the meticulous calibration of caries examiners before and during the study and the use of the previous validated OHRQoL instruments in the context of Norwegian children and adolescents, which also showed a satisfactory internal consistency reliability [19]. Among limitations to be considered were a potential non-response bias among the participants with JIA [37] and the small subgroups of JIA disease categories that might have prevented valid interpretation of the relation between various disease categories and OHRQoL. Furthermore, considering the multilevel influences of oral health, other potential confounding variables of OHRQoL have not been adjusted for in the present study [38]. As a sub-study, the sample size calculation in the present article was based in caries figures and not on OHRQoL. This questions the study's statistical power and needs to be kept in mind while interpreting the results. Finally, evaluation of OHRQoL among the youngest study participants were only conducted by parental proxy-reporting and may reduce the quality of data collected. Thus, evidence suggests that parents tend to underestimate the impact of children’s oral problems as their perspective is different and they might have limited knowledge of their children’s social and emotional well-being [39].
Some descriptive studies have been conducted in European countries evaluating OHRQoL by the application of ECOHIS [19, 40,41,42,43]. Except for one study conducted in Norway by Skeie et al. [19], all of these studies evaluated OHRQoL in preschool children below the age of 6 years, hence complicating direct comparisons with the present study. Whereas the proportion of ECOHIS child impacts in this study amounted to 77.1% in the JIA group and 65.3% among controls, the corresponding figure among children in the study by Skeie et al. [19] was 71.0%. In contrast, the proportions of adolescents with and without JIA having impacts according to the Child-OIDP in the present study were 26.4% and 21.8%, a higher rate of 42.7% was found among adolescents in the study by Skeie et al. [19]. These differences in children’s and adolescents’ impact proportions might be attributed to minor age differences in the study groups investigated (also 17- and 18-year-olds were included in the study by Skeie et al.). The subjective and dynamic aspects of OHRQoL is based on individual experiences values and perceptions [44]. Thus, OHRQoL varies across groups within and across countries, as well as over time [44]. Nevertheless, many studies using Child-OIDP have been published [45,46,47]. A recent systematic review on OHRQoL in adolescents measured by use of Child-OIDP worldwide, reported prevalence rates of impacts within a wide range among adolescents 12 years and older, 15.8%-87% respectively [47].
Few studies have compared sub-scale OHRQoL scores with healthy controls. As shown in Table 2 physical- and psychosocial aspects of the Child impact scores and ‘taken time off from work’ from the family impact sub-scale were the most frequently reported impacts in both groups of younger children investigated. However, the prevalence of child impacts were consistently higher in the JIA group than among the controls, particularly regarding impacts related to physical and psycho-social functioning. Also, according to Table 3, the number of adolescents reporting impacts on the single OIDP items tended to be higher among participants with JIA, compared to controls. Physical aspects in terms of difficulty eating was most frequent among the 8 single OIDP scores. Impact of the function “eating” has also been demonstrated to be related to TMJ arthritis [23]. Although neither scale scores varied by group affiliation in the adjusted logistic regression analyses, children and adolescents with JIA seems to carry a particular burden regarding physical and psycho-social functioning. This is consistent with previous evidence that rheumatic diseases may result in important functional and psycho-social impairments, though examined among adult populations [48].
The present results showed that neither the ECOHIS- nor the Child OIDP scores varied by group affiliation in adjusted logistic regression analyses. This supports the findings of Santos et al. [22], who observed no significant difference in OHRQoL scores between individuals with JIA and controls, as perceived by their caregivers. However, comparisons with other studies are problematic as various OHRQoL instruments have been utilized, adjustment for covariates is seldom implemented and participants in the relevant studies are categorized specifically according to oral health status (e.g., JIA + TMJ arthritis, JIA + periodontitis) [22,23,24,25]. A plausible contributing factor of comparable OHRQoL between participants with JIA and controls is improved therapeutic effect, especially increased efficacy of pharmaceutical drugs, in the management of JIA [49, 50].
