
Abstract
Background
The atherogenic index of plasma (AIP) is a novel biomarker associated with atherosclerosis, and an important risk factor for atherosclerosis, but its relation with cardiovascular prognosis in prediabetic patients with unstable angina pectoris (UAP) is still uncertain.
Methods
This study included 1096 prediabetic patients with UAP who were subjected to follow-up for a maximum of 30 months, with cardiac death, refractory angina, and non-fatal myocardial infarction (MI) being the primary cardiovascular endpoints.
Results
A significantly increased AIP was observed for the group with primary cardiovascular endpoints. Kaplan–Meier curves corresponding to these endpoints revealed pronounced differences between these two AIP groups (Log-rank P < 0.001). Multivariate Cox proportional hazards analyses highlighted AIP as being independent related to this primary endpoint (HR 1.308, 95% CI: 1.213–1.412, P < 0.001). AIP addition to the baseline risk model improved the prediction of the primary endpoint (AUC: baseline model, 0.622, vs. baseline model + AIP, 0.739, P < 0.001).
Conclusions
AIP could be used to predict cardiovascular events in prediabetic individuals with UAP.
Similar content being viewed by others

Introduction
In recent years, the significance of triglycerides (TG) in atherosclerotic cardiovascular disease and the associated clinical practice has been paid increasing attention [1, 2]. The relevance of the lipid ratio or atherogenic indices are widely reported [3], among which the atherogenic index of plasma (AIP) was first proposed in 2001 as a comprehensive lipid index based upon the logarithm of the TG to high-density lipoprotein cholesterol (HDL-C) ratio [4]. Since AIP is closely related to the cholesterol esterification rate, lipoprotein particle size, and residual lipoproteinemia, it is thought to represent a valuable biomarker of plasma atherogenicity [5, 6].
Diabetic dyslipidemia is associated with increases in the levels of TGs with a concomitant drop in HDL-C levels without any corresponding changes in LDL-C levels. Notably, the LDL subfraction distribution in diabetic patients is shifted to small dense LDL (sdLDL), a subtype of LDL with smaller particles and higher density which is susceptible to multiple chemical modifications and further enhances atherosclerosis [7, 8]. As an inexpensive and easily assessed marker, AIP can be used to assess the progression of atherosclerosis, and studies have confirmed that AIP may become a useful substitute for sdLDL [9]. A subsequent study found that AIP was a powerful and reliable biomarker for predicting coronary artery disease (CAD) risk among individuals diagnosed with type 2 diabetes mellitus (T2DM) [10].
Prediabetes is defined by the elevation of blood glucose levels above the normal reference range but not at the threshold necessary for a diagnosis of T2DM, and it is generally considered an intermediate stage between T2DM and normoglycemia [11]. Atherogenic patterns corresponding to cardiovascular risk factors, including obesity, blood pressure, and dyslipidemia, are prominent in prediabetes patients prior to clinical T2DM development [12]. It has been found that the incidence of subclinical atherosclerosis in prediabetic subjects is significantly higher than that in normoglycemic subjects [13]. Considering that AIP is closely associated with elevated cardiovascular disease risk as compared with simple lipid levels [14], and the prognosis of AIP in prediabetic patients with unstable angina pectoris (UAP) is currently unclear, this study sought to investigate the association between AIP and cardiovascular prognosis in prediabetic individuals with UAP.
Methods
Study population
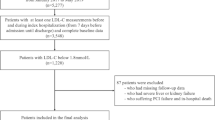
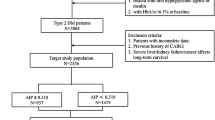
This was a single-center retrospective analysis, including 1927 UAP patients with prediabetes hospitalized in Beijing Anzhen Hospital between January and December of 2018. The exclusion criteria included: (1) severe hepatic insufficiency (abnormal aspartate aminotransferase or alanine aminotransferase) or renal failure insufficiency (estimated glomerular filtration rate (eGFR) < 30 ml/min/1.73 m2); (2) lack of clinical data; (3) history of cancer, coronary artery bypass grafting (CABG), or chronic infectious diseases; and (4) diagnosed or suspected to have a history of type 1 diabetes. Prediabetes [15] was defined as: (1) glycosylated hemoglobin A1c (HbA1c) at 5.7–6.4%; (2) no history of diabetes; and (3) no history of using hypoglycemic drugs or insulin therapy. The definition of UAP includes chest pain on exertion or rest within 2 weeks which are the presence of new or developing, in defect of elevated cardiac enzymes including high-sensitivity troponin I < 19.8 pg/ml and creatine kinase‐ MB < 6.3 ng/ml (the threshold of cardiac enzymes of Anzhen Hospital) [16, 17]. A total of 1096 prediabetic patients with UAP were finally included (Fig. 1).

