
Abstract
Background
Commercially available flexible reamer and curved guide systems allow a certain degree of control over intra-articular tunnel orientation, therefore allows a wide range of intra-osseous femoral tunnel orientations, contrary to the femoral tunneling technique using a straight guide pin, which are determined by knee flexion angle. We sought to find the clinical relevance of intra-osseous femoral tunnel orientations in the respect of tunnel length. To evaluate the relationship between the tunnel axis angle in three orthogonal planes and tunnel length in the anteromedial (AM) and posterolateral (PL) femoral tunnels in patients who underwent anatomic double-bundle anterior cruciate ligament reconstruction (DB-ACLR) using the transportal (TP) technique with a 42o curved guide.
Methods
A total of 40 patients who underwent primary DB-ACLR with the TP technique using a curved guide were evaluated retrospectively. The tunnel axis angle in three orthogonal planes were evaluated on a three-dimensional surface model constructed using an axial computed tomography scan obtained after reconstruction. Then, correlations with tunnel length were analyzed.
Results
In the AM tunnel, tunnel axis angles in the coronal (β = 0.0252, p = 0.022) and sagittal (β = 0.0168, p = 0.029) plane showed significant correlations with tunnel length, while the axial plane did not (p = 0.493) (adjusted R2 = 0.801). In the PL tunnel, only tunnel axis angles in the axial plane (β = 0.0262, p = 0.008) showed a significant relationship with tunnel length (adjusted R2 = 0.700).
Conclusion
Drilling at a higher angle in the coronal and sagittal planes in AM tunnels and at a higher angle in the axial plane in PL tunnels decreases the incidence of short femoral tunnels.
Similar content being viewed by others

Background
Recently, anterior cruciate ligament (ACL) surgical techniques with a primary focus on anatomic reconstruction have been considered to restore normal knee anatomy, kinematics, and stability more thoroughly [1,2,3]. This is provided by placing tunnels in the center of native ACL insertion sites on the tibia and femur using either the single- or double-bundle technique [4]. To achieve anatomic ACL femoral tunnel positions more easily, transportal drilling has been proposed as an alternative to the transtibial technique [5,6,7,8]. However, more horizontal or oblique femoral tunnel positions result in a shorter distance between the notch and the lateral femoral cortex, which results in shorter overall tunnel length, iatrogenic damage to the medial femoral condyle cartilage [9], and a higher chance of posterior wall blowout from tunneling toward the posterior femoral condyle compared to the traditional transtibial technique [10,11,12].
Therefore, there are increasing interests to attain an adequate tunnel length and prevent posterior wall breakage [11,12,13]. Recently, commercially available flexible reamer and curved guide system was made to decrease the chance of injuring the medial femoral condyle cartilage. Furthermore, it has been suggested to achieve longer femoral intraosseous tunnel lengths than with a straight guide pin [14].
During femoral tunneling procedure using curved guide, we noticed changeable intra-articular tunnel orientations could be allowed by the certain degrees of guide’s movement within the intercondylar notch space. Meanwhile, in the femoral tunneling technique with a straight guide pin, the intra-articular tunnel orientation is mainly determined by the knee flexion angle because it involves the fixed intra-articular tunnel orientation from two points: the portal, and a femoral tunnel center within the anatomic femoral footprint (Figs. 1 and 2). Controllable intra-articular tunnel orientation can assure a wide range of tunnel axis angles in three-dimensional planes. We became interested in the interosseous tunnel orientation in three dimensional planes, the extension of the intra-articular tunnel orientation.

During femoral tunneling procedure using curved guide, the change of intra-articular tunnel orientations could be allowed by the certain degrees of guide’s movement within the intercondylar notch space. a First, curved guide is positioned for targeting the intended tunnel position. b Then, the guide can be rotated within the intercondylar notch space

The curved guide system allows a certain degree of control over intra-articular tunnel orientation regardless of the knee flexion angle due to the rotational freedom of the guide in the intercondylar notch space. This is contrary to tunneling with a straight guide pin, which has fixed intra-articular tunnel orientation from two points, the AM or AAM portal and the femoral tunnel center
The purpose of this study was to evaluate the relationship between tunnel axis angle in the three orthogonal planes and tunnel length using in vivo imaging data. The following research question was addressed: In which plane is the tunnel axis angle correlated to the tunnel length in both anteromedial (AM) and posterolateral (PL) femoral tunnels after anatomic double-bundle ACLR? Our hypothesis is that intra-osseous femoral tunnel orientations depending on the entrance angle of the guide pin influence tunnel length, which can be useful for the acquisition of longer tunnel length with use of commercially available flexible reamer and curved guide systems.
