
Abstract
Background
Unipedicular and bipedicular approaches for percutaneous kyphoplasty are reportedly both effective in treating osteoporotic vertebral compression fractures (OVCFs). However, most studies have reported thoracolumbar fractures, with few reports describing the treatment of the lower lumbar spine. Here, we compared the clinical and radiological results of unipedicular and bipedicular approaches for percutaneous kyphoplasty for treating osteoporotic vertebral compression fractures.
Methods
We retrospectively reviewed the records of 160 patients who underwent percutaneous kyphoplasty for lower lumbar (L3–L5) osteoporotic vertebral compression fractures between January 2016 and January 2020. Patient characteristics, surgical outcomes, operation time, blood loss, clinical and radiological features, and complications were compared between two groups. Cement leakage, height restoration, and cement distribution were calculated from the radiographs. Visual pain analog scale (VAS) and Oswestry Disability Index (ODI) were calculated before surgery, immediately post-surgery, and 2 years after surgery.
Results
The mean age, sex, body mass index, injury time, segmental distribution, and morphological classification of fractures before surgery did not differ significantly between the groups. The results showed significant improvements in the VAS score, ODI score, and vertebral height restoration in each group (p < 0.05), with no significant differences between the two groups (p > 0.05). The mean operation time and extent of blood loss were lower in the unipedicular group than those in the bipedicular group (p < 0.05). Different types of bone cement leakage were observed in both groups. Leakage rate was higher in the bipedicular group than in the unipedicular group. Patients in the bipedicular group showed greater improvement in bone cement distribution than those in the unipedicular group (p < 0.05).
Conclusions
The clinical and radiological results of unipedicular percutaneous kyphoplasty for treating osteoporotic vertebral compression fractures in the lower lumbar region were similar to those of bipedicular percutaneous kyphoplasty. However, the unipedicular approach resulted in shorter surgical time, less blood loss, and less bone cement leakage. Thus, the unipedicular approach may be preferable owing to its several advantages.
Similar content being viewed by others

Background
Osteoporotic vertebral compression fractures (OVCFs) have become increasingly common in older patients in recent years. Owing to a decrease in bone mass and an increase in bone fragility, even minimal trauma may be sufficient to cause fractures in older patients [1,2,3]. Various techniques have been developed to treat OVCFs. Among these, percutaneous balloon kyphoplasty (PKP) has been the most effective treatment for OVCFs since it was first described in 1997 [4]. PKP is a minimally invasive spinal surgery technique in which a balloon tamp is inserted into the vertebral body through the pedicle to repair the vertebral height and fix the fracture by injecting polymethyl methacrylate (PMMA) bone cement into the vertebral body [5, 6]. Currently, the standard PKP technique involves a bipedicular approach. In recent years, unipedicular approach has been advocated because of shorter operating and radiation exposure times, which can lower the risk of cement leakage and complications. Most previous studies have shown that the clinical and radiological results of unipedicular percutaneous kyphoplasty for OVCFs are similar to those of bipedicular percutaneous kyphoplasty [7,8,9]. However, the previous studies have mostly focused on the thoracolumbar spine, and there are few reports on the lower lumbar spine (L3–L5). Owing to the large vertebral bodies, the puncture needle does not easily reach the opposite side in the unilateral approach, and the bone cement filler cannot be evenly distributed throughout the vertebral body; therefore, most surgeons prefer the bipedicular approach. To confirm that both procedures can be successfully used in patients with lower lumbar vertebral compression fractures, we compared the clinical and radiological results of the unipedicular and bipedicular approaches for PKP to treat lower lumbar OVCFs.