Flow chart of the study population enrollment. UAP: unstable angina pectoris; HbA1c: glycosylated hemoglobin A1c; CABG: coronary artery bypass grafting; eGFR: estimated glomerular filtration rate; ALT: alanine transaminase; AST: aspartate transaminase; AIP: atherogenic index of plasma
Data collection, definitions, and laboratory examination
Data included patient demographics and clinical characteristics (sex, age, systolic blood pressure (SBP), diastolic blood pressure (DBP), body mass index (BMI), smoking history, medical history, blood biomarkers, and pre-admission medication). The primary endpoint for this analysis consistent of events including cardiac death, refractory angina, and non-fatal myocardial infarction (MI). The secondary endpoints were the individual components of the primary endpoint. Patient follow-up was conducted by trained professional individuals via telephone interviews or outpatient clinic visits to collect relevant medical details at the 3, 6, and 12 month time points, and once per year thereafter for a maximum of 30 months. Before adjudicated by two experienced cardiologists, all events were verified via contact with the treating physicians and medical records. In addition, the mean follow-up time was 26.3 ± 6.5 months, with minimun 0.5 to maximun 30 months, and patients with the lower AIP levels were followed for a longer period (27.6 ± 4.8 vs. 24.1 ± 8.4, p < 0.001).
AIP was assessed from blood samples and calculated as follows: AIP = lg (TG/HDL-C), where each concentration is expressed in mmol/L [4, 18]. After fasting for 12 h, venous blood was collected from each patient. Biochemical parameters, including white TG, total cholesterol (TC), HDL-C, LDL-C, creatinine (Cr), eGFR, serum uric acid (SUA), fasting blood-glucose (FBG), C-reactive protein (CRP), and HbA1c, were analyzed using an automated biochemical analyzer in the clinical laboratory center of Beijing Anzhen Hospital. Ethics approval and consent to participateThe present study was approved by the Clinical Research Ethics Committee ofBeijing Anzhen Hospital, Capital Medical University, and all patients providedwritten informed consent for participation in the present study.
Statistical analysis
Continuous variables were compared via one-way ANOVAs and Kruskal-Wallis tests, whereas categorical variable comparisons were made via chi-squared tests. Correlations of baseline characteristics were assessed via the Spearman or Pearson correlation tests. Receiver-operating characteristic (ROC) curve analyses were performed to establish optimal cutoff point values for AIP. Mainly based on clinical importance, the Cox proportional risk model was employed to evaluate the relations between AIP as a continuous variable and research results, including Model 1 (mainly including the demographic, physical and behavioral variables): adjusted for age, sex (male), BMI, SBP, DBP, smoking, hypertension, dyslipidemia, and prior percutaneous coronary intervention (PCI); Model 2 (based on Model 1 and added laboratory variables of lipids): additionally adjusted for TC and LDL-C, as well as the adjustments included in Model 1; Model 3 (based on Model 2 and added remaining laboratory variables): additionally adjusted for eGFR, FBG, HbA1c, Cr, CRP, and SUA as well as the adjustments included in Model 2; and Model 4 (based on Model 3 and added medication): additionally adjusted for statin usage, angiotensin converting enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB), calcium channel blockers (CCB), β-blocker usage, and antiplatelet treatment, as well as the adjustments included in Model 3. The incremental value of AIP in the context of baseline risk model-based predictive analyses in a model considering risk factors such as age, sex (male), BMI, SBP, DBP, smoking, hypertension, dyslipidemia, prior PCI, TC, LDL-C, eGFR, Cr, CRP and SUA was assessed. Area under the curve (AUC) values for each model were compared via DeLong’s test. The Kaplan–Meier method was used to visualize the survival over time, and the survival curve was compared with the log-rank test. R 4.0.0 was used for all statistical analyses in this study, and in all analyses, P < 0.05 was considered statistically significant.
Results
Baseline characteristics
Under the grouping with or without cardiovascular adverse events, denoted as the event group and non-event group, respectively, there were 141 and 955 patients in the event and non-event groups, respectively. Average age and HDL-C values were significantly lower in the event group relative to the non-event group, whereas significant increases in BMI, TG, AIP, and SUA values for the event group were observed as compared to the non-event group, as shown in Table 1.
