
Abstract
Background
Thyroid fine needle aspiration (FNA) is the procedure of choice in the management of thyroid nodules. Acute thyroid swelling after FNA is a rare complication and is reported in a finite number of literatures. To the best of our knowledge, only seven reported cases exist in literatures. This study describes an addition case with an acute thyroid swelling after FNA, as well as puts forward a new hypothesis of this phenomenon.
Case presentation
The case is presented of a 30-year-old female with an acute thyroid swelling after FNA, with funicular hypoechoic lesions in thyroid gland. The size of thyroid was 1.5-fold enlarged in the unilateral thyroid gland. No complains of pain or other discomforts with her and no signs of hemorrhage were found along the passage of the fine needle. The episode was recovered spontaneously.
Conclusions
An acute thyroid swelling is a rare complication of FNA. A hypothesis of anaphylactic reaction was suggested in our study. Physicians should pay more attention of this phenomenon and more information is needed to support our hypothesis.
Similar content being viewed by others


Background
Thyroid fine needle aspiration (FNA) is the procedure of choice in the management of thyroid nodules. Although invasive, FNA is simple, reliable, and except for slight pain or discomfort at the site of aspiration, complications seem to be rare [1, 2]. Acute thyroid swelling is a rare complication and is reported in a finite number of literatures. Several explanations of the main reason have been suggested but cannot be clarified [3]. Here, the case is described of an acute thyroid swelling after FNA, accompanied with funicular hypoechoic lesions in thyroid gland. A new hypothesis is proposed that it is the anaphylactic reaction resulting in this phenomenon.
Case presentation
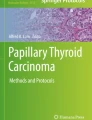
A thirty-year-old woman referred to the hospital because of nodules in her bilateral thyroid lobes. Ultrasonography showed a heterogeneously echoic (iso/hypoechoic) nodule (13 × 8 × 9 mm) with multiple microcalcifications in left lobe and a hypoechoic nodule (5 × 5 × 5 mm) in right lobe. There was neither known allergies nor use of specific medication. Before FNA, a conventional ultrasound and contrast-enhanced ultrasound was performed. 2 mL of SonoVue (Bracco, Italy) suspension (mixed by 5 mL saline and 39 mg SonoVue powder) was administered manually. Her skin of neck was sensitive to turn red after being contacted by the probe. Subsequently, 0.5 ml Lidocaine solution was applied for surface anesthesia. FNA of the nodule in the superior pole of right lobe was performed with a 23-guage needle. As soon as pulling out the needle, an obvious local swelling with multiple funicular hypoechoic lesions was observed in the inferior pole of left thyroid lobe. It lasted for only several seconds. Ten minutes later, FNA of the nodule in left thyroid lobe was performed and similar episode came out immediately after the procedure. The left thyroid lobe was swelling with multiple funicular hypoechoic lesions and enlarged to 1.5-fold increase in contrast with the size before. (Fig. 1) The targeted nodules had nothing different with before. The hypoechoic lesions faded away in thirty minutes without compression. The patient had no complains of pain and dyspnea. No signs of hemorrhage were noted along the passage of the needle. Cytologic diagnosis showed a benign one in the left thyroid lobe and atypical undetermined significance (AUS) in the right thyroid lobe.

Ultrasonography showed the left thyroid lobe was swelling with multiple funicular hypoechoic lesions
Discussion and conclusions
Acute swelling of thyroid is rare and has been reported only in a small number of literatures. It was first reported by Haas. in 1982 [4], with a nearly 2.5-fold increase of the thyroid volume following FNA, being described as a frightening episode. Dal Fabbro et al. (in 1987) [5]and Van den Bruel et al. (in 2008) [6] reported acute transient thyroid swelling with with slightly or acute pain. In 2011, Norrenberg S et al. [3]reported two cases of acute swelling with acute pain over the 20-years process of FNA procedure. The episode lasted for 1 or 3 h. In 2016, Uchida et al. [7] reported an acute transient thyroid swelling and recovered after hydrocortisone treatment. Bouwman [8]reported the episode occurred after several unsuccessful subclavian vein catheterization attempts in 2009. And the author suggested that it was because cephalad needle direction contributed an advertent needle into the thyroid gland. With our case, all of the eight cases showed consistent in ultrasound appearance and 1.5- to 3-fold enlarged of thyroid gland. The episode happened immediately or shortly after FNA. Most cases accompanied with slightly to moderately pain, one of them had choking and one of them was associated with airway obstruction. Different with other cases, the patient in our case did not complain any discomfort. Some cases were treated by analgesic-antipyretics or hydrocortisone, some of them regressed spontaneously. The episode lasted from a few minutes to hours. All of the patients do not show common medical history, clinical manifestations, laboratory examination and pathological results. No uniform drugs were applied. Needles of different sizes were utilized (from 21- to 24-gauge and one subclavian catheter). (Table 1)
The underlying mechanism of acute swelling is not clear yet. Haas did not propose any hypothesis [4]. Dal Fabbro et al. analyzed the cause of it but failed to explain it [5]. They suspected blood causing the swelling, but the negative findings questioned the suspicion. They did not believe an inadvertently injection of air as no signs of emphysema could be detected. In our case, an intrathyroidal bleeding is first suspected but it can be excluded by the following reasons. (a) In our case, the puncture point was in superior pole of right thyroid lobe, but the patchy hypoechoic lesions came out in inferior pole first. (b) No actively bleeding site was observed along the way of the needle passage and no evidence of hematoma formation. (c) No feelings of swelling pain or other discomfort were complained. (d) Without any compression it regressed spontaneously. All of these clues could not support the hypothesis of bleeding. Van den Bruel et al. also excluded this hypothesis on retrospect due to the hyperacute swelling, which had a reversible nature within 1 h [6].