Methods
Demographic data
Between October 2013 to May 2014, 83 patients underwent primary anatomic double-bundle ACL reconstruction with the transportal (TP) technique using a curved guide and flexible reamer (Clancy Anatomic Cruciate Guide System; Smith & Nephew, Andover, MA, USA) (Table 1).
Inclusion criteria were a primary unilateral ACL injury with or without meniscus injury that was treated by double-bundle ACL reconstruction with the TP (accessory AM) technique, as well as patient age ranging from 15 to 60 years. Of the 83 patients, 43 were excluded because they (1) had undergone ACL reconstruction using a rigid guide because there was no flexible reamer size option for either AM or PL grafts less than 6 mm in diameter (n = 19), (2) had undergone ACL reconstruction using another technique (outside-in) (n = 15), (3) had any combined multiple-ligament injury (n = 2), or (4) they had undergone a single bundle reconstruction for open physis (n = 2) and simultaneous reconstruction of the ACL and PCL (n = 4) combined with HTO (n = 1). Finally, 40 patients who underwent anatomic double-bundle ACL reconstruction by the TP technique were retrospectively evaluated in the present study. Institutional Review Board approval (2015-05-085) was obtained from our institution (Samsung Medical Center, Seoul, South Korea) before the study, and the protocol was approved. All patients provided informed consent prior to participation in this study.
Surgical technique
A single surgeon (J.H.W.) experienced in ACL reconstruction performed all operations using the TP arthroscopic-assisted technique. Femoral and tibial tunnels were created in the centers of their respective anatomic insertions. Grafts were fixed with a cortical suspension system using the shortest possible loop (10 to 15 mm) to ensure maximal contact between the grafts and tunnel walls on the femoral side. Bio-absorbable interference screws with a post tie were used on the tibial side for all cases.
Portal formation was conducted in the usual manner. An anteromedial (AM) portal was placed in a slightly more proximal position than usual, with the distal extent of the portal ending at the level of the inferior pole of the patella. An accessory anteromedial (AAM) portal was made approximately 1.5 cm medial from the standard AM portal and just above the medial meniscus anterior horn. The arthroscope was inserted into the AM portal, and another working device was inserted into the AAM portal. After the ACL rupture was confirmed and remnant tissue was debrided, the femoral footprints of both the AM and PL bundles were carefully defined in reference to the ACL remnants and bony ridges [13]. Centers of both footprints were then indicated with a curved microfracture awl. The center of the AM bundle footprint was 6–7 mm distal (shallow) to the posterior cartilage margin, 2 mm from the posterior bony ridge of the lateral femoral condyle [15, 16], and 3–4 mm posterior (low) to the extended line of the posterolateral corner of the intercondylar notch, which was verified at 90° of knee flexion. The center of the PL bundle footprint was positioned 5 mm anterior (high) to the edge of the joint cartilage on an imaginary line perpendicular to the tangent of the lowermost portion of the lateral femoral condyle at 90° of knee flexion [17]. Our considerations in placement of femoral tunnel were 1) to prevent slippage on the medial wall of the lateral femoral condyle while placing guide wires within the anatomical footprint of the ACL 2) to secure appropriate tunnel length of 20 mm or more 3) to prevent of posterior cortical breakage. After creating the femoral tunnel, its length was measured with a ruler. The required EndoButton size (Smith & Nephew Endoscopy, Andover, MA) for the TP technique was then determined. A femoral guide was inserted through the AAM portal, and a 2.4-mm guide pin was advanced 2 to 3 mm to engage the guide to the center of the AM and PL bundle femoral footprints. The knee joint was then bent as fully as possible and the guide was advanced until the pin passed the cortex and skin. After changing the viewing portal from AM to anterolateral, the tibial footprints of both the AM and PL bundles were carefully defined in reference to the ACL remnants and bony ridges. The anterior margin of the ACL footprint was described as the ACL ridge, and the posterior margin was defined as the retro-eminence of the tibial spine [18, 19].