After grouping AIP by the best cutoff value of the ROC curve, the high-AIP group included 393 patients and the low-AIP group included 703 patients. The age and HDL-C of the high-AIP group were significantly reduced as compared to the low-AIP group. The BMI, smoking percentage, TG, TC, LDL-C, AIP, Cr, SUA, FBG,β-blocker, and target vessel of right coronary artery usage were significantly increased in the high-AIP group. These results are displayed in Table 2.
Correlations between AIP and cardiovascular risk factors
Through correlation analyses, presented in Fig. 2, we found that AIP was positively associated with eGFR, LDL-C, TC, HT, DBP, hyperlipidemia, FBG, CRP, BMI, TG, HbA1c, statin usage, pre-PCI, smoking, SUA, sex, and Cr. In addition, AIP was significantly positively correlated with eGFR, HT, DBP, hyperlipidemia, statin usage, HbA1c, and pre-PCI. In contrast, AIP was inversely correlated with age and HDL-C, and no significant difference was found.

Correlations between the AIP and other factors. AIP: atherogenic index of plasma; eGFR: estimated glomerular filtration rate; CRP: C-reactive protein; HbA1c: glycosylated hemoglobin A1c; FBG: fasting blood-glucose; SUA: serum uric acid; Cr: creatinine; HDL-C: high density lipoprotein cholesterol; TC: total cholesterol; TG: triglyceride; LDL-C: low density lipoprotein cholesterol; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index; PCI: percutaneous coronary intervention
Cardiovascular outcomes and Kaplan–Meier analysis
At 30 months follow-up, there were four cases of cardiac death (0.4%), 11 cases of nonfatal myocardial infarction, and 134 cases of recurrent angina (12.2%) (Table 3). The incidences of the primary endpoint, refractory angina, and non-fatal MI rose significantly among individuals with a higher AIP (P < 0.05), although similar cardiac death rates were observed between groups (Table 3). Kaplan-Meier curve analyses corresponding to the primary endpoint revealed significant differences between AIP groups (Log-rank P < 0.001) (Fig. 3A). This difference was primarily attributable to the higher incidences of non-fatal MI and refractory angina (Log-rank P < 0.01) (Fig. 3C and D). Kaplan–Meier curves for cardiac death did not differ between groups (Log-rank P = 0.1) (Fig. 3B).

Kaplan–Meier curves for endpoint events according to the optimal cutoff point of AIP. A: Kaplan–Meier curves for primary endpoint; B: Kaplan–Meier curves for cardiac death; C: Kaplan–Meier curves for non-fatal myocardial infarction; D: refractory angina
Evaluation of AIP in prognostic implication
In multivariate Cox proportional hazards analysis, we found that in all four models, after adjusting other influencing factors, AIP could be used as a predictor of the primary endpoint. These analyses revealed that each unit increase in AIP was independently related to increased primary endpoint risk (Model 1: HR 1.242, 95% CI 1.178–1.309, P < 0.001; Model 2: HR 1.303, 95% CI 1.212–1.400, P < 0.001; Model 3: HR 1.319, 95% CI 1.222–1.423, P < 0.001; Model 4: HR 1.308, 95% CI 1.213–1.412, P < 0.001) (Table 4). After multivariate analysis of model 4 with AIP for different outcomes, AIP was independently related to an elevated risk of non-fatal MI and refractory angina (non-fatal MI: HR 1.619, 95% CI 1.129–2.323, P = 0.009; refractory angina: HR 1.313, 95% CI 1.215–1.419, P < 0.001) (Table 5).
The incremental effects of AIP on adverse prognosis predictive value
Adding AIP to the baseline risk model had a more significant incremental effect on the AUC obtained from the baseline risk model compared to adding FBG, HbA1c, or TG to the baseline risk model (AUC: baseline risk model, 0.622, vs. baseline risk model + AIP, 0.739, P < 0.001) (Table 6; Fig. 4).

