
Abstract
Background
Fixation failure is a relatively common sequela of surgical management of proximal humerus fractures (PHF). The purpose of this study is to understand the current state of the literature with regard to the biomechanical testing of proximal humerus fracture implants.
Methods
A scoping review of the proximal humerus fracture literature was performed, and studies testing the mechanical properties of a PHF treatment were included in this review. Descriptive statistics were used to summarize the characteristics and methods of the included studies.
Results
1,051 proximal humerus fracture studies were reviewed; 67 studies met our inclusion criteria. The most common specimen used was cadaver bone (87 %), followed by sawbones (7 %) and animal bones (4 %). A two-part fracture pattern was tested most frequently (68 %), followed by three-part (23 %), and four-part (8 %). Implants tested included locking plates (52 %), intramedullary devices (25 %), and non-locking plates (25 %). Hemi-arthroplasty was tested in 5 studies (7 %), with no studies using reverse total shoulder arthroplasty (RTSA) implants. Torque was the most common mode of force applied (51 %), followed by axial loading (45 %), and cantilever bending (34 %). Substantial testing diversity was observed across all studies.
Conclusions
The biomechanical literature was found to be both diverse and heterogeneous. More complex fracture patterns and RTSA implants have not been adequately tested. These gaps in the current literature will need to be addressed to ensure that future biomechanical research is clinically relevant and capable of improving the outcomes of challenging proximal humerus fracture patterns.
Similar content being viewed by others


Background
Proximal humerus fractures (PHF) are a challenging injury in need of more reliable surgical techniques and improved health-related outcomes. Intra-articular screw penetration, loss of reduction, and fracture healing complications frequently occur and have limited the success of surgical management [1]. Furthermore, the outcomes associated with three- and four-part fracture patterns are often both unpredictable and worse than anticipated [1–8]. The complications and long recovery times for PHFs have a significant impact on patient quality of life [4, 5, 9] and the health care system [10].
Biomechanical modeling provides controlled testing data to support new surgical implants and novel treatment strategies. Biomechanical research is an important method of evaluating orthopaedic implants as it removes patient factors and focuses on the performance of the implant under strict testing conditions. There has been an increasing focus on biomechanical modeling to test the properties and limits of various techniques and implants used to treat proximal humerus fractures. Since there are numerous surgical implants and PHF patterns that could be tested, the biomechanical literature is potentially a broad landscape of diverse research that has not been previously summarized.
The purpose of the current study was to: 1) use scoping review techniques [11, 12] to systematically evaluate and map the breadth of proximal humerus fracture biomechanical testing literature; 2) to summarize the model designs and testing procedures most commonly employed; and, 3) to identify biomechanical areas that are not well represented in the existing literature.
Methods
Literature search
As part of our larger proximal humerus fracture scoping review (Slobogean et al., [13]), we completed a comprehensive literature search to identify studies on the management of proximal humerus fractures. In consultation with a biomedical librarian, we developed a sensitive search strategy to identify all types of publications involving proximal humerus fractures. Using a combination of keywords and medical subject heading (MeSH) terms related to proximal humerus fractures, we searched the following electronic databases: Medline, Excerpta Medica Database (EMBASE), Cumulative Index of Nursing and Allied Health Literature (CINAHL), Cochrane Database of Systematic Reviews (CDSR), Proquest, Web of Science, Society of Automotive Engineers (SAE) digital library, and Transportation Research Board’s Transport Research International Documentation (TRID) database. All searches were performed in October 2012, and no language or date restrictions were employed.
Study selection
All identified titles were then compiled into a literature review program (DistillerSR), and an independent review process was performed. All studies were reviewed in duplicate by two orthopaedic surgeons, and studies involving biomechanics were identified. We excluded review articles, computer modeling, finite element analysis studies, and studies that were not published in English.
Data abstraction
Two authors (DC and TS) independently abstracted data from each included study focusing on the characteristics of the analysis and the methods utilized to better understand the layout of the literature. Any disagreements on the data abstracted were resolved by consensus in consultation with a third author (GPS). Study characteristics abstracted included publication year, geographic location, sample size, and type of specimen. Methods data abstraction examined pretesting analysis, implant selection, and testing conditions.
Statistical analysis
Descriptive statistics were used to summarize all data. For continuous data, the mean and standard deviation or median and ranges were reported based on the data’s distribution. Counts and proportions were used to describe all other data. No inferential statistical testing was performed.