Independent of group affiliation, caries experience associated significantly with impaired OHRQOL amongst 4–11-year-olds in the present study. This corresponds with previous studies conducted across cultural contexts [51, 52]. The ECOHIS scale was originally developed to assess the impact of dental caries but have been widely used as generic OHRQoL instrument [45]. A systematic review by Kumar et al. [36] found that higher parental education associated with better OHRQoL in children. Contrary, we found that adolescents having lower educated mothers were less likely than their counterparts with higher educated mothers to report oral impacts according to Child OIDP. However, research findings in this area are conflicting and some studies have documented insignificant associations between parental socio-economic status and children’s OHRQoL [36, 51].
Female adolescents with JIA were significantly more likely than male adolescents to report oral impacts according to Child-OIDP; the corresponding association in the control group was nonsignificant. Other studies reporting poorer OHRQoL among female participants compared to males, by the employment of Child-OIDP, consider females more sensitive to problems and appearance than males [53, 54]. Even in the biological era, pain and depressive symptoms, known to impact the quality of life, are common in JIA patients [55,56,57]. Comparable to findings in the general pediatric population, research focusing on young individuals with JIA indicates, although inconsistently, a gender difference; females report such complaints more frequently than males, and the complaints become apparent in their adolescent years [58,59,60,61,62,63]. This may provide an explanation for female adolescents with JIA reporting poorer OHRQoL in this study.
Several JIA-specific covariates related to disease activity and patient/parent-reported pain, and functional disability were associated with Child-OIDP in the present study. OHRQoL is recognized to be part of health-related quality of life [64, 65], hence the association between patient/parent-reported covariates and OHRQoL was anticipated. In the present study biologic DMARDs, ongoing or ever used, were shown to be associated with impaired ECOHIS scores amongst the younger population with JIA. Thus, a more severe disease course as indicated by biologic DMARDs ongoing or ever used, is suggested to be associated with OHRQoL. No disease-specific inventory exists to evaluate OHRQoL in individuals with JIA. Accordingly, various impacts of JIA-specific features on OHRQoL are not necessarily identified by the generic instruments utilized in this study.
Conclusions
This study did not provide consistent evidence to confirm the hypothesis that children and adolescents with JIA are more likely to have impaired OHRQoL compared to their peers without JIA. However, female adolescents with JIA were more likely than males to report impacts on OHRQoL. Furthermore, within the JIA group, adolescents with continued disease activity, flare or reporting pain, or physical disability, had higher risk than their counterparts of impaired OHRQoL.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Notes
The Norwegian JIA Study – Temporo-mandibular Involvement, Oral Health, Uveitis, Bone Health and Quality of Life in Children with Juvenile Idiopathic Arthritis (JIA).
Abbreviations
- bDMARDs:
-
Biologic disease-modifying antirheumatic drugs
- CHAQ:
-
Childhood Health Assessment Questionnaire
- Child-OIDP:
-
Child Oral Impacts on Daily Performances
- COHQoL:
-
Child Oral Health-related Quality of Life measure
- CPQ11-14 :
-
Child Perception Questionnaire
- DMARDs:
-
Disease-modifying antirheumatic drugs
- BW:
-
Bitewing radiographs
- CHAQ:
-
Childhood Health Assessment Questionnaire
- CI:
-
Confidence interval
- dfs/DFS:
-
Decayed and filled surfaces
- ECOHIS:
-
Early Childhood Oral Health Impact Scale
- ILAR:
-
International League of Associations for Rheumatology
- IRR:
-
Incidence rate ratios
- JIA:
-
Juvenile idiopathic arthritis
- MDgloVAS:
-
Physician’s global assessment of disease activity visual analogue scale
- NorJIA:
-
The Norwegian JIA Study (Temporo-mandibular Involvement, Oral Health, Uveitis, Bone Health and Quality of Life in Children with Juvenile Idiopathic Arthritis)
- OHRQoL:
-
Oral health-related quality of life
- OR:
-
Odds ratios
- PRgloVAS:
-
Patient/parent-reported global assessment of overall wellbeing visual analogue scale
- RF:
-
Rheumatoid Factor
- SC:
-
Simple count
- SD:
-
Standard deviations
- sDMARDs:
-
Synthetic disease-modifying antirheumatic drugs
- TMD:
-
Temporomandibular disorder
- TMJ:
-
Temporomandibular joint
- VAS:
-
Visual analogue scale
- VAS pain:
-
Patient/parent-reported pain intensity visual analogue scale
References
Ravelli A, Martini A. Juvenile idiopathic arthritis. Lancet. 2007;369(9563):767–78.
