
Abstract
Background
Type 2 diabetes mellitus (T2DM) is associated with the increased incidence rate of sarcopenia and osteoporosis. Serum creatinine-to-cystatin C ratio (CCR) is a novel and simple tool which can be used as an index of sarcopenia. This study aims to investigate the association between CCR and osteoporosis as well as bone mineral density (BMD) in T2DM patients.
Methods
Four hundred eighteen T2DM patients were recruited, including 166 females and 252 males. General information, BMD data and laboratory data were collected. The correlation between CCR, BMD, bone metabolism markers and osteoporosis was explored by spearman correlation, receiver-operating characteristic (ROC) curve analysis and multiple regression analysis.
Results
Spearman correlation analysis showed that there was a positive correlation between CCR and BMD as well as serum calcium in male patients (r = 0.181–0.381, P < 0.01), but such correlation was not found in the female group. In multivariate regression analysis, it was found that there was a significant correlation between CCR and BMD of total lumbar spine, hip as well as femoral neck in male patients. ROC curve showed that the optimal cut-off value of CCR for predicting osteoporosis in male patients was 6.73 with the sensitivity of 88% and specificity of 63%.
Conclusion
In male T2DM patients, CCR was negatively correlated with osteoporosis and positively correlated with BMD.
Similar content being viewed by others

Introduction
Fractures and osteoporosis show a rising trend in the elderly, which can result in disability, decline in quality of life, and even death [1]. Patients with T2DM are generally more likely to suffer from fracture than the general population [2, 3]. Previous studies have analyzed and reported risk factor associated with osteoporosis in the general population [4]. However, it is important to explore the risk factors for osteoporosis, which may differ from those with T2DM due to metabolic disorders.
Sarcopenia, a geriatric disease characterized by a progressive loss of skeletal muscle mass and loss of muscle function, constitutes a rising, often undiagnosed health problem. The relationship between the sarcopenia and osteoporosis in chronic obstructive pulmonary disease [5], chronic kidney disease [6], primary biliary cholangitis [7] has been well developed. It is also confirmed that skeletal muscle mass is independently associated with osteoporosis in patients with T2DM [8]. However, traditional skeletal muscle mass inspection methods, such as dual-energy-X-ray absorption method, are complex and expensive.
Serum creatinine is a metabolic waste produced by skeletal muscle. Cystatin C can be produced by nucleated cells in the body at a constant production rate, which can only be removed through glomerular filtration. Some studies have supported that the creatinine-to-cystatin C ratio (CCR) can be used as a biomarker of skeletal muscle mass. Takafumi et al. suggested that CCR is an inexpensive and simple method to detect sarcopenia in T2DM patients [9]. However, whether this ratio can be used as a predictor of osteoporosis in `T2DM has not been studied. Therefore, this study aims to explore the relationship between CCR, osteoporosis and BMD in patients with T2DM.
Methods
Subjects
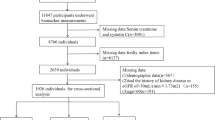
The study included 418 T2DM patients (age > 50 years old) in China. The subjects were evaluated or treated for T2DM at the Second Affiliated Hospital of Wenzhou Medical University and Yuying Children's Hospital from January 2020 to March 2021. Because serum cystatin C does not increase in those with severely impaired kidney function while serum creatinine dose increase [10, 11], we selected patients with normal renal function (glomerular filtration rate > 60 ml/min, creatine ≤ 115µmmol/L). Exclusion criteria included (a) malignant tumors and severe heart or liver diseases; (b) diagnosis of adrenal, gonadal, parathyroid, pituitary and thyroid diseases; (c) long-term use of calcium, vitamin D, or other drugs that influence bone metabolism for more than three months; (d) patients who were bedridden for a long time; and (e) patients who lacked available information. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (No. LCKY2020-03, date: January 2020), and the written informed consent of all participants obtained according to the Declaration of Helsinki.
Health history and clinical assessment
Their height and weight without wearing shoes were measured. BMI was calculated by dividing weight (Kg) by the square of height (m2). The duration of T2DM was calculated in years, which ranged from the diagnosis of T2DM in medical record of patient's to our BMD measurements and blood tests. Smoking and drinking history were considered as never or ever.