Results
Literature review
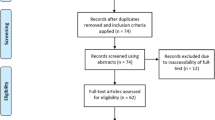
The initial literature search of the PHF literature, which included clinical and basic science studies, resulted in identification of 5,406 titles. 2,540 were found to be duplicates, seven were book titles, and two were retracted studies; these were all excluded. An additional 1,459 titles were removed because they did not meet the eligibility criteria. After review, 1,051 proximal humerus fracture studies were included in our database. From our eligible PHF database, 94 were identified as basic science or biomechanical papers. For the purpose of this study, we excluded an additional 16 non-English language publications, seven basic science articles, three finite element analysis studies, and one review article (Fig. 1). Therefore, 67 proximal humerus biomechanical published studies were included in the current analysis (Additional file 1).

Search and screening flow chart
Study characteristics
The majority of the included publications originated from Europe (48 %) to North America (39 %), comprising 87 % of the total studies. Few biomechanical studies have been published from Asia (4 %), South/Central America (3 %), to the Middle East (3 %) (Fig. 2). The earliest included study identified dates back to 1988 with nothing published again until 1993. Since that time, however, there has been an exponential increase in biomechanical publications, with 13 studies published in 2012 alone (Fig. 3).

Location of research

Frequency of studies published per year
Specimen characteristics
The sample size was reported in every study and the average sample size was found to be 27 ± 28.9 specimens with a range of 5 to 150 specimens (Table 1). The most commonly tested specimen was cadaver bones (87 %) followed by saw bones (7 %), animal bones (4 %), and wood (1 %). Of the cadaver studies, the obtained cadavers were frozen in 45 studies (75 %), embalmed in 12 (20 %), and fresh in 3 (5 %). Of the 58 studies that used cadaver specimens, only 33 (57 %) included information on the age of the cadavers used. In the studies that reported age of the cadaver, the average age was found to be 73.3 ± 8.5 years, with a range of 32 to 101 years of age. Only 45 studies (67 %) undertook some form of pre-testing investigations including plain radiographs (32 studies), bone mineral density testing (31 studies), and CT scans (12 studies) (Table 2).
Sixty studies tested proximal humerus fracture implants in a specific simulated fracture pattern. The most common fracture simulated was a two-part proximal humerus fracture in 41 studies (68 %), followed by a three-part fracture in 14 studies (23 %), and a four-part fracture in five studies (8 %) (Table 1). Of the two-part fracture simulations, 37 involved the surgical neck, three involved the anatomic neck, and one study described making a two-part fracture model, but the location of the osteotomy was not stated. None of the included studies examined fractures of the greater tuberosity.
The most common method of specimen preparation was to create the fracture using a saw, followed by reduction and fixation with the specified construct. Often, in order to simulate medial comminution, a section of bone would be removed and a gap created. This modification of the specimen ensured that reduction and alignment was maintained solely by the implant in the absence of a medial cortical support. This was performed in 35 studies. When compared to fracture type, medial comminution was simulated in 27 (66 %) of the two-part fracture studies, in seven (50 %) of the three-part fracture studies and in none of the four-part fracture studies. One study specified that a gap osteotomy was performed but did not specify the location or the fracture pattern.
Implants evaluated
The most frequently tested implant was a fixed angle locking plate, which was tested in 35 studies (Fig. 4). Intramedullary devices, including intramedullary nails, were tested in 17 studies, followed by non-locking plates in 13 studies, and blade plates in eight studies. Interestingly, arthroplasty implants were only tested in five studies and only included hemi-arthroplasty implants. We did not identify any studies that focused on biomechanical testing of total shoulder implants or reverse total shoulder implants for the treatment of proximal humerus fractures. An overview of the implants evaluated in each study is found in Additional file 2.

Frequency of implant testing
Construct testing
The apparatus and testing procedure of the constructs was found to be highly heterogeneous between studies and many different testing platforms, configurations, and devices were described in the included studies. Despite this heterogeneity, the majority of the studies tested their constructs under similar biomechanical themes, which has allowed us to summarize them. Specifically, the most commonly tested force was torque (34 studies), followed by axial load (30 studies), and cantilever bending, usually in varus or valgus (23 studies) (Table 2).
The testing parameters including the magnitude of the force (20 studies), how the force was applied (64 studies), and the loading mode (54 studies); all testing parameters varied significantly between studies (Table 2). Cyclic loading was utilized in 33 studies, load to failure was used in 28 studies, and compounding cyclic load to failure was used in six studies. In the studies that used cyclic loading to test the construct, the number of cycles varied from 5 to 1,000,000; the most commonly used number of cycles was 1000 (seven studies). Many studies (34 studies) used a combination of testing modes, for example a construct would be put through cyclic loading to a set number of cycles and then undergo a load to failure test.
