
Abstract
Background
Poor glycemic control increases the risk of acute metabolic derangements and long-term consequences, which are the main causes of morbidity and mortality. Maintaining adequate glycemic control is challenging for children with diabetes, particularly in resource-limited settings. There is a paucity of data on the magnitude of poor glycemic control and its predisposing factors in Ethiopian particularly in this study setting. Hence, we aimed to assess the magnitude of poor glycemic control and its associated factors among children and adolescents with type 1 diabetic mellitus in Jugol and Hiwot Fana Compressive Specialized University Hospitals in Harar, eastern Ethiopia.
Methods
A facility-based cross-sectional study was conducted among 231 children and adolescents with type 1 diabetes mellitus in Jugol and Hiwot Fana Compressive Specialized University Hospitals. Participants were included consecutively in the follow-up clinic from November 15, 2022 to January 15, 2023. Data were collected through an interviewer-administered structured questionnaire and a review of medical records. A binary logistic regression model with an adjusted odds ratio (aOR) and a 95% confidence interval (CI) was used to identify the factors associated with poor glycemic control. Statistical significance was set at p < 0.05.
Result
A total of 231 children and adolescents with type 1 diabetes mellitus were included. The magnitude of poor glycemic control was 166 (71.9%) with 95% CI 66.0–77.7%). In multivariable analysis, the age of the child (aOR = 0.19, 95% CI: 0.05–0.83), education of the caregiver (aOR = 4.13;95% CI: 1.82–9.46), meal frequency less than three (aOR = 3.28; 95% CI: 1.25–8.62), and consumption of forbidden foods (aOR = 3.17; 95% CI: 1.21–8.29) were factors significantly associated with poor glycemic control.
Conclusion
Two-thirds of participants had poor glycemic control. There was a statistically significant association between the age of the child, education of the caregiver, meal frequency, and forbidden foods with poor glycemic control. To improve glycemic control, diabetes education on meal use and selection should be conducted during follow-up along with parent education.
Similar content being viewed by others


Background
Diabetes mellitus (DM) is a cause of public health crisis among noncommunicable diseases that is associated with a significant increase in morbidity and mortality among the global population [1]. Worldwide, more than 500 000 children under the age of 18 years are affected by type one diabetes mellitus (T1DM), with an average annual incidence of 3 to 4% [1, 2]. The incidence of pediatric DM varies from 4.4 per 100,000 to 20 per 100,000 children in African countries [3]. Although there are different categories of DM, T1DM is the most prevalent in the pediatric population [4]. T1DM is a severe and long-lasting progressive condition that develops when the pancreas produces insufficient amounts of insulin [5].
Acute metabolic abnormalities such as diabetic ketoacidosis, hypoglycemia, and chronic consequences of diabetes, such as retinopathy, nephropathy, neuropathy, ischemic heart disease, and arterial blockage with gangrene of the extremities, are considered to be high contributors to morbidity and mortality among diabetic children [6]. The most powerful modifiable predictor for the occurrence of both acute and chronic complications of diabetes is poor glycemic control. Glycemic control is a watchword given for the level of blood sugar in the diabetic population, and strict glycemic control can postpone the onset, decrease the progression of chronic diabetes complications and increase cognitive functioning, as supported by the diabetes control and complications trial [4].
According to a study conducted in low and middle-income countries (LMICs), the magnitude of poor glycemic control ranges from 72–90.2% [7,8,9,10]. which implies that children and adolescents with T1DM have poor glycemic control. This in turn leads to deprived health outcomes [11]. In LMICs, the prognosis of children with T1DM is miserable, and many children lack timely diagnosis, treatment, and monitoring which drastically shortens life expectancy to less than one year [4, 11].
Available evidence indicates that children with T1DM have different risk factors for poor glycemic control. For example, glycosylated hemoglobin (HbA1c) levels in children are influenced by many factors, such as age, socioeconomic status, and family structure [8, 12]. It also correlated with diabetes-related characteristics, such as diabetes duration, adherence, and caregiver involvement in the child's treatment. Furthermore, the frequency of self-monitoring of blood glucose, food, duration of diabetes, frequency of clinic visits, use of an insulin regimen, and family engagement in diabetes-related activities are linked to the patient's level of glycemic control [11]. However, the abovementioned factors have been identified in high and middle-income countries, but it is unknown whether these or other variables govern glucose management in an environment where very limited access to medical care is frequently observed [11, 13, 14]. In addition, evidence on the current status of glycemic control among children with diabetes in resource-limited settings has not been updated, and the available data were based on fasting blood sugar levels alone.
