
Abstract
Background
Studies have confirmed that antioxidants contribute to a lower risk of osteoporosis, which is an independent factor for femoral neck fracture (FNF). However, the associations between blood antioxidant levels and femoral neck strength remain unclear.
Objective
Our aim was to test the hypothesis that levels of blood antioxidants are positively associated with composite indices of bone strength in femoral neck, which integrate the bending strength index (BSI), compressive strength index (CSI), and impact strength index (ISI), in a population of middle-aged and elderly individuals.
Methods
This cross-sectional study utilized data from the Midlife in the United States (MIDUS) study. Blood levels of antioxidants were measured and analyzed.
Results
In total, data from 878 participants were analyzed. Results of Spearman correlation analyses indicated that blood levels of 6 antioxidants (total lutein, zeaxanthin, alpha-carotene, 13-cis-beta-carotene, trans-beta-carotene and total lycopene) were positively associated with CSI, BSI, or ISI in middle-aged and elderly individuals. Conversely, blood gamma-tocopherol and alpha-tocopherol levels were negatively associated with CSI, BSI, or ISI scores. Furthermore, linear regression analyses suggested that only blood zeaxanthin levels remained positively associated with CSI (odds ratio, OR 1.27; 95% CI: 0.03, 2.50; p = 0.045), BSI (OR, 0.54; 95% CI: 0.03–1.06; p = 0.037), and ISI (OR, 0.06; 95% CI: 0.00, 0.13; p = 0.045) scores in the study population after adjusting for age and sex.
Conclusions
Our results indicated that elevated blood zeaxanthin levels were significantly and positively associated with femoral neck strength (CSI, BSI, or ISI) in a population of middle-aged and elderly individuals. These findings suggest that zeaxanthin supplementation may reduce FNF risk independently.
Similar content being viewed by others


Introduction
Osteonecrosis of the femoral head (ONFH) is one of the most common debilitating diseases, as it increases the risk of traumatic and nontraumatic fracture occurrence in the general population [1, 2]. Existing evidence in ONFH patients suggests that these individuals have lower bone density of the femoral head, which may be related to a reduction in the osteogenic differentiation of bone marrow stromal cells (BMSCs) and an inhibition of osteogenic gene expression [2, 3]. A recent study demonstrated that nontraumatic ONFH patients had lower bone mineral density (BMD) of the lumbar spine and femoral neck than that of healthy populations [1]. Although BMD is widely used to evaluate bone strength [4, 5], other studies indicate that BMD may only reflect 50%-70% of total bone strength [6, 7]. The comprehensive indices of femoral neck strength include the bending strength index (BSI), compressive strength index (CSI) and impact strength index (ISI) which are good indicators of femoral bone strength, a measure that is considered a predictor for femoral neck fracture (FNF) [8].
Oxidative stress promotes bone loss and remodeling via its impact on the regulation of osteoblast survival and differentiation and enhancement of inflammatory responses [9]. Conversely, antioxidants can inhibit oxidative stress and prevent the pathological process [10]. Existing evidence indicates that the consumption of antioxidant rich fruits and vegetables, such as apples, tomatoes, and oranges, is related to attenuations in bone mass loss, a factor impacting fracture risk, in postmenopausal women [11]. However, the beneficial effects of an increased antioxidant intake on bone strength are controversial. On the one hand, some epidemiological studies have reported that an increased intake of certain antioxidants, including vitamin C, vitamin E, and carotenoids, may confer benefits to BMD in premenopausal and postmenopausal females [12,13,14]. On the other hand, several studies have reported a positive correlation between higher intakes of vitamin C and higher risk of osteoporosis [15, 16]. Furthermore, previous evidence also indicated that antioxidants may produce bone-site specific beneficial effects on bone health [17]. for example, a previous study reported that a high β-carotene consumption was related to increased BMD of the femoral neck and total hip rather than other body parts in postmenopausal women [12].
