
Abstract
Background
The powered circular stapler, which was developed with the aim of providing reliable and reproducible anastomosis, provides complete anastomosis, resulting in a reduced risk of anastomotic leakage. The aim of this study was to compare the incidence of anastomotic leakage between a conventional manual circular stapler (MCS) and the ECHELON CIRCULAR™ Powered Stapler (ECPS) in patients with left-sided colorectal cancer who underwent anastomosis with the double stapling technique.
Methods
A total of 187 patients with left-sided colorectal cancer who underwent anastomosis with the double stapling technique with a conventional MCS or the ECPS during surgery at Osaka City University Hospital between January 2016 and July 2022 were enrolled in this study.
Results
The incidence of anastomotic leakage in the ECPS group was significantly lower than that in the MCS group (4.4% versus 14.3%, p = 0.048). Furthermore, even after propensity score matching, an association was found between the use of the ECPS and a reduced incidence of anastomotic leakage.
Conclusion
The ECPS has the potential to help reduce the rate of anastomotic leakage in left-sided colorectal surgery.
Similar content being viewed by others


Background
Due to advances in surgical techniques and improvements in surgical devices, postoperative complications in digestive surgery have decreased [1]. However, anastomotic leakage remains a serious complication in colorectal surgery and continues to be a concern for colorectal surgeons. Anastomotic leakage can worsen not only short-term outcomes, such as the rate of reoperation and duration of hospitalization but also oncological outcomes, such as the rate of recurrence and survival time [2,3,4]. Furthermore, anastomotic leakage has a negative impact on economic outcomes [1, 5].
Intraoperative factors, such as intestinal perfusion, tension and incomplete anastomosis, have been reported to affect the incidence of anastomotic leakage [6,7,8], in addition to patient background factors, such as sex, body mass index (BMI), diabetes, tumor diameter, distance from anal verge, American Society of Anesthesiologists (ASA) physical status and neoadjuvant chemoradiotherapy [9,10,11]. In addition to the reinforcement of anastomosis, such as additional sutures and the use of a polyglycolic acid (PGA) sheet [12, 13], we focused on a powered circular stapler, the ECHELON CIRCULAR™ Powered Stapler (ECPS) (Ethicon, Somerville, NJ, USA), which was launched in Japan in 2020, as a measure against incomplete anastomosis. This powered circular stapler was developed with the aim of providing reliable and reproducible anastomosis [14]. The use of this new device provides complete anastomosis, resulting in a reduced risk of anastomotic leakage.
The aim of this study was to compare the incidence of anastomotic leakage between a conventional manual circular stapler (MCS) and the ECPS in patients with left-sided colorectal cancer who underwent anastomosis with the double stapling technique (DST).
Methods
Patients
A total of 187 patients with left-sided colorectal cancer who underwent DST anastomosis with a conventional MCS, the ENDOPATH ENDOSCOPIC INTRALUMINAL STAPLER (Ethicon, Somerville, NJ, USA) or the ECPS during surgery at Osaka City University Hospital between January 2016 and July 2022 were enrolled in this study. An expert in colorectal surgery participated in all surgeries. There was no operator bias in the use of circular staplers. High ligation of the inferior mesenteric artery was performed in all cases. Indocyanine green fluorescence imaging was performed to evaluate blood perfusion in patients who underwent surgery after June 2017. Mobilization of the splenic flexure was performed when tension at the anastomotic site was noted. Reinforcement of anastomosis, such as additional sutures and/or a PGA sheet, was added according to the judgment of the surgeon.
Definition of anastomotic leakage
Anastomotic leakage was defined as the extravasation observed on radiologic examinations. Upon clinical symptoms that suggested anastomotic leakage, such as abdominal pain, high fever, pus or fecal discharge from the pelvic drain, or leukocytosis, computed tomography (CT) was performed to confirm the presence of anastomotic leakage. The following CT findings were considered suggestive of anastomotic leakage: abscess, fluid collection, or air bubbles surrounding the anastomotic site. Water-soluble contrast enema was also performed as needed to confirm the presence of communication between the intra- and extraluminal compartments.
Ethics statement
This retrospective study was approved by the Ethics Committee of Osaka City University (approval number: 4182) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients.
Statistical analyses
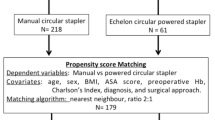
All statistical analyses were performed using the SPSS software package for Windows (IBM, Chicago, IL, USA). The significance of differences according to the circular stapler that was used and the patients’ background/operative outcomes were analyzed using the chi-squared test, Fisher’s exact test, and the Mann–Whitney U test. A logistic regression model was used to evaluate the factors associated with anastomotic leakage. P values < 0.05 were considered to indicate a statistically significant difference. To reduce the impact of selection bias and potential confounding, we performed propensity score matching. The propensity scores were estimated using multivariate logistic regression models, with the groups as the dependent variable and patient characteristics and operative outcomes as covariates. Matching was performed with a one-to-one greedy nearest neighbor algorithm with a caliper of 0.2 without replacement.
