
Abstract
Background
This systematic review and meta-analysis aimed to investigate the role of alendronate combined with step 2 of periodontal therapy in reducing probing pocket depth, improving clinical attachment level, and reducing bone defect depth in intra-bony and inter-radicular defects.
Methods
RCTs with more than 6 months follow-up were included in this study. Risk of bias assessment was performed using the Cochrane collaboration tool. In addition, meta-analysis and trial sequential analysis were used to aggregate the available evidence.
Results
Seven studies met the inclusion criteria and were included in the systematic review. Topical application of alendronate during second step of periodontal therapy significantly improved PD and CAL.
Conclusion
Local application of alendronate may confer a beneficial effect when applied during step II of periodontal therapy even if long term studies are needed to confirm these results.
Clinical relevance
Considering the emerging role of host-inflammatory response in treatment of periodontitis and the antiresorptive and osteostimulative properties of bisphosphonates, several studies are focusing on the role of alendronate as an addition to non-surgical periodontal therapy.
Similar content being viewed by others


Background
Periodontitis is an inflammatory disease affecting tissues surrounding teeth, characterized by destruction of connective tissue attachment and alveolar bone [1]. It is mainly caused by the bacterial biofilm which is responsible for the inflammatory and immunologic reaction that leads to the loss of connective tissue attachment and alveolar bone [2]. Therefore, second step of periodontal therapy is considered crucial to remove the bacterial biofilm both in its soft and calculus form in order to reestablish periodontal health in all patients with loss of periodontal support and/or periodontal pocket formation [3]. This is usually followed by home care measures and in the end by surgery. But while the complete disintegration of the bacterial biofilm can lead to the removal of the cause of the inflammation, several studies demonstrated the role of host inflammatory response in the breakdown of connective tissue and bone and therefore for disease progression [4]. Recent studies explored the use of host-modulators to reduce periodontal disease by altering the inflammatory response [5]. Bisphosphonates (BPs) are carbon-substituted pyrophosphate analogs that bind the mineral component of the bone interfering with the action of osteoclasts [6]. They find application in post-menopausal women for prevention and treatment of osteoporosis [7], in bone related diseases like Paget’s disease and hypercalcemia of malignancy [8]. Some studies showed that BPs induced osteoclasts to secrete inhibitors of osteoclast mediated resorption and stimulated the formation of osteoblast precursors and mineralized nodules, thus promoting bone formation [8, 9]. The role of BPs in treatment of periodontitis has been analyzed in an animal study in order to detect its potential role in retarding bone loss around teeth affected by periodontitis [10]. BPs showed a potential role against bone loss when systemically administered; moreover local adjunct to scaling and root-planning (SRP) caused a decreasing in bone loss and improving mineral density [11]. However, among different BPs, local administration of high doses of alendronate in periodontal pockets, could stimulate the release of IL-1 and IL-6 thus increasing host inflammatory response [12, 13]. Alendronate is an amino bisphosphonate commonly used as a potent inhibitor of bone resorption. However, to be effective, it needs to be administered in high dosage to maintain the necessary concentration of the drug at the osseous defect and systemic administration of BPs can cause several side effects to the gastro-intestinal tract, renal failure and severe hypocalcemia [14]. For these reasons local application might be more successful in controlling local concentration and reducing toxicities. Previous studies demonstrated its role in decreasing bone loss and increasing the bone density of alveolar bone [6]. The aim of this study was to systematically review the role of local 1% alendronate gel in non-surgical therapy of intra-bony and inter-radicular defects.
Methods
Protocol, registration and focused question
A systematic review protocol was written in the planning stages and both the Cochrane Handbook and the PRISMA (“Preferred Reporting Items for Systematic Reviews and Meta-Analyses”) statement were followed for the planning and reporting of the review. In addition, the protocol of this systematic review was registered on the PROSPERO database (registration code: CRD42021223883).
This review was performed aiming to answer the following PICO question: “Do intra-bony and inter-radicular defects (Participants) heal better with the adjunct of 1% alendronate (Intervention) to SRP instead of placebo (Comparison) in terms of PD, CAL and bone defect depth (Outcomes)?