Methods
Patients
We retrospectively analyzed patients with OVCFs of the lower lumbar spine (L3–L5) who underwent PKP between January 2016 and January 2020. The inclusion criteria were (1) age > 50 years, (2) single-level OVCFS, and (3) preoperative magnetic resonance imaging (MRI) performed to assess acute fractures, in which T2-weighted short tau inversion recovery sequence (STIR) showed obvious bone edema in the fractured vertebral body, and (4) PKP performed within 4 weeks of OVCFS occurrence, and (5) the patients received anti-osteoporosis therapy (calcium supplementation and vitamin D) and rehabilitation training postoperatively. The exclusion criteria were (1) OVCFS treated with percutaneous mesh container-plasty, (2) multiple lesions or previous compression fractures, (3) symptoms of neurological deficits, (4) severe spinal deformities or severe comorbidities (ankylosing spondylitis, multiple myeloma, tumor, thyroid or parathyroid disease, hepatic disease, and kidney disease), and (5) vertebral compression fracture due to causes other than osteoporosis. In total, 160 patients were enrolled in this study. The patients were divided into two groups according to the PKP approach: the unipedicular group (n = 82) and the bipedicular group (n = 78). The following data were collected for demographic analysis: age, sex, body mass index (BMI), injury time, segmental distribution, and morphological classification of the fractures. The fractures were classified as A (wedging), B (biconcavity), and C (crush) based on morphology, according to the EVOSG classification published in 1999 [10].
Surgical techniques
The PKP was performed by a single surgeon. All procedures were performed under local anesthesia. The patients were placed in the prone position on four bolsters on a radiolucent operating table with the abdomen freely suspended.
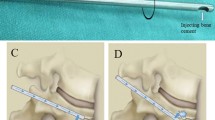
A 1-cm skin incision was made percutaneously lateral to the desired entry point of the pedicle. A trocar (Shandong Guanlong Medical Utensils Co., Ltd., Jinan City, Shandong Province, China) in a cannula was inserted into the pedicle at the fractured vertebra using a pedicular approach as the working channel. After the trocar was removed, a balloon was placed in the working channel and slowly inflated to create a low-pressure cavity for cement injection. Inflation continued until the balloon pressure reached 300 psi. The balloon was then deflated and removed. Next, the PMMA cement was injected into the defect of the fractured body through the cannula under continuous fluoroscopic monitoring. The PMMA insertion was considered complete when it reached the posterior third of the vertebral body or had a tendency toward cortical, epidural, or anterior venous cement leakage. In the bipedicular approach, the same surgical steps are performed for both pedicles. In the unipedicular approach, the puncture angle was increased, with the end of the cannula placed as close to the midline as possible so that the inflated balloon could exceed the midline of the vertebra on the anteroposterior view to allow the PMMA to spread as much as possible throughout the vertebral body (Figs. 1 and 2).

a-f Percutaneous kyphoplasty for the treatment of a L3 vertebral compression fracture in bipedicular approach. a-b Preoperative lateral radiograph and MRI showing a L3 vertebral compression fracture. c-d intraoperative view (e-f) Postoperative lateral radiograph showing cement distribution after undergoing PKP surgery of L3 vertebral compression fracture

a-f Percutaneous kyphoplasty for the treatment of a L4 vertebral compression fracture in unipedicular approach. a-b Preoperative lateral radiograph and MRI showing a L4 vertebral compression fracture. c-d intraoperative view (e-f) Postoperative lateral radiograph showing cement distribution after undergoing PKP surgery of L4 vertebral compression fracture
Measurements
Imaging findings and clinical outcomes were analyzed before and after surgery. Anterior, middle, and posterior vertebral body height ratios (AVBHr, MVBHr, and PVBHr, respectively) were measured using lateral radiographs, as described previously [11]. The methods used to measure the vertebral body height ratios are shown in Fig. 3. Vertebral height was defined as the endplate-to-endplate distance measured from the anterior aspect of the vertebral body on the lateral radiographs. Operation time, estimated blood loss, length of hospital stay, and complications were recorded. The visual analog scale (VAS) was used to evaluate analgesic efficacy (on a scale of 0–10), while the Oswestry Low Back Pain Disability Index (ODI) was used for functional assessment. Cement distribution was calculated using anteroposterior and lateral radiographs. Cement leakage was determined using X-ray films. The immediate and 2-year postoperative follow-up findings of all patients were recorded. Incidence of cement leakage from the vertebral body on postoperative radiographs and type of bone cement leakage were also recorded.

