
Abstract
Background
Low back pain (LBP) is a common cause of contact with the primary healthcare sector. In some patients, symptoms quickly resolve, but others develop long-lasting pain and disability. To improve the care pathway for patients with LBP, the STarT Back Tool (STarT) questionnaire has been developed. It helps initial decision-making by subgrouping patients on the basis of their prognosis and helps to target treatment according to prognosis. An assumption behind the use of STarT is the ability to predict functional improvement. This assumption has never been tested in a population that consists exclusively of patients enrolled when consulting a Danish general practitioner for LBP. The aim of this study was to investigate STarT’s ability to predict a 30% improvement in the Roland Morris Disability Questionnaire (RMDQ) score.
Methods
This was an ancillary analysis using data from a Danish guideline implementation study (registered at ClinicalTrials.gov NCT01699256). An inclusion criterion was age 18 to 65 years of age. Exclusion criteria were pregnancy, fractures, and signs of underlying pathology. Patient-reported STarT score and the Roland Morris Disability Questionnaire were administered at baseline and again after 4, 8, and 52 weeks.
Results
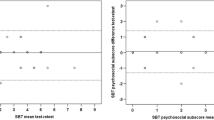
Between January 2013 and July 2014, 475 patients from the original trial participated with questionnaires. From this subpopulation, 441 (92.8%) patients provided information regarding STarT. Baseline and eight-week RMDQ data were available for 304 (64.0%) patients. After 8 weeks, 61 (65.6%) in the low-risk group, 67 (54.9%) in the medium-risk group, and 33 (37.1%) in the high-risk group had achieved a 30% improvement in the RMDQ score. After 8 weeks, high-risk patients were at 61% (95% CI: 20–125%, P < 0.001) higher risk of not achieving a 30% improvement in the RMDQ score compared with patients in either the low-risk group or the medium-risk group.
Conclusion
STarT was predictive for functional improvement in patients from general practice with LBP.
Trial registration
ClinicalTrials.gov NCT01699256, Nov 29, 2016 (registered retrospectively).
Similar content being viewed by others

Background
The Global Burden of Disease study showed that low back pain (LBP) is very common, with an estimated point-prevalence of 9.4% and, therefore, a leading contributor to disability worldwide [1]. Most episodes of LBP only last a few days, but many patients with LBP experience recurrent symptoms, and up to 45% of patients complaining of LBP who consult primary care physicians will have LBP after 1 year [2, 3]. The underlying causes of LBP are often unknown but are in many cases multifactorial, including both biological [4] and psychosocial factors that may be important for pain and recovery [5,6,7]. A multitude of different treatments exist, including general information on LBP, general exercises to improve the patients’ overall physical condition, specific strengths or flexibility exercises targeted at a specific physical problem, treatments aimed at work or ergonomic-related issues, personal problems, problems with family and social life, manual therapy, massage, yoga, and cognitive behavioural therapy [8,9,10]. Furthermore, treatments can be delivered to individuals or to groups; treatments can be supervised and performed in the healthcare setting or instructed/agreed upon to be performed at patients’ homes, public places, or at sport clubs. Hence, as the reason underlying LBP is often multifactorial, and the care of patients is complex; methods to support targeted treatment can avoid the treatment of patient characteristics unrelated to the patients’ pain [11]. Therefore, tools that are able to guide initial decision-making and that can improve care are needed. Subgrouping patients into risk strata by the STarT Back Tool (STarT) has been suggested to target treatment to modifiable factors that are causally related to outcome among sub-groups of patients presenting with LBP in primary care [12].
The STarT back tool
STarT integrates biological, psychological, and social factors and includes nine questions that are used to subgroup patients into a low-, medium- or high-risk subgroup according to the risk of persistent disabling pain [13]. For each subgroup, the STarT follows a set of recommendations for treatment. Patients in the low-risk group are recommended to receive information on LBP and advice to stay as physically active as possible and to continue daily activities. Supplementary to information and advice, GPs are expected to recommend standardized treatment focusing on addressing physical symptoms and function to patients in the medium-risk group. In addition, healthcare professionals are expected to pay special attention to cognitive behaviour to address psychosocial obstacles to recovery for patients in the high-risk group [14]. The STarT has been found to be effective in predicting functional outcomes and has also been found to be effective when applied in two large studies in UK settings [15, 16]. Currently, stratification by the STarT is recommended in the newly published NICE guidelines [10].