Oliveira S, Ravelli A, Pistorio A, Castell E, Malattia C, Prieur AM, et al. Proxy-reported health-related quality of life of patients with juvenile idiopathic arthritis: the Pediatric Rheumatology International Trials Organization multinational quality of life cohort study. Arthritis Rheum. 2007;57(1):35–43.
Thierry S, Fautrel B, Lemelle I, Guillemin F. Prevalence and incidence of juvenile idiopathic arthritis: a systematic review. Jt Bone Spine. 2014;81(2):112–7.
Ravelli A, Consolaro A, Horneff G, Laxer RM, Lovell DJ, Wulffraat NM, et al. Treating juvenile idiopathic arthritis to target: recommendations of an international task force. Ann Rheum Dis. 2018;77(6):819–28.
Mays JW, Sarmadi M, Moutsopoulos NM. Oral manifestations of systemic autoimmune and inflammatory diseases: diagnosis and clinical management. J Evid Based Dent Pract. 2012;12(3 Suppl):265–82.
Walton AG, Welbury RR, Thomason JM, Foster HE. Oral health and juvenile idiopathic arthritis: a review. Rheumatology (Oxford). 2000;39(5):550–5.
Synodinos PN, Polyzois I. Oral health and orthodontic considerations in children with juvenile idiopathic arthritis: review of the literature and report of a case. J Ir Dent Assoc. 2008;54(1):29–36.
Skeie MS, Gil EG, Cetrelli L, Rosen A, Fischer J, Astrom AN, et al. Oral health in children and adolescents with juvenile idiopathic arthritis—a systematic review and meta-analysis. BMC Oral Health. 2019;19(1):285.
Glick M, Monteiro da Silva O, Seeberger GK, Xu T, Pucca G, Williams DM, et al. FDI Vision 2020: shaping the future of oral health. Int Dent J. 2012;62(6):278–91.
Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. J Am Dent Assoc. 2016;147(12):915–7.
Constitution [Internet]. Constitution of the World Health Organization [cited 22 Nov 2021]. https://www.who.int/about/governance/constitution.
McGrath C, Rogers SN. Overview of instruments used to assess quality of life in dentistry. In: Preedy VR, Watson RR, editors. Handbook of disease burdens and quality of life measures. New York, NY: Springer; 2010. p. 145–59.
Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. 2011;90(11):1264–70.
Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G. Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J Dent Res. 2002;81(7):459–63.
Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G. Measuring parental perceptions of child oral health-related quality of life. J Public Health Dent. 2003;63(2):67–72.
Locker D, Jokovic A, Stephens M, Kenny D, Tompson B, Guyatt G. Family impact of child oral and oro-facial conditions. Community Dent Oral Epidemiol. 2002;30(6):438–48.
Gherunpong S, Tsakos G, Sheiham A. Developing and evaluating an oral health-related quality of life index for children; the CHILD-OIDP. Community Dent Health. 2004;21(2):161–9.
Pahel BT, Rozier RG, Slade GD. Parental perceptions of children’s oral health: the Early Childhood Oral Health Impact Scale (ECOHIS). Health Qual Life Outcomes. 2007;5:6.
Skeie MS, Skaare AB, Sande M, Sirevåg LJ, Åstrøm AN. Oral helserelatert livskvalitet blant barn og ungdom. Gyldighet og måleegenskaper av to instrumenter i norsk versjon. Nor Tannlaegeforen Tid. 2017;127:592–8.
Birungi N, Fadnes LT, Engebretsen IMS, Lie SA, Tumwine JK, Astrom AN, et al. Caries experience and oral health related quality of life in a cohort of Ugandan HIV-1 exposed uninfected children compared with a matched cohort of HIV unexposed uninfected children. BMC Public Health. 2020;20(1):423.