Biochemical parameters
Serum samples were collected at 6 am after fasting at night (at least 8 h). Cobas c702 chemistry autoanalyzer (Roche Diagnostics, Switzerland) methods were used to measure serum lipid metabolism indicators, including high density lipoprotein cholesterol (HDL-C), total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), triglyceride (TG); glucose metabolism indicators, including (FBG) fasting blood glucose, (HbA1c) glycosylated hemoglobin; Bone metabolism indicators, including β-CTX, PINP, 25-hydroxy-vitamin (25(OH)D) and parathyroid hormone (PTH); other laboratory markers such as creatinine, calcium, uric and albumin. Serum cystatin C concentrations were detected using an immunoturbidimetric technique with the Modular Analytics Cobas 6000 analyzer (Roche Diagnostics, Switzerland). The CCR was then calculated as the serum creatine concentration (mg/L) divided by the cystatin C concentration (mg/L).
BMD measurement
Whole-body dual-energy X-ray absorptiometry (DXA; USA, Hologic Discovery) was used to measure body fat content, trunk muscle mass and BMD of the lumbar spine, femur neck, total hip and skeletal muscle mass index (ASMI). The calculation formula of ASMI is as follows: appendicular skeletal muscle mass (ASM)/height2 [12]. T scores was calculated by using the DXA database [13]. Osteoporosis, osteopenia, and normal bone mass was determined based on the following T-scores: ≤ − 2.5, − 2.5 to 1.0, and > − 1.0, respectively, in the total hip, femoral neck, or lumbar area [13].
Statistical analysis
The proportion was used to describe categorical variables and mean ± standard deviation to describe continuous variables. Intergroup differences were evaluated using one-way analysis of variance for normally distributed variables, using the Mann–Whitney U test for non-normally distributed variables, and using the chi-squared test for categorical variables. The BMD as well as incident of osteoporosis was different between genders; as a result, male and female were independently analyzed. Spearman coefficient was used to analyze CCR, BMD and bone metabolism index. Each parameter was selected for which P value < 0.05 in initial univariate results, age, diabetic duration, BMI, smoking, drinking, TC, TG, HDL-C, LDL-C, albumin, uric, HbA1c, FBG and CCR for the multivariate analyses for the correlation between BMD of femoral neck, lumbar spine, hip and other variables. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by Logistic analysis. We plotted the receiver operating characteristic (ROC) curve and calculated the area under the curve (AUC) to assess the clinical value of CCR in predicting osteoporosis. In order to make CCR significantly different between osteoporosis group and normal group, with α = 0.05, two-tailed and a power of 80%, we needed at least 33 patients per group.
Results
Basic characteristics
Patient characteristics are shown in Table 1. The retrospective study included 418 T2DM patients with a BMI of 24.5 ± 3.2 kg/m2 and an average age of 60.8 ± 7.3 years old. The BMD of the hip, femur neck and lumbar spine were higher in males (1.007 vs 0.903, 0.941 vs 0.826, 1.194 vs 1.012, all P < 0.01) compared with females. The levels of HDL-c, FBG, HbA1c, LDL-c, PINP, β-CTX and the incidence of osteoporosis in males were significantly lower than those in females. The levels of creatinine, cystatin C, CCR and ASM/height2 were significantly higher in males than those in females.
Comparison of CCR, and other biochemical and clinical indicators in T2DM patients with normal BMD values, osteoporosis and osteopenia
Based on the BMD T score measured by DXA, T2DM patients were divided into normal BMD, osteoporosis and osteopenia groups (Table 2). Compared with normal BMD group, BMI, albumin, creatinine, uric and ASM/height2 were significantly reduced and age, diabetic duration, FBG, cystatin C, PINP and β-CTX levels significantly increased in the osteoporosis and osteopenia groups. The BMD of the total hip, femur neck and total lumbar spine in the osteoporosis and osteopenia groups were significantly decreased. Compared with the normal BMD group, the level of CCR in osteoporosis group was lower.
Spearman correlations analysis between CCR, BMD and bone metabolism index
The Spearman correlation coefficients (r) of CCR and BMD of lumbar, femur neck, hip, PTH, serum Ca, ASM/height2 were 0.381, 0.302, 0.323, -0.141, 0.181 and0.215 in male groups, respectively. However, CCR was not correlated with the BMD in female groups (Table 3).