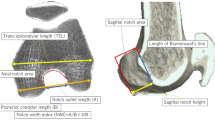
Measurement of tunnel axis angle using three-dimensional computed tomography
Computed tomography (CT) scans were performed on all knees after ACL reconstruction. The knee was placed in full extension. Digital Imaging and Communications in Medicine data were extracted from the picture archiving and communication system. Data were segmented by Mimics software (Materialise, Leuven, Belgium), a commercially available image processing software used to create three-dimensional (3D) surface models from stacks of two-dimensional image data. The data were then imported into Geomagic Studio software, version 12.0 (Geomagic, Rock Hill, SC, USA), and the 3D surface model was projected into coronal, axial, and sagittal planes to measure the tunnel axis angle in each plane (Fig. 3). As described by Basdekis et al. [20], the angle between the tunnel and the line tangent to the distal and posterior aspects of the femoral condyles was measured in the coronal and axial planes. The sagittal plane angle between the tunnel and the extended intersectional line of the femoral shaft was measured. A lower tunnel angle in the sagittal plane indicated that the tunnel orientation is extended compared with the femoral shaft, while a higher tunnel angle in the sagittal plane indicated that tunnel orientation is flexed compared with the femoral shaft.

Angle in each plane projected from a three-dimensional surface model. a The angle between the tunnel and a line tangent to distal aspects in the coronal plane was measured. b The angle between the tunnel and a line tangent to the posterior aspects of the femoral condyles was measured in the axial plane. c The angle between the tunnel and the extended intersectional line of the femoral shaft in the sagittal plane was measured
To measure the femoral tunnel length, the plane in which the entire length of the femoral tunnel showed the maximal width was selected. The distance between the centers of the intra-articular and extra-articular tunnel apertures was measured [21]. To evaluate its correlation with distal femoral anatomy, the lateral posterior condyle (LPC) AP size (LPC offset distance) and medial-to lateral (M-L) epicondylar distance were measured [21]. The incidence of posterior cortical damage was evaluated by 3D CT scan. Cases with posterior cortical damage or in which the tunnel center was not placed within the anatomical footprint boundary would have been excluded, but none occurred in this study.
Reliability and statistical analysis
Two orthopedic surgeons (independent observers) together developed and agreed to the measurement methods. They were blinded to each other’s measurements and their own prior measurements. They measured the tunnel axis angle in sagittal, coronal, and axial planes, and tunnel length for AM and PL bundles of all knees. The intra-class correlation coefficient was used to assess the interobserver reliability of measurements.
Uni- and multivariate regression analyses evaluated the relationship between independent influential factors and tunnel length using the SigmaStat software package. Influential factors were considered demographic factors (sex, age, and body mass index), LPC offset distance, and M-L epicondylar distance. Significance was set at P < 0.05. All statistical analyses were performed using SAS ver. 9.3 (SAS Institute, Cary, NC, USA).
Results
The interobserver and intraobserver reliability ranged from 0.83 to 0.96 and 0.85 to 0.95, respectively (Table 2). The mean AM tunnel length was 33.5 ± 4.3 mm (range, 21.6 to 42.9), and the mean PL tunnel length was 35.4 ± 4.0 mm (range, 24 to 41.0).
Influence of tunnel Axis angle change in 3-D planes on tunnel length in AM and PL femoral tunnels
Tables 3 and 4 show data regarding measured variables.
In the AM femoral tunnel, the mean tunnel axis angle was 44.5o ± 5.7o in the coronal plane, 40.9o ± 6.4o in the sagittal plane, and 32.9o ± 7.2o in the axial plane. Univariate regression analyses identified that the patient factors related to longer femoral tunnel length include male gender (β = 0.5212, p = 0.001), age (β = 0.0145, p = 0.023), height (β = 0.0375, p < 0.001), weight (β = 0.0119, p = 0.008), femoral condyle size (M-L epicondylar distance) (β = 0.4473, p < 0.001), and greater femoral tunnel axis angle in the coronal (β = 0.0465, p < 0.001) and axial (β = 0.0285, p = 0.003) planes.