Predictive ability of the STarT back tool
Numerous studies performed in different healthcare settings have tested the predictive ability of the STarT. The findings from these studies are inconclusive, hampering widespread use across different healthcare settings [17,18,19,20,21,22,23,24]. In a recent guideline implementation trial for patients with LBP, a subgroup of patients completed a range of questionnaires, including the STarT at baseline and the Roland-Morris Disability Questionnaire (RMDQ), after 4, 8, and 52 weeks [25]. These data provide the opportunity to perform an ancillary analysis of the guideline implementation trial and study the STarT’s predictive ability in a population consisting solely of patients consulting general practice. In a UK primary care setting, a 30% improvement between baseline and follow-up has been estimated as guidance for defining clinically relevant improvement in function when applying the RMDQ [26].
The aim
The aim was to study whether the STarT score for patients consulting general practice with LBP was predictive of a functional improvement of 30% in the RMDQ score after 8 weeks.
Methods
Design and setting
This was an ancillary analysis of a cluster randomised controlled trial on guideline implementation for LBP in Danish general practice. Reporting of the present study follows the STROBE Statement [27].
From January 2013 to July 2014, 60 general practices in the North Denmark Region participated in a guideline implementation trial. The cluster randomised controlled trial compared two strategies for supporting the implementation of LBP guidelines with the primary aim of reducing the referral of patients from primary care to secondary care. General practices in the intervention group had an outreach visit from a guideline facilitator, were offered access to feedback on their treatment of low back pain, and had the opportunity to score their patients with STarT (which was embedded in their electronic medical record). The GPs’ STarT scoring results are not reported in this study. Practices participating in the guideline implementation study had a project module installed in their electronic medical record system, and GPs were encouraged to perform diagnostic coding during consultations with LBP patients [25]. The International Coding for Primary Care (ICPC-2) diagnostic codes L02, L03, L84, and L86 [28] triggered a pop-up in the medical record system. If a patient met the inclusion criteria, the GP invited the patient to participate in the guideline implementation study. The inclusion criteria were consulting general practice with LBP of any duration for the first time within 3 months, age 18 to 65 years, with or without associated radiculopathy, and a complete STarT questionnaire at baseline. The exclusion criteria were insufficient language skills to fill out questionnaires in Danish, pregnancy, and serious underlying disease (e.g., signs of fracture, osteoporosis, cauda equina syndrome, malignancy, or spinal inflammatory arthritis) [29]. Patients consenting to participate in the guideline implementation study were informed that participation with questionnaires was not a requirement for study participation, but they were encouraged to do so. For this ancillary analysis, we included patients from both the intervention group and the control group who filled in the RMDQ and had a complete STarT questionnaire at baseline. Patients with perfect function (RMDQ = 0) at baseline were excluded.
Patients filled in a questionnaire at home after the initial consultation and were sent follow-up questionnaires after four, eight, and 52 weeks. Patients could choose to complete the questionnaires on the internet or to fill out and return paper versions. Paper versions of the questionnaires were sent to the research unit in a prepaid envelope and the responses were typed into the database by two of the researchers (AR and CEJ). When completing the questionnaires on the internet, the data were directly stored in the project’s database. Every nine STarT items were programmed with a limiter, prompting the patient to respond to all nine items before access to page two of the questionnaire was possible. The 23 RDMQ items were, however, not provided with a limiter. The use of limiters to avoid missing values was not possible in the paper version of the questionnaires, but text was inserted encouraging a reply to all questions. If patients did not respond to a questionnaire, reminders (emails or postal letters) were sent following one- and two-week delays [25]. The database was hosted by an external data manager at the North Denmark Region Department of Information Technology. The project database was provided with access login, written recording and daily backup copying.
Outcome measure
The predictor variable was the patient reported STarT risk group (low, medium, or high) at baseline. The primary outcome was assessed by a relative risk combining the low-risk group and the medium-risk group and comparing these to the high-risk group in terms of good outcomes. A good outcome was defined as receiving a minimal clinically relevant improvement in the RMDQ score (0–23 points) after 8 weeks [30]. The outcome was dichotomised using a standard cut-off at 30% improvement [21, 22, 26, 31]. As previous studies also included a secondary cut-off point between the low-risk group and the medium-risk group, this was applied as a secondary analysis. Furthermore, clinically relevant improvements after four and 52 weeks were included as secondary analyses.