To reduce the burden of poor glycemic control, various guidelines and recommendations have been made, such as those from the American Diabetes Association (ADA), the international society of pediatrics and adolescent diabetes (ISPAD), and the noncommunicable disease management guidelines of the Ministry of Health (MoH) Ethiopia [15,16,17]. Pediatric T1DM is always managed with aggressive insulin regimens, whether by several daily injections or continuous subcutaneous insulin infusions [18]. For all pediatric patients with diabetes, the ISPAD recommends routine self-monitoring of glucose using precise finger stick blood glucose measurements, with or without continuous glucose monitoring or intermittently scanned along with hemoglobin A1C (HgA1c) analysis every 2–3 months. Therefore, regular blood glucose monitoring should be advocated in T1DM children and adolescents to improve metabolic management. Moreover, providing support to families with children with diabetes, such as medical, financial, and social assistance, is crucial for effective diabetes management and control [1].
However, due to multiple reasons, such as parental illiteracy, poor healthcare infrastructure, and limited resources, children with diabetes suffer from poor glycemic control that persists across low-income countries, including Ethiopia. In addition, there is a paucity of data on the magnitude of poor glycemic control and its predisposing factors in children and adolescents in Ethiopia, particularly in Harari hospitals. Therefore, this study aimed to assess the magnitude of poor glycemic control and identify the associated factors among T1DM children on followed up at DM clinics in Harar eastern Ethiopia.
Methods and materials
Study setting, design, and population
This multicenter, cross-sectional study was conducted at public hospitals in the Harari region, eastern Ethiopia. Hiwot Fana Comprehensive Specialized University Hospital is a teaching referral hospital at Haramaya University and Jugol General Hospital located in Harar Town. These hospitals serve more than six million people in eastern Ethiopia. All T1DM children and adolescents who were followed up at a Hiwot Fana Compressive Specialized University Hospital and Jugol General Hospital from November 15, 2022 to January 15 2023 were included. Children aged less than or equal to 18 years and who were diagnosed with T1DM with regular follow-up were involved.
Inclusion and exclusion criteria
Children and adolescents with at least one HbA1c level and/or three consecutive measurements of fasting blood sugar (FBS) between November 15, 2022 to January 15 2023 were included. However, children and adolescents who were on treatment for less than 3 months were not included in this study.
Sample size and procedure
The sample size was determined by a single proportion formula by considering 16.4% glycemic control as a proportion (P) from a previous study conducted in Ethiopia [4] with the following assumptions 95% confidence interval (CL) and marginal error of 5%. The calculated sample size was 210; we added a 10% nonresponse rate, and the final sample size was 231. The sample was proportionally allocated to the selected hospitals based on the estimated average follow-up in the previous three months (January to March 2022) in both hospitals. A total of 231 participants were included using a consecutive sampling technique from those who were on follow-up with T1DM from November 15, 2022 to January 15, 2023, and who fulfilled the inclusion criteria.
Data collection
Data were collected using a pretested, structured interviewer-administered questionnaire and a review of medical records with a validated data abstraction checklist adapted from previous studies [4, 11,12,13,14]. The tool contains information on the sociodemographic conditions of the caregiver and children such as age, sex, educational status, marital status of caregiver, occupational status, and place of residence); clinical characteristics and medication-related factors (duration of diabetes, medication duration, anthropometric parameters, insulin type, and amount, follow-up, comorbidities, and medication use and place of insulin storage); nutritional-related factors (the number of meals per day, meal content, consuming forbidden foods); and health facility related factors (frequency of clinic visits, a distance of health facility, means of transportation, counseling by a health professional, presence of health insurance). HbA1c and FBG levels were measured according to the hospital standard of practice for laboratory procedures. HbA1c was measured using high-performance liquid chromatography, and a level greater than 7.5% indicated poor glycemic control [1].
Data were collected by two BSc nurses supervised by two senior nurses with a second degree. Patient records were retrieved using the medical registration number identified in the total DM caseload in the registration follow-up logbook. Data collection was carried out over two months, from November 15, 2022 to January 15, 2023.
Poor glycemic control
Is defined as HbA1c is more than 7.5% and/or the average FBG level is either < 70 or > 145 mg/dl [1].