C-statistics evaluating incremental effect of FBG, HbA1c, TG and AIP beyond baseline risk model. AIP: atherogenic index of plasma; FBG: fasting blood-glucose; HbA1c: glycosylated hemoglobin A1c; TG: triglyceride
Discussion
AIP in metabolism and T2DM
In studies examining the relationship between AIP and cardiovascular health (CVH) scores, the number of desirable CVH markers was inversely related to the high prevalence of AIP [19]. Besides, moderate- and high-intensity physical activity are significantly negatively corelated with AIP [20]. In addition, it has been found that more aggregated risk factors in T2DM patients include increased TG, higher BP, central obesity, and insulin resistance. Potential mechanisms are increases in inflammation, oxidative stress, and endothelial cell dysfunction, which is associated with lower HDL-C levels [21]. AIP is a convenient clinical indicator that can aid in detecting high-risk T2DM complications and those of associated diseases, and it can be reliably used to monitor follow-up outcomes in high-risk T2DM patient populations [22]. One study found that the AIP of T2DM patients with metabolic syndrome was higher than that of T2DM patients without metabolic syndrome [23]. Through multivariate logistic regression analysis, another study found AIP to be independently related to metabolic syndrome, suggesting that lipid ratio can be used to reliably predict the risk of metabolic syndrome [24]. A third study proposed a direct relationship between dietary fat mass, increased BMI, and AIP dyslipidemia [25]. In our study, it was found that AIP was positively correlated with hyperlipidemia, HbA1c, and BMI, and it might be associated with the metabolism of lipids and diabetes.
The molecular mechanism of AIP in atherosclerosis
The ability of lipids to migrate under the intima is an important step in the development of atherosclerosis. Lipids and their lipoprotein components have been designated as mediators and markers of CAD, characterized by a high ratio of LDL-C to HDL-C and an elevated level of TG [26]. Some studies have suggested AIP as an alternative to sdLDL particles [4] and shown that it may be a robust predictor for the risk of cardiovascular disease and atherosclerosis [27]. The specific mechanism of AIP and atherosclerosis is still unclear, but sdLDL is strongly atherosclerotic. This may be because sdLDL particles are more readily exposed on the surface, so they can easily penetrate the vascular endothelium and bind to arterial wall glycoproteins. As a result, lipid deposits gradually develop and are transformed into foam cells. Furthermore, sdLDL is easily oxidized to oxidized LDL-C [28], which can in turn aggregate adhesion molecules and chemokines, driving monocytes to differentiate into macrophages [29]. In response to cholesterol, large quantities of foam cells will be generated, thus inducing atherosclerosis. Moreover, sdLDL can suppress antioxidant production, thus accelerating atherosclerosis [30]. Studies have shown that AIP is the best factor to determine the cholesterol esterification rate of HDL-C and is more useful than conventional lipid parameters [31], so AIP could be considered as an auxiliary tool for personal blood lipid profiles [32]. Although our study did not include the analysis of basic research and the data of sdLDL, AIP may still become an alternative compound lipid index for sdLDL, providing a certain reference value for clinicians. However, more studies are still needed to explore the specific mechanism of AIP.
The relationship between AIP and cardiovascular outcomes
Dyslipidemia is a key risk factor associated with CAD. AIP is a new comprehensive lipid index that may be a powerful predictor of risk in CAD [33]. Previous studies have pointed out that AIP is significantly associated with coronary artery calcium (CAC) progression in patients without cardiovascular disease (CVD). Although AIP is not an independent predictor of CAC progression, it should be considered along with other traditional risk factors when assessing CVD risk [34]. In patients with baseline CAC levels, AIP was also significantly related to the progression of CAC, and researchers have indicated that AIP has predictive value for CAC progression in adults who are asymptomatic and do not have severe CAC at baseline [35]. Based on a series of coronary computed tomography angiography (CCTA) results, AIP was proved to be an independent predictor of rapid plaque progression [36].