Linear regression analyses for BMD
Age, BMI and HbA1c had a significant effect on osteoporosis prevalence. Accordingly, subgroup analysis was performed based on BMI, age and HbA1c (Table 4). After adjusting age, diabetic duration, BMI, smoking, drinking, TC, TG, HDL-C, LDL-C, albumin, uric, HbA1c and FBG, CCR had an independent relationship with the BMD of the femoral neck, lumbar spine, and hip in the male group, but that among female patients was not significant.
Logistic regression analyses of male osteoporosis
Logistic regression analysis was used to test the association between CCR and osteoporosis (Table 5). Although the odds ratio decreased after adjusting age, diabetic duration, BMI, smoking, drinking, TC, TG, HDL-C, LDL-C, albumin, uric, HbA1c and FBG, the correlation between CCR and osteoporosis remained significant in male patients (odd ratio = 0.498, P < 0.031), but the female group did not show such relationship.
Prognostic value of CCR
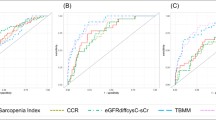
ROC curve analysis related to the impact of CCR on the diagnosis of osteoporosis in male group (Fig. 1). The area under ROC curve was 0.788. The optimal cut-off value of CCR for predicting osteoporosis was 6.73 with the sensitivity of 88% and the specificity of 63%.

ROC curve analysis related to the impact of CCR on the osteoporosis in male group
Discussion
As far as we know, this study is the first to investigate the relationship between CCR, osteoporosis and BMD in patients in T2DM patients. The main finding of this study is that in male T2DM patients, CCR is positively correlated with BMD, at total hip, lumbar and femur neck, and negatively correlated with osteoporosis.
Reduced muscle mass, or sarcopenia, is a well-known risk factor for osteoporosis. Reduced muscle mass affects balance and thereby increases the risk of falls and subsequent fractures [14]. In this way, gradual age-related decline in bone and muscle (i.e., osteoporosis and sarcopenia) can result in increased morbidity and mortality [15]. Considering the close relationship between sarcopenia and osteoporosis and the effects of muscle mass on fracture risk, identification and treatment of those conditions is important in older populations. Therefore, recent studies have suggested a more inclusive name be given to the combination of sarcopenia and osteoporosis, such as ‘dysmobility syndrome,’ which integrates their pathogenesis and unites them as a single therapeutic target [16]. However, although osteoporosis has been clearly defined, the definition of sarcopenia remains unclear [17]. In addition, although DXA is the currently accepted gold standard test for evaluating body composition, including both bone density and muscle mass [18], it is not easily accessible or commonly available to general populations because of time and cost. From this background, we hypothesized that CCR, known to be a stable marker of sarcopenia [19], could be related to bone health status.
Serum creatinine reflects one’s physical activity status as well as skeletal muscle mass, and both are important for maintaining bone health [20]. In addition, creatinine degradation is stimulated by reactive oxygen species and in particular by the hydroxyl radical. Fernández-Real et al. reported that telomere length of subcutaneous adipose tissue cells was positively associated with serum creatinine but not with GFR. In other words, decreased serum creatinine is associated with a marker of cellular senescence and oxidative stress and consequently decreased serum creatinine may result in deterioration of BMD via oxidative stress [21].
Cystatin C is significantly associated with renal function. 1,25-dihydroxyvitamin D synthesis is decreased even in mild renal impairment, leading to reduced calcium absorption, secondary hyperparathyroidism, bone loss, and consequently, fracture [22, 23]. Taken together, we can speculate that CCR, a cheap and simple method, can be used as a marker to assess osteoporosis in type 2 diabetes and it can be also alternative for body composition analysis in subjects with normal renal function.
The association between CCR and sarcopenia has been established among the subjects with chronic obstructive pulmonary disease [24], advanced cancer [25], obstructive coronary artery disease [26] and healthy subjects [27]. Takafumi et al. recommend CCR as a practical screening marker for sarcopenia in T2DM patients [9]. Our findings are consistent with previous studies. It is found that CCR is positively associated with ASM/height2 in male group (r = 0.215, P = 0.002), but such relationship is not found in female group.
Reduced muscle mass can result in the worsening of insulin sensitivity, which in turn can result in diabetes [28]. Diabetes and other systemic diseases caused by sarcopenia can lead to both abnormal bone metabolism and muscle loss [29]. Our results suggest that low CCR is an important risk factor for osteoporosis and decreased BMD in male T2DM patients. As far as we know, this study is the first to show a direct correlation between CCR, osteoporosis and BMD in patients with T2DM.