Statistical analysis
For each STarT risk group, baseline characteristics were presented with numbers (%) for categorical variables and mean (sd) or median [iqr] for continuous variables. Baseline characteristics were patients’ age, gender, college education (y/n), employment (y/n), sick leave within 14 days (hours), RMDQ score (0–23 points) [30], numerical pain rating (0–10 points) [32], and self-reported health (EQ VAS, 0–100 points) [33]. Differences in baseline characteristics were tested by Fischer’s Exact test for categorical outcomes (gender, education level, and employment status), with the Student’s t-test (age, numerical pain rating, EQ VAS, and RMDQ), or by the Mann-Whitney test (sick leave) for continuous outcomes. For continuous outcomes, the tests were only comparing the low-risk group with the high-risk group.
For estimating the predictive ability of the STarT, a combination of the low-risk group and the medium-risk group was compared with the high-risk group and the low-risk group was compared with the medium-risk group + the high-risk group by relative risks. A regression analysis was performed to study whether the allocation group in the guideline implementation study was likely to have introduced bias into the estimates. The regression analysis includes baseline RMDQ score, allocation group in the cluster randomised controlled trial together with all the following baseline variables: age (continuous), gender (male/female), college level education (yes/no), employment status (employed, yes/no), sick leave (any LBP-related sick leave 14 days prior to baseline), numerical pain rating (continuous), and EQ VAS (continuous).
The study size was 441 patients by including all patients with a complete STarT from the guideline implementation trial [25]. Single responses from the 23-item RMDQ were coded 0 (no) if they were missing, allowing the inclusion of these observations in the analysis. Patients with a RMDQ score of 0 (optimal function) were excluded from the analysis as they could not achieve a 30% improvement. Throughout the analyses, a P value of <0.05 was considered statistically significant. Analyses were performed using Stata, IC version 14.0 (College Station, Texas, USA).
Results
Between January 2013 to July 2014, 1101 patients were included in the cluster randomised controlled trial. A subpopulation of 475 patients participated with questionnaires and was eligible to be included in this ancillary analysis. Among the 475 patients eligible for this analysis, 441 had a complete STarT questionnaire and formed our study population (Fig. 1). According to STarT, 124 (28%) scored low, 176 (40%) scored medium, and 141(32%) scored high (Table 1).

Flow chart. Note: 1101 patients were included in the cluster randomised trial, from which 475 participated with questionnaires. 441 patients had a complete STarT score and were included in this study.
Patients eligible for this study (n = 475) were older than patients not eligible (n = 626); mean of 45.2 years vs 41.7 years. However, in terms of age and referral to secondary care, there were no statistically significant differences between patients eligible for this study and the other patients included in the guideline implementation trial. From the eligible subpopulation of 475 patients, 304 (64.0%) patients provided complete information regarding STarT at baseline and completed the RMDQ questionnaire at baseline and after 8 weeks.
After 8 weeks, 61 (65.6%) in the low-risk group, 67 (54.9%) in the medium-risk group, and 33 (37.1%) in the high-risk group achieved a 30% improvement in RMDQ. High-risk patients were at a higher risk of not achieving a 30% improvement in RMDQ after 8 weeks compared with patients in the low- and medium-risk groups (RR 1.61 [1.20–2.15, p < 0.001]). For all comparisons, the higher STarT group(s) were at higher risk of not achieving a clinically relevant improvement in RMDQ compared with other patients (the low-risk group + the medium-risk group (Table 2).
A regression analysis to study the effect of patients’ allocation group in the guideline implementation trial showed no statistically significant or clinically relevant changes in estimates (Table 3). The only factors staying significantly predictive of functional improvement in the adjusted model were the STarT group and EQ VAS.