Van den Bruel et al. [6]previously proposed the theory of vasodilation and capillary leaking. They hypothesized Calcitonin Gene Related Peptide (CGRP) could be responsible for the observed phenomenon. Immunostaining for CGRP was positive in their cases but CGRP almost universally expressed by medullary thyroid cancer. Sarah Norrenberg et al. also suggested the proposal of CGRP could not explain the phenomenon in other cases [3].
From our perspective, this rare episode was hypothesized as a kind of anaphylactic reaction even though the hypothesis was ruled out by previous literatures. Sarah Norrenberg et al. [3] proposed that allergy could not explain this phenomenon because no signs of allergy were observed and no common solution was in contact with the skin or the gland tissue. Dal Fabbro [5] suggested that an allergic etiology seems unlikely, owing to the extremely rapid onset of swelling and to the fact that they did not inject any drug. When the episode occurred in our case, an anaphylactic reaction was suspected by the cause of the contrast-enhanced agents. The polymer of the encapsulated shell of microbubbles could be a foreign antigen to human body. But the hypothesis could not be applied in other cases. The main reason of this phenomenon may be not foreign materials, such as drugs, but the innate molecules. FNA can trigger biochemical alterations in serum, since it may destroy thyroid follicles, resulting in thyroglobulin release into the circulation [9]. May be the thyroglobulin or other molecules provoke an anaphylactic reaction of thyroid itself. On account of the sensitive skin of the patient, we highly suspected the possibilities of the hypersensitivity reaction even without allergic history. An allergic reaction is rapid in onset and could result in dilation of vessels and an increase of vascular permeability, which is supported by the hypothesis of previous literature [2]. The ultrasound appearance, a transient homogeneous echoic lesion in the extranodular thyroid parenchyma, could be a proof of this hypothesis. Many of those who have experienced anaphylaxis have survived the episode without any treatment [10]. The feature of self-limiting in reported episode keeps consistent with the characteristic of anaphylaxis reaction.
In conclusion, acute thyroid swelling after FNA of the thyroid gland is a rare complication. Ultrasonography showed thyroid lobes enlarged from 1.5 to 3-fold with funicular hypoechoic lesions accompanied with pain or not. The self-limiting course lasted for 30 min to 4 h, which is not life-threatened. No exact pathology or etiology has been convinced. We proposed a hypothesis of anaphylactic reaction but can’t be verified by laboratory data. We hope ultrasound physicians could pay attention to this rare complication and manage the frightened situation appropriately. More information is needed to support our hypothesis.
Availability of data and materials
Not applicable.
Abbreviations
- FNA:
-
Fine needle aspiration
- CGRP:
-
Calcitonin Gene Related Peptide
- AUS:
-
Atypical undetermined significance
References
Cappelli C, Pirola I, Agosti B, Tironi A, Gandossi E, Incardona P, Marini F, Guerini A, Castellano M. Complications after fine-needle aspiration cytology: a retrospective study of 7449 consecutive thyroid nodules. Br J Oral Maxillofac Surg. 2017;55(3):266–9.
Polyzos SA, Anastasilakis AD. Rare potential complications of thyroid fine needle biopsy. Hippokratia. 2011;15(2):116–9.
Norrenberg S, Rorive S, Laskar P, Catteau X, Delpierre I, Avni FE, Salmon I. Acute transient thyroid swelling after fine-needle aspiration biopsy: rare complication of unknown origin. Clin Endocrinol (Oxf). 2011;75(4):568–70.
Haas SN. Acute thyroid swelling after needle biopsy of the thyroid. N Engl J Med. 1982;307(21):1349.
Dal Fabbro S, Barbazza R, Fabris C, Perelli R. Acute thyroid swelling after fine needle aspiration biopsy. J Endocrinol Invest. 1987;10(1):105.
Van den Bruel A, Roelandt P, Drijkoningen M, Hudders JP, Decallonne B, Bouillon R. A thyroid thriller: acute transient and symmetric goiter after fine-needle aspiration of a solitary thyroid nodule. Thyroid. 2008;18(1):81–4.
Uchida T, Himuro M, Komiya K, Goto H, Takeno K, Honda A, Sato J, Kawano Y, Suzuki R, Watada H. Evanescent hyperechoic changes after fine-needle aspiration biopsy of the thyroid in a series with a low overall prevalence of complications. J Ultrasound Med. 2016;35(3):599–604.
Bouwman RA, Meijerink MR, Beishuizen A. Acute transient thyroid swelling after catheterization of the subclavian vein. Crit Care. 2009;13(5):419.
Polyzos SA, Anastasilakis AD. Alterations in serum thyroid-related constituents after thyroid fine-needle biopsy: a systematic review. Thyroid. 2010;20(3):265–71.
Reber LL, Hernandez JD, Galli SJ. The pathophysiology of anaphylaxis. J Allergy Clin Immunol. 2017;140(2):335–48.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from the Guide Project for Key Research and Development Foundation of Liaoning Province (No. 2019JH8/10300008), Scientific Research Project of the Educational Department of Liaoning Province (ZF2019023) and 345 Talent Project. This funder was supported by YH.
Author information
Authors and Affiliations
Contributions
TZ was a major contributor in collection, analysis and interpretation of the images and in writing the manuscript. YY and HJ reviewed the literatures and revised the manuscript. YH performed the examination and designed the study. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by Institutional Review Board of China Medical University.
Consent for publication
Written, informed consent for publication was obtained from all the study individuals. Copy of the consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhu, T., Yang, Y., Ju, H. et al. Acute thyroid swelling after fine needle aspiration—a case report of a rare complication and a systematic review. BMC Surg 21, 175 (2021). https://doi.org/10.1186/s12893-021-01160-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12893-021-01160-z