Inclusion and exclusion criteria
Only studies fulfilling the following inclusion criteria were considered eligible for inclusion in this review: (1) Type of studies: Randomized controlled trials with a follow-up of at least 6 months. A shorter follow up was not considered as it would be unlike to reflect a meaningful difference in treatment response between test and control; (2) Types of participants: Adults (> = 18 years old), systematically healthy individuals diagnosed with periodontitis; (3) Types of intervention: Studies evaluating the adjunctive use of alendronate 1% gel administered locally during step 2 of periodontal therapy in intra-bony and inter-radicular defects; Comparison: patients receiving placebo or none adjunct treatment during step II of periodontal therapy; (4) Outcomes: Primary outcome: reduction in PD, CAL gain and bone defect depth. Hence, the following exclusion criteria were considered: (1) Non RCT or RCTs with a follow up < 6 months were excluded; (2) Studies involving less than 20 sites per group; (3) studies including participants with systemic diseases or that were taking medications were excluded.
Information sources and search strategy
Studies were identified through an online search on PubMed, Scopus, and Web of Science. The search strategy included terms related to the population and the intervention. A combination of MESH terms and Free Text words combined with Boolean operators; for example in PubMed the following string was used: (((‘bisphosphonate’ OR ‘BP’ OR ‘alendronate’ OR ‘alendronate gel’) AND (‘osseous defects’ OR ‘intrabony defects’ OR ‘infrabony defects’ OR ‘furcation defects’ OR ‘furcation’ OR ‘periodontitis’))). A manual search was performed through several scientific journals, namely: Journal of Dental Research, Journal of Clinical Periodontology, Journal of Periodontology, International Journal of Periodontics and Restorative Dentistry, Journal of Oral and Maxillofacial Surgery. The bibliographies of pertinent review articles and studies finally included for data extraction were also screened.
Study selection and data collection process
Eligibility of studies was assessed by two independent authors in a standardized manner (CA, VCAC). In the first round, records were screened by only reading title and abstract of publications. The studies assessed as eligible were included in the second round and underwent full-text reading. Only studies fulfilling the inclusion criteria were considered eligible and included in the review for the subsequent data extraction. Disagreements between authors were solved through discussion and a third author (GT) evaluated the agreement between reviewers by calculating a value of K-statistic. In addition, data extraction and collection were performed by two authors (CA, KZ) in a joint session using an ad hoc extraction sheet.
Risk of bias assessment
The Cochrane Collaboration Tool was used for risk of bias assessment in the included studies [15]. The analysis was performed by two reviewers (CA and VCAC) in a joint session on the basis of seven domains: (a) random sequence generation, (b) allocation concealment, (c) selective reporting, (d) blinding of participants, (e) blinding outcome assessment, (f) incomplete outcome data and (g) other sources of bias. The judgment for each entry involved answering a question: the answer ‘YES’ meant low risk of bias, ‘NO’ meant high risk of bias and ‘UNCLEAR’ indicated either lack of information or uncertainty about potential biases. The GRADE methodology was used to assess the quality of the body of retrieved evidence (GRADEpro, Version 20. McMaster University, 2014).
Summary measures and planned methods for analysis
For the pooled analysis of PD reduction, CAL gain and bone defect depth reduction, the mean difference (MD) and its standard error (SE) between the two groups were calculated. The presence/absence of heterogeneity was assessed by means of the Higgins Index (I2). Data were pooled with a fixed-or a random-effect model on the basis of an I2 lower or upper the cut-off of 50%. The inverse of variance test was used to analyze the overall effects. We combined split-mouth and parallel designs as suggested by Elbourne et al. [16] and we estimated the absence of a carryover effect since we assumed that treated defects were not adjacent [17]. Mean Difference (MD) between test and control and Standard Error (SE) were calculated according to the method described by Lesaffre et al. [18]. In addition, subgroup analysis was performed on the basis of the study design (split-mouth or parallel groups) for PD reduction and CAL gain to investigate systematic differences. A subgroup analysis was performed on the basis of the type of bony defect (intra-bony or furcation defect) for bone defect depth reduction. In addition, subgroup analysis was performed on the basis of the type of bony defects (intra-bony or furcation defects). Trial sequential analysis (TSA) was performed with the goal to assess the power of the meta-analytic findings and to adjust results of the meta-analysis for the presence of types I (5%) and II (10%) errors. In particular, the alpha-spending function, trial sequential monitoring boundaries and the required information size (RIS) were calculated. TSA was performed using a model-variance based approach and performing heterogeneity correction on the basis of meta-analysis results. Results of the TSA were evaluated by graphically assessing if the cumulative Z-curve crossed the trial sequential monitoring boundaries, the futility boundaries and the RIS threshold.