Regarding the prognostic capability of AIP, studies have found that AIP is positively related to CVD risk and may be a better predictor of mortality than individual cholesterol risk factors [37]. In a 15-year cohort study, researchers found that AIP could independently predict CVD development and its associated mortality [38]. Considering the presence of subclinical atherosclerosis could not be underestimated according to previous studies [39], the association of AIP with advanced subclinical CAD is also higher than that of traditional risk factors [40]. As for diabetic patients, studies have found that AIP may be a powerful biomarker when monitoring cardiovascular event risk in T2DM patients [41]. In non-diabetic patients, higher AIP levels may predict the development of ischemic heart disease [42]. Higher level of AIP is significantly associated with the prevalence of prediabetes and T2DM [43]. Compared with people with normal blood glucose, the level of AIP in patients with prediabetes is significantly increased, and the risk of CVD occurs earlier [44]. At the same time, Mahat et al. found that prediabetes patients have abnormal AIP, suggesting that prediabetes is prone to develop CVD [45]. In addition, El-Eshmawy et al. have confirmed that AIP is significantly correlated with inflammatory indicators in prediabetes, which indicates that AIP may participate in atherosclerosis through inflammatory response [46]. POST-PCI study, a multicenter randomized clinical trial with a primary endpoint including hospitalization for UAP, included 80% of patients with angina [47]. In the concurrent ISCHEMIA trial, approximately 20% of patients had previously undergone PCI, which was similar to our study. Approximately two thirds of the patients in this trial had angina symptoms in the four weeks prior to randomization [48]. With reference to these two large clinical studies, we identified the composite endpoints in our study. In our study, through multivariate regression analysis, it was found that in model 4, AIP was independently and positively correlated with the primary endpoint, and the predictive value for adverse prognosis also suggested that AIP was better than other blood indicators based on the baseline risk model. We explored the relation between AIP and cardiovascular outcomes in prediabetic patients with UAP, and the results suggested that patients with higher levels of AIP may have more cardiovascular events. In conclusion, the study of AIP-related prognosis provides a potential direction for studying CVD risk in UAP and developing intervention strategies for these patients.
Conclusion
As a composite lipid index, AIP is closely related to the prognosis of prediabetic patients with UAP, and it has the potential to be a convenient and valuable clinical reference index.
Limitations
Our study has certain limitations. First, our study is a follow-up study, not a multi-center randomized controlled trial with a high level of evidence, so the conclusions drawn from the study may be biased. In addition, the validation procedure of this study is still on going. Second, AIP is an index calculated based on previous research results. The significance of our research is to provide a certain clinical reference value. AIP may represent the components of sdLDL, but its specific mechanism in the human body and the prognosis of patients is still unknown. More research on its mechanism is needed.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIP:
-
atherogenic index of plasma
- UAP:
-
unstable angina pectoris
- TG:
-
triglyceride
- HDL-C:
-
high density lipoprotein cholesterol
- LDL-C:
-
low density lipoprotein cholesterol
- sdLDL:
-
small dense low density lipoprotein
- CAD:
-
coronary artery disease
- T2DM:
-
type 2 diabetes mellitus
- SAP:
-
unstable angina pectoris
- eGFR:
-
estimated glomerular filtration rate
- HbA1c:
-
glycosylated hemoglobin A1c
- CABG:
-
coronary artery bypass grafting
- BMI:
-
body mass index
- SBP:
-
systolic blood pressure
- DBP:
-
diastolic blood pressure
- MI:
-
myocardial infarction
- TC:
-
total cholesterol
- CRP:
-
C-reactive protein
- Cr:
-
creatinine
- SUA:
-
serum uric acid
- FBG:
-
fasting blood-glucose
- ROC:
-
receiver-operating characteristic
- PCI:
-
percutaneous coronary intervention
- ACEI:
-
angiotensin converting enzyme inhibitor
- ARB:
-
angiotensin receptor blocker, CCB:calcium channel blockers
- AUC:
-
area under the curve
- CVH:
-
cardiovascular health
- CAC:
-
coronary artery calcium
- CAD:
-
cardiovascular disease
- CCTA:
-
coronary computed tomography angiography
References
Lawler PR, Kotrri G, Koh M, et al. Real-world risk of cardiovascular outcomes associated with hypertriglyceridaemia among individuals with atherosclerotic cardiovascular disease and potential eligibility for emerging therapies. Eur Heart J. 2020;41(1):86–94. https://doi.org/10.1093/eurheartj/ehz767.
Toth PP, Philip S, Hull M, Granowitz C. Association of elevated triglycerides with increased Cardiovascular Risk and direct costs in statin-treated patients. Mayo Clin Proc. 2019;94(9):1670–80. https://doi.org/10.1016/j.mayocp.2019.03.028.
Bo MS, Cheah WL, Lwin S, Moe Nwe T, Win TT, Aung M. Understanding the relationship between Atherogenic Index of plasma and Cardiovascular Disease Risk factors among staff of an University in Malaysia. J Nutr Metab. 2018;2018:7027624. https://doi.org/10.1155/2018/7027624.
Dobiásová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index: correlation with lipoprotein particle size and esterification rate in apob-lipoprotein-depleted plasma (FER(HDL)). Clin Biochem. 2001;34(7):583–8. https://doi.org/10.1016/s0009-9120(01)00263-6.
Dobiásová M. AIP–atherogenic index of plasma as a significant predictor of cardiovascular risk: from research to practice. Vnitr Lek. 2006;52(1):64–71.