Good glycemic control
Is defined as HbA1c is less than 7.5% and/or the average FBG level is either > 70 or < 145 mg/dl [1].
Length
Measured with the sliding board if age was less than 2 years and more than that, was measured by standing board and older measured meter.
Weight
Measured with a weight scale with calibration for each participant and interpreted as follows: Weight for age, between 3 and 2SD – normal and below 2SD- malnourished; Length/height for age, between 3 and 2SD – normal and below 2SD- malnourished; Weight for Length/height, between 3 and 2SD – normal and below 2SD- malnourished; Body Mass Index (BMI) for age, between 3 and 2SD – normal and below 2SD- malnourished.
Consuming forbidden foods
Is defined as if children consumed bread, pasta, rice, and sugar-added foods on a regular or daily basis.
Data quality control
To ensure the quality of data, a pretest was conducted on 5% of participants at Dil Chora referral hospital of the DM follow-up clinic. Two days of training were provided to all data collectors and supervisors. The data collection process was closely supervised, and the completeness of each questionnaire was checked daily by supervisors and the principal investigator. During data cleaning, a logical checking technique was employed to identify errors. Finally, double data entry was performed to verify the data consistency.
Data processing and analysis
The collected data were checked for completeness and coded, entered into Epi Data version 4.6, and exported to SPSS 26 for analysis. Frequency, means and proportions were used for the descriptive analysis. Glycemic control was classified as good if FBG was between 70–145 mg/dl or HbA1c level was < 7.5% and out of these values indicated poor glycemic control. A binary logistic regression model was used to determine the association between each independent variable and the outcome variable. All variables with p ≤ 0.25 in the bivariable logistic regression were entered into the final multivariable analysis to control confounders. The goodness of fit of the model was tested using the Hosmer‒Lemeshow test (> 0.05). A multicollinearity test was performed to determine the correlation between the independent variables using variance inflation factors (VIF > 10). The adjusted odds ratio (aOR) with 95% confidence intervals (CI) and a p value less than 0.05 were considered a statistically significant association.
Results
Sociodemographic characteristics of the participants
Among 231 study participants included in this study, 129 (55.8%) were male. The age of the patients ranged from 1–18 years, with a mean age of 13 ± 4.9 years, and those between the ages 10 and 18 accounted for 124 (53.7%). Regarding educational status, two third of the participants 155 (67.1%) were in elementary school and 57 (24.7%) were in high school. Of the study participants, 144 (62.3%) were from rural areas. The average standard deviation (SD) of family size was 6 ± 2.1 and approximately three-quarters of the participants had a family size ranging from 5 to 10. The mean and SD of the family's monthly income were 4379 ± 4904.7 ETB and 177 (76.6%) of them earned between 1000 and 5000 birrs (Fig. 1, Table 1).

Monthly family income of children and adolescents with T1DM in Jugol General Hospital and Hiwot Fana Compressive Specialized University Hospital, Harar, Eastern Ethiopia, November 15, 2022 to January 15, 2023. (n = 231)
Parental sociodemographic characteristics
Fathers were caregivers for 72 (28.6%) of the patients, 66 (31.2%) were cared by mothers and 54 (23.4%) of the participants had no caregivers. Of the 177 caregivers in the study, 91 (51.4%) were female and 86 (48.6%) were male. The age of the caregivers ranged from 18 to 75 years, with a mean of 36.8 ± 10.18 years. Half of the caregivers 89 (50.2%) were unable to read and write and only 43 (24.7%) attended secondary school or above. More than three-fourths of the caregivers, 139 (78.5%) were married and 27 (15.3%) were single. Seventy-nine of the caregivers (44.6%) were farmers, and 34 (19.2%) were housewives (Table 2).
Nutritional characteristics
Of the total participants, 109 (47.2%) had three meals and one snack per day. Among the participants, 50 (21.6%) had consumed forbidden food, and two-thirds of them 35 (70%) consumed foods that had a high content such as bread, pasta, and macaroni. Of the participants, 45 (19.4%) were underweight, 62 (21%) were stunted, 60 (25.9%) were wasting, 55 (23.8%), and 22 (9.4%) were malnourished when assessed with WFA, L/HFA, W/H, BMI for age and MUAC respectively (Table 3).