This cross-sectional study was conducted using data from the Midlife in the United States (MIDUS) study. We aimed to investigate the associations between the 10 blood antioxidants and BSI, CSI and ISI in the middle-aged and elderly individuals.
Methods
Study participants
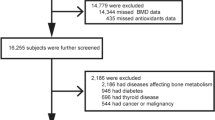
The MIDUS Study mainly aimed to investigate the psychosocial and behavioral factors involved in age-related health conditions among a national sample of Americans [18, 19]. Data used in our study were obtained from participants in the Biomarker Project of MIDUS II (N = 1,255). The Biomarker Project recruited participants from the original MIDUS I cohort and aimed to measure various biological indicators in blood, urine, saliva, and other biological samples from 2004 to 2009 [19]. Additional details regarding the study methods and samples have been published elsewhere [18, 19]. Of the 1,255 participants in the Biomarker Project, we excluded data from 377 participants who had missing data on important variables. The final analysis from 878 participant samples were seen in Fig. 1. All methods were carried out in accordance with relevant guidelines and regulations, approval from appropriate Institutional Review Boards at the Midlife in the United States (MIDUS) study centers [three general clinical research centers (GCRC), including Georgetown University, the University of California at Los Angeles and the University of Wisconsin-Madison] was granted for this study and all participants gave informed consent before participation. We retrospectively analyzed MIDUS data from an open database (Inter-University Consortium for Political and Social Research).

Flow chart displaying the final analysis of the included samples
Blood measurements
Details for the collection methods of biological samples in the Biomarker Project have been previously described [20]. In summary, we measured and analyzed blood levels of 10 antioxidant markers (total lutein, zeaxanthin, beta-cryptoxanthin, 13-cis-beta-carotene, alpha-carotene, trans-beta-carotene, total lycopene, gamma-tocopherol, alpha-tocopherol, and retinol). Blood antioxidant measurements were obtained from fasting blood samples collected in the morning.
Assessment of femoral neck strength
During each participants visit, the BMD values of the left hip and lumbar spine (L1-L4) were measured by DXA scans via Hologic 4500 (UCLA and Georgetown sites) technology or GE Healthcare Lunar Prodigy (Madison site). Femoral neck width (FNW) and femoral neck axis length (FNAL) were also measured from the hip scans using manufacturer guidelines. The composite indices of femoral neck strength (g/kg-m), including CSI, BSI, and ISI, were calculated by the following formulas [21]: 1) CSI = BMD × FNW/Weight; 2) BSI = (BMD × FNW2)/(FNAL × Weight); 3) ISI = (BMD × FNW × FNAL)/(Height × Weight).
Statistical analyses
For research purposes, Spearman correlation analyses were preliminarily performed to examine the relationships between the 10 antioxidants and femoral neck strength (BSI, CSI and ISI). Then, linear regression analyses were conducted to assess the independent relationships among variables with antioxidants as independent variables and femoral neck strength indices as dependent variables (CSI, BSI and ISI) in the models. Age and sex have been reported to be related to bone mass loss [22], therefore the models were adjusted for age (Model 1) and sex (Model 2) successively. Standardized correlation coefficients and 95% confidence intervals (CIs) were reported for these models.
We used multiple linear regression analyses to explore the relationships between the 10 measured antioxidants and femoral neck strength, stratified by age, sex and BMI. We used the median age value to form a categorical variable for age (< 53 years and ≥ 53 years) and dichotomized BMI as < 24 kg/m2 or ≥ 24 kg/m2. Then, we tested for effect modification of age, sex and BMI on the associations. R version 4.0 and SPSS 25.0 were used for all analyses. The P value ≤ 0.05 represented a statistically significant difference.