The analysis of BMI, age, HbA1c subgroups further showed that among the male patients with higher BMI, older age and higher glycosylated hemoglobin levels, the association between CCR and bone mineral density was higher than that in the control group. Accordingly, for the above patients, CCR may be a simple predictor of BMD in male T2DM.
CCR is an important component of sarcopenia and a predictor of various adverse health outcomes. Lu et al. found that subjects with low CCR is a risk factor for adverse cardiovascular events in patients with obstructive coronary artery disease [9]. Liu et al. suggested that low CCR is a risk factor for long-term poor prognosis and 30-day mortality and in Acute Ischemic Stroke Patients [30]. Qiu et al. reported that low CCR can lead to increased risk of diabetes [31]. Therefore, it is valuable to identify patients with sarcopenia in clinical practice.
In our study, CCR is negatively associated with osteoporosis in male group (OR = 0.498, P = 0.031), but the female group does not show such relationship, Which has been confirmed in previous studies that male have a closer relationship between bone mass and muscle mass than in females [32,33,34]. Although we could not elucidate why this association was more prominent in men than in women, it might be explained by the fact that females tend to have lower skeletal muscle mass than males. Additionally, increased body fat in postmenopausal women might alter the bone-muscle (CCR) relationship. Conversion of androgens to estrogens in adipose tissue could have a modest effect on bone, especially in postmenopausal women [35]. However, in men, adipose tissue is not an important sex hormone source and as they have relatively small fat mass, it may not considerably influence on the bone-muscle (CCR) relationship [36].
Compared with traditional detection methods such as CT, dual-energy-X-ray absorptiometry and bioimpedance analysis, CCR detection only requires blood sampling, which is easy to be analyzed, and does not require the patients to bear the high costs of detection. As a result, CCR is more acceptable. In addition, the CCR results are easy to understand and intuitive. Therefore, it is more convenient for clinicians to use the CCR to assess osteoporosis.
This study has several limitations. First of all, it had a retrospective design, a relatively small size, and was conducted at a single hospital. Secondly, we do not know the causal relationship between osteoporosis and the CCR because of the cross-sectional design. Thirdly, we do not consider the dietary intake of meat, or drugs, such as cimetidine, determination of exercise. These factors may change creatinine levels and affect CCR. Fourthly, the concentrations of serum cystatin C and creatinine is significantly affected by renal function, suggesting that the CCR may not be suitable for identifying osteoporosis in patients with abnormal renal function, and the prevalence of osteoporosis in patients with chronic kidney diseases is relatively high [37].
Conclusion
In summary, this study reported for the first time that lower CCR is closely related to osteoporosis and low BMD in male T2DM patients. When the diagnostic cut-off value of male CCR is 6.73, the risk of osteoporosis increase, with a sensitivity of 88% and a specificity of 63%.
Availability of data and materials
The data that support the findings of this study are available from Institutional Review Board of the second affiliated hospital and Yuying Children’s Hospital of Wenzhou Medical University but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Institutional Review Board of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University.
Change history
01 August 2022
A Correction to this paper has been published: https://doi.org/10.1186/s12891-022-05707-w
Abbreviations
- CCR:
-
Creatinine-to-cystatin C ratio
- BMD:
-
Bone Mineral Density
- FBG:
-
Fasting blood glucose
- BMI:
-
Body mass index
- HbA1c:
-
Glycosylated hemoglobin
- 25(OH)D:
-
25-Hydroxy-vitamin
- PTH:
-
Parathyroid hormone
References
Lin X, Xiong D, Peng YQ, Sheng ZF, Wu XY, Wu XP, Wu F, Yuan LQ, Liao EY. Epidemiology and management of osteoporosis in the People’s Republic of China: current perspectives. Clin Interv Aging. 2015;10:1017–33.
Janghorbani M, Van Dam RM, Willett WC, Hu FB. Systematic review of type 1 and type 2 diabetes mellitus and risk of fracture. Am J Epidemiol. 2007;166(5):495–505.
Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes–a meta-analysis. Osteoporos Int. 2007;18(4):427–44.
Holm JP, Hyldstrup L, Jensen JB. Time trends in osteoporosis risk factor profiles: a comparative analysis of risk factors, comorbidities, and medications over twelve years. Endocrine. 2016;54(1):241–55.