Duration and clinical characteristics
More than half (58.4%) of the study participants’ mean age at diagnosis was 7–12 years with SD of 9 ± 4.2 and duration of doagnosis range and SD of 1–5, and 3.6 ± 2.7 years respectively. This implies that the patients were on medication for a mean SD of 3.6 ± 2.6 years. The majority of the study participants, 213 (92.2%) were on nonpremixed NPH/RI regimen, while 6 (2.6%) used premixed NPH/RI insulin. The mean dose of insulin is 0.85 ± 0.24 IU/kg and 109 (47.2%) of the patients use a refrigerator to store the insulin. One handred seventy six (76.2%) of the study participants have administered the insulin by themselves and only 21 (9.1%) missed one dose of insulin. Three-quarters of the patients (75.3%) had their glucometer and approximately three-fourths of them (78%) used it 3 or more times a week. Only 13 (5.6%) of the study participants had comorbidities, with epilepsy accounting for 6 (46.2%). All injections that were administered and supervised in the last 24 h by the caregiver accounted for 61 (26.4%) and 71(30.7%) of the cases respectively. Seventy-five (42.4%) of the caregivers set up the meter, performed the finger prick, or supervised the task, while 70 (39.5%) had no participation in all care activities. Almost all of the patients 223 (96.5%) did not use any medications that could increase blood sugar (Table 4).
Health system characteristics
The average distance of study participants’ residency from health facilities was 72 ± 86 km, and 188 (81.4%) used public transport as a means of transportation. The average time taken from home to the health facility was 2 to 3h. Almost all of the patients 229 (99.1%) received counseling during the diagnosis of diabetes and 201 (87%) received all of the advice related to diabetes and insulin. A total of 211 (91.3%) patients had follow-up every month, while 20 (8.7 %7%) patients had follow-up every 2 months. Forty (17.3%) patients said that they faced problems in the hospital during health care delivery, with long waiting times, accounting for 27 (67.5%). Third- fourths of the study participants 174 (75.3%) had health insurance (Table 5).
The magnitude of poor glycemic control
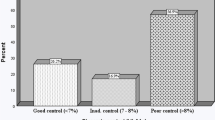
Of the total participants, more than two-thirds had poor glycemic control (71.9%) (95% CI: 66.0–77.7%). The mean and median HgbA1c levels were 10.4 and 10.8% respectively. The mean and median FBG levels were 220 and 200 mg/dl respectively. The mean HgbA1c and FBG were 10.4 ± 3.1 and 220 ± 116 respectively (Fig. 2).

Glycemic control of children and adolescents with T1DM in Jugol General Hospital and Hiwot Fana Compressive Specialized University Hospital, Harar, Eastern Ethiopia, November 15, 2022 to January 15, 2023. (n = 231)
Factors associated with poor glycemic control
In the bivariable logistic regression analysis, the age of the child, education level of both the child and caregiver, meal frequency, glucometer, BMI of the study participants who administered the medication, and consumption of forbidden food were eligible for the final model. However, only the age of the children, educational level of the caregiver, consumption of forbidden foods, and meal frequency were significantly associated with poor glycemic control in children and adolescents with T1DM.
Accordingly, preschool children were less likely by 81% to have poor glycemic control than those aged between 10 and 18 years (aOR = 0.19; 95% CL: 0.05–0.83). Those children who had a caregiver who was unable to read and write were four times more likely to have poor glycemic control than those who had secondary education (aOR = 4.13;95% CI: 1.82–9.46). Moreover, children whose meal frequency less than three were 3.28 times more likely to develop poor glycemic control than those children with a meal frequency of three and more than two snacks (aOR 3.28; 95% CI: 1.25–8.62). Furthermore, patients who ate forbidden foods were 3.17 times more likely to have poor glycemic control than their counterparts (aOR 3.17; 95%CI: 1.21–8.29) (Table 6).
Discussion
This study aimed to assess the magnitude of poor glycemic control and its associated factors among children and adolescents with T1DM in the Harari region, eastern Ethiopia. Accordingly, the magnitude of poor glycemic control was 71.9% (95% CI: 66.0–77.7%). In this study, the age of the patients, education of the primary caregiver, meal frequency, and consumption of forbidden food were independently associated with poor glycemic control.