Aljameel AH. Oral Health-related quality of life outcomes for individuals with disabilities: a review. J Clin Diagn Res. 2020;14(10):1–6.
Santos D, Silva C, Silva M. Oral health and quality of life of children and adolescents with juvenile idiopathic arthritis according to their caregivers’ perceptions. Spec Care Dentist. 2015;35(6):272–8.
Isola G, Perillo L, Migliorati M, Matarese M, Dalessandri D, Grassia V, et al. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur J Orthodont. 2019;41(2):117–24.
Bucci R, Rongo R, Amato A, Martina S, D’Anto V, Valletta R. The Psychological impact of dental aesthetics in patients with juvenile idiopathic arthritis compared with healthy peers: a cross-sectional study. Dent J-Basel. 2019;7(4):98.
Polizzi A, Santonocito S, Di Stefano M, Ferlito S, Indelicato F, Palazzo G. The effects on Oral Related Quality of Life induced by periodontitis in patients with juvenile idiopathic arthritis. Mediterr J Clin Psychol. 2020;8(1):2282–1619.
Rahimi H, Twilt M, Herlin T, Spiegel L, Pedersen TK, Kuseler A, et al. Orofacial symptoms and oral health-related quality of life in juvenile idiopathic arthritis: a two-year prospective observational study. Pediatr Rheumatol Online J. 2018;16(1):47.
Moghaddam LF, Vettore MV, Bayani A, Bayat AH, Ahounbar E, Hemmat M, et al. The Association of Oral Health Status, demographic characteristics and socioeconomic determinants with oral health-related quality of life among children: a systematic review and meta-analysis. BMC Pediatr. 2020;20(1):1–15.
Knorst JK, Sfreddo CS, de F. Meira G, Zanatta FB, Vettore MV, Ardenghi TM. Socioeconomic status and oral health-related quality of life: a systematic review and meta-analysis. Community Dent Oral Epidemiol. 2021;49(2):95–102.
Barbosa TS, Gaviao MB. Oral health-related quality of life in children: part II. Effects of clinical oral health status. A systematic review. Int J Dent Hyg. 2008;6(2):100–7.
Gil EG, Astrom AN, Lie SA, Rygg M, Fischer J, Rosen A, et al. Dental caries in children and adolescents with juvenile idiopathic arthritis and controls: a multilevel analysis. BMC Oral Health. 2021;21(1):417.
Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–2.
Adulyanon S, Sheiham A. Oral impact on daily performance. In: Slade GD, editor. Measuring oral health and quality of life. Chapel Hill: University of North Carolina; 1997. p. 151–60.
Filocamo G, Davi S, Pistorio A, Bertamino M, Ruperto N, Lattanzi B, et al. Evaluation of 21-numbered circle and 10-centimeter horizontal line visual analog scales for physician and parent subjective ratings in juvenile idiopathic arthritis. J Rheumatol. 2010;37(7):1534–41.
Ruperto N, Ravelli A, Pistorio A, Malattia C, Cavuto S, Gado-West L, et al. Cross-cultural adaptation and psychometric evaluation of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ) in 32 countries. Review of the general methodology. Clin Exp Rheumatol. 2001;19(4 Suppl 23):S1-9.
Amarante E, Raadal M, Espelid I. Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol. 1998;26(2):87–94.
Kumar S, Kroon J, Lalloo R. A systematic review of the impact of parental socio-economic status and home environment characteristics on children’s oral health related quality of life. Health Qual Life Outcomes. 2014;12:41.
Locker D. Response and nonresponse bias in oral health surveys. J Public Health Dent. 2000;60(2):72–81.
Fisher-Owens SA, Gansky SA, Platt LJ, Weintraub JA, Soobader MJ, Bramlett MD, et al. Influences on children’s oral health: a conceptual model. Pediatrics. 2007;120(3):e510–20.
Barbosa TS, Gaviao MB. Oral health-related quality of life in children: part III. Is there agreement between parents in rating their children’s oral health-related quality of life? A systematic review. Int J Dent Hyg. 2008;6(2):108–13.