Supplementary fixation methods were infrequently evaluated in the biomechanics literature. Sutures were used to augment fixation in three studies; two of the studies tested hemi-arthroplasty implants and one study tested locking plates. Tension band wiring, either on its own or as an augment to a construct, was used in four studies. Bone grafting with structural grafts was tested in three studies and two studies examined the use of cement as an augment.
Discussion
The literature describing the biomechanical testing of proximal humerus fracture implants is broad and heterogeneous. It is evident that biomechanical testing is being performed more frequently to compare proximal humerus fracture treatments; however, significant limitations to the clinical utility of the current testing models exist. These include a lack of models for three- and four-part fractures and a high variability in the testing parameters utilized.
The most common model identified was the simulated two-part fracture. From a practical perspective, this is not surprising since the fracture (osteotomy) occurs in the surgical neck region and does not require the investigator to recreate fractured tuberosity fragments or impaction of the humeral head. Two-part fractures are also appealing to model because fixation is easily achieved in the humeral head and shaft, and mechanical testing can focus on axial, bending, and torsional loads across a single fracture line. Despite the study design advantages of focusing on two-part fractures, it is our opinion that three- and four-part fractures represent the true surgical challenge and should be the focus of most biomechanical testing [7, 8]. Fourteen studies simulated a three-part fracture, and only five studies used a four-part model.
Another key finding of our scoping review was the substantial heterogeneity in testing parameters. We found almost no duplication of testing configurations and minimal standardization, which would allow comparison between studies. Consequently, we classified the studies based on biomechanical testing themes such as direction of force and testing mode. In most studies, the direction of force could be placed into one of three categories: torque, axial load, or cantilever bending (varus or valgus). In addition to variations in the direction of force applied, a wide range of force magnitude and cycles were observed. For example, 33 studies used cyclic loading to test their constructs; however, the number of loading cycles used in each study ranged from 5 to 1,000,000 cycles. Furthermore, in many of these studies the magnitude of the force applied was not reported, or there was a wide variety in combinations of forces.
Similar heterogeneity was also observed in the reporting of cadaveric specimens used. Authors commonly did not report the age of the specimens or the pre-testing analysis conducted to ensure the validity of results. Only 57 % of studies reported the age of the specimens and 67 % reported their pre-testing analysis. Specifically, fewer than half of the studies reported the bone mineral density of their specimens, which is essential for ensuring testing specimens are comparable and the results can be interpreted within the context of other published studies.
The final gap identified in our scoping review was the lack of biomechanical testing of arthroplasty implants in proximal humerus fracture models. Although there are likely many studies that test the mechanical properties of shoulder arthroplasty implants in an intact humerus, only five studies were identified that performed testing within a PHF model. This lack of relevant testing is important to recognize because the implantation of a humeral arthroplasty stem in the setting of a proximal humerus fracture is technically challenging and inherently unstable due the displacement of the tuberosity fragments. Furthermore, given the exponential increase in reverse total shoulder arthroplasty for PHF patients, relevant biomechanical testing would provide invaluable information to help guide treatment decisions [2].
Conclusion
The primary strength of this scoping review is the ability to identify key development areas to improve the quality and relevance of biomechanical modeling for proximal humerus fracture treatments. Our results suggest a strong need for implant testing in three- and four-part fracture models, testing of shoulder arthroplasty prostheses in a PHF model, and standardization of testing parameters to ensure results can be compared between studies. We anticipate this review will serve as springboard for designing studies aiming to address these key gaps in the future application of biomechanical testing for proximal humerus fracture treatments.
Abbreviations
- CDSR:
-
Cochrane database of systematic reviews
- CINAHL:
-
Cumulative Index of Nursing and Allied Health Literature
- EMBASE:
-
Excerpta medica database
- IQR:
-
Interquartile range
- MeSH:
-
Medical subject heading
- PHF:
-
Proximal humerus fracture
- RTSA:
-
Reverse total shoulder arthroplasty
- SAE:
-
Society of Automotive Engineers
- TRID:
-
Transport research international documentation
References
Jost B, Spross C, Grehn H, Gerber C. Locking place fixation of fractures of the proximal humerus: analysis of complications, revision strategies, and outcome. J Shoulder Elbow Surg. 2013;22:542–9. doi:10.1016/j.jse.2012.06.008.
Acevedo DC, Mann T, Abboud JA, Getz C, Baumhauer JF, Voloshin I. Reverse total shoulder arthroplasty for the treatment of proximal humeral fractures: patters of use among newly trained orthopaedic surgeons. J Shoulder Elbow Surg 2014. [Epub ahead of print]. doi: 10.1016/j.jse.2014.01.005.