a-c Methods of measurements on images. a Lateral radiograph showing evaluation of the anterior vertebral body height ratio (AVBHr), middle vertebral body height ratio (MVBHr), and posterior vertebral body height ratio (PVBHr). AVBHr=A2/A1, MVBHr=M2/M1, and PVBHr=P2/P1. b-c Lateral and Frontal radiograph showing the evaluation of cement distribution. Cement distribution =a/(a+b)
Furthermore, two independent spine surgeons performed the clinical evaluation of the patients. Additionally, three other spine surgeons assessed the radiographs.
Statistical analysis
Statistical analyses were performed using the PASW Statistics for Windows (version 18.0; SPSS Inc., Chicago, IL, USA). Numeric variables are presented as means ± standard deviation. Repeated-measures analysis of variance (ANOVA) was used to analyze the differences between preoperative and postoperative VAS scores, ODI scores, and vertebral height restoration. Student’s t-test was used to compare measurements between the two groups. Nominal variables (sex, distribution of the fractured vertebra, and cement leakage) were presented as numbers (percentages) and compared using chi-square tests. P values < 0.05 were considered to indicate statistically significant differences.
Results
The clinical characteristics of the 160 patients are summarized in Table 1. The mean ages of the patients in the unipedicular and bipedicular groups were 75.86 ± 7.74 years and 74.23 ± 8.17 years, respectively. Age, sex, injury time, BMI, segmental distribution, and morphological classification of fractures before surgery did not differ significantly between the groups. Operation time and blood loss were significantly reduced in the unipedicular group compared to the bipedicular group (32.01 ± 4.48 vs. 42.42 ± 6.01, 5.46 ± 1.22 vs. 8.73 ± 1.20; p < 0.05). There were no significant differences in the lengths of hospital stay between the two groups. Details are presented in Table 2.
Clinical outcomes
Most patients in both groups experienced excellent pain relief and improved physical abilities. The VAS scores decreased from 7.30 ± 1.01 preoperatively to 2.39 ± 0.76 postoperatively in the unipedicular group (p < 0.05) and from 7.23 ± 0.88 preoperatively to 2.38 ± 0.72 postoperatively in the bipedicular group (p < 0.05). The ODI scores decreased from 70.59 ± 4.22 preoperatively to 26.74 ± 2.50 postoperatively in the unipedicular group (p < 0.05) and from 70.88 ± 3.66 preoperatively to 26.58 ± 2.46 postoperatively in the bipedicular group (p < 0.05). The VAS and ODI scores did not differ significantly between the two groups either postoperatively or 2 years postoperatively. The operation time and blood loss in the unipedicular group were less than those in the bipedicular group (32.01 ± 4.48 vs. 42.42 ± 6.01, 5.46 ± 1.22 vs. 8.73 ± 1.20; p < 0.05). The details are presented in Tables 2 and 3.
Radiographic evaluation
The anterior, middle, and posterior vertebral height ratios improved from (85.46% ± 10.26%, 80.32% ± 13.81%, and 90.87% ± 8.91%, respectively) preoperatively to (92.34% ± 9.42%, 86.58% ± 14.22%, and 92.50% ± 8.86%, respectively) postoperatively in the unipedicular group and from (85.69% ± 11.22%, 77.26% ± 12.81%, and 88.81% ± 9.96%, respectively) preoperatively to (90.86% ± 8.98%, 85.26% ± 11.84%, and 90.03% ± 8.39%, respectively) postoperatively in the bipedicular group. The cement distribution on the lateral radiographs did not differ significantly between the two groups (62.17% ± 11.40% vs. 62.05% ± 10.26%; p > 0.05). However, the anteroposterior radiographs showed a higher cement distribution in the bipedicular group compared to that in the unipedicular group (57.78% ± 11.36% vs. 52.13% ± 10.39%; p < 0.05). Bone cement exceeded the midline of the vertebral body in all patients. The radiographic results are presented in Table 4.