The findings of this study are almost comparable with those reported in Arabian Gulf countries, African adolescents, and Sudanese children 72.6%, 67.4%, and 76% had poor glycemic control respectively [7, 19, 20]. However, the present findings are relatively lower than those of studies conducted in southern Ethiopia (83.6%) [4], Jimma (84%) [21], Sudan (76–78.9%) [7, 22] and Tanzania (97.3%) [9, 23]. This discrepancy could be explained by the vast differences in population sizes employed in the study. It may also be due to differences in the quality of care delivered to the patients as of time run in all of the study area. On the other hand, the findings in this study are much higher than the study conducted in the northwest part of Ethiopia (39.3%) [24]. This reveals how crucial it is to reduce our population's HbA1c level within an optimal range to minimize the devastating events that can occur following a poor level of glycemia among diabetic children in this particular study setting.
Glycemic control in children is influenced by a wide range of factors, such as young age, sex, BMI, socioeconomic status, education level, duration of diagnosis, and primary caregiver [11, 14, 25]. In this study, preschool-aged children were less likely by 81% to have poor glycemic control than adolescents. This finding is consistent with studies conducted in Dar es Salaam Tanzania and Egypt [9, 10, 12, 13]. The reason can be associated with parental participation and supervision in this age group [26, 27]. This is also because as a child matures, they undergo a variety of physical and lifestyle alterations [28, 29]. Furthermore, this might be due to hormonal effects and a decline in parental supervision of different clinical aspects of diabetes care in adolescents [14, 16].
Education of the primary caregiver which is linked to glycemic control is an independent factor. Children with parents who cannot read and write have poor glycemic control and a four-fold increased risk of poor glycemic control compared to children supported by educated parents. This is in agreement with studies conducted in Tanzania and Bulgaria, which reported that children and adolescents from families with poor parental education frequently struggle to achieve and maintain effective diabetes management [23, 30]. This is due to its effect on the child's care, follow-up, and correct drug handling and delivery [8, 26, 27].
In this study, patients who consumed foods with high levels of carbohydrates and sugar were 3.2 times more likely to have poor glycemic control than those who did not consume these foods. This finding is consistent with research conducted in Germany, Austria, and Italy, which signifies a link between consuming fewer carbohydrates, totally restraining food containing much darling, and lower HbA1c readings [25, 31,32,33]. These results suggest the need for medical nutrition therapy and attention to diabetes education to help children overcome barriers that impair glycemic control [34]. This finding also implies that monitoring carbohydrate intake, whether by carbohydrate counting or experience-based estimation is the key to achieving glycemic control [35]. An international organization such as the ISPAD recommends further research to examine any potential metabolic and glycemic benefits of carbohydrate restriction in the treatment of DM [36].
Frequency of meal was another independent factor significantly associated with poor glycemic control. A meal frequency of less than three were 3.3 times more likely to have poor glycemic control as compared to their counterparts having a meal frequency of three and more than two snacks. The findings of this study are consistent with research carried out in Japan, which stated that those with low meal frequency increases the mean 24 h interstitial glucose concentration among young diabetic population [37]; this finding also supported by the study done in Germany [38] and USA [39, 40]. The frequency of diet among T1DM may differ from that of healthy individuals due to disease-related factors that may affect the course of diabetes; waiting too long between meals and/or eating one big meal can rise blood sugar level [37]; furthermore, skiping meal frequently can lower metabolism, making it actually harder to manage blood glucose [41]. This insight will have an important implication in determining mealing approach to individuals with diabetes; recent evidence suggests that both meal frequency and daily energy distribution can influence glycaemic control [41, 42]. Similarly,in studies of meal frequency, conducted in individuals with T1DM, consumption of breakfast, the habit of regular meal pattern with multiple smaller meals (4–7 meals per day) and more frequent meals have been associated with better glycaemic control [41, 43].
In general, this study points to positive implications for clinical care, health service management, and research within the area of diabetic specialization. Clinically, healthcare workers can help patients by focusing on identifed factors associated with glycemic control among T1DM children at clinical setting. Healthcare managers can access current evidence regarding the overall magnitude of glycemic control in this particular study setting to take remedial action to strengthen service delivery by healthcare providers and other stakeholders. Researchers can also be motivated to conduct further research in this area emphasizing on diabetic nutritin by taking this study as a preliminary finding.
Limitations of the study
The study might be prone to recall bias for some intellectual questions and FBG measurements obtained from medical records might be subject to measurement errors that lead to underestimation or overestimation of the result. However, an effort was made to overcome these issues by taking the mean value of three-month consecutive values of FBG measurements and HA1c values in almost all patients.