Results
Characteristics of participants
A total of 878 samples were analyzed. As shown in Table 1, the age [53 (44–61) years], sex [male, 356 (40.55%)] and BMI [28.61 (25.07–32.97)] of our study sample were similar to the complete sample from the Biomarker Project. 377 Biomarker Project participants were mainly excluded from our analyses due to the presence of missing data for the femoral neck strength (BSI, CSI and ISI) and blood antioxidant variables. Hence, our study participants may have similar BDM [0.78 (0.66–1.02) gms/cm2], CSI [3.49 (3.05–4.03) g/kg-m], BSI [1.17 (1.00–1.36) g/kg-m] and ISI [0.20 (0.16–0.23) g/kg-m] values with the Biomarker Project sample. Similarly, the blood levels of antioxidants, including total lutein, zeaxanthin, beta-cryptoxanthin, 13-cis-beta-carotene, alpha-carotene, trans-beta-carotene, total lycopene, gamma-tocopherol, alpha-tocopherol, and retinol, were 0.20 (0.14–0.28) µmol/L, 0.05 (0.04–0.08) µmol/L, 0.17 (0.11–0.27) µmol/L, 0.05 (0.03–0.09) µmol/L, 0.06 (0.03–0.09) µmol/L, 0.37 (0.19–0.75) µmol/L, 0.39 (0.28–0.53) µmol/L, 3.66 (2.23–5.62) µmol/L, 25.95 (20.07–34.53) µmol/L and 1.58 (1.26–1.92) µmol/L, respectively.
Spearman correlation analyses between blood levels of the measured antioxidants and bone strength of the femoral neck
We observed that elevated blood levels of total lutein, zeaxanthin, 13-cis-beta-carotene, alpha-carotene, trans-beta-carotene and total lycopene levels were positively associated with CSI (all P ≤ 0.05), and blood levels of gamma-tocopherol and alpha-tocopherol were negatively associated with CSI. Levels of circulating beta-cryptoxanthin and retinol were not associated with CSI (P > 0 0.05). Circulating concentrations of total lutein, zeaxanthin, beta-cryptoxanthin, 13-cis-beta-carotene, alpha-carotene, trans-beta-carotene and total lycopene were positively associated with BSI (all P ≤ 0.05). However, blood gamma-tocopherol and alpha-tocopherol concentrations were inversely related to BSI (all P ≤ 0.05). Similar results were present for ISI (Table 2).
Adjusted associations between blood antioxidant levels and bone strength of the femoral neck
The results of our age and sex adjusted linear regression analyses, as shown in Table 3, confirmed that elevated blood zeaxanthin (r = 1.27; 95% CI: 0.03, 2.50; P = 0.045) and 13-cis-beta-carotene levels (r = 0.11; 95% CI: 0.28, 1.94; P = 0.009) were associated with increased CSI in the femoral neck, whereas elevated blood gamma-tocopherol (r = -0.03; 95% CI: -0.05, -0.01; P = 0.006) and alpha-tocopherol (r = -0.01; 95% CI: -0.01, -0.00; P = 0.024) levels were associated with lower CSI. Moreover, we found that blood total lutein (r = 0.19; 95% CI: 0.03, 0.35; P = 0.024), zeaxanthin (r = 0.54; 95% CI: 0.03, 1.06; P = 0.037), beta-cryptoxanthin (r = 0.22; 95% CI: 0.09, 0.36; P = 0.001), 13-cis-beta-carotene (r = 0.37; 95% CI: 0.02, 0.71; P = 0.036) and alpha-carotene (r = 0.28; 95% CI: 0.02, 0.54; P = 0.035) levels were positively associated with BSI. Finally, the results of the linear regression analyses were similar for ISI, as shown in Table 3.
Subgrouping analyses on the associations between blood zeaxanthin levels and bone strength of the femoral neck
The above results showed that only elevated blood zeaxanthin levels were positively and significantly correlated with CSI, BSI, and ISI, respectively. Thus, we further analyzed scatter plots and found that higher blood zeaxanthin levels may have contributed to higher composite indices of femoral neck strength (Fig. 2). Furthermore, we conducted subgrouping analyses to evaluate the effects of age, sex, and BMI on the relationship between blood zeaxanthin levels and bone strength of the femoral neck. Interestingly, although the interaction effects for age, sex, and BMI were not statistically significant (all interaction P values ≥ 0.05), as shown in Table 4, we still found that elevated blood zeaxanthin levels were associated with higher CSI, BSI and ISI in female participants aged ≥ 53 years or with a BMI ≥ 24 kg/m2.