Complications
Leakage of bone cement outside the vertebral body was observed in both groups on the postoperative anteroposterior and lateral radiographs. The bone cement leakage rates were 23.1% (19 of 82) in the unipedicular group (six in the disc, five in the vertebral vein, and eight in the paravertebral vein) and 25.6% (20 of 78) in the bipedicular group (five in the disc, four in the vertebral vein, and 10 in the paravertebral vein) and did not differ significantly between the two groups (p = 0.716) (Table 2). None of the bone cement leakages required special treatment and no clinical symptoms were attributed to cement leakage. No other major postoperative complications, such as neurological damage, hemorrhage, infection, or pulmonary embolism, were observed.
Discussion
Both unilateral and bilateral PKP have proven effective in the treatment of OVCFs. Previous studies have shown that both the unipedicular and bipedicular approaches can achieve considerable improvements in vertebral height restoration and pain relief. However, few studies have been conducted on the lower lumbar spine. While Rebolledo et al. [12] compared unilateral and bilateral PKP in the lower lumbar vertebrae, they included only seven patients. Chen et al. [13] reported four cases of L3 and L4 in 2010. The present study included 66 cases of L3, 63 cases of L4, and 31 cases of L5 OVCFs, respectively, which have not been previously reported.
Clinical outcomes
The primary purpose of kyphoplasty is to relieve pain and improve patient function, thereby improving quality of life. In the present study, the VAS and ODI scores significantly improved in both groups postoperatively (p < 0.05), with no statistically significant difference between the unilateral and bilateral groups, a finding consistent with previous reports. Wang et al. [7] reported better VAS and ODI scores in the bipedicular group than in the unipedicular group postoperatively; however, the difference was not statistically significant. Zhang et al. [14] reported superior 3-month follow-up outcomes of the bipedicular approach for PKP compared to the unipedicular approach. Some articles reported contradictory findings; Song et al. [8] reported greater improvement in VAS scores in the unipedicular group than in the bipedicular group. However, most previous studies focused on the thoracolumbar spine, with few reports on the lower lumbar spine; thus, additional studies are required.
Radiographic evaluation
Both techniques can effectively restore vertebral body height. In 2010, Chen et al. [15] reported that bipedicular PKP was more effective than unipedicular PKP in improving the vertebral height. More recently, in their 2020 study, Lee et al. [9] reported no differences in height restoration between the two techniques. We also concluded that both techniques provided similar restoration of vertebral height, with no differences in the anterior or middle vertebral heights post-operatively. However, the imaging findings in the present study showed an unremarkable degree of vertebral compression of the fractured segment in the lower lumbar region; therefore, the recovery of vertebral height postoperatively was limited in both groups.
Bone cement distribution is important for postoperative functional improvement and stabilization of the vertebral body, and likely plays a major role in pain relief [16,17,18,19,20,21]. Tan et al. [22] reported that a fully distributed bone cement can better restore the strength and maintain the height of the vertebral body. In the present study, the distribution of cement on the lateral radiographs did not differ between the two groups; however, the anteroposterior radiographs showed a wider distribution for the bipedicular approach than for the unipedicular approach. Owing to the large puncture angle, the end of the cannula should reach the midline as far as possible. Therefore, the cement exceeded the midline of the vertebral body in the anteroposterior radiographs of the selected cases in the unipedicular approach group. Chen et al. [17] showed that cement augmentation crossing the midline resulted in increased stiffness on both sides, with strong potential for achieving biomechanical balance. The present study showed similar radiographic and clinical outcomes between the unilateral and bilateral groups. Thus, unilateral kyphoplasty can provide stability for lower lumbar compression fractures when the cement exceeds the midline of the vertebral body.
Complications
Kyphoplasty carries the risk of complications, including pulmonary embolism, cement leakage, neurological deficits, and even paraplegia [23, 24]. The most common complication of percutaneous vertebroplasty is cement leakage, particularly cortical and venous leakages. Bone cement can enter the pulmonary artery through the paravertebral vein and cause a pulmonary embolism, which can lead to death. Risk factors for postoperative cement leakage include cortical disruption, higher cement volume, intravertebral cleft, and solid cement distribution [25, 26]. Previous studies have demonstrated that the unipedicular approach results in fewer cement leaks. Zhang et al. [14] reported bone cement leakage rates of 20.8% (five of 24) in the unipedicular group and 34.6% (nine in 26) in the bipedicular group, which did not differ significantly between groups. Lee et al. [9] reported no significant differences in the leakage rates of cement into the intradiscal space (14% in the unipedicular group and 18% in the bipedicular group). A 2019 meta-analysis by Chen et al. concluded that the unilateral approach decreased the incidence of cement leakage in PKP [27]. Similar to previous reports, the cement leakage rate in the bipedicular group (25.6%) in the present study was higher than that in the unipedicular group (21.3%). However, there were no significant differences between the two groups.