Conclusion
Two-thirds of the participants had poor glycemic control. There was a statistically significant association between the age of the child, education of the caregiver, meal frequency, forbidden foods with poor glycemic control. To improve glycemic control, diabetes education including meal utilization, selection, and integrating the finding into routine care will help to address gaps in caregiver nutritional literacy and their ability to provide appropriate care.
Availability of data and materials
Data is available upon reasonable request from the corresponding author.
Abbreviations
- ADA:
-
American Diabetes Association
- AOR:
-
Adjusted odd Ratio
- BMI:
-
Body Mass Index
- DM:
-
Diabetes Mellitus
- FBG:
-
Fasting Blood Glucose
- HbA1c:
-
Glycated Hemoglobin A1C
- IHREC:
-
Institutional Health Research Ethical Committee
- ISPAD:
-
International Society of Pediatrics and Adolescent Diabetes
- SD:
-
Standard Deviation
- SPSS:
-
Statistical Package for Social Sciences
- T1DM:
-
Type 1 Diabetes Mellitus
References
Mayer-Davis EJ, Kahkoska AR, Jefferies C, Dabelea D, Balde N, Gong CX, et al. ISPAD clinical practice consensus guidelines 2018: definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2018;19(July):7–19.
Mobasseri M, Shirmohammadi M, Amiri T, Vahed N, Fard HH, Ghojazadeh M. Prevalence and incidence of type 1 diabetes in the world: a systematic review and meta-analysis. Heal Promot Perspect. 2020;10(2):98–115.
Ganu D. Increasing Incidence and prevalence of type 1 diabetes in children under 20 years of age between 1999–2019 in Sub-Saharan Africa : A systematic review. 2020;3(1):1–8.
Shibeshi MS, Daba AK, Meiso KM, Tadesse BT. Glycemic control among children and adolescents with diabetes in Southern Ethiopia: a cross-sectional study. BMC Endocr Disord. 2022;22(1):161.
Cataloguing WL. Global Report on Diabetes. ISBN. 2016;978:6–86.
Scott C, Patel A, Maka N, MacDonald JC. Crohn’s disease of the gallbladder. BMJ Case Rep. 2021;14(9):e243579.
Taha Z, Eltoum Z, Washi S. Predictors of glucose control in children and adolescents with type 1 diabetes: Results of a cross-sectional study in Khartoum, Sudan. Open Access Maced J Med Sci. 2018;6(11):2035–9.
Alassaf A, Odeh R, Gharaibeh L, Ibrahim S, Ajlouni K. Personal and clinical predictors of poor metabolic control in children with type 1 diabetes in Jordan. J Diabetes Res. 2019;2019:15–8.
Mclarty RP, Alloyce JP, Chitema GG, Msuya LJ. Glycemic control , associated factors , acute complications of Type 1 Diabetes Mellitus in children , adolescents and young adults in Tanzania. 2020;(July):1–8.
Mohammad H, Farghaly H, Metwalley K, Monazea E, Abd E-H. Predictors of glycemic control in children with Type 1 diabetes mellitus in Assiut-Egypt. Indian J Endocrinol Metab. 2012;16(5):796.
Niba LL, Aulinger B, Mbacham WF, Parhofer KG. Predictors of glucose control in children and adolescents with type 1 diabetes: results of a cross-sectional study in Cameroon. BMC Res Notes. 2017;10(1):1–10.
Al-Agha AE, Alafif M, Abd-Elhameed IA. Glycemic control, Complications, and associated autoimmune diseases in children and adolescents with type 1 diabetes in Jeddah. Saudi Arabia Saudi Med J. 2015;36(1):26–31.
Noorani M, Ramaiya K, Manji K. Glycaemic control in type 1 diabetes mellitus among children and adolescents in a resource limited setting in Dar es Salaam- Tanzania. BMC Endocr Disord. 2016;16(1):1–8. https://doi.org/10.1186/s12902-016-0113-y.
Andrade CS, Ribeiro GS, Santos CAST, Neves RCS, Moreira ED. Factors associated with high levels of glycated haemoglobin in patients with type 1 diabetes: a multicentre study in Brazil. BMJ Open. 2017;7(12):1–10.