Scatter diagram depicting the associations between blood zeaxanthin and the femoral neck strength (BSI, CSI and ISI)
Discussion
There are many studies investigating the associations between antioxidants and bone health. For instance, it has been reported that greater serum carotenoid and lutein concentrations are associated with higher BMD in Chinese adults [23], and an adequate intake of vegetables may reduce the risk of osteoporotic fractures among elderly men. The antioxidation of carotenoids may counteract the mechanism of osteoporosis related to leanness [24]. Consistent with carotenoids, elevations in serum levels of lutein and zeaxanthin play a role in bone health [25]. Oxidative stress is associated with lower BMD, which is more pronounced in individuals with low serum levels of vitamin E, as are often observed in older men [26]. Consistently, our results also showed that increased antioxidant levels were cross-sectionally associated with elevated indices of femoral neck strength (CSI, BSI, and ISI) in a representative sample of Americans. A positive correlation between zeaxanthin levels and femoral neck strength (CSI, BSI, and ISI) was also observed after adjustment for age and sex. One recent meta-analysis concluded that the role of vitamin A or its derivatives on BMD remain unclear, although most of the included studies showed a favorable effect of vitamin A on BMD [27]. This is also consistent with our results which showed no significant associations between blood retinol levels and BMD or bone strength of the femoral neck.
Antioxidants are important substances for eliminating free radicals. It can reduce the oxidative stress responses in the body and increase BMD. Therefore, consuming adequate amounts of fruits and vegetables can reduce the risk of osteoporosis and its complications, such as pain and fracture [28]. Recent epidemiological evidence concluded that relatively high intakes of antioxidants, including carotenoids [6], vitamin E, vitamin C, and flavonoids were linked to an increased BMD in postmenopausal women [12,13,14, 29]. A recent study reported a causal link between increased circulating α-tocopherol and elevated BMD [30]. Another observational study also found that total dietary antioxidant capacity of as inversely associated with the risk of osteoporosis in postmenopausal women and positively associated with bone mass in both pre- and postmenopausal women [31]. These previous observational studies consistently asserted that the intake of antioxidants may strongly impact BMD in femoral neck. Conversely, our study showed negative associations between blood total lutein, beta-cryptoxanthin, alpha-carotene and all trans-beta-carotene levels and BMD, after adjusting for age and sex. There were no significant associations between blood gamma-tocopherol or alpha-tocopherol concentrations and BMD. A possible reason for this finding is that we included a sample of generally healthy participants in our analyses rather than a specific population, such as postmenopausal women or elderly individuals. Another important reason may be that we measured the participants’ circulating antioxidant levels, rather than assessing fruit and vegetable intake, which was a commonly used method in previous studies. Our results showed that the circulating levels of antioxidants were negatively correlated or uncorrelated with the BMD of the femoral neck, which is an interesting phenomenon and needs to be confirmed in future investigations.
Osteoporosis typically occurs in individuals who are 50 years of age or older. A decrease in bodily hormone levels, particularly in postmenopausal women, leads to the proliferation of osteoclasts and the acceleration in bone loss. Increased fruit and vegetable intake has been related to bone mineral content in premenopausal women [28]. Further, the increased intake of vitamin C was related to higher femur BMD in premenopausal women [32]. These studies suggest that antioxidant intake confers clear benefits on BMD in premenopausal women. Consistently, our study also suggested that blood antioxidant levels were positively associated with femoral neck strength (CSI, BSI and ISI) in female subjects aged ≥ 53 years. These findings confirm that the consumption of antioxidant rich food is beneficial to increase femoral neck strength and may subsequently prevent FNF. Interestingly, we also observed a positive correlation between blood antioxidant levels and femoral neck strength in participants with overweight or obesity (BMI ≥ 24 kg/m2), but not in participants with a normal BMI (BMI < 24 kg/m2). This may suggest that supplementation with antioxidants is beneficial to increase the strength of the femoral neck in individuals with an overweight or obese BMI.