Results
Studies selection and studies features
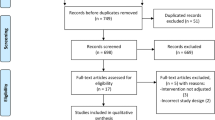
A total of 1242 records were screened by title and abstract from electronic databases. After the first round, 12 out of these papers were considered eligible for full-text examination. At the end of full text examination, seven papers met the inclusion criteria and were included in this systematic review [19,20,21,22,23,24,25]. The flow chart of the selection process is reported on Fig. 1. All the included studies were RCTs comparing the combination therapy of second step of periodontal therapy + Alendronate gel 1% (test group) with second step of periodontal therapy + placebo (control group). Reasons for exclusion of the remaining paper are reported on Additional file 1. The articles publication years ranged between 2012 and 2018. Two studies reported data about furcation defects [19, 20] while 5 reported data about intra-bony defects [21,22,23,24,25]. All the studies reported a 6-month follow-up [22,23,24,25], while only two studies reported a 12-months follow-up [19, 20]. One study had a split mouth design [21], while six had a parallel design [19, 20, 22,23,24,25]. Five studies had 2 arms of comparison [20,21,22,23,24], while two had three arms [19, 25]. Six out of seven of the included studies were funded by pharmaceutical companies [19, 20, 22,23,24,25]. In all the included studies, alendronate was injected into the periodontal pockets using a syringe with a blunt cannula during step II of periodontal therapy (Table 1).

PRISMA flow chart showing different phases of the selection process
Outcomes, for which meta-analysis of the included studies was not performed due to lack of data, are resumed in Table 2. Results of the risk of bias assessment are summarized in Fig. 2. One study showed unclear risk of bias for randomization [21] while two studies showed unclear risk of bias for allocation concealment [19, 22] and one study had high risk of bias for allocation concealment [21]. Six studies had low risk of bias [19, 20, 22,23,24,25] while one reported high risk of bias [21] (Fig. 2).

Risk of bias assessment according to the Cochrane Collaboration tool
Meta-analysis and trial sequential analysis
A total number of 408 patients were treated in the included studies in both test and control groups. A total of 207 sites were treated in the test group while 209 sites were treated in the control group.
PD reduction
Meta-analysis of PD reduction showed a significant difference (p < 0.00001) when alendronate was topically applied during step II periodontal therapy compared to placebo; MD = 2.01 (95% CI [1.60, 2.43]). Such results were characterized by a high rate of heterogeneity (I2 = 82%), for such reason a random effects model was used for data interpolation. A subgroup analysis was performed based on study design (parallel-groups vs split-mouth) to test for a possible influence of study design on the analyzed outcome. The effect estimate for parallel group studies was 2.11 (95% CI [1.69, 2.51]) and for split-mouth 0.30 (95% CI [− 1.23, 1.83]) and although both groups showed a benefit for alendronate compared to placebo an important difference was detected. Results of the TSA confirmed the previously performed meta-analysis with the z-curve crossing the lower alpha spending boundary, in addition the meta-analysis was characterized by a good power of evidence since the RIS (74 patients) was crossed (Fig. 3).

Meta-analysis (A) and Trial sequential analysis (B) for the effects of Alendronate therapy on PD reduction
CAL gain
Meta-analysis of CAL gain revealed a significant improvement (p < 0.00001) when alendronate was topically applied, MD = 1.72 (95% CI [1.30, 2.15]). Such results were characterized by a high rate of heterogeneity among studies (I2 = 88%) and for this reason a random effect model was used for data interpolation. A sub-group analysis was performed based on study design (parallel groups vs split-mouth); the effect estimate for parallel group studies was 1.82 (95% CI [1.37, 2.28]) and for split-mouth 0.90 (95% CI [0.08, 1.72]), also in this case study design influenced the effect size of results. The TSA confirmed the previously performed meta-analysis with the z-curve crossing the lower alpha spending boundary, in addition the meta-analysis was characterized by a good power of evidence since the RIS (74 patients) was also crossed (Fig. 4).

Meta-analysis (A) and Trial sequential analysis (B) for the effects of Alendronate therapy on CAL gain
Bone defect depth reduction
The analysis of bone defect depth reduction shows a significant difference between the therapy with alendronate compared to control: MD = 1.86 (95% CI [1.53, 2.19]), with results characterized by a high rate of heterogeneity (I2 = 97%). TSA confirmed such findings with the z-curve crossing the lower alpha spending boundary and RIS threshold (99 patients). No differences were detected between intra-bony and inter-radicular defects (p = 0.18) (Fig. 5).