Bekes K, Omara M, Safar S, Stamm T. The German version of Early Childhood Oral Health Impact Scale (ECOHIS-G): translation, reliability, and validity. Clin Oral Investig. 2019;23(12):4449–54.
Jankauskiene B, Narbutaite J, Kubilius R, Gleiznys A. Adaptation and validation of the early childhood oral health impact scale in Lithuania. Stomatologija. 2012;14(4):108–13.
Taoufik K, Divaris K, Kavvadia K, Koletsi-Kounari H, Polychronopoulou A. Development and Validation of the greek version of the Early Childhood Oral Health Impact Scale (ECOHIS). Open Dent J. 2020;14:88–96.
Contaldo M, della Vella F, Raimondo E, Minervini G, Buljubasic M, Ogodescu A, et al. Early Childhood Oral Health Impact Scale (ECOHIS): literature review and Italian validation. Int J Dent Hyg. 2020;18(4):396–402.
Ingelhart MR, Bagramian R. Oral health related quality of life. Chichago: University of North Carolina, School of Dentistry, Quintessence Publishing Co Inc; 2002.
Zaror C, Pardo Y, Espinoza-Espinoza G, Pont A, Munoz-Millan P, Martinez-Zapata MJ, et al. Assessing oral health-related quality of life in children and adolescents: a systematic review and standardized comparison of available instruments. Clin Oral Investig. 2019;23(1):65–79.
Pentapati KC, Yeturu SK, Siddiq H. A reliability generalization meta-analysis of Child Oral Impacts on Daily Performances (C-OIDP) questionnaire. J Oral Biol Craniofac Res. 2020;10(4):776–81.
Alvarez-Azaustre MP, Greco R, Llena C. Oral health-related quality of life in adolescents as measured with the child-OIDP questionnaire: a systematic review. Int J Environ Res Public Health. 2021;18(24):12995.
Schmalz G, Patschan S, Patschan D, Ziebolz D. Oral-health-related quality of life in adult patients with rheumatic diseases—-a systematic review. J Clin Med. 2020;9(4):1172.
Giancane G, Muratore V, Marzetti V, Quilis N, Benavente BS, Bagnasco F, et al. Disease activity and damage in juvenile idiopathic arthritis: methotrexate era versus biologic era. Arthritis Res Ther. 2019;21(1):168.
Ruperto N, Martini A. Current and future perspectives in the management of juvenile idiopathic arthritis. Lancet Child Adolesc Health. 2018;2(5):360–70.
Chaffee BW, Rodrigues PH, Kramer PF, Vitolo MR, Feldens CA. Oral health-related quality-of-life scores differ by socioeconomic status and caries experience. Community Dent Oral Epidemiol. 2017;45(3):216–24.
Bittencourt JM, Martins LP, Paiva SM, Pordeus IA, Martins-Junior PA, Bendo CB. Early childhood caries and oral health-related quality of life of Brazilian children: does parents’ resilience act as moderator? Int J Paediatr Dent. 2021;31(3):383–93.
Bianco A, Fortunato L, Nobile CGA, Pavia M. Prevalence and determinants of oral impacts on daily performance: results from a survey among school children in Italy. Eur J Pub Health. 2009;20(5):595–600.
Pavithran V, Murali R, Krishna M, Shamala A, Yalamalli M, Kumar A, et al. Impact of oral diseases on daily activities among 12- to 15-year-old institutionalized orphan and non-orphan children in Bengaluru city: a cross-sectional analytical study. Indian J Dent Res. 2020;31(3):396–402.
Fair DC, Rodriguez M, Knight AM, Rubinstein TB. Depression And anxiety in patients with juvenile idiopathic arthritis: current insights and impact on quality of life, a systematic review. Open Access Rheumatology. 2019;11:237–52.
Arnstad ED, Rypdal V, Peltoniemi S, Herlin T, Berntson L, Fasth A, et al. Early self-reported pain in juvenile idiopathic arthritis as related to long-term outcomes: results from the Nordic Juvenile Idiopathic Arthritis Cohort Study. Arthritis Care Res (Hoboken). 2019;71(7):961–9.