Limitations
The present study had some limitations. First, it was a retrospective analysis with incomplete data for some cases and inadequate follow-up time. Additionally, postoperative CT images were lacking, which may have more accurately reflected the distribution of bone cement postoperatively. Further prospective studies with longer or more frequent follow-ups are required to confirm our findings.
Conclusions
The results of our study demonstrated that both unipedicular and bipedicular PKP techniques were effective for treating OVCFs in the lower lumbar region. However, the bipedicular approach provided better cement distribution than the unipedicular approach. We observed no statistically significant differences in pain relief, functional recovery, or vertebral height restoration between the two groups. However, the unipedicular approach has the advantages of short operation time, less blood loss, and less radiation exposure. In conclusion, the unipedicular approach may be clinically preferred because of its advantages.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ANOVA:
-
Analysis of variance
- BMI:
-
Body mass index
- MRI:
-
Magnetic resonance imaging
- ODI:
-
Oswestry Low Back Pain Disability Index
- OVCFs:
-
Osteoporotic vertebral compression fractures
- PKP:
-
Percutaneous balloon kyphoplasty
- PMMA:
-
Polymethyl methacrylate
- STIR:
-
Short tau inversion recovery
- VAS:
-
Visual analog scale
References
Papapoulos SE. Anabolic bone therapies in 2014: New bone-forming treatments for osteoporosis. Nat Rev Endocrinol. 2015;11:69–70.
Litwic A, Cooper C, Dennison E. Osteoporosis therapies in 2014. Panminerva Med. 2014;56:273–83.
Kim KW, Cho KJ, Kim SW, et al. A nation-wide, outpatient-based survey on the pain, disability, and satisfaction of patients with osteoporotic vertebral compression fractures. Asian spine journal. 2013;7:301–7.
Galibert P, Deramond H, Rosat P, et al. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie. 1987;33:166–8.
Liu J, Li X, Tang D, et al. Comparing pain reduction following vertebroplasty and conservative treatment for osteoporotic vertebral compression fractures: a meta-analysis of randomized controlled trials. Pain Physician. 2013;16:455–64.
Theodorou DJ, Theodorou SJ, Duncan TD, et al. Percutaneous balloon kyphoplasty for the correction of spinal deformity in painful vertebral body compression fractures. Clin Imaging. 2002;26:1–5.
Wang W, Duan K, Ma M, et al. Can an unipedicular approach replace bipedicular percutaneous vertebroplasty for osteoporotic vertebral compression fracture? J Back Musculoskelet Rehabil. 2019;32:261–7.
Song BK, Eun JP, Oh YM. Clinical and radiological comparison of unipedicular versus bipedicular balloon kyphoplasty for the treatment of vertebral compression fractures. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2009;20:1717–23.
Lee CH, Kim HJ, Lee MK, et al. Comparison of efficacies of unipedicular kyphoplasty and bipedicular kyphoplasty for treatment of single-level osteoporotic vertebral compression fractures: A STROBE-compliant retrospective study. Medicine. 2020;99:e22046.
Ismail A, Cooper C, Felsenberg D, et al. Number and type of vertebral deformities: epidemiological characteristics and relation to back pain and height loss. European Vertebral Osteoporosis Study Group. Osteoporosis int. 1999;9:206–13.
Thaler M, Lechner R, Nogler M, et al. Surgical procedure and initial radiographic results of a new augmentation technique for vertebral compression fractures. Eur spine j. 2013;22:1608–16.
Rebolledo BJ, Gladnick BP, Unnanuntana A, et al. Comparison of unipedicular and bipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a prospective randomised study. Bone joint j. 2013;95-B:401–6.