Chiang JL, Maahs DM, Garvey KC, Hood KK, Laffel LM, Weinzimer SA, et al. Type 1 Diabetes in Children and Adolescents : A Position Statement by the American Diabetes Association. 2018;41(September):2026–44.
DiMeglio LA, Acerini CL, Codner E, Craig ME, Hofer SE, Pillay K, et al. ISPAD clinical practice consensus guidelines 2018: glycemic control targets and glucose monitoring for children, adolescents, and young adults with diabetes. Pediatr Diabetes. 2018;19:105–14.
MOH. Guidelines on Clinical and Programmatic Management of Major Non Communicable Diseases. 2016;220.
Care D, Suppl SS. Children and adolescents: Standards of medical care in diabetes—2021. Diabetes Care. 2021;44:S180–99.
Hafidh K, Abdella NA. Glycemic control of adult patients with type 1 diabetes mellitus in Arabian Gulf Countries; PREDICT. BMC Endocr Disord. 2022 Dec;22(1).
Djonou C, Tankeu AT, Dehayem MY, Tcheutchoua DN, Mbanya JC, Sobngwi E. Glycemic control and correlates in a group of sub Saharan type 1 diabetes adolescents 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Res Notes. 2019;12(1):1–5. https://doi.org/10.1186/s13104-019-4054-1.
Cheneke W, Suleman S, Yemane T, Abebe G. Assessment of glycemic control using glycated hemoglobin among diabetic patients in Jimma University specialized hospital. Ethiopia BMC Res Notes. 2016;9(1):1–10.
Abdelseed NAH. glycemic control and knowledge among children and adolescents with type 1 diabetes mellitus; a cross-sectional study. J Sci Res Med Biol Sci. 2021;2(1):1–9.
McLarty RP, Alloyce JP, Chitema GG, Msuya LJ. Glycemic control, associated factors, acute complications of Type 1 diabetes mellitus in children, adolescents and young adults in Tanzania. Endocrinol Diabetes Metab. 2021;4(2):e00200.
Kidie AA, Ayal BG, Ayele T, Fentie EA. Poor glycemic control and associated factors among pediatric diabetes mellitus patients in northwest Ethiopia , 2020 : facility ‑ based cross sectional retrospective study design. Sci Rep. 2022;1–7.
Seckold R, Howley P, King BR, Bell K, Smith A, Smart CE. Dietary intake and eating patterns of young children with type 1 diabetes achieving glycemic targets. BMJ Open Diabetes Res Care. 2019;7(1):e000663.
A AlAgha M, M Majdi W, Aljefri HM, Abdelfattah Ali M, Alagha AE, Abd Elhameed IA, et al. Effect of Parents’ Educational Level and Occupational Status on Child Glycemic Control. J Patient Care. 2017;03(02):2–4.
Ndahura NB, Munga J, Kimiywe J, Mupere E. Caregivers ’ nutrition knowledge and dietary intake of type 1 diabetic children aged 3–14 years in Uganda. Diabetes Metab Syndr Obes. 2021;14:127–37.
Rotteveel J, Waarde WMB, Houdijk ECAM, Nuboer R, Winterdijk P, Snoek FJ. Youth with type 1 diabetes taking responsibility for self- management : the importance of executive functioning in achieving glycemic control results from the longitudinal DINO Study. 2019;42:225–31.
Musenge EM, Michelo C, Mudenda B, Manankov A. Glycaemic control and associated self-management behaviours in diabetic outpatients: a hospital based observation study in Lusaka, Zambia. J Diabetes Res. 2016;2016:7934654.
Archinkova M, Konstantinova M, Savova R, Iotova V, Petrova C, Kaleva N, et al. Glycaemic control among Bulgarian children and adolescents with type 1 diabetes–an impact of the social status and the educational level of the parents. Biotechnol Biotechnol Equip. 2018;32(2):535–41.
Jaja TC, Yarhere IE. Dyslipidaemia in Nigerian children and adolescents with diabetes mellitus: prevalence and associated risk factors. Int J Diabetes Metab. 2019;25(1–2):45–51.
Lejk A, Chrzanowski J, Cieślak A, Fendler W, Myśliwiec M. Effect of nutritional habits on the glycemic response to different carbohydrate diet in children with type 1 diabetes mellitus. Nutrients. 2021;13(11):1–11.
