
Abstract
Background
Eosinophilic cystitis (EC) is a rare inflammatory disease characterized by the gathering and infiltration of numerous eosinophilia (EOS) in the bladder wall. Because of Few cases of EC have been reported globally, the epidemiology of EC is not well known. We report herein the details of one very scarce case of large tumor-like eosinophilic cystitis complicated with cystitis glandularis (CG) diagnosed by biopsy.
Case presentation
A 45-year-old Chinese man was referred to our hospital for the treatment of right lumbago and odynuria. Ultrasound examination indicated the low echo on the right portion wall and the neck of the bladder. Computed tomography showed a remarkable enhancing large mass that measured 5.0 cm × 2.3 cm located on the right portion of the bladder with undefined margin. For further treatment, diagnostic transurethral resection of the bladder was performed, the postoperative histopathological diagnosis was EC complicated with CG. After transurethral resection, antibiotics, glucocorticoids, and antihistamines were treated. The patient recovered uneventfully and was discharged on postoperative day 8 without evidence of recurrence followed-up for 6 months.
Conclusion
Large tumor-like eosinophilic cystitis complicated with cystitis glandularis is rare, malignant tumors need to be ruled out. We deem that prompt biopsy led to the exact diagnosis, appropriate treatment led to better prognosis.
Similar content being viewed by others


Background
EC is a scarce inflammatory disease of the bladder, first presented in 1960 by Brown [1]. Because of the small number of patients suffer from EC, only about Two hundred cases of EC have been described, the etiology and pathogenesis of EC is not well understood, treatment modalities are not agreed upon. Most EC patients present with mucosal lesions of the bladder, only few studies have described mass-forming or malignancy-mimicking EC. As far as we know, there is no literature published about EC complicated with cystitis glandularis. The report of this case brings a guide for doctors to comprehend EC complicated with CG.
Case presentation
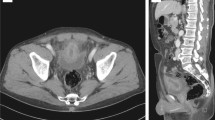
A 45-year-old Chinese man was referred to our hospital for the treatment of right lumbago and odynuria, with no fever or gross hematuria. His past medical history was unremarkable and there was no history of any allergy or external trauma except a long working history in construction site. On admission, no abnormality was found in physical examination, Blood analyses revealed no leukocytosis (white blood cell count of 6.52 × 109/L), no elevation of eosinophils (eosinophils count of 0.44 × 109/L, eosinophil ratio Accounted for 6.7%). Renal function was normal (Serum creatinine level of 77.4 umol/L). Urinalysis confirmed no hematuria, leucocytes or protein. Ultrasound examination indicated the low echo on the right portion wall and the neck of the bladder, with dilation of the right lower ureter (Fig. 1A, B). Computed tomography showed no hydronephrsisa but a remarkable enhancing large mass that measured 5.0 cm × 2.3 cm located on the right portion of the bladder with undefined margin (Fig. 1C). Cystoscopy confirmed a huge follicle-like mass lesion on the right portion wall and the neck of the bladder with a broad base, in which blood vessels growing (Fig. 2). Cystoscopic biopsy affirmed the chronic mucosal inflammation of bladder (Fig. 3A, B). For further treatment, diagnostic transurethral resection of the bladder was performed, the postoperative histopathological diagnosis was EC complicated with CG (Fig. 3C). After transurethral resection, antibiotics, glucocorticoids, and antihistamines were treated, the catheter was indwelled continuously until postoperative day 6. The patient recovered uneventfully and was discharged on postoperative day 8. Cystoscopy and eosinophils levels of blood and urine were required to be examined every 3 months during the first year. There was no evidence of recurrence followed up for 6 months.

Ultrasound examination. A Low echo on the right portion wall of the bladder. B Low echo on the neck of the bladder; C a remarkable enhancing large mass on the right portion of the bladder with undefined margin

Cystoscopy showed a huge follicle-like mass lesion on the right portion wall and the neck of the bladder with a broad base