Discussion
In patients with LBP consulting Danish general practice, the STarT subgroups were predictive of the patients’ functional improvement measured by the RMDQ score. After 8 weeks, 61 (65.6%) in the low-risk group, 67 (54.9%) in the medium-risk group, and 33 (37.1%) in the high-risk group achieved a 30% improvement in the RMDQ score. High-risk patients were at a 61% higher risk of not achieving a 30% improvement in the RMDQ score after 8 weeks compared with the combined group of patients at medium risk and patients at low risk according to STarT.
In previous studies, follow-up has been applied after 12 weeks [21, 22]; therefore, the follow-up point after 8 weeks, being the closest to the main trial, was applied as the primary analysis in this study and this deviation from previous studies can be considered a limitation. However, the use of follow-up points after 4 weeks (short term), 8 weeks (medium term), and 52 weeks (long term) is considered a strength of this study. Furthermore, neither the choice of follow-up period nor the choice of cut-off used to dichotomize the STarT score significantly changed the conclusion. This similarly strengthens the interpretation of results. This is an ancillary analysis of data collected for a cluster randomised controlled trial, where general practices and their patients were randomised to different strategies to manage LBP. This may weaken the interpretation of results. In particular, the integration of the STarT in general practitioners’ medical record systems in the intervention group could have biased the results. Applying STarT to guide treatment has been found to be effective in improving patients’ RMDQ scores [15], and this improvement has been found to be particularly present among high-risk patients [15]. Thus, offering GPs the opportunity to use STarT might have led to an underestimation of the RRs in this study. However, including the allocation group in an adjusted model did not affect the results. Patients were given the questionnaire at the consultation at the day of inclusion. About 90% replied the same day; however, a few patients replied with a one- or two-day delay. This delay might have improved patients’ RMDQ score at baseline and might have caused an underestimation of the real improvement in the RMDQ score. In our study, this could lead to a small underestimation of the relative risks. It could have been of interest to adjust for the duration of LBP or even to exclude patients with pain lasting less than 14 days, as STarT has been found to be unable to predict outcome among these patients [23]. These data were, however, not available in the present study.
In a study from the US, patients were recruited directly from physiotherapy clinics, where the STarT could identify distinctive patterns between the low-risk group and the high-risk group but not when comparing the medium-risk group with the other two groups [17]. In line with the present study, the STarT’s ability to identify patients at risk of higher levels of disability by the Oswestry Disability Index has been supported in a study recruiting from a university community in Canada. They recruited participants by advertising in a local newspaper to screen for LBP in a chiropractic clinic [18]. In contrast to these findings, STarT has not been able to predict outcomes in two studies of patients seeking care at chiropractic clinics in Denmark using the RMDQ score as an outcome measure and the UK using the Patient Global Impression of Change as an outcome measure [18, 20]. A Danish study with a combined population from physiotherapy clinics and general practices found the STarT was able to predict improvements in the RMDQ score (RR 2.4 for low-risk vs. medium-risk and RR 2.8 for low-risk vs. high-risk) [21]. Lower predictive ability has been found in Danish secondary care (RR 1.5 for low-risk vs. medium-risk and RR 1.7 for low-risk vs. high-risk) [22]. The STarT was originally validated in a UK general practice setting [34] and in line with the original STarT trial, the present study consists exclusively of patients enrolled when consulting their general practitioner for LBP, which may increase generalizability to other general practice settings.
Compared with the present study, previous studies had very similar baseline characteristics in terms of pain rating [17,18,19,20,21,22,23]. In addition to the healthcare setting, pain duration seems important when comparing STarT subgroups. STarT has not been found suitable for patients with acute pain, especially not for patients with pain for less than 2 weeks [23, 24].
Findings from this study confirm the results from the original trial validating the STarT [34], thereby adding knowledge to support the ability of STarT to predict improvements in the RMDQ score in general practice settings. Even though STarT is found to be predictive of functional improvements in this study, this does, however, not support the effectiveness of the targeted treatment arms, which were applied in UK studies. Therefore, more research on the effect of stratifying treatment according to the STarT outside of the UK is needed.
Conclusion
The STarT subgroups were predictive of functional improvement in Danish general practice. This study supports wider implementation of the STarT.