In the PL femoral tunnels, the mean tunnel axis angle was 30.5o ± 6.3o in the coronal plane, 51.7o ± 16.4o in the sagittal plane, and 25.1o ± 6.1o in the axial plane. Univariate regression analyses identified that the patient factors related to longer femoral tunnel length include male gender (β = 0.6471, p < 0.001), height (β = 0.0399, p < 0.001), weight (β = 0.0136, p = 0.001), femoral condyle size (M-L epicondylar distance) (β = 0.4751, p < 0.001), and greater femoral tunnel axis angle in all three planes: coronal (β = 0.0326, p = 0.001) sagittal (β = −0.0087, p = 0.038), and axial (β = 0.0224, p = 0.038).
Multivariate regression analysis (Table 4) identified a disparate result between the AM and PL tunnels. In the AM tunnel, coronal (β = 0.0252, p = 0.022) and sagittal (β = 0.0168, p = 0.029) angles showed a significant correlation with AM femoral tunnel length, while this was not identified in the axial plane (p = 0.493) (adjusted R2 = 0.801). In the PL tunnel, only the axial angle (β = 0.0262, p = 0.008) showed a significant relationship with PL femoral tunnel length (adjusted R2 = 0.700).
Discussion
The principal findings of our study are that tunnel length is correlated with tunnel axis angle in the three-dimensional planes, but differently in AM and PL tunnels. In AM tunnels, tunnel length was related to tunnel axis angle in the coronal and sagittal planes (p = 0.022, 0.029 respectively), whereas PL tunnel lengths were related only to the tunnel axis angle in the axial plane (p = 0.008).
Several authors have recommended appropriate tunnel lengths. The ideal or minimal tunnel length remains unclear, but most surgeons anecdotally prefer to have 20 mm or more of graft to allow strong tendon healing to the bone within the tunnel. The lack of graft incorporation is a common cause of surgical failure [14]. Greis et al. reported that the length of a tendon placed within a bone tunnel influences tendon pullout strength, and advocated maximizing the tendon length inside the bone tunnels [22]. Previous cadaveric and clinical studies reported that the mean femoral tunnel length drilled through AM portals ranges from 15.7 − 34.2 mm [23, 24]. Moreover, extra length is required to flip and subsequently seat a suspensory fixation button device on the outside of the femoral cortex.
To attain adequate tunnel length with the AM portal technique and prevent posterior wall breakage, many researchers have investigated femoral tunnel orientation and intraosseous length changes with knee flexion angle. Basdekis et al. [20] and Bedi et al. [25] noted that increasing knee flexion increases the tunnel length and decreases the risk of posterior cortical breakage. Iyyampillai et al. suggested that femoral tunnel drilling with maximal knee hyperflexion in ACL reconstruction consistently produced tunnel lengths greater than 30 mm with no posterior wall fractures [26]. However, others have suggested that increased sagittal inclination or reduced guide wire axial angles have little effect on tunnel length [20, 25, 27]. Some have refuted the correlation of knee flexion angle with tunnel length because maximum flexion varies from one subject to another. In addition, tunnel lengths might be affected by patient height, weight, leg size, operative positioning, and larger lateral femoral condyle dimensions [14, 26].
However, previous studies have been based on fixed intra-articular tunnel orientation by drilling with a straight guide pin. We thought it was necessary to investigate tunnel configurations made using curved guides with a three-dimensional approach because it allows a certain degree of control over intra-articular tunnel orientation. Few previous studies have investigated the ideal tunnel axis angle for longer tunnel lengths [22, 28]. These studies were limited because they were experimental studies using a bone saw or cadaver, and the results are difficult to reproduce in a practical surgical situation. To our knowledge, no in vivo studies have been conducted with respect to the potential correlation between femoral tunnel length and guide pin entrance angle after anatomic ACLR with the TP technique.
Regression analyses confirmed our hypothesis that tunnel length is influenced by changes in the tunnel axis angle, and the AM and PL tunnels were significantly correlated with changes in the tunnel axis angle for each different plane.