Results
The MCS was used in 119 cases (MCS group), and the ECPS was used in 68 cases (ECPS group). Associations between the type of circular stapler and the patients’ characteristics/operative outcomes are summarized in Table 1. The ECPS was significantly associated with nonsmokers, lower BMI, a higher proportion of robot-associated surgery and smaller circular staplers and tended to be associated with lower rectal cancer. Associations between the type of circular stapler and postoperative complications are summarized in Table 2. The incidence of anastomotic leakage in the ECPS group was significantly lower than that in the MCS group (4.4% versus 14.3%, p = 0.048). The reoperation rate in the ECPS group was lower than that in the MCS group (1.5% versus 2.5%, p > 0.999); however, the difference did not reach statistical significance due to the extremely small number of events. No patients with anastomotic bleeding were observed in the ECPS or MCS group. The associations between anastomotic leakage and various factors are shown in Table 3. According to a univariate analysis, anastomotic leakage showed significant associations with male sex, large tumor, absence of diverting ileostomy, long operation time, and manual circular stapler. Furthermore, even after propensity score matching using the three covariates of BMI, tumor location, and smoking, which have been reported to affect anastomotic leakage and which showed significant differences in patient backgrounds, the ECPS remained associated with a reduced incidence of anastomotic leakage.
Discussion
This study demonstrated that the use of the ECPS reduces the rate of anastomotic leakage in left-sided colorectal surgery, as demonstrated in previous reports [15,16,17]. To our knowledge, this is the first report from Asia to evaluate the usefulness of the ECPS for the prevention of anastomotic leakage in colorectal surgery. In this study, the ECPS group had some adverse conditions (e.g., lower anastomosis) in comparison to the MCS group. Nevertheless, the outcomes in the ECPS group were better than those in the MCS group. Furthermore, even after propensity score matching, an association was found between the use of the ECPS and a reduced incidence of anastomotic leakage. These results strongly support the usefulness of the ECPS.
The introduction of the circular stapler in colorectal surgery has greatly contributed not only to shortening the operation time but also to the establishment of stable procedures that are not affected by the skill of the surgeon and to the improvement of clinical outcomes [15]. In addition to various past improvements in circular stapler technology, the ECPS was developed based on the concept of increased strength at the anastomotic site, a gentler approach to the tissue, minimization of variation in usage and standardization of performance across users [14, 18]. The details of the improvements are as follows.
First, the powered stapling system, which is operated by electricity, was introduced [17]. Since MCS requires a strong force to fire, movement at the distal tip becomes large when using MCS, especially when performed by a surgeon with small hands or insufficient grip strength [17, 19]. Therefore, MCS may cause suboptimal tension on the tissue at the anastomotic site, which may cause microtissue damage, leading to anastomotic trouble [19,20,21]. On the other hand, the ECPS requires less force to fire. Therefore, movement at the distal tip can be reduced, resulting in a reduction in suboptimal tissue tension at the anastomotic site and providing more stable stapler positioning and staple line formation [14, 15, 17,18,19].
Second, 3D stapling technology has been newly introduced. Although the staple array of the ECPS is 2 rows, the same as the MCS, the area covered by one staple of the ECPS is increased in comparison to the MCS due to the use of a 3D staple shape that compresses the tissue widely and sterically [15, 19]. As a result, the physical pressure resistance increases in comparison to the MCS. Although it is unclear whether there is a direct correlation between physical pressure resistance and the rate of anastomotic leakage, it is an undeniable fact that the use of the ECPS dramatically reduced the rate of anastomotic leakage in several previous reports [15,16,17]. Furthermore, it has been reported that improved staple formation contributes to the prevention of bleeding at the anastomotic site as well as anastomotic leakage [14].
Third, Gripping Surface Technology (GST), which provides gentler handling with precise compression only where it is needed, has also been introduced [15]. This improvement minimizes tissue damage, resulting in a 33% reduction in compressive force on tissue.
As described above, the ECPS has been improved in various points in comparison to the MCS. Nevertheless, the increase in selling price is set to be mild. Thus, the ECPS may account for most of the circular stapler market share in the near future.
In this study, small-diameter circular staplers were more frequently used in the ECPS group than in the MCS group. The reason for this is the recent increase in the use of smaller-sized circular staplers, based on the hypothesis that the use of circular staplers of smaller diameter may reduce the overstretching of tissue, resulting in less anastomotic trouble. However, the size of the circular stapler was not associated with the incidence of anastomotic leakage, as documented in a previous report [22].