Abbreviations
- EQ VAS:
-
EuroQol Visual Analogue Scale
- GP:
-
General Practitioner
- LBP:
-
Low Back Pain
- NICE:
-
The National Institute for Health and Care Excellence
- RMDQ:
-
Roland Morris Disability Questionnaire
- RR:
-
Relative Risk
- STarT:
-
STarT Back Tool
- UK:
-
United Kingdom
References
Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, Williams G, Smith E, Vos T, Barendregt J, Murray C, Burstein R, Buchbinder R. The global burden of low back pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(6):968–74.
Manchikanti L, Singh V, Falco FJ, Benyamin RM, Hirsch JA. Epidemiology of low back pain in adults. Neuromodulation. 2014;17(Suppl 2):3–10.
Schiottz-Christensen B, Nielsen GL, Hansen VK, Schodt T, Sorensen HT, Olesen F. Long-term prognosis of acute low back pain in patients seen in general practice: a 1-year prospective follow-up study. Fam Pract. 1999;16(3):223–32.
Hancock MJ, Maher CG, Laslett M, Hay E, Koes B. Discussion paper: what happened to the 'bio' in the bio-psycho-social model of low back pain? Eur Spine J. 2011;20(12):2105–10.
Nicholas MK, Linton SJ, Watson PJ, Main CJ. "decade of the flags" working group. Early identification and management of psychological risk factors ("yellow flags") in patients with low back pain: a reappraisal. Phys Ther. 2011;91(5):737–53.
Foster NE, Bishop A, Thomas E, Main C, Horne R, Weinman J, Hay E. Illness perceptions of low back pain patients in primary care: what are they, do they change and are they associated with outcome? Pain. 2008;136(1–2):177–87.
Cook CE, Taylor J, Wright A, Milosavljevic S, Goode A, Whitford M. Risk factors for first time incidence sciatica: a systematic review. Physiother Res Int. 2014;19(2):65–78.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–47.
Koes BW, van Tulder MW, Thomas S. Diagnosis and treatment of low back pain. BMJ. 2006;332(7555):1430–4.
Low back pain and sciatica in over 16s: assessment and management. NICE guideline [NG59]. 2016. https://www.nice.org.uk/guidance/ng59. Accessed 27 Dec 2016.
Hill JC, Vohora K, Dunn KM, Main CJ, Hay EM. Comparing the STarT back screening tool's subgroup allocation of individual patients with that of independent clinical experts. Clin J Pain. 2010;26(9):783–7.
Foster NE, Hill JC, Hay EM. Subgrouping patients with low back pain in primary care: are we getting any better at it? Man Ther. 2011;16(1):3–8.
Main CJ, Sowden G, Hill JC, Watson PJ, Hay EM. Integrating physical and phychological approaches to treatment in low back pain: the development and content of the STarT back trial's "high-risk" intervention (STarT back; ISRCTN 37113406). Physiotherapy. 2012;98(2):110–6.
Sowden G, Hill JC, Konstantinou K, Khanna M, Main CJ, Salmon P, Somerville S, Wathall S, Foster NE. IMPaCT back study team. Targeted treatment in primary care for low back pain: the treatment system and clinical training programmes used in the IMPaCT back study (ISRCTN 55174281). Fam Pract. 2012;29(1):50–62.
Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE, Konstantinou K, Main CJ, Mason E, Somerville S, Sowden G, Vohora K, Hay EM. Comparison of stratified primary care management for low back pain with current best practice (STarT back): a randomised controlled trial. Lancet. 2011;378(9802):1560–71.
Foster NE, Mullis R, Hill JC, Lewis M, Whitehurst DG, Doyle C, Konstantinou K, Main C, Somerville S, Sowden G, Wathall S, Young J, Hay EM. IMPaCT back study team. Effect of stratified care for low back pain in family practice (IMPaCT back): a prospective population-based sequential comparison. Ann Fam Med. 2014;12(2):102–11.
Beneciuk JM, Robinson ME, George SZ. Subgrouping for patients with low back pain: a multidimensional approach incorporating cluster analysis and the STarT back screening tool. J Pain. 2015;16(1):19–30.
Page I, Abboud J, O Shaughnessy J, Laurencelle L, Descarreaux M. Chronic low back pain clinical outcomes present higher associations with the STarT Back Screening Tool than with physiologic measures: a 12-month cohort study. BMC Musculoskelet Disord. 2015;16:201–015–0669-0.