Compared with previous observational studies, our study has several advantages. Our data were obtained from the MIDUS study, which enrolled a representative sample of Americans. The MIDUS II Biomarker Project conducted high-quality assessments on blood samples, which were obtained from a large sample of the general population. Our study included measures of almost all lipid soluble antioxidants, which allowed us to comprehensively analyze the relationships between blood antioxidants and bone strength. In addition to BMD, we also analyzed femoral neck strength indices (CSI, BSI, and ISI), making this the first study to analyze the relationship between blood antioxidants and femoral neck fracture-related indicators. Importantly, the retrospective analyses conducted in the present study did impose some limitations. First, the inherent disadvantages of cross-sectional studies made it difficult to assess causal associations between antioxidants and both BMD and femoral neck bone strength, although the pathological mechanism by which reducing oxidative stress may attenuate bone mass loss is well characterized. Second, the statistical models were adjusted for age, sex, and BMI, but there are other known and unknown confounding variables that were not measured or included in the analyses. For example, we did not include information on disease history, including such conditions as hypertension, coronary heart disease and diabetes, in the analyses. Additionally, data related to menopausal status in females and drug treatment status (e.g., vitamin D supplementation or other drug treatments that may cause osteoporosis) were not included in the analyses. Therefore, the results may be impacted by these factors. Third, 377 samples from the MIDUS II Biomarker Project (N = 1,225) were not analyzed due to missing data, and only data from 878 subjects were included in our study, potentially producing an offset of the sample section.
Conclusion
We comprehensively conducted a cross-sectional analysis of the relationship between blood levels of 10 antioxidants and bone strength of the femoral neck. Our results indicate that increasing blood levels of antioxidants, especially zeaxanthin, may increase femoral neck strength (CSI, BSI, and ISI). These findings supported that antioxidant supplementation can further reduce FNF risk.
Availability of data and materials
The data used in the present study are publicly available through the Inter-University Consortium for Political and Social Research (ICPSR): www.icpsr.umich.edu/web/ICPSR/studies/29282.
Change history
26 May 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12891-023-06535-2
References
Gangji V, Soyfoo MS, Heuschling A, Afzali V, Moreno-Reyes R, Rasschaert J, Gillet C, Fils JF, Hauzeur JP. Non traumatic osteonecrosis of the femoral head is associated with low bone mass. Bone. 2018;107:88–92.
Li L, Ding Y, Liu B, Wang Z, Carlone DL, Yu X, Wei X, Zhang F, Lineaweaver WC, Yang B, Xia W, Wang DZ, Zhao D. Transcriptome landscape of the late-stage alcohol-induced osteonecrosis of the human femoral head. Bone. 2021;150:116012.
Han L, Wang B, Wang R, Gong S, Chen G, Xu W. The shift in the balance between osteoblastogenesis and adipogenesis of mesenchymal stem cells mediated by glucocorticoid receptor. Stem Cell Res Ther. 2019;10(1):377.
Cosman F, McMahon D, Dempster D, Nieves JW. Standard Versus Cyclic Teriparatide and Denosumab Treatment for Osteoporosis: A Randomized Trial. J Bone Miner Res. 2020;35(2):219–25.
Kanis JA, McCloskey EV, Johansson H, Oden A, Melton LJ 3rd, Khaltaev N. A reference standard for the description of osteoporosis. Bone. 2008;42(3):467–75.
Lorentzon M, Cummings SR. Osteoporosis: the evolution of a diagnosis. J Intern Med. 2015;277(6):650–61.