Chen L, Yang H, Tang T. Unilateral versus bilateral balloon kyphoplasty for multilevel osteoporotic vertebral compression fractures: a prospective study. Spine. 2011;36:534–40.
Zhang L, Liu Z, Wang J, et al. Unipedicular versus bipedicular percutaneous vertebroplasty for osteoporotic vertebral compression fractures: a prospective randomized study. BMC Musculoskelet Disord. 2015;16:145.
Chen C, Chen L, Gu Y, et al. Kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approachment: a comparative study in early stage. Injury. 2010;41:356–9.
Evans AJ, Jensen ME, Kip KE, et al. Vertebral compression fractures: pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty retrospective report of 245 cases. Radiology. 2003;226:366–72.
Chen B, Li Y, Xie D, et al. Comparison of unipedicular and bipedicular kyphoplasty on the stiffness and biomechanical balance of compression fractured vertebrae. Eur spine j. 2011;20:1272–80.
Liang D, Ye LQ, Jiang XB, et al. Biomechanical effects of cement distribution in the fractured area on osteoporotic vertebral compression fractures: a three-dimensional finite element analysis. J Surg Res. 2015;195:246–56.
He X, Li H, Meng Y, et al. Percutaneous Kyphoplasty Evaluated by Cement Volume and Distribution: An Analysis of Clinical Data. Pain Physician. 2016;19:495–506.
Li Q, Long X, Wang Y, et al. Clinical observation of two bone cement distribution modes after percutaneous vertebroplasty for osteoporotic vertebral compression fractures. BMC Musculoskelet Disord. 2021;22:577.
Mo L, Wu Z, Liang, et al. Influence of bone cement distribution on outcomes following percutaneous vertebroplasty: a retrospective matched-cohort study. J Int Med Res. 2021;49:3000605211022287.
Tan L, Wen B, Guo Z, et al. The effect of bone cement distribution on the outcome of percutaneous Vertebroplasty: a case cohort study. BMC Musculoskelet Disord. 2020;21:541.
Nieuwenhuijse MJ, Van Erkel AR, Dijkstra PD. Cement leakage in percutaneous vertebroplasty for osteoporotic vertebral compression fractures: identification of risk factors. The spine j. 2011;11:839–48.
Kim YJ, Lee JW, Park KW, et al. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: incidence, characteristics, and risk factors. Radiology. 2009;251:250–9.
Tang B, Cui L, Chen X, et al. Risk Factors for Cement Leakage in Percutaneous Vertebroplasty for Osteoporotic Vertebral Compression Fractures: An Analysis of 1456 Vertebrae Augmented by Low-Viscosity Bone Cement. Spine. 2021;46:216–22.
Hong SJ, Lee S, Yoon JS, et al. Analysis of intradiscal cement leakage during percutaneous vertebroplasty: multivariate study of risk factors emphasizing preoperative MR findings. J Neuroradio. 2014;41:195–201.
Chen W, Xie W, Xiao Z, et al. Incidence of Cement Leakage Between Unilateral and Bilateral Percutaneous Vertebral Augmentation for Osteoporotic Vertebral Compression Fractures: A Meta-Analysis of Randomized Controlled Trials. World neurosurgery. 2019;122:342–8.
Acknowledgements
Not applicable.
Funding
The authors declare that this study has received no financial support.
Author information
Authors and Affiliations
Contributions
Concept: YQ and SH; Design: YQ and YL; Supervision: CT; Materials: GS and XZ; Data Collection and/or Processing: YL and GS; Analysis and/or Interpretation: YQ and YL; Literature Review: GS and CT; Writing: YQ; Critical Review: YQ and SH. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Third Affiliated Hospital of Wenzhou Medical University. The Committee waived the requirement for informed consent. All procedures were carried out in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qian, Y., Li, Y., Shen, G. et al. Comparison of unipedicular and bipedicular kyphoplasty for treating acute osteoporotic vertebral compression fractures in the lower lumbar spine: a retrospective study. BMC Musculoskelet Disord 24, 410 (2023). https://doi.org/10.1186/s12891-023-06545-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06545-0