For AM tunnels, multivariate regression showed that tunnel length had significant correlations with tunnel orientation in the sagittal and coronal planes (p = 0.022, p = 0.029, respectively) with high reliability (adjusted R2 = 0.801), while there was no significant correlation in the axial plane (p = 0.493). We interpreted this result as 1) longer tunnel lengths can be achieved when the sagittal tunnel angle is increased because outer orifice of the tunnel on the globular-shaped lateral condyle would be made further from the tunnel placement position, 2) the increased coronal tunnel angle provides tunnels with longer hypotenuses, and 3) there was no significant correlation in axial tunnel angle with tunnel length because the inner orifice of the AM tunnels is located in the posterior side of the anatomic ACL footprint, making it technically difficult to create a tunnel outlet oriented near the lateral epicondyle or the apex of lateral femoral condyle, due to abrupt tunnel bending angles. Contrary to the AM tunnels, for the PL tunnels, only the axial tunnel angle showed a significant correlation to tunnel length (p = 0.008, adjusted R2 = 0.700). We explained this result as 1) the PL tunnel can made easily in the outer orifice near the apex of the lateral femoral condyle, lateral epicondyle, and nearer to the lateral epicondyle, which would increase the axial tunnel angle and lengthen the tunnel, and 2) significant correlations with the tunnel axis angle in the sagittal and coronal planes were not identified due to restricted changes in the tunnel axis angle in the sagittal and coronal planes by its more intra-articular horizontal tunnel orientation even though the curved guide was used.
Recently, the CLANCY 42° curved guide (Clancy Anatomic Cruciate Guide System; Smith & Nephew, Andover, MA) has been utilized with the TP technique to access native femoral ACL insertion. This method achieves longer tunnel lengths with straight, rigid instrumentation that does not require hyperflexion, but is associated with the loss of visualization, fat pad ingress, poor arthroscopic inflow, inability to seat instrumentation, and the bending of rigid guide wires [14]. Andrew et al. noticed that commercially available flexible reamers and curved guides result in longer femoral interosseous tunnel lengths than those achieved with a straight guide pin [14, 29]. Furthermore, the rotational freedom of the intra-articular portion of a curved guide can assure a wide variability of tunnel angle orientation (Fig. 1) (video clip is available as a Additional file 1: Movie S1).
Additional file 1: Movie S1. Intentional rotary movement of intra-articular portion of a curved guide. The rotational freedom of the intra-articular portion of a curved guide can assure a wide variability of tunnel angle orientation. (MOV 101932 kb)
Our results provide a technical consideration for the acquisition of longer tunnel lengths, combined with the use of commercially available flexible reamer and curved guide systems. This study also indicates that three-dimensional tunnel orientations should be stressed for appropriate femoral tunnel length in anatomic ACL reconstruction.
This study has several limitations. At first, there may be a certain degree of variability in the AM and PL femoral tunnel center locations. However, every efforts were put to standardize the starting position of femoral tunnels according to anatomic landmarks of the lateral femur and the knee flexion angle, described in previous literature from our team [15, 24]. And the individual data in the present study has been controlled for patient factors and anatomic variables that may affect tunnel length, and this study was performed using 3D virtual models constructed by applying reverse engineering software with high reliability and accuracy. Several authors have stressed the limitations of two-dimensional radiographic assessment [30, 31]. Khalfayan et al. [32] included inadequate radiographic data as one of the exclusion criteria in their study. Sommer et al. [33] were concerned with tunnel invisibility on the tunnel view and inaccurate projection on the lateral view. Seconds, we are not able to be sure that all femoral tunnels in this study provide the best configuration of tunnels. However, our considerations at femoral tunneling should be common agreements to other surgeons for anatomic ACL reconstruction.
Conclusion
Drilling at a higher angle in the coronal and sagittal planes in AM tunnels and at a higher angle in the axial plane in PL tunnels decreases the incidence of short femoral tunnels.