The histopathological diagnosis. A, B Cystoscopic biopsy affirmed the chronic mucosal inflammation of bladder; C numerous eosinophils per high power field of view and Brunn nests existed
Discussion and conclusion
In contrast with other cystitis, EC is a scarce inflammatory disease with low incidence, only about Two hundred cases of EC have been described globally. Among the 135 cases, the age of EC patients ranged from 5 to 87 years old, with an average age of 41.6 years old and no gender difference [2]. EC is thought to be associated with BRAFI463T gene mutation [3], which may lead to molecular defects of haematopoietic stem cells or myeloid cell. Sanaphylaxis caused by a variety of physical, chemical, biological and pathological factors is involved in the pathogenesis of EC, one-third of case’s cause still not found [4]. Such as parasites, dust, bladder injury, food and drug allergy, these antigens can cause an immunoglobulin E-mediated release of eosinophilic chemotactic factor which would ultimately lead to tissue damaged by releasing lysosomal enzymes and cytokines [5]. For the above reasons, we speculated that this patient was related to his long history of working in construction site. In addition, peripheral eosinophilia was not observed in this case, hypereosinophilia was not considered.
Peripheral eosinophilia is detected in about 43% of cases [2], more than half of cases without significantly elevation of peripheral eosinophilia. Eosinophils are rarely shed and degrade rapidly in urine, therefore urinalysis usually reveals proteinuria, microscopic haematuria, pyuria [6], only rare cases with eosinophiluria. Bladder irritation was the main manifestation of most EC patients, with frequency (67%) and dysuresia (62%) [2]. The main manifestation of our patient was right lumbago and odynuria, which may owning to the huge follicle-like mass lesion on the right portion wall and the neck of the bladder. It is suggested that not all bladder irritation or abnormal urinalysis could be found in EC cases. Imaging examinations are not helpful in determining those present as diffuse or irregular thickening of the bladder wall, or as nodular or huge masses. There was no characteristic manifestations with EC. Tumor-mimicking masses, polyps, follicles, ulcers, mucosal edema, hyperemia and erythema have all been reported. The large tumor-mimicking masses like our case was relatively rare and easily misdiagnosed. Eventually, pathological biopsy is needed, more than 25 eosinophils per high power field of view can be diagnosed with EC [7]. Significantly elevation of peripheral eosinophilia with the mucosa and submucosa was seriously involved in acute stage of EC, chronic mucosal inflammation was usually observed in chronic stage [8], which may the reason why cystoscopic biopsy affirmed the chronic mucosal inflammation of bladder with no eosinophilia founded in this patient.
Few literatures was reported on EC complicated with other disease. We report herein the case of large mass-forming EC complicated with CG diagnosed by biopsy. CG is a inflammatory disease with a low incidence, which characterized by the Brunn nests existed in the lamina propria of bladder stimulated by inflammation, obstruction and stone [9]. CG with large-area follicle-like and papillomatoid changes was classified as high-risk type, which with the risk of malignant transformation [10]. For patients with tumour-like masses, we speculate that EC and CG may mutually aggravate the progression of the disease, but whether EC would complicated with CG or malignancy tumor is unknown.
There is no consensus on the treatment of EC, medical treatments such as glucocorticoids, antihistamines, and antibiotics can be regarded as the initial treatment [11]. The recurrence of those patient who treated with medicine was 17%, whereas that was only 2.6% who treated with surgery [2]. For our patient, diagnostic transurethral resection of the bladder was performed, after that, antibiotics, glucocorticoids, and antihistamines were treated. Surgery is recommended for the treatment of those with large tumor-like or follicle-like lesions [10]. The patient recovered uneventfully without evidence of recurrence, which revealed that surgical treatment was preferred for large tumor-like EC complicated with CG.
Taken together, large tumor-like eosinophilic cystitis complicated with cystitis glandularis is rare, malignant tumors need to be ruled out. We deem that prompt biopsy led to the exact diagnosis, appropriate treatment led to better prognosis.
Availability of data and materials
All relevant data and materials are included in this article.
Abbreviations
- EC:
-
Eosinophilic cystitis
- EOS:
-
Eosinophilia
- CG:
-
Cystitis glandularis
References
Brown EW. Eosinophilic granuloma of the bladder. J Urol. 1960;83:665–8.
van DEN Ouden D. Diagnosis and management of eosinophilic cystitis: a pooled analysis of 135 cases. Eur Urol. 2000;37(4):386–94.
Choi MY, Tsigelny IF, Boichard A, et al. BRAF mutation as a novel driver of eosinophilic cystitis. Cancer Biol Ther. 2017;18(9):655–9.
Li G, Cai B, Song H, et al. Clinical and radiological character of eosinophilic cystitis. Int J Clin Exp Med. 2015;8(1):533–9.
Galutira PJT, Canonigo BB, Cabansag MRF, et al. Presenting manifestations of eosinophilic cystitis in two Filipino children. Int Urol Nephrol. 2010;42(3):557–63.
Kumar S, Sharma V, Ganesamoni R, Singh S. Eosinophilic cystitis mimicking tuberculosis: an analysis of five cases with review of literature. Urol Ann. 2013;5(1):50–2.
Zhou AG, Amin A, Yates JK, et al. Mass forming eosinophilic cystitis in pediatric patients. Urology. 2017;101:139–41.
Kim MS, Park H, Park CS, et al. Eosinophilic cystitis associated with eosinophilic enterocolitis: case reports and review of the literature. Br J Radiol. 2010;83(990):e122–5.
Lancelin F, Anidjar M, Villette JM, et al. Telomerase activity as apotential maker in preneoplastic bladder lesions. BJU Int. 2000;85(4):526–31.
Chinese Urology Association. Chinese expert consensus on clinical diagnosis and treatment of glandular cystitis. Clin J Urol. 2020;41(8):566–8.
Werbrouck C, Marrannes J, Verhamme L, et al. Eosinophilic cystitis mimicking bladder tumor. JBR-BTR. 2014;97(6):375.
Acknowledgements
Not applicable.
Funding
Nil.
Author information
Authors and Affiliations
Contributions
JBY and QC completed the initial manuscript and revision. KZ, XBL and KFD has participated in writing the part of diagnosis and differential diagnosis in this paper, offered valuable advice on the revised the manuscript. JH and RC looked up the references. QC, the corresponding author, Provided ideas for research and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of First People's Hospital of Zigong City. We have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal.
Consent for publication
Written informed consent was attained from the study participants for publication of this Case Report and any accompanying images.
Competing interests
There are no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ye, J.B., Chen, Q., Zeng, K. et al. Eosinophilic cystitis complicated with cystitis glandularis: a case report. BMC Urol 22, 55 (2022). https://doi.org/10.1186/s12894-022-01007-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12894-022-01007-6