Chua JR, Tee ML. Association of sarcopenia with osteoporosis in patients with chronic obstructive pulmonary disease. Osteoporos Sarcopenia. 2020;6(3):129–32.
Kim JE, Lee YH, Huh JH, Kang DR, Rhee Y, Lim SK. Early-stage chronic kidney disease, insulin resistance, and osteoporosis as risk factors of sarcopenia in aged population: the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV), 2008–2009. Osteoporos Int. 2014;25(9):2189–98.
Saeki C, Oikawa T, Kanai T, Nakano M, Torisu Y, Sasaki N, Abo M, Saruta M, Tsubota A. Relationship between osteoporosis, sarcopenia, vertebral fracture, and osteosarcopenia in patients with primary biliary cholangitis. Eur J Gastroenterol Hepatol. 2021;33(5):731–7.
Pan Y, Xu J. Association between muscle mass, bone mineral density and osteoporosis in type 2 diabetes. J Diabetes Investig. 2022;13(2):351–8.
Osaka T, Hamaguchi M, Hashimoto Y, Ushigome E, Tanaka M, Yamazaki M, Fukui M. Decreased the creatinine to cystatin C ratio is a surrogate marker of sarcopenia in patients with type 2 diabetes. Diabetes Res Clin Pract. 2018;139:52–8.
Dai H, Xu J. Preoperative geriatric nutritional risk index is an independent prognostic factor for postoperative survival after gallbladder cancer radical surgery. BMC Surg. 2022;22(1):133.
Sjostrom P, Tidman M, Jones I. Determination of the production rate and non-renal clearance of cystatin C and estimation of the glomerular filtration rate from the serum concentration of cystatin C in humans. Scand J Clin Lab Invest. 2005;65(2):111–24.
Gojanovic M, Holloway-Kew KL, Hyde NK, Mohebbi M, Shivappa N, Hebert JR, O’Neil A, Pasco JA. The dietary inflammatory index is associated with low muscle mass and low muscle function in older Australians. Nutrients. 2021;13(4):1166.
Kanis JA. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos Int. 1994;4(6):368–81.
Liu-Ambrose T, Eng JJ, Khan KM, Carter ND, McKay HA. Older women with osteoporosis have increased postural sway and weaker quadriceps strength than counterparts with normal bone mass: overlooked determinants of fracture risk? J Gerontol A Biol Sci Med Sci. 2003;58(9):M862–6.
Bonewald LF, Kiel DP, Clemens TL, Esser K, Orwoll ES, O’Keefe RJ, Fielding RA. Forum on bone and skeletal muscle interactions: summary of the proceedings of an ASBMR workshop. J Bone Miner Res. 2013;28(9):1857–65.
Binkley N, Krueger D, Buehring B. What’s in a name revisited: should osteoporosis and sarcopenia be considered components of “dysmobility syndrome?” Osteoporos Int. 2013;24(12):2955–9.
Cooper C, Dere W, Evans W, Kanis JA, et al. Frailty and sarcopenia: definitions and outcome parameters. Osteoporos Int. 2012;23(7):1839–48.
Haderslev KV, Haderslev PH, Staun M. Accuracy of body composition measurements by dual energy x-ray absorptiometry in underweight patients with chronic intestinal disease and in lean subjects. Dyn Med. 2005;4(1):1.
Patel SS, Molnar MZ, Tayek JA, Ix JH, Noori N, Benner D, Heymsfield S, Kopple JD, Kovesdy CP, Kalantar-Zadeh K. Serum creatinine as a marker of muscle mass in chronic kidney disease: results of a cross-sectional study and review of literature. J Cachexia Sarcopenia Muscle. 2013;4(1):19–29.
Baxmann AC, Ahmed MS, Marques NC, Menon VB, Pereira AB, Kirsztajn GM, Heilberg IP. Influence of muscle mass and physical activity on serum and urinary creatinine and serum cystatin C. Clin J Am Soc Nephrol. 2008;3(2):348–54.
Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev. 2000;80(3):1107–213.
Francis RM, Peacock M, Barkworth SA. Renal impairment and its effects on calcium metabolism in elderly women. Age Ageing. 1984;13(1):14–20.