Abbreviations
- AAM:
-
Accessory anteromedial
- ACLR:
-
Anterior cruciate ligament reconstruction
- AM:
-
Anteromedial
- CT:
-
Computed tomography
- HTO:
-
High tibial osteotomy
- LPC offset distance:
-
Lateral posterior condyle (LPC) AP size
- M-L:
-
From medial to lateral
- PL:
-
Posterolateral
- TP:
-
Transportal
References
Bedi A, Maak T, Musahl V, Citak M, O'Loughlin PF, Choi D, et al. Effect of tibial tunnel position on stability of the knee after anterior cruciate ligament reconstruction: is the tibial tunnel position most important? Am J Sports Med. 2011;39:366–73.
Debandi A, Maeyama A, Hoshino Y, Asai S, Goto B, Smolinski P, et al. The effect of tunnel placement on rotational stability after ACL reconstruction: evaluation with use of triaxial accelerometry in a porcine model. Knee Surg Sports Traumatol Arthrosc. 2013;21:589–95.
Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008;36:678–85.
Yasuda K, van Eck CF, Hoshino Y, Fu FH, Tashman S. Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 1: basic science. Am J Sports Med. 2011;39:1789–99.
Bernard M, Hertel P, Lais E, Gomez F. Reconstruction of the proximal insertion of the anterior cruciate ligament. Studies on the accuracy of a non-instrumental method. Unfallchirurg. 1990;93:565–9.
Giron F, Buzzi R, Aglietti P. Femoral tunnel position in anterior cruciate ligament reconstruction using three techniques. A cadaver study. Arthroscopy. 1999;15:750–6.
Arnold MP, Kooloos J, van Kampen A. Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001;9:194–9.
Pastrone A, Ferro A, Bruzzone M, Bonasia DE, Pellegrino P, D'Elicio D, et al. Anterior cruciate ligament reconstruction creating the femoral tunnel through the anteromedial portal. Surgical technique. Curr Rev Musculoskelet Med. 2011;4:52–6.
Lubowitz JH. Anteromedial portal technique for the anterior cruciate ligament femoral socket: pitfalls and solutions. Arthroscopy. 2009;25:95–101.
Rupp S, Muller B, Seil R. Knee laxity after ACL reconstruction with a BPTB graft. Knee Surg Sports Traumatol Arthrosc. 2001;9:72–6.
Scopp JM, Jasper LE, Belkoff SM, Moorman CT 3rd. The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy. 2004;20:294–9.
Howell SM, Gittins ME, Gottlieb JE, Traina SM, Zoellner TM. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001;29:567–74.
Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy. 2007;23:1218–25.
Silver AG, Kaar SG, Grisell MK, Reagan JM, Farrow LD. Comparison between rigid and flexible systems for drilling the femoral tunnel through an anteromedial portal in anterior cruciate ligament reconstruction. Arthroscopy. 2010;26:790–5.
Kim JG, Wang JH, Lim HC, Ahn JH. Femoral graft bending angle and femoral tunnel geometry of transportal and outside-in techniques in anterior cruciate ligament reconstruction: an in vivo 3-dimensional computed tomography analysis. Arthroscopy. 2012;28:1682–94.
Fu FH, Jordan SS. The lateral intercondylar ridge--a key to anatomic anterior cruciate ligament reconstruction. J Bone Joint Surg Am. 2007;89:2103–4.
Yasuda K, Kondo E, Ichiyama H, Kitamura N, Tanabe Y, Tohyama H, et al. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy. 2004;20:1015–25.
Purnell ML, Larson AI, Clancy W. Anterior cruciate ligament insertions on the tibia and femur and their relationships to critical bony landmarks using high-resolution volume-rendering computed tomography. Am J Sports Med. 2008;36:2083–90.
Ziegler CG, Pietrini SD, Westerhaus BD, Anderson CJ, Wijdicks CA, Johansen S, et al. Arthroscopically pertinent landmarks for tunnel positioning in single-bundle and double-bundle anterior cruciate ligament reconstructions. Am J Sports Med. 2011;39:743–52.
Basdekis G, Abisafi C, Christel P. Influence of knee flexion angle on femoral tunnel characteristics when drilled through the anteromedial portal during anterior cruciate ligament reconstruction. Arthroscopy. 2008;24:459–64.