Anink J, Prince FHM, Dijkstra M, Otten MH, Twilt M, ten Cate R, et al. Long-term quality of life and functional outcome of patients with juvenile idiopathic arthritis in the biologic era: a longitudinal follow-up study in the Dutch Arthritis and Biologicals in Children Register. Rheumatology. 2015;54(11):1964–9.
Nolen-Hoeksema S, Girgus JS. The emergence of gender differences in depression during adolescence. Psychol Bull. 1994;115(3):424–43.
Boerner KE, Keogh E. 127The effect of sex and gender on child and adolescent pain. In: Stevens BJ, Hathway G, Zempsky WT, Stevens BJ, Hathway G, Zempsky WT, editors. Oxford textbook of pediatric pain. Oxford: Oxford University Press; 2021.
Stinson JN, Luca NJ, Jibb LA. Assessment and management of pain in juvenile idiopathic arthritis. Pain Res Manag. 2012;17(6):391–6.
Beales JG, Keen JH, Holt PJ. The child’s perception of the disease and the experience of pain in juvenile chronic arthritis. J Rheumatol. 1983;10(1):61–5.
Giancane G, Alongi A, Rosina S, Calandra S, Consolaro A, Ravelli A. Open issues in the assessment and management of pain in juvenile idiopathic arthritis. Clin Exp Rheumatol. 2017;35(Suppl 107(5)):123–6.
Hanns L, Cordingley L, Galloway J, Norton S, Carvalho LA, Christie D, et al. Depressive symptoms, pain and disability for adolescent patients with juvenile idiopathic arthritis: results from the Childhood Arthritis Prospective Study. Rheumatology (Oxford). 2018;57(8):1381–9.
Zimmer S, Bergmann N, Gabrun E, Barthel C, Raab W, Ruffer JU. Association between oral health-related and general health-related quality of life in subjects attending dental offices in Germany. J Public Health Dent. 2010;70(2):167–70.
Sekulic S, John MT, Davey C, Rener-Sitar K. Association between oral health-related and health-related quality of life. Zdrav Varst. 2020;59(2):65–74.
Wallace CA, Ruperto N, Giannini E, Childhood Arthritis and Rheumatology Research Alliance, Pediatric Rheumatology International Trials Organization and Pediatric Rheumatology Collaborative Study Group, et al. Preliminary criteria for clinical remission for select categories of juvenile idiopathic arthritis. J Rheumatol. 2004;31(11):2290–4.
Wallace CA, Giannini EH, Huang B, Itert L, Ruperto N, Childhood Arthritis Rheumatology Research Alliance (CARRA),Pediatric Rheumatology Collaborative Study Group (PRCSG),Paediatric Rheumatology International Trials Organisation (PRINTO), et al. American College of Rheumatology provisional criteria for defining clinical inactive disease in select categories of juvenile idiopathic arthritis. Arthritis Care Res (Hoboken). 2011;63(7):929–36.
Acknowledgements
This study is part of the multicenter NorJIA Study (The Norwegian JIA Study – Temporo-mandibular Involvement, Oral Health, Uveitis, Bone Health and Quality of Life in Children with Juvenile Idiopathic Arthritis (JIA)). NorJIA is a collaboration among universities (University of Bergen, Norwegian University of Science and Technology, The Arctic University of Norway), university hospitals (Haukeland University Hospital, St. Olav’s Hospital, University Hospital of North Norway) and oral health centers (Oral Health Centre of Expertise in Western Norway-Vestland, Center for Oral health Services and Research, Trondheim, Public Dental Health Service Competence Centre of Northern Norway) in Bergen, Trondheim and Tromsø. Represented by Karen Rosendahl MD PhD (PI), Marit Slåttelid Skeie DDS PhD, Marite Rygg MD PhD, Ellen Nordal MD PhD, Anne N. Åstrøm DDS PhD, Karin Tylleskär MD, Annika Rosén DDS PhD, Elisabeth Grut Gil DDS, Johannes Maria Fischer DDS, Xieqi Shi DDS PhD, Oskar Angenete MD, Lena Cetrelli DDS, Gunnar Lyngstad DDS, Marie Sager DDS, Astrid J Feuerheim PhD, Anette Lundestad MD, Thomas Augdal MD, Paula Frid DDS, Veronika Rypdal MD, Josefine Halbig DDS, Athanasia Bletsa DDS PhD, Marit Midtbø DDS PhD, Larissa von Wangenheim Marti DDS, Mats Säll DDS and Keijo Luukko DDS PhD. We are indebted to radiographers Marianne Lothe Vollan and Erik Haro, and the study nurses Tone Kvinnsland Amdal, Susanne Irene Tobiesen Eidset, Line Rapp Simonsen, Marte Grimsmo Teige, Brita Lena Hansen, and Lisbeth Aune. Finally, we are thankful to all the children and their caregivers who participated in the study.