Meier RA, Messmer P, Regazzoni P, Rothfischer W, Gross T. Unexpected high complication rate following internal fixation of unstable proximal humerus fractures with an angled blade plate. J Orthop Trauma. 2006;20:253–60.
Misra A, Kapur R, Maffulli N. Complex proximal humerus fractures in adults—a systematic review of management. Injury. 2001;32:363–72.
Ockert B, Siebenbürger G, Kettler M, Braunstein V, Mutschler M. Long-term functional outcomes (median 10 years) after locked plating for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2014. [Epub ahead of print] doi: 10.1016/j.jse.2013.11.009.
Ong CC, Kwon YW, Walsh M, Davidovitch R, Zuckerman JD, Egol KA. Outcomes of open reduction and internal fixation of proximal humerus fractures managed with locking plates. Am J Orthop. 2012;4:407–12.
Sohn HS, Shin SJ. Minimally invasive plate osteosynthesis for proximal humerus fractures: Clinical and radiographic outcomes according to fracture type. J Shoulder Elbow Surg 2014, [Epub ahead of print]. doi: 10.1016/j.jse.2013.12.018.
Tepass A, Rolauffs B, Weise K, Bahrs SD, Dietz K, Bahrs C. Complication rates and outcomes stratified by treatment modalities in proximal humerus fractures: a systematic literature review from 1970–2009. Patient Saf Surg. 2013;7:34. doi:10.1186/1754-9493-7-34.
Hanson B, Neidenbach P, de Boer P, Stengel D. Functional outcomes after non-operative management of fractures of the proximal humerus. J Shoulder Elbow Surg. 2009;18:612–21. doi:10.1016/j.jse.2009.03.024.
Kim SH, Szabo RM, Marder RA. Epidemiology of humerus fractures in the United States nationwide emergency department sample 2008. Arthritis Care Res. 2012;64:407–14. doi:10.1002/acr.21563.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. doi:10.1186/1748-5908-5-69.
McColl MA, Shortt S, Godwin M, Smith K, Rowe K, O’Brien P, et al. Models for integrating rehabilitation and primary care: a scoping study. Arch Phys Med Rehabil. 2009;90:1523–31. doi:10.1016/j.apmr.2009.03.017.
Slobogean GP, Johal H, Lefaivre K, MacIntyre NJ, Sprague SA, Scott T, et. al. A scoping review of the proximal humerus fracture literature. BMC Musculoskelet Disord. 2015;16(1):112
Acknowledgements
The authors would like to acknowledge Dean Giustini for his assistance with the literature search; Dawn Richards and Ravi Jain for their contributions as knowledge users; and Mikyla Grau, Manraj Chahal, Katherine Dmetrichuk, and Victoria Zuk for assistance with project coordination.
This study was coordinated at McMaster University and funded by a research grant from the Canadian Institutes of Health Research (Grant Number: 124598). The funding source had no role in the study design, data collection, dada analysis, interpretation of the data, writing of the manuscript, or the decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
DC participated in acquisition and interpretation of data and participated in manuscript review and critical appraisal and revision. KAL participated in acquisition and interpretation of data and participated in manuscript review and critical appraisal and revision. HJ participated in the acquisition and interpretation of data and participated manuscript review and critical appraisal and revision. NJM participated in the interpretation of data and in manuscript review and critical appraisal and revision. SAS participated in project design and coordination and helped to draft the manuscript. TS participated in the gathering and analysis of data and helped to draft the manuscript. PG participated in the interpretation of the data with regard to clinical relevance in orthopaedic surgery and participated in manuscript review and critical appraisal and revision. PAC participated in the interpretation of the data with regard to relevance in biomechanics and participated in manuscript review and critical appraisal and revision. MM participated in the interpretation of the data with regard to clinical relevance in orthopaedic surgery and participated in manuscript review and critical appraisal and revision. MB participated in project design and participated in manuscript review and critical appraisal and revision. GPS conceived the project and participated in its design, the interpretation and analysis of data, and manuscript review and critical appraisal and revision. All authors read and approved the final manuscript.
Additional files
Additional file 1:
Studies included in the analysis. (DOCX 28 kb)
Additional file 2:
Implants tested in each included study. (XLSX 46 kb)
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Cruickshank, D., Lefaivre, K.A., Johal, H. et al. A scoping review of biomechanical testing for proximal humerus fracture implants. BMC Musculoskelet Disord 16, 175 (2015). https://doi.org/10.1186/s12891-015-0627-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-015-0627-x