In the current study, anastomotic leakage was observed in three patients in the ECPS group. All three patients had lower anastomosis and required a long operation time of ≥ 9 h. In addition, the tumor diameter was ≥ 7 cm in 2 of these 3 cases. Given these facts, there may have been invisible damage to the intestinal tract in these three patients who developed anastomotic leakage.
The present study is associated with several limitations. First, this was a retrospective study with a small cohort in a single center. Based on previous reports on medical statistics [23, 24], we abandoned the multivariate analysis with a Cox proportional hazards model for anastomotic leakage due to an insufficient total number of events. Instead, propensity score matching was performed to reduce the impact of selection bias and potential confounding factors. However, due to the small number of cases, the relationship between the reduced incidence of anastomotic leakage and the use of the ECPS showed a trend but did not reach statistical significance. Large prospective studies should be performed to confirm our findings. Second, additional reinforcement may have the potential to have some impact on the rate of anastomotic leakage, although there was no statistically significant correlation in this study because additional reinforcement tended to be omitted in patients with a low risk of anastomotic leakage. Third, the ECPS, which was launched in recent years, was more frequently used in robot-assisted surgery in comparison to the MCS due to historical backdrop. However, it has been reported that robot-assisted surgery and laparoscopic surgery are comparable in terms of postoperative complications [25].
Conclusion
In conclusion, the ECPS has the potential to help reduce the rate of anastomotic leakage in left-sided colorectal surgery.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
body mass index
- ASA:
-
American Society of Anesthesiologists
- PGA:
-
polyglycolic acid
- ECPS:
-
ECHELON CIRCULAR™ Powered Stapler
- MCS:
-
manual circular stapler
- DST:
-
double-stapling technique
- CT:
-
computed tomography
- N/A:
-
not applicable
References
Boccola MA, Buettner PG, Rozen WM, Siu SK, Stevenson AR, Stitz R, Ho YH. Risk factors and outcomes for anastomotic leakage in colorectal surgery: a single-institution analysis of 1576 patients. World J Surg. 2011;35:186–95.
Wang S, Liu J, Wang S, Zhao H, Ge S, Wang W. Adverse Effects of Anastomotic Leakage on local recurrence and Survival after curative anterior resection for rectal Cancer: a systematic review and Meta-analysis. World J Surg. 2017;41:277–84.
Bashir Mohamed K, Hansen CH, Krarup PM, Fransgård T, Madsen MT, Gögenur I. The impact of anastomotic leakage on recurrence and long-term survival in patients with colonic cancer: a systematic review and meta-analysis. Eur J Surg Oncol. 2020;46:439–47.
Bell SW, Walker KG, Rickard MJ, Sinclair G, Dent OF, Chapuis PH, Bokey EL. Anastomotic leakage after curative anterior resection results in a higher prevalence of local recurrence. Br J Surg. 2003;90:1261–6.
Hammond J, Lim S, Wan Y, Gao X, Patkar A. The burden of gastrointestinal anastomotic leaks: an evaluation of clinical and economic outcomes. J Gastrointest Surg. 2014;18:1176–85.
Sciuto A, Merola G, De Palma GD, Sodo M, Pirozzi F, Bracale UM, Bracale U. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J Gastroenterol. 2018;24:2247–60.
Qu H, Liu Y, Bi DS. Clinical risk factors for anastomotic leakage after laparoscopic anterior resection for rectal cancer: a systematic review and meta-analysis. Surg Endosc. 2015;29:3608–17.
Parthasarathy M, Greensmith M, Bowers D, Groot-Wassink T. Risk factors for anastomotic leakage after colorectal resection: a retrospective analysis of 17 518 patients. Colorectal Dis. 2017;19:288–98.
Braunschmid T, Hartig N, Baumann L, Dauser B, Herbst F. Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate. Surg Endosc. 2017;31:5318–26.
Docherty JG, McGregor JR, Akyol AM, Murray GD, Galloway DJ. Comparison of manually constructed and stapled anastomoses in colorectal surgery. West of Scotland and Highland Anastomosis Study Group.Ann Surg. 1995; 221: 176–84.
Watanabe J, Ishibe A, Suwa Y, Suwa H, Ota M, Kunisaki C, Endo I. Indocyanine green fluorescence imaging to reduce the risk of anastomotic leakage in laparoscopic low anterior resection for rectal cancer: a propensity score-matched cohort study. Surg Endosc. 2020;34:202–8.