Meta-analysis (A) and Trial sequential analysis (B) for the effects of Alendronate therapy on bone defect depth reduction
GRADE
Evidence by subgroups was qualified using the GRADE approach. Low quality of evidence supports the beneficial effect of alendronate 1% as an adjunct to second step of periodontal therapy in the treatment of intra-bony and inter-radicular defects. The level of evidence was downgraded due to inconsistency results of the included studies. Results of the GRADE evaluation are summarized in Additional file 1.
Discussion
This systematic review aimed to provide a clear focus on the role of alendronate 1% as an adjunct to second step of periodontal therapy in treatment of intra-bony and inter-radicular defects. Since the introduction of host-modulators in the treatment of periodontal disease [26], several studies have been performed to analyze the role of different substances in combination with second step of periodontal therapy [27,28,29,30,31].
Results of the present study showed that the topical application of Alendronate gel 1% can provide a significant benefit in PD reduction, CAL gain and bone defect depth reduction when applied after non-surgical periodontal treatment. A significant difference between parallel groups and split-mouth design was detected when subgroup analysis was performed for PD reduction and CAL gain. No significant differences were detected between intra-bony and inter-radicular defects when subgroup analysis was performed for bone defect depth reduction. BPs are often administered orally for the treatment of post-menopausal osteoporosis showing a wide range of adverse events including gastro-intestinal side effects, acute phase syndrome, secondary hyperparathyroidism, hypocalcemia, musculoskeletal pain and osteonecrosis of the jaw; therefore local application of alendronate might appear to be safer and devoid of side effects since none of the studies had drop-out patients that seemed to be related to local treatment; furthermore local administration offers the advantage of reaching a higher concentration of drug at the osseous defect with a reduced dosage [32]. However, even if these results might seem promising in providing a beneficial effect as an adjunct to subgingival instrumentation of intra-bony and inter-radicular defects, there are several concerns that must be taken into account when interpreting these results.
First of all, only two of the included studies [19, 20] reported data about inter-radicular defects, hence further studies are needed to confirm the results obtained of a potential beneficial effect of alendronate in this subtype of defects.
Of the seven included studies, only one provided more detailed information about the subgingival instrumentations performed [21]; in the remaining six it was not considered the number of sessions performed, the kind of instruments that were used or the experience of the operators who had performed the treatment. Moreover, the adjunct of alendronate during subgingival instrumentation is an adjunctive cost to conventional step II of periodontitis treatment.
We did not set the smoking status as an exclusion criterion, so this factor should be considered in the outcome of treatment, even if the use of alendronate as a host modulator in intraosseous defects could be particularly important for smokers whose healing capacity is impaired [33, 34]. Since only two studies [19, 20] had a 12-months follow-up, studies with a longer follow-up are necessary to confirm such results. An important point that should be considered when interpreting these results is that six studies [19, 20, 22,23,24,25] out of seven were conducted in the same country (India). Therefore, it must be considered the risk of a geographical bias, data from a more heterogeneous population would play an important role in confirming these findings. In addition, six [19, 20, 22,23,24,25] out of seven studies were funded by external pharmaceutical companies providing a potential confounding effect in the interpretation of results. An important issue is that one of the included studies [21] had a split-mouth design. Since its introduction by Ramfjord et al. in 1968 [35], split-mouth design has been widely used in oral health related studies. It generally requires less patients since the same individual serves as both test and control. However this kind of design presents some critical aspects as carry-across effect and needs a more complicated analysis in comparison with whole mouth studies [17, 36]. These results are consistent with the findings of Donos et al. [37] and the EFP Stage I-III periodontitis guideline [3] which affirm that only the adjunct of antiseptics and antibiotics may provide a beneficial effects to step II of periodontal therapy.
Conclusion
Based on the results available from these RCTs, this review shows that local delivery of alendronate seems to be effective in improving PD, CAL and bone defect depth. However, studies conducted by different research groups and on a geographically more heterogeneous population with a more standardized protocol are necessary to confirm these findings. Therefore, even if topical administration of Alendronate could have a potential beneficial effect on periodontitis clinical parameters, multicentric studies with a longer follow-up are needed to clarify this point.
Availability of data and materials
Not applicable.
Abbreviations
- CAL:
-
Clinical attachment level
- MD:
-
Mean difference
- PD:
-
Probing depth
- RCT:
-
Randomized clinical trial
- SE:
-
Standard error
- TSA:
-
Trial sequential analysis
References
Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodontol. 2018;89(Suppl 1):S159–72.