Wang JH, Kim JG, Ahn JH, Lim HC, Hoshino Y, Fu FH. Is femoral tunnel length correlated with the intercondylar notch and femoral condyle geometry after double-bundle anterior cruciate ligament reconstruction using the transportal technique? An in vivo computed tomography analysis. Arthroscopy. 2012;28:1094–103.
Iyyampillai G, Raman ET, Rajan DV, Krishnamoorthy A, Sahanand S. Determinants of femoral tunnel length in anterior Cruciate ligament reconstruction: CT analysis of the influence of tunnel orientation on the length. Knee Surg Relat Res. 2013;25:207–14.
Chang CB, Choi JY, Koh IJ, Lee KJ, Lee KH, Kim TK. Comparisons of femoral tunnel position and length in anterior cruciate ligament reconstruction: modified transtibial versus anteromedial portal techniques. Arthroscopy. 2011;27:1389–94.
Lubowitz JH, Konicek J. Anterior cruciate ligament femoral tunnel length: cadaveric analysis comparing anteromedial portal versus outside-in technique. Arthroscopy. 2010;26:1357–62.
Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ 3rd. Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: a cadaveric study of femoral tunnel length and obliquity. Arthroscopy. 2010;26:342–50.
Tompkins M, Milewski MD, Carson EW, Brockmeier SF, Hamann JC, Hart JM, et al. Femoral tunnel length in primary anterior cruciate ligament reconstruction using an accessory medial portal. Arthroscopy. 2013;29:238–43.
Hamilton SC, Jackson ER 2nd, Karas SG. Anterior cruciate ligament femoral tunnel drilling through anteromedial portal: axial plane drill angle affects tunnel length. Arthroscopy. 2011;27:522–5.
Lubowitz JH, Akhavan S, Waterman BR, Aalami-Harandi A, Konicek J. Technique for creating the anterior cruciate ligament femoral socket: optimizing femoral footprint anatomic restoration using outside-in drilling. Arthroscopy. 2013;29:522–8.
Park SH, Moon SW, Lee BH, Chae SH, Ahn JH, Chang M, et al. The sagittal plane angle and tunnel-related complications in double-bundle anterior cruciate ligament reconstruction using the transportal technique: an in vivo imaging study. Arthroscopy. 2015;31:283–92.
Golish SR, Baumfeld JA, Schoderbek RJ, Miller MD. The effect of femoral tunnel starting position on tunnel length in anterior cruciate ligament reconstruction: a cadaveric study. Arthroscopy. 2007;23:1187–92.
Hoser C, Tecklenburg K, Kuenzel KH, Fink C. Postoperative evaluation of femoral tunnel position in ACL reconstruction: plain radiography versus computed tomography. Knee Surg Sports Traumatol Arthrosc. 2005;13:256–62.
Khalfayan EE, Sharkey PF, Alexander AH, Bruckner JD, Bynum EB. The relationship between tunnel placement and clinical results after anterior cruciate ligament reconstruction. Am J Sports Med. 1996;24:335–41.
Sommer C, Friederich NF, Muller W. Improperly placed anterior cruciate ligament grafts: correlation between radiological parameters and clinical results. Knee Surg Sports Traumatol Arthrosc. 2000;8:207–13.
Acknowledgements
The authors thank all members of the Sports Medicine Center, Samsung Medical Center for their great scientific debates.
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI15C2424) and by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIP) (NO.2012R1A1A2044586). The funding sources were not involved in the study design, collection, analysis or interpretation of the data, writing of the manuscript, or in the decision to submit the manuscript for publication.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Authors’ contributions
JHW and BHL participated in the study design and helped to draft the manuscript. DKL as a consultant for statistical analysis performed the statistical analysis. STC conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
.Consent for publication
The authors have received written consent from all patients to publish this study
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The current study obtained Institutional Review Board approval from our institution (SMC IRB 2015-05-085) before study onset, and our protocol was also approved. Informed consent was obtained from all participants.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, J.H., Lee, D.K., Chung, S.T. et al. Influence of change of tunnel axis angle on tunnel length during double-bundle ACL reconstruction via the transportal technique. BMC Musculoskelet Disord 18, 237 (2017). https://doi.org/10.1186/s12891-017-1599-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-017-1599-9