ESHRE Capri Workshop Group. Bone fractures after menopause. Hum Reprod Update. 2010;16(6):761–73.
Ahn SH, Kim H, Kim BJ, Lee SH, Koh JM. Insulin resistance and composite indices of femoral neck strength in Asians: the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Clin Endocrinol (Oxf). 2016;84(2):185–93.
Kimball JS, Johnson JP, Carlson DA. Oxidative Stress and Osteoporosis. J Bone Joint Surg Am. 2021;103(15):1451–61.
Wong RH, ThaungZaw JJ, Xian CJ, Howe PR. Regular Supplementation With Resveratrol Improves Bone Mineral Density in Postmenopausal Women: A Randomized. Placebo-Controlled Trial J Bone Miner Res. 2020;35(11):2121–31.
Hu D, Cheng L, Jiang W. Fruit and vegetable consumption and the risk of postmenopausal osteoporosis: a meta-analysis of observational studies. Food Funct. 2018;9(5):2607–16.
Regu GM, Kim H, Kim YJ, Paek JE, Lee G, Chang N, Kwon O. Association between Dietary Carotenoid Intake and Bone Mineral Density in Korean Adults Aged 30–75 Years Using Data from the Fourth and Fifth Korean National Health and Nutrition Examination Surveys (2008–2011). Nutrients. 2017;9(9):1025.
Odai T, Terauchi M, Hirose A, Kato K, Miyasaka N. Bone Mineral Density in Premenopausal Women Is Associated with the Dietary Intake of α-Tocopherol: A Cross-Sectional Study. Nutrients. 2019;11(10):2474.
Hardcastle AC, Aucott L, Reid DM, Macdonald HM. Associations between dietary flavonoid intakes and bone health in a Scottish population. J Bone Miner Res. 2011;26(5):941–7.
Kim YA, Kim KM, Lim S, Choi SH, Moon JH, Kim JH, Kim SW, Jang HC, Shin CS. Favorable effect of dietary vitamin C on bone mineral density in postmenopausal women (KNHANES IV, 2009): discrepancies regarding skeletal sites, age, and vitamin D status. Osteoporos Int. 2015;26(9):2329–37.
Sugiura M, Nakamura M, Ogawa K, Ikoma Y, Yano M. High Vitamin C Intake with High Serum β-Cryptoxanthin Associated with Lower Risk for Osteoporosis in Post-Menopausal Japanese Female Subjects: Mikkabi Cohort Study. J Nutr Sci Vitaminol (Tokyo). 2016;62(3):185–91.
Wattanapenpaiboon N, Lukito W, Wahlqvist ML, Strauss BJ. Dietary carotenoid intake as a predictor of bone mineral density. Asia Pac J Clin Nutr. 2003;12(4):467–73.
Brim OG, Ryff CD, Kessler RC. The MIDUS national survey: an overview. 392. In: Brim OG, Ryff CD, Kessler RC, editors. How Healthy Are We? A National 393 Study of Well-Being at Midlife. Chicago: University of Chicago Press; 2004. p. 1–36.
Ryff CD, Seeman T, Weinstein M. Midlife in the United States (MIDUS 2): Biomarker Project, 2004–2009 (ICPSR 29282; Version V9). ICPSR. 2019. https://doi.org/10.3886/ICPSR29282.v9.
Dienberg Love G, Seeman TE, Weinstein M, Ryff CD. Bioindicators in the MIDUS national study: protocol, measures, sample, and comparative context. J Aging Health. 2010;22(8):1059–80.
Khosla S. Pathogenesis of age-related bone loss in humans. J Gerontol A Biol Sci Med Sci. 2013;68(10):1226–35.
Mosekilde L. Sex differences in age-related loss of vertebral trabecular bone mass and structure–biomechanical consequences. Bone. 1989;10(6):425–32. https://doi.org/10.1016/8756-3282(89)90074-4.