Haffajee AD, Socransky SS. Microbial etiological agents of destructive periodontal diseases. Periodontol. 2000;1994(5):78–111.
Sanz M, Herrera D, Kebschull M, Chapple I, Jepsen S, Beglundh T, Sculean A, Tonetti MS, Participants EFPW, Methodological C. Treatment of stage I–III periodontitis—the EFP S3 level clinical practice guideline. J Clin Periodontol. 2020;47(Suppl 22):4–60.
Van Dyke TE. Pro-resolving mediators in the regulation of periodontal disease. Mol Aspects Med. 2017;58:21–36.
Salvi GE, Lang NP. Host response modulation in the management of periodontal diseases. J Clin Periodontol. 2005;32(Suppl 6):108–29.
Tenenbaum HC, Shelemay A, Girard B, Zohar R, Fritz PC. Bisphosphonates and periodontics: potential applications for regulations of bone mass in the periodontium and other therapeutic/diagnostic uses. J Periodontol. 2002;73(7):813–22.
Liberman UA, Weiss SR, Broll J, Minne HW, Quan H, Bell NH, Rodriguez-Portales J, Downs RW Jr, Dequeker J, Favus M. Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The alendronate phase III Osteoporosis Treatment Study Group. N Engl J Med. 1995;333(22):1437–43.
Chavassieux PM, Arlot ME, Reda C, Wei L, Yates AJ, Meunier PJ. Histomorphometric assessment of the long-term effects of alendronate on bone quality and remodeling in patients with osteoporosis. J Clin Invest. 1997;100(6):1475–80.
Goziotis A, Sukhu B, Torontali M, Dowhaniuk M, Tenenbaum HC. Effects of bisphosphonates APD and HEBP on bone metabolism in vitro. Bone. 1995;16(4 Suppl):317s–27s.
Brunsvold MA, Chaves ES, Kornman KS, Aufdemorte TB, Wood R. Effects of a bisphosphonate on experimental periodontitis in monkeys. J Periodontol. 1992;63(10):825–30.
Akram Z, Abduljabbar T, Kellesarian SV, Abu Hassan MI, Javed F, Vohra F. Efficacy of bisphosphonate as an adjunct to nonsurgical periodontal therapy in the management of periodontal disease: a systematic review. Br J Clin Pharmacol. 2017;83(3):444–54.
Adami S, Bhalla AK, Dorizzi R, Montesanti F, Rosini S, Salvagno G, Lo Cascio V. The acute-phase response after bisphosphonate administration. Calcif Tissue Int. 1987;41(6):326–31.
Schweitzer DH, Oostendorp-Van De Ruit M, Van Der Pluijm G, Lowik CW, Papapoulos SE. Interleukin-6 and the acute phase response during treatment of patients with paget’s disease with the nitrogen-containing bisphosphonate dimethylaminohydroxypropylidene bisphosphonate. J Bone Miner Res. 1995;10(6):956–62.
Reddy GT, Kumar TM, Veena KM. Formulation and evaluation of alendronate sodium gel for the treatment of bone resorptive lesions in periodontitis. Drug Deliv. 2005;12(4):217–22.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:D5928.
Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A. Meta-analyses involving cross-over trials: methodological issues. Int J Epidemiol. 2002;31(1):140–9.
Lesaffre E, Garcia Zattera MJ, Redmond C, Huber H, Needleman I, Dentistry ISO. Reported methodological quality of split-mouth studies. J Clin Periodontol. 2007;34(9):756–61.
Lesaffre E, Philstrom B, Needleman I, Worthington H. The design and analysis of split-mouth studies: what statisticians and clinicians should know. Stat Med. 2009;28(28):3470–82.
Ipshita S, Kurian IG, Dileep P, Kumar S, Singh P, Pradeep AR. One percent alendronate and aloe vera gel local host modulating agents in chronic periodontitis patients with class II furcation defects: a randomized, controlled clinical trial. J Investig Clin Dent. 2018;9(3):E12334.
Pradeep AR, Kumari M, Rao NS, Naik SB. 1% alendronate gel as local drug delivery in the treatment of class II furcation defects: a randomized controlled clinical trial. J Periodontol. 2013;84(3):307–15.
Dutra BC, Oliveira A, Oliveira PAD, Manzi FR, Cortelli SC, Cota LOD, Costa FO. Effect of 1% sodium alendronate in the non-surgical treatment of periodontal intraosseous defects: a 6-month clinical trial. J Appl Oral Sci. 2017;25(3):310–7.