Quispe R, Manalac RJ, Faridi KF, et al. Relationship of the triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio to the remainder of the lipid profile: the very large database of Lipids-4 (VLDL-4) study. Atherosclerosis. 2015;242(1):243–50. https://doi.org/10.1016/j.atherosclerosis.2015.06.057.
Ivanova EA, Myasoedova VA, Melnichenko AA, Grechko AV, Orekhov AN. Small dense low-density lipoprotein as Biomarker for atherosclerotic Diseases. Oxid Med Cell Longev. 2017;2017:1273042. https://doi.org/10.1155/2017/1273042.
Vergès B. Pathophysiology of diabetic dyslipidaemia: where are we? Diabetologia. 2015;58(5):886–99. https://doi.org/10.1007/s00125-015-3525-8.
Wang C, Du Z, Ye N, et al. Using the Atherogenic Index of plasma to Estimate the prevalence of ischemic stroke within a General Population in a rural area of China. Biomed Res Int. 2020;2020:7197054. https://doi.org/10.1155/2020/7197054.
Zhou K, Qin Z, Tian J, Cui K, Yan Y, Lyu S. The Atherogenic Index of plasma: a powerful and Reliable Predictor for Coronary Artery Disease in patients with type 2 diabetes. Angiology. 2021;72(10):934–41. https://doi.org/10.1177/00033197211012129.
American Diabetes Association. Diagnosis and classification of diabetes mellitus [published correction appears in Diabetes Care. 2010;33(4):e57]. Diabetes Care. 2010;33 Suppl 1Suppl 1:S62–9. https://doi.org/10.2337/dc10-S062.
Haffner SM, Stern MP, Hazuda HP, Mitchell BD, Patterson JK. Cardiovascular risk factors in confirmed prediabetic individuals. Does the clock for coronary heart disease start ticking before the onset of clinical diabetes? JAMA. 1990;263(21):2893–8. https://doi.org/10.1001/jama.263.21.2893.
Zhu X, Chen Z, Yang P, Liu L, Wu L, Wang Y. The association of subclinical atherosclerosis with prediabetes is stronger in people with dyslipidaemia than in those with normoglycaemia: a cross-sectional study in chinese adults. Prim Care Diabetes. 2020;14(6):760–7. https://doi.org/10.1016/j.pcd.2020.07.007.
Reyes-Ferrada W, Solis-Urra P, Plaza-Díaz J, et al. Cardiorespiratory Fitness, Physical Activity, Sedentary Time and its Association with the Atherogenic Index of plasma in chilean adults: influence of the Waist circumference to height ratio. Nutrients. 2020;12(5):1250. https://doi.org/10.3390/nu12051250.
American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Suppl 1):15–S33. https://doi.org/10.2337/dc21-S002.
Yao H, Guo Q, Cheng Y, Zhu T, Ma Q, Zhou Y. Predictors and morphological properties of culprit healed plaques in patients with angina pectoris. Clin Cardiol. 2022;45(12):1199–210. https://doi.org/10.1002/clc.23896.
Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the management of Acute Coronary Syndromes in patients presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267–315. https://doi.org/10.1093/eurheartj/ehv320.
Edwards MK, Blaha MJ, Loprinzi PD. Influence of sedentary behavior, physical activity, and cardiorespiratory fitness on the atherogenic index of plasma. J Clin Lipidol. 2017;11(1):119–25. https://doi.org/10.1016/j.jacl.2016.10.014.
Mazidi M, Katsiki N, Mikhailidis DP, Banach M. Association of ideal cardiovascular health metrics with serum uric acid, inflammation and atherogenic index of plasma: a population-based survey. Atherosclerosis. 2019;284:44–9. https://doi.org/10.1016/j.atherosclerosis.2018.09.016.
Edwards M, Loprinzi P. The Dose-Response Association between reported moderate to vigorous intensity physical activity and atherogenic index of plasma: NHANES, 1999–2006. J Phys Act Health. 2019;16(5):368–70. https://doi.org/10.1123/jpah.2016-0389.
Li Z, Huang Q, Sun L, Bao T, Dai Z. Atherogenic index in type 2 diabetes and its relationship with chronic microvascular complications. Int J Endocrinol. 2018;2018:1765835. https://doi.org/10.1155/2018/1765835.