Vieth R, Ladak Y, Walfish PG. Age-related changes in the 25-hydroxyvitamin D versus parathyroid hormone relationship suggest a different reason why older adults require more vitamin D. J Clin Endocrinol Metab. 2003;88(1):185–91.
Hirai K, Tanaka A, Homma T, Goto Y, Akimoto K, Uno T, Yoshitaka U, Miyata Y, Inoue H, Ohta S, et al. Serum creatinine/cystatin C ratio as a surrogate marker for sarcopenia in patients with chronic obstructive pulmonary disease. Clin Nutr. 2021;40(3):1274–80.
Fu X, Tian Z, Wen S, Sun H, Thapa S, Xiong H, Liu H, Li L, Yu S. A new index based on serum creatinine and cystatin C is useful for assessing sarcopenia in patients with advanced cancer. Nutrition. 2021;82:111032.
Lu YW, Tsai YL, Chou RH, Kuo CS, Chang CC, Huang PH, Lin SJ. Serum creatinine to cystatin C ratio is associated with major adverse cardiovascular events in patients with obstructive coronary artery disease. Nutr Metab Cardiovasc Dis. 2021;31(5):1509–15.
Tabara Y, Okada Y, Ochi M, Ohyagi Y, Igase M. Association of creatinine-to-cystatin c ratio with myosteatosis and physical performance in older adults: the Japan shimanami health promoting program. J Am Med Dir Assoc. 2021;22(11):2366-2372.e3.
Srikanthan P, Hevener AL, Karlamangla AS. Sarcopenia exacerbates obesity-associated insulin resistance and dysglycemia: findings from the national health and nutrition examination survey III. PLoS One. 2010;5(5):e10805.
Landi F, Cruz-Jentoft AJ, Liperoti R, Russo A, Giovannini S, Tosato M, Capoluongo E, Bernabei R, Onder G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: results from ilSIRENTE study. Age Ageing. 2013;42(2):203–9.
Liu W, Zhu X, Tan X, Yang L, Wang Y, Diao S, Huang S, Zhang X, Yang Y, Ni J. Predictive Value of Serum Creatinine/Cystatin C in Acute Ischemic Stroke Patients under Nutritional Intervention. J Nutr Health Aging. 2021;25(3):335–9.
Qiu S, Cai X, Yuan Y, Xie B, Sun Z, Wu T. Changes in creatinine-to-cystatin C ratio over 4 years, risk of diabetes, and cardiometabolic control: the China health and retirement longitudinal study. J Diabetes. 2021;13(12):1025–33.
Zofkova I. Hormonal aspects of the muscle-bone unit. Physiol Res. 2008;57(Suppl 1):S159-169.
Macdonald H, Kontulainen S, Petit M, Janssen P, McKay H. Bone strength and its determinants in pre- and early pubertal boys and girls. Bone. 2006;39(3):598–608.
Lang TF. The bone-muscle relationship in men and women. J Osteoporos. 2011;2011:702735.
Thomas T, Burguera B. Is leptin the link between fat and bone mass? J Bone Miner Res. 2002;17(9):1563–9.
Mudali S, Dobs AS. Effects of testosterone on body composition of the aging male. Mech Ageing Dev. 2004;125(4):297–304.
Hsu CY, Chen LR, Chen KH. Osteoporosis in patients with chronic kidney diseases: a systemic review. Int J Mol Sci. 2020;21(18):6846.
Acknowledgements
The authors thank research staff, all subjects, and students who participated in this study.
Funding
Zhejiang Provincial Department of Health(2016KYB194), General Research Project of Zhejiang Provincial Education Department(Y201534290), Wenzhou Science and Technology Bureau(Y20120163).
Author information
Authors and Affiliations
Contributions
HFD – study concept and design; preparation, review and approval of manuscript. JX – data collection and interpretation; preparation, review and approval of manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (No. LCKY2020-03, date: January 2020), and obtained the written informed consent of all participants according to the Declaration of Helsinki. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: the first author Huifan Dai needs to be changed to Huifang Dai; and the author department of Huifang Dai is the same as that of Jing Xu.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dai, H., Xu, J. Creatinine-to-cystatin C ratio as a marker of sarcopenia for identifying osteoporosis in male patients with type 2 diabetes mellitus. BMC Musculoskelet Disord 23, 672 (2022). https://doi.org/10.1186/s12891-022-05636-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05636-8