Sharma A, Raman A, Pradeep AR. Role of 1% alendronate gel as adjunct to mechanical therapy in the treatment of chronic periodontitis among smokers. J Appl Oral Sci. 2017;25(3):243–9.
Sharma A, Pradeep AR. Clinical efficacy of 1% alendronate gel in adjunct to mechanotherapy in the treatment of aggressive periodontitis: a randomized controlled clinical trial. J Periodontol. 2012;83(1):19–26.
Sharma A, Pradeep AR. Clinical efficacy of 1% alendronate gel as a local drug delivery system in the treatment of chronic periodontitis: a randomized, controlled clinical trial. J Periodontol. 2012;83(1):11–8.
Pradeep AR, Kanoriya D, Singhal S, Garg V, Manohar B, Chatterjee A. Comparative evaluation of subgingivally delivered 1% alendronate versus 1.2% atorvastatin gel in treatment of chronic periodontitis: a randomized placebo-controlled clinical trial. J Investig Clin Dent. 2017;8(3):e12215.
Paquette DW, Williams RC. Modulation of host inflammatory mediators as a treatment strategy for periodontal diseases. Periodontol. 2000;2000(24):239–52.
Keskiner I, Saygun I, Bal V, Serdar M, Kantarci A. Dietary supplementation with low-dose omega-3 fatty acids reduces salivary tumor necrosis factor-alpha levels in patients with chronic periodontitis: a randomized controlled clinical study. J Periodontal Res. 2017;52(4):695–703.
Feng HS, Bernardo CC, Sonoda LL, Hayashi F, Romito GA, De Lima LA, Lotufo RF, Pannuti CM. Subgingival ultrasonic instrumentation of residual pockets irrigated with essential oils: a randomized controlled trial. J Clin Periodontol. 2011;38(7):637–43.
Kurian IG, Dileep P, Ipshita S, Pradeep AR. Comparative evaluation of subgingivally-delivered 1% metformin and aloe vera gel in the treatment of intrabony defects in chronic periodontitis patients: a randomized, controlled clinical trial. J Investig Clin Dent. 2018;9(3):E12324.
Pankaj D, Sahu I, Kurian IG, Pradeep AR. Comparative evaluation of subgingivally delivered 1.2% rosuvastatin and 1% metformin gel in treatment of intrabony defects in chronic periodontitis: a randomized controlled clinical trial. J Periodontol. 2018;89(11):1318–25.
Yen CA, Damoulis PD, Stark PC, Hibberd PL, Singh M, Papas AS. The effect of a selective cyclooxygenase-2 inhibitor (celecoxib) on chronic periodontitis. J Periodontol. 2008;79(1):104–13.
Needleman IG, Pandya NV, Smith SR, Foyle DM. The role of antibiotics in the treatment of periodontitis (part 2—controlled drug delivery). Eur J Prosthodont Restor Dent. 1995;3(3):111–7.
Johnson GK, Hill M. Cigarette smoking and the periodontal patient. J Periodontol. 2004;75(2):196–209.
Preber H, Bergstrom J. The effect of non-surgical treatment on periodontal pockets in smokers and non-smokers. J Clin Periodontol. 1986;13(4):319–23.
Ramfjord SP, Nissle RR, Shick RA, Cooper H Jr. Subgingival curettage versus surgical elimination of periodontal pockets. J Periodontol. 1968;39(3):167–75.
Hujoel PP, Derouen TA. Validity issues in split-mouth trials. J Clin Periodontol. 1992;19(9 Pt 1):625–7.
Donos N, Calciolari E, Brusselaers N, Goldoni M, Bostanci N, Belibasakis GN. The adjunctive use of host modulators in non-surgical periodontal therapy. A systematic review of randomized, placebo-controlled clinical studies. J Clin Periodontol. 2020;47(Suppl 22):199–238.
Funding
The work has no funding.
Author information
Authors and Affiliations
Contributions
All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This article does not contain any studies with human participants or animals performed by any of the authors. For this type of study, formal consent is not required.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Results of the GRADE evaluation.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Arena, C., Caponio, V.C.A., Zhurakivska, K. et al. Added effect of 1% topical alendronate in intra-bony and inter-radicular defects as part of step II periodontal therapy: a systematic review with meta-analysis and trial sequential analysis. BMC Oral Health 22, 15 (2022). https://doi.org/10.1186/s12903-022-02044-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-022-02044-1