Kleiner A, Cum B, Pisciotta L, Cincione IR, Cogorno L, Prigione A, et al. Safety and efficacy of eucaloric very low-carb diet (EVLCD) in type 1 diabetes: a one-year real-life retrospective experience. Nutrients. 2022;14(15):1–11.
Davison KAK, Negrato CA, Cobas R, Matheus A, Tannus L, Palma CS, et al. Relationship between adherence to diet , glycemic control and cardiovascular risk factors in patients with type 1 diabetes : a nationwide survey in Brazil. 2014;1–11.
Care D, Suppl SS. Children and adolescents: Standards of medical care in diabetes- 2020. Diabetes Care. 2020;43(January):S163–82.
Annan SF, Higgins LA, Jelleryd E, Baptista J, Hannon T, Rose S, et al. ISPAD GUIDELINES ISPAD clinical practice consensus guidelines 2022 : nutritional management in children and adolescents with diabetes. 2022;1–25
Hatamoto Y, Tanoue Y, Yoshimura E, Matsumoto M, Hayashi T, Ogata H, et al. Delayed eating schedule raises mean glucose levels in young adult males : a randomized controlled cross-over trial. J Nutr. 2023;153(4):1029–37. https://doi.org/10.1016/j.tjnut.2022.12.024.
Baechle C, Hoyer A, Castillo-reinado K, Stahl-pehe A, Kuss O, Holl RW, et al. Eating Frequency and Carbohydrate Intake in Adolescents with Type 1 Diabetes Differ from Those in Their Peers and are Associated with Glycemic Control.
Mendoza JA, Haaland W, Agostino RBD, Martini L, Pihoker C, Frongillo EA, et al. Food insecurity is associated with high risk glycemic control and higher health care utilization among youth and young adults with type 1 diabetes. Diabetes Res Clin Pract. 2018;138:128–37.
FS Malik AD Liese BA Reboussin KA Sauder EA Frongillo JM Lawrence et al 2023 Prevalence and Predictors of Household Food Insecurity and Supplemental Nutrition Assistance Program Use in Youth and Young Adults With Diabetes : The SEARCH for Diabetes in Youth Study 46 February 278 285
Ahola AJ, Mutter S, Forsblom C, Harjutsalo V, Groop H. Meal timing , meal frequency , and breakfast skipping in adult individuals with type 1 diabetes – associations with glycaemic control. Sci Rep [Internet]. 2019;1–10. Available from: https://doi.org/10.1038/s41598-019-56541-5
Satriale F, Garman JC, Roy S, Parascando J, Berg A, Oser T. Understanding Nutritional Knowledge and Experiences in Families With a Child Newly Diagnosed With Type 1 Diabetes. 2022;52–8.
Chacko E. Meal frequency and diabetes : A case study. 2021 11;860:2-5.
Acknowledgements
We thank Haramaya University for its technical support. We would also extend our gratitude to the head and staff of Hiwot Fana Specialized University Hospital and Jugol Hospital, the study participants, data collectors, and the supervisor for their collaboration.
Funding
This work was technically and financially supported by Haramaya University, Ethiopia. This organization had no role in study selection, data collection, analysis, conclusion, and interpretation.
Author information
Authors and Affiliations
Contributions
BDH, AD and BSH made a substantial contribution from conception to data interpretation of the findings. AM, FM, MK, AA, GT, made significant contributions to the study design, analysis, and interpretation of the findings. FM drafted the manuscript. All authors have carefully revised the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Before starting the data collection process, the study protocol was approved by Haramaya University, College of Health and Medical Sciences Institution Health Research Ethical Review Committee (IHRERC)/191/2022. An official letter of cooperation was submitted to Hiwot Fana Comprehensive Specialized University Hospital and Jugol General Hospital concerned bodies to obtain cooperation and consent to facilitate the study. Voluntary and written informed consent was obtained from hospital head and from all study participants and/or their legal gardians. This study did not expose children with diabetes to unnecessary risks. Confidentiality was kept at all levels of the study; it was assured by excluding names and identifiers in the questionnaire and the data were used only for this study purpose. The study was conducted in accordance with the guidelines and regulations of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Habteyohans, B.D., Hailu, B.S., Meseret, F. et al. Poor glycemic control and its associated factors among children with type 1 diabetes mellitus in Harar, eastern Ethiopia: A cross-sectional study. BMC Endocr Disord 23, 208 (2023). https://doi.org/10.1186/s12902-023-01453-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01453-9