Zhu XW, Deng FY, Lei SF. Meta-analysis of Atherogenic Index of plasma and other lipid parameters in relation to risk of type 2 diabetes mellitus. Prim Care Diabetes. 2015;9(1):60–7. https://doi.org/10.1016/j.pcd.2014.03.007.
Pourfarzam M, Zadhoush F, Sadeghi M. The difference in correlation between insulin resistance index and chronic inflammation in type 2 diabetes with and without metabolic syndrome. Adv Biomed Res. 2016;5:153. https://doi.org/10.4103/2277-9175.188489.
Zhang X, Zhang X, Li X, Feng J, Chen X. Association of metabolic syndrome with atherogenic index of plasma in an urban chinese population: a 15-year prospective study. Nutr Metab Cardiovasc Dis. 2019;29(11):1214–9. https://doi.org/10.1016/j.numecd.2019.07.006.
Moussavi Javardi MS, Madani Z, Movahedi A, Karandish M, Abbasi B. The correlation between dietary fat quality indices and lipid profile with atherogenic index of plasma in obese and non-obese volunteers: a cross-sectional descriptive-analytic case-control study. Lipids Health Dis. 2020;19(1):213. https://doi.org/10.1186/s12944-020-01387-4.
NIH Consensus conference. Triglyceride, high-density lipoprotein, and coronary heart disease. NIH Consensus Development Panel on Triglyceride, High-Density Lipoprotein, and Coronary Heart Disease. JAMA. 1993;269(4):505–510.
Wu TT, Gao Y, Zheng YY, Ma YT, Xie X. Atherogenic index of plasma (AIP): a novel predictive indicator for the coronary artery disease in postmenopausal women. Lipids Health Dis. 2018;17(1):197. https://doi.org/10.1186/s12944-018-0828-z.
Kawakami A, Aikawa M, Alcaide P, Luscinskas FW, Libby P, Sacks FM. Apolipoprotein CIII induces expression of vascular cell adhesion molecule-1 in vascular endothelial cells and increases adhesion of monocytic cells. Circulation. 2006;114(7):681–7. https://doi.org/10.1161/CIRCULATIONAHA.106.622514.
Huang Y, Hu Y, Mai W, et al. Plasma oxidized low-density lipoprotein is an independent risk factor in young patients with coronary artery disease. Dis Markers. 2011;31(5):295–301. https://doi.org/10.3233/DMA-2011-0832.
Jacob RF, Walter MF, Self-Medlin Y, Mason RP. Atorvastatin active metabolite inhibits oxidative modification of small dense low-density lipoprotein. J Cardiovasc Pharmacol. 2013;62(2):160–6. https://doi.org/10.1097/FJC.0b013e318294998d.
Tan MH, Johns D, Glazer NB. Pioglitazone reduces atherogenic index of plasma in patients with type 2 diabetes. Clin Chem. 2004;50(7):1184–8. https://doi.org/10.1373/clinchem.2004.031757.
Dobiásová M, Urbanová Z, Samánek M. Relations between particle size of HDL and LDL lipoproteins and cholesterol esterification rate. Physiol Res. 2005;54(2):159–65.
Cai G, Shi G, Xue S, Lu W. The atherogenic index of plasma is a strong and independent predictor for coronary artery disease in the chinese Han population. Med (Baltim). 2017;96(37):e8058. https://doi.org/10.1097/MD.0000000000008058.
Nam JS, Kim MK, Nam JY, et al. Association between atherogenic index of plasma and coronary artery calcification progression in korean adults. Lipids Health Dis. 2020;19(1):157. https://doi.org/10.1186/s12944-020-01317-4.
Won KB, Han D, Lee JH, et al. Atherogenic index of plasma and coronary artery calcification progression beyond traditional risk factors according to baseline coronary artery calcium score. Sci Rep. 2020;10(1):21324. https://doi.org/10.1038/s41598-020-78350-x.
Won KB, Heo R, Park HB, et al. Atherogenic index of plasma and the risk of rapid progression of coronary atherosclerosis beyond traditional risk factors. Atherosclerosis. 2021;324:46–51. https://doi.org/10.1016/j.atherosclerosis.2021.03.009.
Edwards MK, Blaha MJ, Loprinzi PD. Atherogenic index of plasma and Triglyceride/High-Density lipoprotein cholesterol ratio Predict Mortality Risk Better Than individual cholesterol risk factors, among an older Adult Population. Mayo Clin Proc. 2017;92(4):680–1. https://doi.org/10.1016/j.mayocp.2016.12.018.