Funding
Open access funding provided by University of Bergen. The current study is supported by universities (University of Bergen, Norwegian University of Science and Technology, The Arctic University of Norway), university hospitals (Haukeland University Hospital, St. Olav’s Hospital, University Hospital of North Norway) and oral health centers (Oral Health Centre of Expertise in Western Norway-Vestland, Center for Oral health Services and Research, Trondheim, Public Dental Health Service Competence Centre of Northern Norway) in Bergen, Trondheim and Tromsø, and “Norsk Revmatikerforbund” (Norway) as part of the data collection. First author’s PhD program are financed by University of Bergen. The reported funding’s did not play a role in in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
EGG: Contributed to the design and data collection of this sub-study, performed statistical analysis, and wrote the manuscript in consultation with ANÅ, MSS and SAL. ANÅ and MSS: Conceived and designed this sub-study. SAL: Performed statistical analysis. MR: Aided in interpretation and writing of the manuscript and to the design and data collection of the NorJIA study. JF, JH, PF, KT, KR: Contributed to data collection and provided valuable comments. BJ, AR, AB, KL, XS, LC: Provided valuable comments. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Regional Committees for Medical and Health Research Ethics (2012/542/REC), Rogaland, Vestland (West). Written informed consents were obtained from the caregivers and the adolescents as appropriate. The study was registered at ClinicalTrials.gov (No: NCT03904459, 05.04.2019). All procedures were performed in accordance with relevant guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Sample size calculation.
Additional file 2.
Calibration.
Additional file 3.
Table S1. Categories for socio-behavioral characteristics, as originally coded and as re-coded for analyses.
Additional file 4.
Table S1. Categories for Early Childhood Oral Health Impact Scale (ECOHIS) (4–11 years) and questions regarding satisfaction with oral health (global measures), as originally coded and as re-coded for analyses.
Additional file 5.
Table S1. Categories for Child Oral Impacts on Daily Performances (Child-OIDP) (12–16 years) and questions regarding satisfaction with oral health (global measures), as originally coded and as re-coded for analyses.
Additional file 6.
Description of JIA-specific background variables.
Additional file 7.
Table S1. Categories for JIA-specific background variables, as originally coded and re-coded for analyses.
Additional file 8.
Table S1. Discriminant validity of the Early Childhood Oral Health Impact Scale (ECOHIS) and Child Oral Impacts on Daily Performances (Child-OIDP) according to the global measures and group affiliation.
Additional file 9.
Table S1. Group affiliation, socio-behavioral, and clinical characteristics in relation to the outcome variable Early Childhood Oral Health Impact Scale (ECOHIS) total score and Child Oral Impacts on Daily Performance (Child-OIDP) simple count (SC) score. Unadjusted and adjusted negative binominal regressions.
Additional file 10.
Table S1. Disease-specific features and dental caries in relation to the outcome variable Early Childhood Oral Health Impact Scale (ECOHIS) total score and Child Oral Impacts on Daily Performance (Child-OIDP) simple count (SC) score. Unadjusted and adjusted negative binominal regressions.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gil, E.G., Skeie, M.S., Halbig, J. et al. Oral health-related quality of life in 4–16-year-olds with and without juvenile idiopathic arthritis. BMC Oral Health 22, 387 (2022). https://doi.org/10.1186/s12903-022-02400-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-022-02400-1