Kongsted A, Andersen CH, Hansen MM, Hestbaek L. Prediction of outcome in patients with low back pain--a prospective cohort study comparing clinicians' predictions with those of the Start back tool. Man Ther. 2016;21:120–7.
Newell D, Field J, Pollard D. Using the STarT back tool: does timing of stratification matter? Man Ther. 2015;20(4):533–9.
Morso L, Kent P, Albert HB, Hill JC, Kongsted A, Manniche C. The predictive and external validity of the STarT back tool in Danish primary care. Eur Spine J. 2013;22(8):1859–67.
Morso L, Kent P, Manniche C, Albert HB. The predictive ability of the STarT back screening tool in a Danish secondary care setting. Eur Spine J. 2014;23(1):120–8.
Morso L, Kongsted A, Hestbaek L, Kent P. The prognostic ability of the STarT back tool was affected by episode duration. Eur Spine J. 2016;25(3):936–44.
Karran EL, McAuley JH, Traeger AC, Hillier SL, Grabherr L, Russek LN, Moseley GL. Can screening instruments accurately determine poor outcome risk in adults with recent onset low back pain? A systematic review and meta-analysis. BMC Med 2017;15(1):13-016-0774-4.
Riis A, Jensen CE, Bro F, Maindal HT, Petersen KD, Bendtsen MD, Jensen MB. A multifaceted implementation strategy versus passive implementation of low back pain guidelines in general practice: a cluster randomised controlled trial. Implement Sci. 2016;11(1):143.
Jordan K, Dunn KM, Lewis M, Croft P. A minimal clinically important difference was derived for the Roland-Morris disability questionnaire for low back pain. J Clin Epidemiol. 2006;59(1):45–52.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. STROBE initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–7.
Okkes IM, Becker HW, Bernstein RM, Lamberts H. The march 2002 update of the electronic version of ICPC-2. A step forward to the use of ICD-10 as a nomenclature and a terminology for ICPC-2. Fam Pract. 2002;19(5):543–6.
Riis A, Jensen CE, Bro F, Maindal HT, Petersen KD, Jensen MB. Enhanced implementation of low back pain guidelines in general practice: study protocol of a cluster randomised controlled trial. Implement Sci. 2013;8:124–5908–8-124.
Roland MO, Morris RW. A study of the natural history of back pain. Part 1: development of a reliable and sensitive measure of disability in low back pain. Spine. 1983;8(2):141–4.
Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, Von Korff M, Bouter LM, de Vet HC. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine (Phila Pa 1976). 2008;33(1):90–4.
Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–58.
Cortes J, Blanco JF, Pescador D, Asensio N, Castro C, Herrera JM. New model to explain the EQ-5D VAS in patients who have undergone spinal fusion. Qual Life Res. 2010;19(10):1541–50.
Hill JC, Dunn KM, Lewis M, Mullis R, Main CJ, Foster NE, Hay EM. A primary care back pain screening tool: identifying patient subgroups for initial treatment. Arthritis Rheum. 2008;59(5):632–41.
Acknowledgements
Not applicable.
Funding
This study was funded by TrygFonden, The Danish Rheumatism Association, The Danish Research Foundation for General Practice, The Obel Family Foundation, The Spar Nord Foundation, Medical Specialist Heinrich Kopps Grant, and the North Denmark Region.
Availability of data and materials
The dataset analysed during the current study is available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
AR, MSR, CEJ, and MBJ contributed in the design of this study. AR and CEJ were responsible for the original data collection. AR, MSR, and MBJ contributed to interpreting the data. AR, MSR, CEJ, and MBJ participated in writing the manuscript. AR, MSR, CEJ, and MBJ read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Danish Data Protection Agency (2016–41-4905). The study is based on questionnaire data and did not need approval from a Danish Health Ethics Committee. Participants were informed of the study by their GP and provided written (paper or online) informed consent.
Consent for publication
Not applicable.
Competing interests
MSR is a member of the Editorial board of BMC Musculoskeletal Disorders. The others authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Riis, A., Rathleff, M.S., Jensen, C.E. et al. Predictive ability of the start back tool: an ancillary analysis of a low back pain trial from Danish general practice. BMC Musculoskelet Disord 18, 360 (2017). https://doi.org/10.1186/s12891-017-1727-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-017-1727-6