Sadeghi M, Heshmat-Ghahdarijani K, Talaei M, Safaei A, Sarrafzadegan N, Roohafza H. The predictive value of atherogenic index of plasma in the prediction of cardiovascular events; a fifteen-year cohort study. Adv Med Sci. 2021;66(2):418–23. https://doi.org/10.1016/j.advms.2021.09.003.
Rizza S, Longo S, Piciucchi G, et al. Carotid intimal medial thickness in rotating night shift is related to IL1β/IL6 axis. Nutr Metab Cardiovasc Dis. 2020;30(10):1826–32. https://doi.org/10.1016/j.numecd.2020.05.028.
Won KB, Jang MH, Park EJ, et al. Atherogenic index of plasma and the risk of advanced subclinical coronary artery disease beyond traditional risk factors: an observational cohort study. Clin Cardiol. 2020;43(12):1398–404. https://doi.org/10.1002/clc.23450.
Fu L, Zhou Y, Sun J, et al. Atherogenic index of plasma is associated with major adverse cardiovascular events in patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2021;20(1):201. https://doi.org/10.1186/s12933-021-01393-5.
Kim JJ, Yoon J, Lee YJ, Park B, Jung DH. Predictive value of the Atherogenic Index of plasma (AIP) for the risk of Incident Ischemic Heart Disease among non-diabetic Koreans. Nutrients. 2021;13(9):3231. https://doi.org/10.3390/nu13093231.
Shi Y, Wen M. Sex-specific differences in the effect of the atherogenic index of plasma on prediabetes and diabetes in the NHANES 2011–2018 population. Cardiovasc Diabetol. 2023;22(1):19. Published 2023 Jan 30. https://doi.org/10.1186/s12933-023-01740-8.
Keerthi GS, Pal P, Pal GK, Sahoo JP, Sridhar MG, Balachander J. Attenuated baroreflex sensitivity in normotensive prediabetes and diabetes in indian adults. Endocr Res. 2016;41(2):89–97. https://doi.org/10.3109/07435800.2015.1076454.
Mahat RK, Singh N, Rathore V, Gupta A, Shah RK. Relationship between Atherogenic Indices and Carotid Intima-Media Thickness in Prediabetes: A Cross-Sectional Study from Central India. Med Sci (Basel). 2018;6(3):55. Published 2018 Jul 5. https://doi.org/10.3390/medsci6030055.
El-Eshmawy MM, Gad DF, El-Baiomy AA. Elevated serum levels of Ischemia Modified Albumin and Malondialdehyde are related to Atherogenic Index of plasma in a cohort of Prediabetes. Endocr Metab Immune Disord Drug Targets. 2020;20(8):1347–54. https://doi.org/10.2174/1871530320666200503052226.
Park DW, Kang DY, Ahn JM, et al. Routine functional testing or Standard Care in High-Risk patients after PCI. N Engl J Med. 2022;387(10):905–15. https://doi.org/10.1056/NEJMoa2208335.
Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stable coronary disease. N Engl J Med. 2020;382(15):1395–407. https://doi.org/10.1056/NEJMoa1915922.
Acknowledgements
We thank all our colleagues at the department of Cardiology, Beijing Anzhen Hospital, Capital Medical University.
Funding
This study was supported by the grant from Natural Science Foundation of Beijing, China (Grant No. 7214223) and Beijing Hospitals Authority Youth Programme (Grant No. QML20210601) to QG. YZ was supported by National Key Research and Development Program of China (2017YFC0908800), Beijing Municipal Health Commission (Grant No. PXM2020_026272_000002 and Grant No. PXM2020_026272_000014) and Natural Science Foundation of Beijing, China (Grant No. 7212027).
Author information
Authors and Affiliations
Contributions
This study was completed in collaboration with the following authors: GQY and ZYJ defined the study theme and methods. LY, FXX and YJQ analyzed the data. LY and FXX wrote the paper. ZB and ZGY edited the paper. All authors read and approved the final manuscript. Yang Liu and Xunxun Feng were contributed equally to the article as the first authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study adhered to the tenants of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of Anzhen Hospital. All patients provided written informed consent for participation in the present study. The data retrospectively obtained from electronic medical records which provided real and effective data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, Y., Feng, X., Yang, J. et al. The relation between atherogenic index of plasma and cardiovascular outcomes in prediabetic individuals with unstable angina pectoris. BMC Endocr Disord 23, 187 (2023). https://doi.org/10.1186/s12902-023-01443-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01443-x