Zhang ZQ, Cao WT, Liu J, Cao Y, Su YX, Chen YM. Greater serum carotenoid concentration associated with higher bone mineral density in Chinese adults. Osteoporos Int. 2016;27(4):1593–601.
Dai Z, Wang R, Ang LW, Low YL, Yuan JM, Koh WP. Protective effects of dietary carotenoids on risk of hip fracture in men: the Singapore Chinese Health Study. J Bone Miner Res. 2014;29(2):408–17.
Bovier ER, Hammond BR. The Macular Carotenoids Lutein and Zeaxanthin Are Related to Increased Bone Density in Young Healthy Adults. Foods. 2017;6(9):78.
Ostman B, Michaëlsson K, Helmersson J, Byberg L, Gedeborg R, Melhus H, Basu S. Oxidative stress and bone mineral density in elderly men: antioxidant activity of alpha-tocopherol. Free Radic Biol Med. 2009;47(5):668–73.
Khojah Q, AlRumaihi S, AlRajeh G, Aburas A, AlOthman A, Ferwana M. Vitamin A and its dervatives effect on bone mineral density, a systematic review. J Family Med Prim Care. 2021;10(11):4089–95.
Li JJ, Huang ZW, Wang RQ, Ma XM, Zhang ZQ, Liu Z, Chen YM, Su YX. Fruit and vegetable intake and bone mass in Chinese adolescents, young and postmenopausal women. Public Health Nutr. 2013;16(1):78–86.
Zeng LF, Luo MH, Liang GH, Yang WY, Xiao X, Wei X, Yu J, Guo D, Chen HY, Pan JK, Huang HT, Liu Q, Guan ZT, Han YH, Zhao D, Zhao JL, Hou SR, Wu M, Lin JT, Li JH, Liang WX, Ou AH, Wang Q, Li ZP, Liu J. Can Dietary Intake of Vitamin C-Oriented Foods Reduce the Risk of Osteoporosis, Fracture, and BMD Loss? Systematic Review With Meta-Analyses of Recent Studies. Front Endocrinol (Lausanne). 2020;3(10):844.
Michaëlsson K, Larsson SC. Circulating Alpha-Tocopherol Levels, Bone Mineral Density, and Fracture: Mendelian Randomization Study. Nutrients. 2021;13(6):1940.
Kim D, Han A, Park Y. Association of Dietary Total Antioxidant Capacity with Bone Mass and Osteoporosis Risk in Korean Women: Analysis of the Korea National Health and Nutrition Examination Survey 2008–2011. Nutrients. 2021;13(4):1149.
Macdonald HM, New SA, Golden MH, Campbell MK, Reid DM. Nutritional associations with bone loss during the menopausal transition: evidence of a beneficial effect of calcium, alcohol, and fruit and vegetable nutrients and of a detrimental effect of fatty acids. Am J Clin Nutr. 2004;79(1):155–65.
Acknowledgements
Not applicable.
Funding
This study was not supported by any funding.
Author information
Authors and Affiliations
Contributions
Peng Niu wrote the main manuscript; Yongxi Liu and Yanfeng Zhang completed the validation; Lei Li revised the draft. All authors reviewed the manuscript. The author(s) read and approved the final manuscript.
Author information
Not applicable.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations, and approval from appropriate Institutional Review Boards at the Midlife in the United States (MIDUS) study centers was granted for this study and all participants gave informed consent before participation. We retrospectively analyzed MIDUS data from an open database (ICPSR).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: an article note (The affiliation “The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou City, 324002, Zhejiang Province, China” of Dr. Lei Li is the main or first institution of this research.) was added to emphasize the main institution of this research.
The affiliation “The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou City, 324002, Zhejiang Province, China” of Dr. Lei Li is the main or first institution of this research.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Niu, P., Liu, Y., Zhang, Y. et al. Associations between blood antioxidant levels and femoral neck strength. BMC Musculoskelet Disord 24, 252 (2023). https://doi.org/10.1186/s12891-023-06370-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06370-5