Maeda K, Nagahara H, Shibutani M, Ohtani H, Sakurai K, Toyokawa T, Muguruma K, Tanaka H, Amano R, Kimura K, Sugano K, Ikeya T, Iseki Y, Hirakawa K. Efficacy of intracorporeal reinforcing sutures for anastomotic leakage after laparoscopic surgery for rectal cancer. Surg Endosc. 2015;29:3535–42.
Shibutani M, Nagahara H, Fukuoka T, Iseki Y, Okazaki Y, Hirakawa K, Ohira M. Prevention of anastomotic leakage using a polyglycolic acid sheet in double-stapling technique anastomosis for rectal surgery. Ann Med Surg (Lond). 2021;72:103117.
Rojatkar P, Henderson CE, Hall S, Jenkins SA, Paulin-Curlee GG, Clymer JW. DA Nagle. A novel powered circular stapler designed for creating secure anastomoses. Med Devices Diagn Eng. 2017;2:94–100.
Pla-Martí V, Martín-Arévalo J, Moro-Valdezate D, García-Botello S, Mora-Oliver I, Gadea-Mateo R, Cozar-Lozano C, Espí-Macías A. Impact of the novel powered circular stapler on risk of anastomotic leakage in colorectal anastomosis: a propensity score-matched study. Tech Coloproctol. 2021;25:279–84.
Herzig DO, Ogilvie JW, Chudzinski A, Ferrara A, Ashraf SQ, Jimenez-Rodriguez RM, Van der Speeten K, Kinross J, Schimmelpenning H, Sagar PM, Cannon JA, Schwiers ML, Singleton DW, Waggoner JR, Fryrear R 2nd, Sylla P. Assessment of a circular powered stapler for creation of anastomosis in left-sided colorectal surgery: a prospective cohort study. Int J Surg. 2020;84:140–6.
Sylla P, Sagar P, Johnston SS, Dwarakanathan HR, Waggoner JR, Schwiers M, Roy S. Outcomes associated with the use of a new powered circular stapler for left-sided colorectal reconstructions: a propensity score matching-adjusted indirect comparison with manual circular staplers. Surg Endosc. 2022;36:2541–53.
Mirnezami R, Soares A, Chand M. Enhancing the precision of circular stapled colorectal anastomosis: could powered stapler technology provide the solution? Tech Coloproctol. 2019;23:687–9.
Atallah S, Kural S, Banda N, Banda A, Bawaney F, Cabral F, Neychev V, Patel C, Larach S. Initial clinical experience with a powered circular stapler for colorectal anastomosis. Tech Coloproctol. 2020;24:479–86.
Offodile AC 2nd, Feingold DL, Nasar A, Whelan RL, Arnell TD. High incidence of technical errors involving the EEA circular stapler: a single institution experience. J Am Coll Surg. 2010;210:331–5.
Kono E, Tomizawa Y, Matsuo T, Nomura S. Rating and issues of mechanical anastomotic staplers in surgical practice: a survey of 241 japanese gastroenterological surgeons. Surg Today. 2012;42:962–72.
Nagaoka T, Yamaguchi T, Nagasaki T, Akiyoshi T, Nagayama S, Fukunaga Y, Chino A, Ishizuka N, Konishi T. Safety of small circular Staplers in double stapling technique anastomosis for sigmoid Colon and rectal Cancer. Dis Colon Rectum. 2021;64:937–45.
Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49:1373–9.
Harrell FE. Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. New York: Springer-Verlag; 2015.
Jayne D, Pigazzi A, Marshall H, Croft J, Corrigan N, Copeland J, Quirke P, West N, Rautio T, Thomassen N, Tilney H, Gudgeon M, Bianchi PP, Edlin R, Hulme C, Brown J. Effect of robotic-assisted vs conventional laparoscopic surgery on risk of Conversion to Open Laparotomy among Patients undergoing resection for rectal Cancer: the ROLARR Randomized Clinical Trial. JAMA. 2017;318:1569–80.
Acknowledgements
We thank Brian Quinn, who edited our manuscript on behalf of JMC, Ltd.
Funding
No funding was acquired for this study.
Author information
Authors and Affiliations
Contributions
MS designed the study, performed the statistical analysis and draft the manuscript. TF, YI, HK and KK collected the clinical data and revised the manuscript critically. KM designed the study and critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research conformed to the provisions of the Declaration of Helsinki. Written informed consent was obtained from all participants. This retrospective study was approved by the Ethics Committee of Osaka City University (approval number: 4182).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shibutani, M., Fukuoka, T., Iseki, Y. et al. Impact of a circular powered stapler on preventing anastomotic leakage in patients with left-sided colorectal cancer: a retrospective study. BMC Surg 23, 205 (2023). https://doi.org/10.1186/s12893-023-02104-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-023-02104-5